
Need for Orthodontic Treatment in Pupils Aged between 12 and 15 in the Valencian Region (Spain)

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Sample Size and Selection Criteria
2.3. Calibration Prior to the Study
2.4. Authorizations
2.5. Material Used
2.6. Data Collection
2.7. Data Processing and Statistical Analysis
- I. Professionals, senior managers, and senior technicians;
- II. Other managers, middle-level technicians, and commerce;
- III. Intermediate-level and administrative positions;
- IV (a). Skilled manual workers;
- IV (b). Semi-skilled manual workers;
- V. Unskilled workers;
- “Not classifiable” was the category denoting those without a declared or a wrongly declared profession, wrongly classified, or belonging to the armed forces.
3. Results
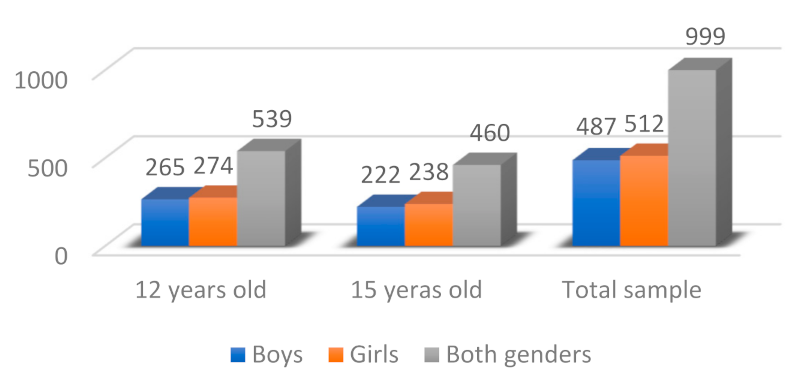
3.1. Population Examined
3.2. Wearers of Orthodontic Appliances
3.3. Socio-Economic Status
3.4. Traits of Malocclusion
3.5. Treatment Need: The IOTN-DHC Indices (IOTN Dental Health Component)
3.6. Treatment Need: IOTN-AC Indices (IOTN Aesthetic Component)
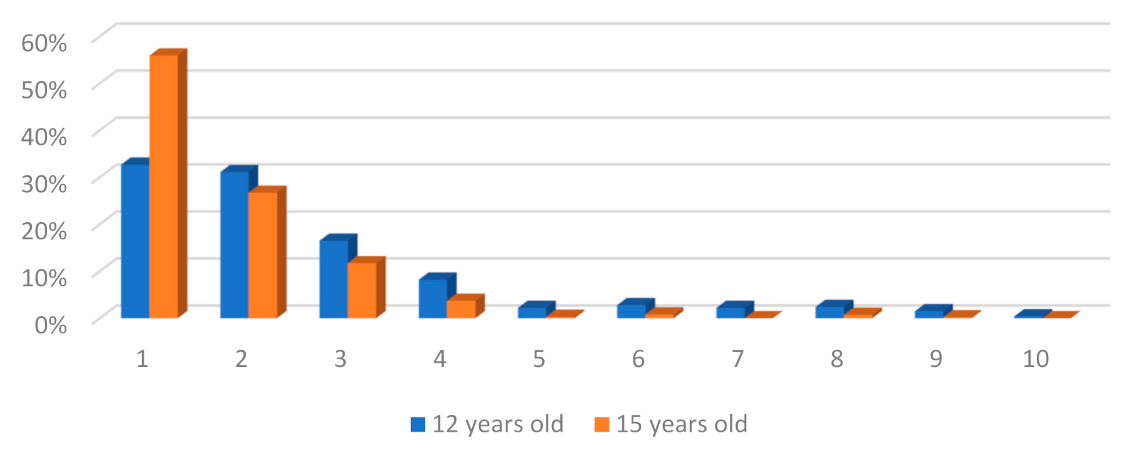
3.7. Treatment Need: DAI Index
3.8. Differences between Gender and Socio-Economic Status
4. Discussion
Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bellot-Arcis, C.; Montiel-Company, J.M.; Almerich-Silla, J.M.; Paredes-Gallardo, V.; Gandia-Franco, J.L. The use of occlusal indices in high-impact literature. Community Dent. Health 2012, 29, 45–48. [Google Scholar] [PubMed]
- Baca-García, A.; Baca, P.; Bravo, M.; Baca, A. Valoración y medición de las maloclusiones: Presente y futuro de los índices de maloclusión. Revisión bibliográfica. Arch. Odontoestomatol. 2002, 18, 654–662. [Google Scholar]
- World Health Organization OMS. Oral Health Surveys: Basic Methods, 5th ed.; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- World Health Organization OMS. Oral Health Surveys: Basic Methods, 4th ed.; WHO: Geneva, Switzerland, 1997. [Google Scholar]
- World Health Organization. Clasificación Internacional del Funcionamiento de la Discapacidad y de la Salud; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Almerich-Silla, J.; Montiel-Company, J.; Bellot-Arcís, C.; Puertes-Fernández, N. Cross-sectional study of malocclusion in Spanish children. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e15–e19. [Google Scholar] [CrossRef] [PubMed]
- Almerich-Torres, T.; Montiel-Company, J.M.; Bellot-Arcís, C.; Iranzo-Cortés, J.E.; Ortolá-Siscar, J.C.; Almerich-Silla, J.M. Caries Prevalence Evolution and Risk Factors among Schoolchildren and Adolescents from Valencia (Spain): Trends 1998–2018. Int. J. Environ. Res. Public Health 2020, 17, 6561. [Google Scholar] [CrossRef] [PubMed]
- Domingo Salvany, A.; Marcos Alonso, J. Proposal of an indicator of “social class” based on the occupation. Gac. Sanit. 1989, 3, 320–326. [Google Scholar] [CrossRef]
- Alonso, J.; Perez, P.; Saez, M.; Murillo, C. Validity of the occupation as an indicator of social class, according to the British Registrar General classification. Gac. Sanit. 1997, 11, 205–213. [Google Scholar] [CrossRef] [Green Version]
