
Association between Anxiety, Depressive Symptoms, and Quality of Life in Patients Undergoing Diagnostic Flexible Video Bronchoscopy

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
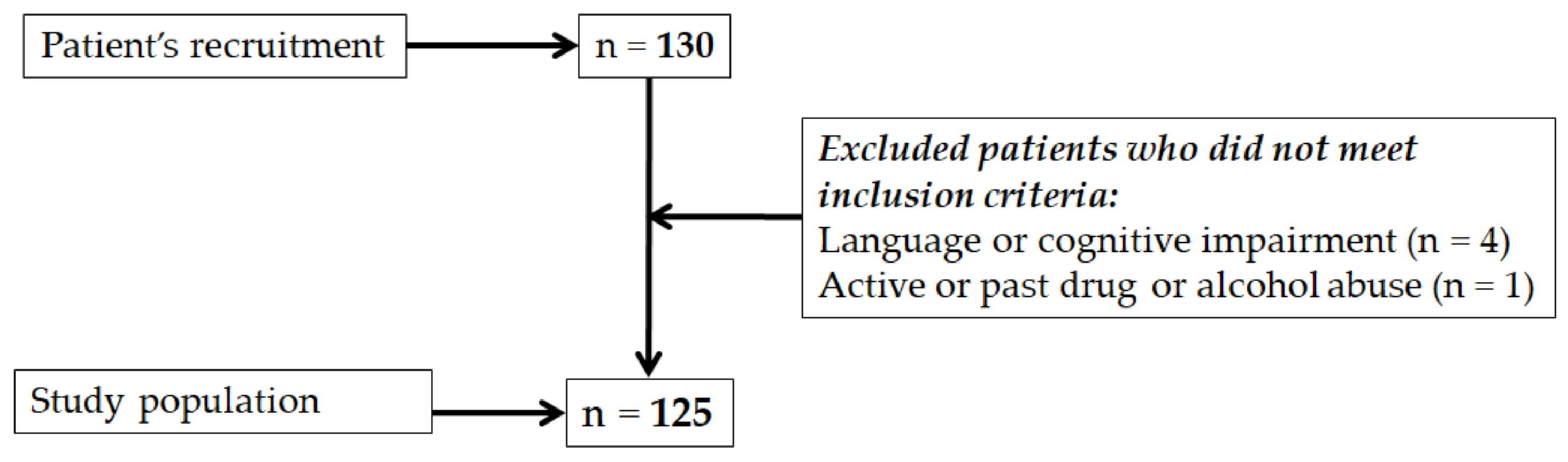
2.2. Study Population
2.3. Patients and Methods
2.4. Statistical Analysis
3. Results
3.1. Subject Characteristic
3.2. Depression and Anxiety Scores in Patients Undergoing Diagnostic FVB
3.3. Association between Anxiety, Depression, Quality of Life, and the FVB Procedure
4. Discussion
The Study Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Diette, G.B.; White, P.; Terry, P.; Jenckes, M.; Wise, R.A.; Rubin, H.R. Quality Assessment through Patient Self-Report of Symptoms Prefiberoptic and Postfiberoptic Bronchoscopy. Chest 1998, 114, 1446–1453. [Google Scholar] [CrossRef] [Green Version]
- British Thoracic Society. Quality Standards for Diagnostic Flexible Bronchoscopy in Adults. BTS Rep. 2014, 6, 1–37. [Google Scholar] [CrossRef]
- Faro, A.; Wood, R.E.; Schechter, M.S.; Leong, A.B.; Wittkugel, E.; Abode, K.; Chmiel, J.F.; Daines, C.; Davis, S.; Eber, E.; et al. Official American Thoracic Society Technical Standards: Flexible Airway Endoscopy in Children. Am. J. Respir. Crit. Care Med. 2015, 191, 1066–1080. [Google Scholar] [CrossRef]
- Aljohaney, A. Level and Predictors of Anxiety in Patients Undergoing Diagnostic Bronchoscopy. Ann. Thorac. Med. 2019, 14, 198–204. [Google Scholar] [CrossRef]
- Poi, P.J.H.; Chuah, S.Y.; Srinivas, P.; Liam, C.K. Common Fears of Patients Undergoing Bronchoscopy. Eur. Respir. J. 1998, 11, 1147–1149. [Google Scholar] [CrossRef] [Green Version]
- Leal, P.C.; Goes, T.C.; da Silva, L.C.F.; Teixeira-Silva, F. Trait vs. State Anxiety in Different Threatening Situations. Trends Psychiatry Psychother. 2017, 39, 147–157. [Google Scholar] [CrossRef]
- Baxter, A.J.; Scott, K.M.; Vos, T.; Whiteford, H.A. Global Prevalence of Anxiety Disorders: A Systematic Review and Meta-Regression. Psychol. Med. 2013, 43, 897–910. [Google Scholar] [CrossRef]
- Jones, K.M.; Castle, D.J.; Curran, E.M.; Piterman, L. Difficult-to-treat-depression: What do general practitioners think? Med. J. Aust. 2013, 199, 6–8. [Google Scholar] [CrossRef]
- Fiksdal, A.; Hanlin, L.; Kuras, Y.; Gianferante, D.; Chen, X.; Thoma, M.V.; Rohleder, N. Associations between Symptoms of Depression and Anxiety and Cortisol Responses to and Recovery from Acute Stress. Psychoneuroendocrinology 2019, 102, 44–52. [Google Scholar] [CrossRef]
- Merry, S.; Hetrick, S. Prevention of Depression and Anxiety: Is the Whole Better than the Sum of the Parts? Evid.-Based Ment. Health 2017, 20, e1. [Google Scholar] [CrossRef]
- Katon, W.; Lin, E.H.B.; Kroenke, K. The Association of Depression and Anxiety with Medical Symptom Burden in Patients with Chronic Medical Illness. Gen. Hosp. Psychiatry 2007, 29, 147–155. [Google Scholar] [CrossRef]
