
Hospital Childbirth: Perspectives of Women and Professionals for a Positive Experience—A Qualitative Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
- Women who gave birth to a live newborn, gestation greater than or equal to 37 weeks, cephalic presentation, 18 years of age or older, with adequate oral and written comprehension of Spanish and/or Basque language, and competent to understand and provide written informed consent.
- Professionals who had worked for at least 2 years in the labor ward.
- Individual semi-structured interviews were conducted 8 weeks (M-A) and 8 months (M-B) after childbirth. An open question began both the first and second interviews: at the 8th week, the question was “How was your birthing experience?”; at the 8th month, the question was “What do you remember about your birthing experience?”. During the interviews, the women were free to describe their experiences [25]. The interview duration ranged from 20 to 65 min, and they were conducted in the place chosen by the woman: at home, in cafeterias or in parks.
- Focus groups: The 4 focus groups (G1, G2, G3, and G4) included obstetricians, nursing assistants, and midwifery personnel who worked at the labor room. Three homogeneous groups and one heterogeneous group in terms of discipline were formed (see Table 2). The meetings were held in a hospital room, respecting the wishes of the participants. To guide the sessions, the following question was asked: “How do you view women’s childbirth experiences?” During the process, equitable participation was encouraged. At the end of the sessions, emerging topics and subtopics were discussed. Finally, a summary was made aloud and participants were encouraged to add or rectify the data.
- Participants’ observation: Participant observation was conducted in “natural” field situations [26] and it served to obtain direct experience of the childbirth phenomenon. The data obtained in situ were compared with the information obtained in the interviews and focus groups.
- Field journal: This was used to deepen in the meaning of the discourses and behaviors.
3. Results
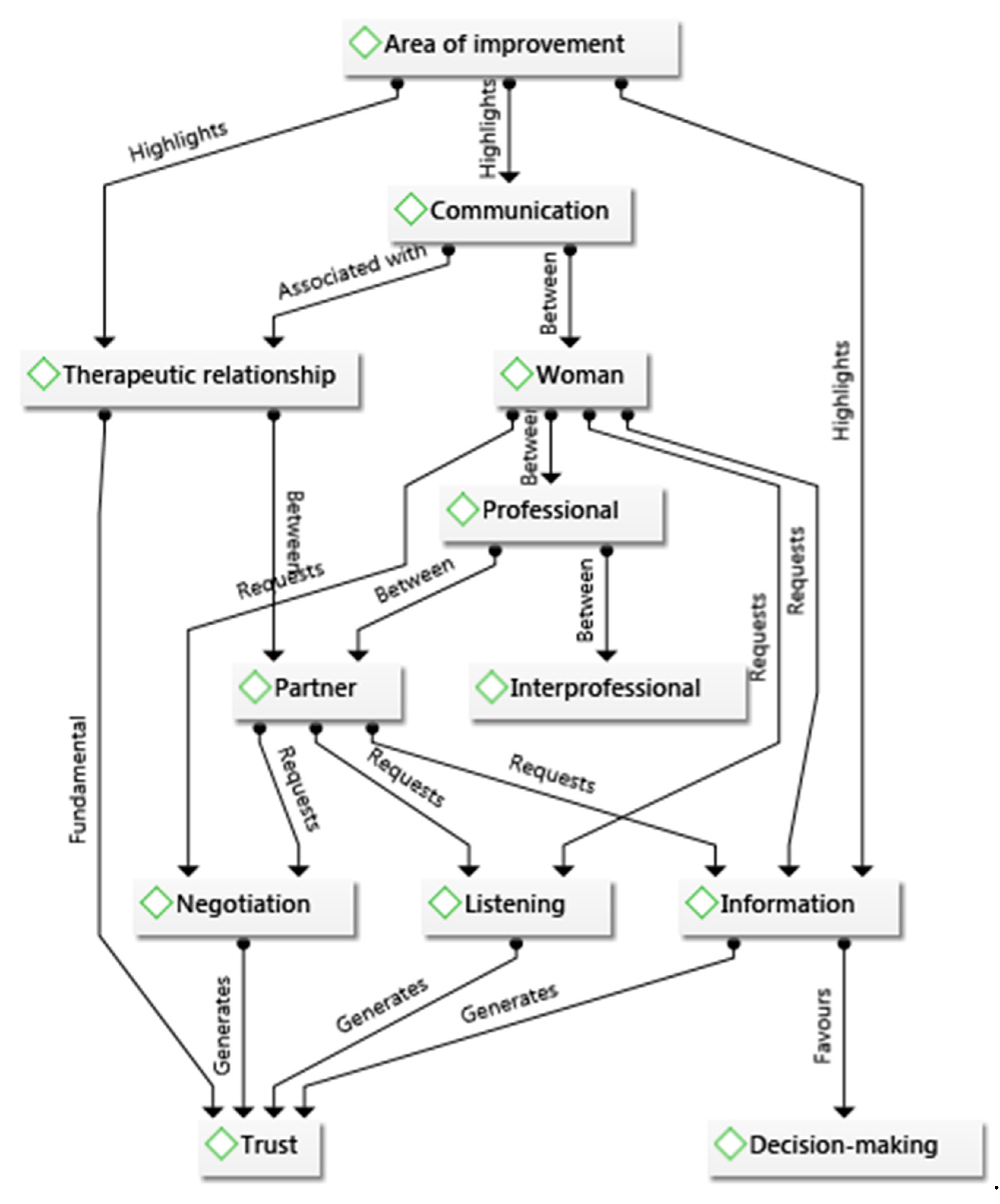
3.1. Strengthening Communication and the Therapeutic Relationship
“An explanation: this is what’s happened, we’ve done this, we’ve done the other… From now on you are going to notice this. This is normal, this is not normal”(25 M-A, 49:10).
“Sometimes we tell them too many things, and then we cannot get into detail and that is when they are left with biased information”4 G-1 (155:4).
“It would be better to try to say it another way in that moment of so much pain and when they are not well… a little more tactfully”17 M-A (34:32).
“Any suggestions? They are very good professionals, but there are some who should change their attitude”23 M-A (45:63).