- Bravo-Pérez, M.; Casals-Peidró, E.; Cortés-Martincorena, F.J.; Lodra-Calvo, J.C. Encuesta de Salud Oral en España, 2005. RCOE 2006, 11, 409–456. [Google Scholar]
- Onyeaso, C.O.; Sanu, O.O. Perception of personal dental appearance in Nigerian adolescents. Am. J. Orthod. Dentofac. Orthop. 2005, 127, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Paula, D.F., Jr.; Silva, É.T.; Campos, A.C.V.; Nuñez, M.O.; Leles, C.R. Effect of anterior teeth display during smiling on the self-perceived impacts of malocclusion in adolescents. Angle Orthod. 2011, 81, 540–545. [Google Scholar] [CrossRef]
- Llodra-Calvo, J.C. Encuesta de salud oral en España 2010. RCOE 2012, 17, 13–41. [Google Scholar]
- Kok, Y.V.; Mageson, P.; Harradine, N.W.T.; Sprod, A.J. Comparing a quality of life measure and the Aesthetic Component of the Index of Orthodontic Treatment Need (IOTN) in assessing orthodontic treatment need and concern. J. Orthod. 2004, 31, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Ngom, P.I.; Diagne, F.; Dieye, F.; Diop-Ba, K.; Thiam, F. Orthodontic treatment need and demand in Senegalese school children aged 12–13 years. An appraisal using IOTN and ICON. Angle Orthod. 2007, 77, 323–330. [Google Scholar] [CrossRef] [Green Version]
- Sardenberg, F.; Oliveira, A.C.; Paiva, S.M.; Auad, S.M.; Vale, M.P. Validity and reliability of the Brazilian version of the psychosocial impact of dental aesthetics questionnaire. Eur. J. Orthod. 2011, 33, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Hedayati, Z.; Fattahi, H.R.; Jahromi, S.B. The use of index of orthodontic treatment need in an Iranian population. J. Indian Soc. Pedod. Prev. Dent. 2007, 25, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Bernabé, E.; Flores-Mir, C. Orthodontic treatment need in Peruvian young adults evaluated through Dental Aesthetic Index. Angle Orthod. 2006, 76, 417–421. [Google Scholar]
- Bellot Arcís, C. Necesidad de Tratamiento Ortodóncico en la Población Adulta de la Comunidad Valenciana. Ph.D. Thesis, Universitat de València, Valencia, Spain, 2011. [Google Scholar]
- Puertes Fernández, N. Necesidad de Tratamiento Ortodóncico e Impacto Psicosocial de la Estética Dental en los Adolescentes de la Comunidad Valenciana (2010). Ph.D. Thesis, Universitat de València, Valencia, Spain, 2014. [Google Scholar]
- Brook, P.H.; Shaw, W.C. The development of an index of orthodontic treatment priority. Eur. J. Orthod. 1989, 11, 309–320. [Google Scholar] [CrossRef] [Green Version]
- Otuyemi, O.D.; Ogunyinka, A.; Dosumu, O.; Cons, N.C.; Jenny, J. Malocclusion and orthodontic treatment need of secondary school students in Nigeria according to the dental aesthetic index (DAI). Int. Dent. J. 1999, 49, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Llodra Calvo, J.C.; Bravo Pérez, M.; Cortés Martinicorena, F.J. Encuesta de Salud Oral en España (2000). RCOE 2002, 7, 19–63. [Google Scholar]
- Esa, R.; Razak, I.A.; Allister, J.H. Epidemiology of malocclusion and orthodontic treatment need of 12–13-year-old Malaysian schoolchildren. Community Dent. Health 2001, 18, 31–36. [Google Scholar] [PubMed]