- Janson, C.; Björnsson, E.; Hetta, J.; Boman, G. Anxiety and Depression in Relation to Respiratory Symptoms and Asthma. Am. J. Respir. Crit. Care Med. 1994, 149, 930–934. [Google Scholar] [CrossRef]
- Catastini, P.; Di Marco, S.; Furriolo, M.; Genovese, C.; Grande, A.; Iacinti, E.; Iusco, D.R.; Nobili, R.M.V.; Pescini, R.; Ragni, R.; et al. The Prevalence of Anxiety and Depression in Italian Patients with Cystic Fibrosis and Their Caregivers. Pediatr. Pulmonol. 2016, 51, 1311–1319. [Google Scholar] [CrossRef]
- Garbarino, S.; Bardwell, W.A.; Guglielmi, O.; Chiorri, C.; Bonanni, E.; Magnavita, N. Association of Anxiety and Depression in Obstructive Sleep Apnea Patients: A Systematic Review and Meta-Analysis. Behav. Sleep Med. 2020, 18, 35–57. [Google Scholar] [CrossRef]
- Ho, C.S.; Ly Tan, E.; Ho, R.C.; Chiu, M.Y. Relationship of Anxiety and Depression with Respiratory Symptoms: Comparison between Depressed and Non-Depressed Smokers in Singapore. Int. J. Environ. Res. Public Health 2019, 16, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whalley, D.; McKenna, S.P. Measuring Quality of Life in Patients with Depression or Anxiety. Pharmacoeconomics 1995, 8, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Rifel, J.; Švab, I.; Selič, P.; Rotar Pavlič, D.; Nazareth, I.; Car, J. Association of Common Mental Disorders and Quality of Life with the Frequency of Attendance in Slovenian Family Medicine Practices: Longitudinal Study. PLoS ONE 2013, 8. [Google Scholar] [CrossRef] [Green Version]
- Hohls, J.K.; König, H.-H.; Quirke, E.; Hajek, A. Association between Anxiety, Depression and Quality of Life: Study Protocol for a Systematic Review of Evidence from Longitudinal Studies. BMJ Open 2019, 9, 27218. [Google Scholar] [CrossRef]
- Wenzel, A. State-Trait Anxiety Inventory. SAGE Encycl. Abnorm. Clin. Psychol. 2017, 1, 3–4. [Google Scholar] [CrossRef]
- Spielberger, C.; Gorsuch, R.; Lushene, R.; Vagg, P.R.; Jacobs, G. Manual for the State-Trait. Anxiety Inventory (Form. Y1–Y2); Consulting Psychologists Press: Palo Alto, CA, USA, 1983; Volume IV. [Google Scholar]
- Wrzsiński, K.; Sosnowski, T.; Jaworowska, A.; Fecenec, D. Inwentarz Stanu i Cechy Lęku Polska Adaptacja STAI. In Pracownia Testów Psychologicznych Polskiego Towarzystwa Psychologicznego sp. z o.o., 4th ed.; Psychological Tests Laboratory, Polish Psychological Association: Warszawa, Poland, 2011. [Google Scholar]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An Inventory for Measuring Depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- The World Health Organization Quality of Life Assessment (WHOQOL): Position Paper from the World Health Organization. Soc. Sci Med. 1995, 41, 1403–1409. [CrossRef]