“I feel like we may be lacking reassurance afterwards. For example, an instrument in a situation of urgency… they start wondering: is it because I have not pushed? Why have they induced me? Why?… These doubts remain unsolved”1 G-3 (149:20).
3.2. Unifying Criteria between Hospitals and Primary Care Centers to Provide Coordinated and Coherent Information
“Everyone is willing to help you. What happens is that there are 50,000 different midwives, each of whom has an opinion”15 M-A (30:68).
“The different criteria should be unified. Otherwise, you feel a little confused”37 M-B (136:35).
“I see women sometimes come with very idealized information about childbirth; that is dangerous”(3G-2, 153:8).
“I think there has been a lot of information given by theorists who have never been to a delivery room. So they are creating expectations… which are not real”(3G-1, 153:7).
“In the same way that we write medical protocols, I believe that follow-up protocols must be established, information that is not biased”(1G-1, 149:32).
“It would be necessary to analyze: why is there a lack of communication between primary and hospital midwives? It would be important”(3G-1, 153:6).
“It is important that there be more communication between gynaecologists, midwives, assistants… this teamwork does not exist nowadays”(3G-1, 153:21).
“The population… has changed a lot; I believe that coordination between the hospital and the primary care centers is still pending”(1 G-1, 149:28).
3.3. Involvement of the Partner in the Whole Process of Pregnancy-Childbirth-Puerperium
“That the father took part. If he is involved in the pregnancy, in childbirth, I believe that will help him be involved in the upbringing”(33 M-B, 133:7).
“I would like the schedule to be more flexible because, for example, my husband could not come to public antenatal classes and neither could I until I took the leave, I couldn’t go because the schedules coincided”(25 MA, 49:47).
“Yes, I would have liked them to be more practical, they seemed very theoretical to me. We were there for two hours and the midwife would spend two hours talking and we would not speak”(21 M-A, 41:54).
“Not dedicating so much time to theory, but having more practical lessons instead”(23 M-B, 115:5).
“They tell you that it is advisable to breastfeed for up to six months, but your maternity leave lasts four months… and many times you cannot… there are many contradictions. Also in the case of fathers, because for me it is very important that both parents are with the child so that bonding occurs”(37 M-A, 73:73).
3.4. Improvement of the Spaces Used in Prenatal Care and Births
“The room was very small and we all went without partners because we could not fit and we could not do the exercises”(28 M-B, 125:36).
“Another thing that could change would be the space of the delivery room, which is not friendly at all”2 G-2 (151:59).
“That everyone have the option of being in a comfortable and intimate place with their newborn […]”(4 G-3, 155:34).