- Puertes-Fernandez, N.; Montiel-Company, J.M.; Almerich-Silla, J.M.; Manzanera, D. Orthodontic treatment need in a 12-year-old population in the Western Sahara. Eur. J. Orthod. 2011, 33, 377–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, C.R.; Couto, G.B.L.; Orestes Cardoso, S. Assessment of orthodontic treatment needs in Brazilian schoolchildren according to the Dental Aesthetic Index (DAI). Community Dent. Health 2007, 24, 145–148. [Google Scholar] [PubMed]
- Rwakatema, D.S.; Ng’ang’a, P.M.; Kemoli, A.M. Awareness and concern about malocclusion among 12–15 year-old children in Moshi, Tanzania. E. Afr. Med. J. 2006, 83, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Ansai, T.; Miyazaki, H.; Katoh, Y.; Yamashita, Y.; Takehara, T.; Jenny, J.; Cons, N.C. Prevalence of malocclusion in high school students in Japan according to the Dental Aesthetic Index. Community Dent. Oral Epidemiol. 1993, 21, 303–305. [Google Scholar] [CrossRef]
- Abdullah, M.S.; Rock, W.P. Assessment of orthodontic treatment need in 5,112 Malaysian children using the IOTN and DAI indices. Community Dent. Health 2001, 18, 242–248. [Google Scholar] [PubMed]
- van Wyk, P.J.; Drummond, R.J. Orthodontic status and treatment need of 12-year-old children in South Africa using the Dental Aesthetic Index. SADJ 2005, 60, 334–336. [Google Scholar]
- Boronat-Catalá, M.; Bellot-Arcís, C.; Montiel-Company, J.M.; Catalá-Pizarro, M.; Almerich-Silla, J.M. Orthodontic treatment need of 9, 12 and 15 year-old children according to the Index of Orthodontic Treatment Need and the Dental Aesthetic Index. J. Orthod. 2016, 43, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Jenny, J.; Cons, N.C.; Kohout, F.J.; Jakobsen, J. Differences in need for orthodontic treatment between Native Americans and the general population based on DAI scores. J. Public Health Dent. 1991, 51, 234–238. [Google Scholar] [CrossRef]
- Katoh, Y.; Ansai, T.; Takehara, T.; Yamashita, Y.; Miyazaki, H.; Jenny, J.; Cons, N.C. A comparison of DAI scores and characteristics of occlusal traits in three ethnic groups of Asian origin. Int. Dent. J. 1998, 48, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Martín-Cid, C.; Barbería-Leache, E.; González-Sanz, A.M.; Rioboó-García, R. Prevalencia de maloclusiones en niños de la Comunidad Autónoma de Madrid según el índice estético dental. Rev. Española Ortod. 2009, 39, 91–102. [Google Scholar]
- Baca-Garcia, A.; Bravo, M.; Baca, P.; Baca, A.; Junco, P. Malocclusions and orthodontic treatment needs in a group of Spanish adolescents using the Dental Aesthetic Index. Int. Dent. J. 2004, 54, 138–142. [Google Scholar] [CrossRef]
- Hamamci, N.; Basaran, G.; Uysal, E. Dental Aesthetic Index scores and perception of personal dental appearance among Turkish university students. Eur. J. Orthod. 2009, 31, 168–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, S.; Mandall, N.A.; DiBiase, D.; Shaw, W.C. The reliability of the Index of Orthodontic Treatment Need over time. J. Orthod. 2000, 27, 47–53. [Google Scholar] [CrossRef]