- Power, M.; Kuyken, W. World Health Organization Quality of Life Assessment (WHOQOL): Development and General Psychometric Properties. Soc. Sci. Med. 1998, 46, 1569–1585. [Google Scholar] [CrossRef]
- Gonzalez, R.; De-La-Rosa-Ramirez, I.; Maldonado-Hernandez, A.; Dominguez-Cherit, G. Should Patients Undergoing a Bronchoscopy Be Sedated? Acta Anaesthesiol. Scand. 2003, 47, 411–415. [Google Scholar] [CrossRef] [PubMed]
- José, R.J.; Shaefi, S.; Navani, N. Sedation for Flexible Bronchoscopy: Current and Emerging Evidence. Eur. Respir. Rev. 2013, 22, 106–116. [Google Scholar] [CrossRef] [PubMed]
- Sessler, C.N.; Gosnell, M.S.; Grap, M.J.; Brophy, G.M.; O’Neal, P.V.; Keane, K.A.; Tesoro, E.P.; Elswick, R.K. The Richmond Agitation-Sedation Scale: Validity and Reliability in Adult Intensive Care Unit Patients. Am. J. Respir. Crit. Care Med. 2002, 166, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, R.; Murray, J. Spielberger’s State-Trait Anxiety Inventory: Measuring Anxiety with and without an Audience during Performance on a Stabilometer. Percept. Mot. Ski. 1983, 57, 15–18. [Google Scholar] [CrossRef] [PubMed]
- Weber, K.; Baertschi, M.; Andreas, S. Anxiety Disorders in Old Age: Psychiatric Comorbidities, Quality of Life, and Prevalence According to Age, Gender, and Country Early Developmental Stages of Psychopathology Study View Project Health Coaching for Chronic Conditions View Project. Artic. Am. J. Geriatr. Psychiatry 2017, 26, 174–185. [Google Scholar] [CrossRef]
- Vadla, D.; Bozikov, J.; Blazeković-Milaković, S.; Kovacić, L. Anxiety and depression in elderly-prevalence and association with health care. Lijec. Vjesn. 2013, 135, 134–138. [Google Scholar] [PubMed]
- De Lijster, J.M.; Dierckx, B.; Utens, E.M.W.J.; Verhulst, F.C.; Zieldorff, C.; Dieleman, G.C.; Legerstee, J.S. The Age of Onset of Anxiety Disorders: A Meta-Analysis. Can. J. Psychiatry 2017, 62, 237–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sargin, M.; Uluer, M.S.; Aydogan, E.; Hanedan, B.; Tepe, M.İ.; Eryılmaz, M.A.; Ebem, E.; Özmen, S. Anxiety Levels in Patients Undergoing Sedation for Elective Upper Gastrointestinal Endoscopy and Colonoscopy. Med. Arch. 2016, 70, 112–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillén-Riquelme, A.; Buela-Casal, G. [Meta-analysis of group comparison and meta-analysis of reliability generalization of the State-Trait Anxiety Inventory Questionnaire (STAI)]. Rev. Esp. Salud Publica 2014, 88, 101–112. [Google Scholar] [CrossRef]
- Creighton, A.S.; Davison, T.E.; Kissane, D.W. The Assessment of Anxiety in Aged Care Residents: A Systematic Review of the Psychometric Properties of Commonly Used Measures. Int. Psychogeriatr. 2018, 30, 967–979. [Google Scholar] [CrossRef]