“Everyone should have the option of being with their newborn”4 G-3 (155:34).
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larkin, P.; Begley, C.M.; Devane, D. “Not enough people to look after you”: An exploration of women’s experiences of childbirth in the Republic of Ireland. Midwifery 2012, 28, 98–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. WHO Recommendations: Intrapartum Care for a Positive Childbirth Experience; Licence: CC BY-NC-SA 3.0 IGO.; WHO: Geneva, Switzerland, 2018; Available online: https://www.who.int/reproductivehealth/publications/intrapartum-care-guidelines/en/ (accessed on 25 June 2021).
- Bringedal, H.; Aune, I. Able to choose? Women’s thoughts and experiences regarding informed choices during birth. Midwifery 2019, 77, 123–129. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, D.; Butler, M.M.; Casey, M. A participatory action research study exploring women’s understandings of the concept of informed choice during pregnancy and childbirth in Ireland. Midwifery 2017, 46, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Coates, D.; Thirukumar, P.; Spear, V.; Brown, G.; Henry, A. What are women’s mode of birth preferences and why? a systematic scoping review. Women Birth 2020, 33, 323–333. [Google Scholar] [CrossRef]
- Thompson, R.; Miller, Y.D. Birth control: To what extent do women report being informed and involved in decisions about pregnancy and birth procedures? BMC Pregnancy Childbirth 2014, 14, 62. [Google Scholar] [CrossRef] [Green Version]
- Hosseini Tabaghdehi, M.; Keramat, A.; Kolahdozan, S.; Shahhosseini, Z.; Moosazadeh, M.; Motaghi, Z. Positive childbirth experience: A qualitative study. Nurs. Open 2020, 7, 1233–1238. [Google Scholar] [CrossRef] [Green Version]
- Striebich, S.; Ayerle, G. Fear of childbirth (foc): Pregnant women’s perceptions towards the impending hospital birth and coping resources–a reconstructive study. J. Psychosom. Obs. Gynaecol. 2020, 41, 231–239. [Google Scholar] [CrossRef]
- Iida, M.; Horiuchi, S.; Nagamori, K. Women’s experience of receiving team-midwifery care in japan: A qualitative descriptive study. Women Birth 2021, 34, 493–499. [Google Scholar] [CrossRef]
- Aannestad, M.; Herstad, M.; Severinsson, E. A meta-ethnographic synthesis of qualitative research on women’s experience of midwifery care. Nurs. Health Sci. 2020, 22, 171–183. [Google Scholar] [CrossRef]
- Beecher, C.; Devane, D.; White, M.; Greene, R.; Dowling, M. Women’s experiences of their maternity care: A principle- based concept analysis. Women Birth 2020, 33, 419–425. [Google Scholar] [CrossRef]
- Hunter, A.; Devane, D.; Houghton, C.; Grealish, A.; Tully, A.; Smith, V. Woman-centred care during pregnancy and birth in ireland: Thematic analysis of women’s and clinicians’ experiences. BMC Pregnancy Childbirth 2017, 17, 322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NICE. Intrapartum Care: Care of Healthy Women and Their Babies during Childbirth; Clinical Guideline 190; RCOG Press: London, UK, 2014; Available online: https://www.nice.org.uk/guidance/cg190 (accessed on 25 June 2021).
- Thelin, I.L.; Lundgren, I.; Hermansson, E. Midwives’ lived experience of caring during childbirth—A phenomenological study. Sex. Reprod. Healthc. 2014, 5, 113–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goberna-Tricas, J.; Banús-Giménez, M.R.; Palacio-Tauste, A.; Linares-Sancho, S. Satisfaction with pregnancy and birth services: The quality of maternity care services as experienced by women. Midwifery 2011, 27, e231–e237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hunter, L.P. Being with woman: A guiding concept for the care of laboring women. J. Obstet. Gynecol. Neonatal Nurs. 2002, 31, 650–657. [Google Scholar] [CrossRef]
- Bradfield, Z.; Duggan, R.; Hauck, Y.; Kelly, M. Midwives being “with woman”: An integrative review. Women Birth 2018, 31, 143–152. [Google Scholar] [CrossRef]
- Redshaw, M. Women as consumers of maternity care: Measuring “satisfaction” or “dissatisfaction”? Birth 2008, 35, 73–76. [Google Scholar] [CrossRef]
- Klomp, T.; De Jonge, A.; Hutton, E.K.; Hers, S.; Lagro-Janssen, A.L.M. Perceptions of labour pain management of Dutch primary care midwives: A focus group study. BMC Pregnancy Childbirth 2016, 16, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Social Services and Equality. Estrategia de Atención al Parto Normal en el Sistema Nacional de Salud. Informe Sobre la Atención Al Parto y Nacimiento en El Sistema Nacional de Salud; Ministry of Health, Social Services and Equality: Madrid, Spain, 2012; Available online: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/pdf/InformeFinalEAPN_revision8marzo2015.pdf (accessed on 30 June 2021).