- Uçüncü, N.; Ertugay, E. The use of the Index of Orthodontic Treatment need (IOTN) in a school population and referred population. J. Orthod. 2001, 28, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Alkhatib, M.N.; Bedi, R.; Foster, C.; Jopanputra, P.; Allan, S. Ethnic variations in orthodontic treatment need in London schoolchildren. BMC Oral Health 2005, 5, 8. [Google Scholar] [CrossRef] [Green Version]
- Mandall, N.A.; Wright, J.; Conboy, F.; Kay, E.; Harvey, L.; O’Brien, K.D. Index of orthodontic treatment need as a predictor of orthodontic treatment uptake. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 703–707. [Google Scholar] [CrossRef]
- Souames, M.; Bassigny, F.; Zenati, N.; Riordan, P.J.; Boy-Lefevre, M.L. Orthodontic treatment need in French schoolchildren: An epidemiological study using the Index of Orthodontic Treatment Need. Eur. J. Orthod. 2006, 28, 605–609. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svedstrom-Oristo, A.L.; Pietila, T.; Pietila, I.; Vahlberg, T.; Alanen, P.; Varrela, J. Acceptability of dental appearance in a group of Finnish 16- to 25-year-olds. Angle Orthod. 2009, 79, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Emerich, K.; Williams, S.; Bodal, M. An appraisal and comparison of three methods of selecting patients for orthodontic treatment. Eur. J. Paediatr. Dent. 2011, 12, 143–149. [Google Scholar]
- Chaitra, K.; Reddy, N.; Reddy, S. Vanishree Orthodontic treatment: Need and demand in north karnataka school children. J. Clin. Diagn. Res. 2014, 8, ZC37–ZC42. [Google Scholar] [CrossRef]
- Jamilian, A.; Darnahal, A.; Damani, E.; Talaeipour, M.; Kamali, Z. Prevalence of Orthodontic Treatment Need and Occlusal Traits in Schoolchildren. Int. Sch. Res. Not. 2014, 2014, 349793. [Google Scholar] [CrossRef]
- Tsiouli, K.; Karamesinis, K.; Antonarakis, G.S.; Christou, P. Prediction model of regional orthodontic workforce needs, using Greece as an example. Eur. J. Paediatr. Dent. 2016, 17, 29–33. [Google Scholar]
- Woon, K.C.; Thong, Y.L.; Abdul Kadir, R. Permanent dentition occlusion in Chinese, Indian and Malay groups in Malaysia. Aust. Orthod. J. 1989, 11, 45–48. [Google Scholar] [PubMed]
- Burden, D.J.; Pine, C.M.; Burnside, G. Modified IOTN: An orthodontic treatment need index for use in oral health surveys. Community Dent. Oral Epidemiol. 2001, 29, 220–225. [Google Scholar] [CrossRef]
- Josefsson, E.; Bjerklin, K.; Lindsten, R. Malocclusion frequency in Swedish and immigrant adolescents-influence of origin on orthodontic treatment need. Eur. J. Orthod. 2007, 29, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ngom, P.I.; Brown, R.; Diagne, F.; Normand, F.; Richmond, S. A cultural comparison of treatment need. Eur. J. Orthod. 2005, 27, 597–600. [Google Scholar] [CrossRef] [PubMed]
- Ghijselings, I.; Brosens, V.; Willems, G.; Fieuws, S.; Clijmans, M.; Lemiere, J. Normative and self-perceived orthodontic treatment need in 11- to 16-year-old children. Eur. J. Orthod. 2014, 36, 179–185. [Google Scholar] [CrossRef]
- Proffit, W.R.; Fields, H.W. La Maloclusión y la Deformidad Dentofacial en la Sociedad Actual. In Ortodoncia Contemporánea. Teoría y Práctica; Proffit, W.R., Fields, H.W., Eds.; Ediciones Harcourt: Madrid, Spain, 2001; pp. 1–22. [Google Scholar]
- Bravo, L.A. Naturaleza de la maloclusión y justificación del tratamiento ortodóncico. In Manual de Ortodoncia; Bravo, L.A., Ed.; Síntesis: Madrid, Spain, 2003; pp. 26–52. [Google Scholar]
- Tickle, M.; Kay, E.J.; Bearn, D. Socio-economic status and orthodontic treatment need. Community Dent. Oral Epidemiol. 1999, 27, 413–418. [Google Scholar] [CrossRef]
- Hassan, A.H.; Amin, H. Association of orthodontic treatment needs and oral health-related quality of life in young adults. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 42–47. [Google Scholar] [CrossRef]
- Gazit-Rappaport, T.; Haisraeli-Shalish, M.; Gazit, E. Psychosocial reward of orthodontic treatment in adult patients. Eur. J. Orthod. 2010, 32, 441–446. [Google Scholar] [CrossRef]
- Paula, D.F., Jr.; Santos, N.C.M.; da Silva, E.T.; Nunes, M.F.; Leles, C.R. Psychosocial Impact of Dental Esthetics on Quality of Life in Adolescents. Angle Orthod. 2009, 79, 1188–1193. [Google Scholar] [CrossRef] [Green Version]
- Hunt, O.; Hepper, P.; Johnston, C.; Stevenson, M.; Burden, D. The Aesthetic Component of the Index of Orthodontic Treatment Need validated against lay opinion. Eur. J. Orthod. 2002, 24, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; McGrath, C.; Hägg, U. Associations between orthodontic treatment need and oral health—Related quality of life among young adults: Does it depend on how you assess them? Community Dent. Oral Epidemiol. 2011, 39, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Montiel-Company, J.M.; Bellot-Arcis, C.; Almerich-Silla, J.M. Validation of the psychosocial impact of dental aesthetics questionnaire (Pidaq) in Spanish adolescents. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e168–e173. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| 12 Years Old | 15 Years Old | |
|---|---|---|
| Overjet/reverse overjet | 3.34 (3.16–3.52) | 2.61 (2.45–2.76) |
| Overbite/openbite | 3.52 (3.33–3.71) | 2.88 (2.72–3.05) |
| Midline shift | 0.65 (0.56–0.74) | 0.59 (0.50–0.68) |
| Incisal crowding 1 segment | 28.8% (25.1–32.7%) | 22.8% (19.2–26.9%) |
| Incisal crowding 2 segments | 30.8% (27.0–34.8%) | 22.0% (18.4–26.0%) |
| Incisal spacing 1 segment | 17.5% (14.5–20.9%) | 11.6% (8.9–14.8%) |
| Incisal spacing 2 segments | 6.1% (4.4–8.5%) | 3.0% (1.8–5.0%) |
| Inter-incisal diastema | 0.32 (0.25–0.39) | 0.18 (0.13–0.23) |
| Highest maxillary irregularity | 1.61 (1.46–1.77) | 1.20 (1.05–1.36) |
| Highest mandibular irregularity | 1.41 (1.30–1.53) | 1.12 (1.01–1.25) |
| Unilateral posterior cross-bite | 10.4% (8.1–13.3%) | 8.9% (6.6–11.9%) |
| Bilateral posterior cross-bite | 2.2% (1.3–3.9%) | 2.4% (1.3–4.2%) |
| Molar class II right side | 23.2% (19.8–26.9%) | 20.9% (17.4–24.8%) |
| Molar class II left side | 25.5% (21.9–29.3%) | 4.6% (3.2–6.8%) |
| Molar class III right side | 5% (3.5–7.2%) | 4.8% (3.2–7.1%) |
| Molar class III left side | 23.3% (19.6–27.3%) | 5.4% (3.7–7.9%) |
| Canine class II right side | 23.2% (19.8–26.9%) | 18.3% (15.0–22.0%) |
| Canine class II left side | 26.2% (22.2–30.7%) | 19.8% (16.4–23.7%) |
| Canine class III right side | 5.2% (3.6–7.4%) | 5.2% (3.5–7.6%) |