- Working Group of the Clinical Practice Guide on Attention to Normal Delivery. Guía De Práctica Clínica Sobre la Atención al Parto Normal; Quality Plan for the National Health System of the Ministry of Health and Social Policy; Basque Country Health Technology Assessment Agency (OSTEBA), Galician Health Technology Assessment Agency (Avalia-t): Gasteiz-Vitoria, Spain, 2010; Available online: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/pdf/equidad/guiaPracClinPartoCompleta.pdf (accessed on 30 June 2021).
- Maternidad Hospitalaria. Estándares Y Recomendaciones; Ministry of Health and Social Policy Publication Center: Madrid, Spain, 2009; Available online: https://www.mscbs.gob.es/organizacion/sns/planCalidadSNS/docs/AHP.pdf (accessed on 30 June 2021).
- Van Manen, M. Researching Lived Experience: Human Science for an Action Sensitive Pedagogy; State University of New York Press: Alabany, NY, USA, 1990. [Google Scholar]
- Morse, J. “Data were saturated…”. Qual. Health Res. 2015, 25, 587–588. [Google Scholar] [CrossRef] [Green Version]
- Rapley, T. Doing Conversation, Discourse and Document Analysis, 2nd ed.; Sage Publications: London, UK, 2018. [Google Scholar]
- Taylor, S.J.; Bogdan, R. Introduction to Qualitative Research Methods: A Guidebook and Resource; Wiley: New York, NY, USA, 1998. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology—Qualitative research in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Miles, M.B.; Huberman, A.M.; Saldaña, J. Qualitative Data Analysis: A Methods Sourcebook, 4th ed.; Sage Publications: London, UK, 2020. [Google Scholar]
- Creswell, J.W.; Poth, C.N. Qualitative Inquiry and Research Design: Choosing among Five Approaches, 4th ed.; Sage Publications: London, UK, 2018. [Google Scholar]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage Publications: Newbury Park, CA, USA, 1985. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (coreq): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Karlström, A.; Nystedt, A.; Hildingsson, I. The meaning of a very positive birth experience: Focus groups discussions with women. BMC Pregnancy Childbirth 2015, 15, 251. [Google Scholar] [CrossRef] [Green Version]
- Borrelli, S.E.; Spiby, H.; Walsh, D. The kaleidoscopic midwife: A conceptual metaphor illustrating first-time mothers’ perspectives of a good midwife during childbirth. A grounded theory study. Midwifery 2016, 39, 103–111. [Google Scholar] [CrossRef]
- Lohmann, S.; Mattern, E.; Ayerle, G.M. Midwives’ perceptions of women’s preferences related to midwifery care in Germany: A focus group study. Midwifery 2018, 61, 53–62. [Google Scholar] [CrossRef] [Green Version]
- Eggermont, K.; Beeckman, D.; Van Hecke, A.; Delbaere, I.; Verhaeghe, S. Needs of fathers during labour and childbirth: A cross-sectional study. Women Birth 2017, 30, e188–e197. [Google Scholar] [CrossRef] [PubMed]
- Steen, M.; Downe, S.; Bamford, N.; Edozien, L. Not-patient and not-visitor: A metasynthesis fathers’ encounters with pregnancy, birth and maternity care. Midwifery 2012, 28, 422–431. [Google Scholar] [CrossRef] [PubMed]
- Setola, N.; Naldi, E.; Cocina, G.; Eide, L.; Iannuzzi, L.; Daly, D. The impact of the physical environment on intrapartum maternity care: Identification of eight crucial building spaces. HERD 2019, 12, 67–98. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mondy, T.; Fenwick, J.; Leap, N.; Foureur, M. How domesticity dictates behaviour in the birth space: Lessons for designing birth environments in institutions wanting to promote a positive experience of birth. Midwifery 2016, 43, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Hammond, A.; Homer, C.S.E.; Foureur, M. Friendliness, functionality and freedom: Design characteristics that support midwifery practice in the hospital setting. Midwifery 2017, 50, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, C.; Wijk, H.; Höglund, L.; Sjöblom, H.; Hessman, E.; Berg, M. Effects of birthing room design on maternal and neonate outcomes: A systematic review. HERD J. 2020, 13, 198–214. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristics | N = 42 N (%) or Mean ± Standard Deviation | |