| Canine class III left side | 4.7% (3.2–6.8%) | 6.3% (4.4–8.9%) |
| Age Group | |||
|---|---|---|---|
| 12 | 15 | ||
| Grade of malocclusion | Grade 1. No treatment need | 20.2% | 37% |
| (17.0–23.8%) | (32.7–41.5%) | ||
| Grade 2. Little treatment need | 43.6% | 38.4% | |
| (39.5–47.8%) | (34.1–43.0%) | ||
| Grade 3. Borderline treatment need | 23.6% | 17.6% | |
| (20.2–27.3%) | (14.4–21.4%) | ||
| Grade 4. Treatment required | 10.6% | 5.9% | |
| (8.3–13.5%) | (4.1–8.4%) | ||
| Grade 5. Treatment required | 2.0% | 1.1% | |
| (1.1–3.6%) | (0.4–2.5%) | ||
| 12 Years Old | 15 Years Old | ||
|---|---|---|---|
| DAI grades | Grade 1: No treatment need/slight treatment need | 52.5% | 66.7% |
| (48.3–56.7%) | (62.3–70.9%) | ||
| Grade 2: Elective treatment | 17.4% | 12.4% | |
| (14.5–20.9%) | (9.7–15.7%) | ||
| Grade 3: Highly desirable treatment | 14.9% | 10.5% | |
| (12.1–19.1%) | (7.9–13.6%) | ||
| Grade 4: Mandatory treatment | 15.2% | 10.4% | |
| (12.4–18.5%) | (7.9–13.6%) |
| Gender | Socio-Economic Status | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Boys | Girls | p-Value | Low | Intermediate | High | p-Value | |||
| Treatment need | 12 years old | IOTN-DCH | 14.0% | 11.3% | 0.36 | 18.0% | 9.0% | 12.6% | 0.05 |
| (13.3–18.7%) | (8.1–15.6%) | (12.5–25.2%) | (5.9–13.7%) | (8.6–18.1%) | |||||
| IOTN-AC | 4.5% | 4.0% | 0.77 | 5.0% | 2.9% | 5.3% | 0.43 | ||
| (2.6–7.7%) | (2.3–7.0%) | (2.5–10.0%) | (1.3–6.1%) | (2.9–9.4%) | |||||
| DAI | 27.9% | 32.1% | 0.29 | 34.5% | 30.0% | 26.8% | 0.32 | ||
| (22.9–33.6%) | (26.9–37.9%) | (27.2–42.8%) | (24.2–36.5%) | (21.0–33.6%) | |||||
| 15 years old | IOTN-DCH | 8.1% | 5.9% | 0.35 | 7.5% | 8.1% | 5.3% | 0.57 | |
| (5.2–12.5%) | (3.6–9.6%) | (3.9–14.2%) | (5.0–12.9%) | (2.8–9.8%) | |||||
| IOTN-AC | 0.5% | 1.3% | 0.35 | 2.8% | 0.5% | 0.0% | 0.04 * | ||
| (0.08–2.5%) | (0.4–3.6%) | (1.0–8.0%) | (0.01–3.0%) | (0.0–2.2%) | |||||
| DAI | 22.5% | 19.3% | 0.39 | 25.5% | 18.4% | 20.7% | 0.36 | ||
| (17.5–28.5%) | (14.8–24.8%) | (18.1–34.5%) | (13.5–24.6%) | (15.3–27.4%) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iranzo-Cortés, J.E.; Montiel-Company, J.M.; Bellot-Arcís, C.; Almerich-Torres, T.; Almerich-Silla, J.M. Need for Orthodontic Treatment in Pupils Aged between 12 and 15 in the Valencian Region (Spain). Int. J. Environ. Res. Public Health 2021, 18, 10162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910162
Iranzo-Cortés JE, Montiel-Company JM, Bellot-Arcís C, Almerich-Torres T, Almerich-Silla JM. Need for Orthodontic Treatment in Pupils Aged between 12 and 15 in the Valencian Region (Spain). International Journal of Environmental Research and Public Health. 2021; 18(19):10162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910162
Chicago/Turabian StyleIranzo-Cortés, José Enrique, José María Montiel-Company, Carlos Bellot-Arcís, Teresa Almerich-Torres, and José Manuel Almerich-Silla. 2021. "Need for Orthodontic Treatment in Pupils Aged between 12 and 15 in the Valencian Region (Spain)" International Journal of Environmental Research and Public Health 18, no. 19: 10162. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910162