|---|---|---|
| Age | Age range in years: 25–43 | 34.6 ± 3.375 |
| Education | Primary | 4 (9.5%) |
| Secondary | 4 (9.5%) | |
| Post-secondary non-tertiary education | 9 (21.4%) | |
| Tertiary education or higher | 25 (59.5%) | |
| Weeks of pregnancy | Range in weeks: 37–42 | 39.8 ± 1.313 |
| Parity | Primiparous | 25 (59.5%) |
| Multiparous | 17 (40.5%) | |
| Type of delivery onset | Spontaneous | 24 (57.2%) |
| Induced | 18 (42.8%) | |
| Mode of birth | Normal | 27 (64.3%) |
| Forceps | 3 (7.1%) | |
| Vacuum extractor | 5 (11.9%) | |
| Spatula | 2 (4.8%) | |
| Urgent caesarean | 5 (11.9%) | |
| Analgesia use | None | 2 (4.8%) |
| Local anaesthesia | 3 (7.1%) | |
| Epidural anaesthesia | 37 (88.1%) | |
| Infant hospitalization | No | 38 (90.5%) |
| Yes | 4 (9.5%) |
| Focus Groups | Age | Profession | Years in the Labor Room |
|---|---|---|---|
| G1 | 54 | Obstetrician | 24 |
| G1 | 32 | Obstetrician | 3 |
| G1 | 44 | Obstetrician | 19 |
| G1 | 53 | Obstetrician | 22 |
| G2 | 58 | Midwife | 35 |
| G2 | 43 | Midwife | 10 |
| G2 | 53 | Midwife | 18 |
| G2 | 35 | Midwife | 6 |
| G3 | 55 | Midwife | 30 |
| G3 | 45 | Midwife | 21 |
| G4 | 58 | Midwife | 32 |
| G4 | 40 | Nursing assistant | 2 |
| G4 | 31 | Obstetrician | 3 |
| G4 | 50 | Nursing assistant | 8 |
| G4 | 61 | Midwife | 36 |
| Examples of Meaning Units | Codes | Category | Theme | |
|---|---|---|---|---|
| 8 weeks | “She was a little rude and did not talk to me, she talked to my husband. In addition, I thought, but the patient is me” 37 M-A (136:9). | C: Addressing the patient C: Ways of giving information C: Listening C: Communication | Professional treatment and its characteristics | Strengthening communication and the therapeutic relationship |
| 8 months | “Suddenly, a woman who never identified herself as the midwife who was going to deliver me came in, so I was lost because I had never seen her before” 14 M-B (28:24). | RP: Impersonal treatment RP: Cold and distant |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereda-Goikoetxea, B.; Huitzi-Egilegor, J.X.; Zubeldia-Etxeberria, J.; Uranga-Iturrioz, M.J.; Elorza-Puyadena, M.I. Hospital Childbirth: Perspectives of Women and Professionals for a Positive Experience—A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 10238. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910238
Pereda-Goikoetxea B, Huitzi-Egilegor JX, Zubeldia-Etxeberria J, Uranga-Iturrioz MJ, Elorza-Puyadena MI. Hospital Childbirth: Perspectives of Women and Professionals for a Positive Experience—A Qualitative Study. International Journal of Environmental Research and Public Health. 2021; 18(19):10238. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910238
Chicago/Turabian StylePereda-Goikoetxea, Beatriz, Joseba Xabier Huitzi-Egilegor, Josune Zubeldia-Etxeberria, Maria Jose Uranga-Iturrioz, and Maria Isabel Elorza-Puyadena. 2021. "Hospital Childbirth: Perspectives of Women and Professionals for a Positive Experience—A Qualitative Study" International Journal of Environmental Research and Public Health 18, no. 19: 10238. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910238