- Asher, M.; Asnaani, A.; Aderka, I.M. Gender Differences in Social Anxiety Disorder: A Review. Clin. Psychol. Rev. 2017, 56, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Amiri, S.; Behnezhad, S. Obesity and Anxiety Symptoms: A Systematic Review and Meta-Analysis. Neuropsychiatrie 2019, 33, 72–89. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Sun, Q.; Zhai, L.; Bai, Y.; Wei, W.; Jia, L. The Prevalence of Depression and Anxiety Symptoms among Overweight/Obese and Non-Overweight/Non-Obese Children/Adolescents in China: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Güngör, N.K. Overweight and Obesity in Children and Adolescents. JCRPE J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef]
- Robinson, E.; Haynes, A.; Sutin, A.; Daly, M. Self-Perception of Overweight and Obesity: A Review of Mental and Physical Health Outcomes. Obes. Sci. Pract. 2020, 6, 552–561. [Google Scholar] [CrossRef]
- Bedolla-Barajas, M.; Morales-Romero, J.; Fonseca-López, J.C.; Pulido-Guillén, N.A.; Larenas-Linnemann, D.; Hernández-Colín, D.D. Anxiety and depression in adult patients with asthma: The role of asthma control, obesity and allergic sensitization. J. Asthma 2021, 58, 1058–1066. [Google Scholar] [CrossRef]
- Phan, T.; Carter, O.; Waterer, G.; Chung, L.P.; Hawkins, M.; Rudd, C.; Ziman, M.; Strobel, N. Determinants for Concomitant Anxiety and Depression in People Living with Chronic Obstructive Pulmonary Disease. J. Psychosom. Res. 2019, 120, 60–65. [Google Scholar] [CrossRef]
- Phan, T.; Carter, O.; Adams, C.; Waterer, G.; Ping Chung, L.; Hawkins, M.; Rudd, C.; Ziman, M.; Strobel, N. Discriminant Validity of the Hospital Anxiety and Depression Scale, Beck Depression Inventory (II) and Beck Anxiety Inventory to Confirmed Clinical Diagnosis of Depression and Anxiety in Patients with Chronic Obstructive Pulmonary Disease. Chron. Respir. Dis. 2016, 13, 220–228. [Google Scholar] [CrossRef] [Green Version]
- Karsten, J.; Penninx, B.W.J.H.; Riese, H.; Ormel, J.; Nolen, W.A.; Hartman, C.A. The State Effect of Depressive and Anxiety Disorders on Big Five Personality Traits. J. Psychiatr. Res. 2012, 46, 644–650. [Google Scholar] [CrossRef] [Green Version]
- Bagby, R.M.; Psych, C.; Quilty, L.C.; Ryder, A.C. Personality and depression. Can. J. Psychiatry 2008, 53, 14–25. [Google Scholar] [CrossRef] [Green Version]
- Klein, D.N.; Kotov, R.; Bufferd, S.J. Personality and Depression: Explanatory Models and Review of the Evidence. Annu. Rev. Clin. Psychol. 2011, 7, 269–295. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Lin, Y.; Xu, Y.; Zhou, H. The Impact of Depression and Anxiety on Quality of Life in Chinese Cancer Patient-Family Caregiver Dyads, a Cross-Sectional Study. Health Qual. Life Outcomes 2018, 16, 230. [Google Scholar] [CrossRef]
- Creighton, A.S.; Davison, T.E.; Kissane, D.W. The Correlates of Anxiety among Older Adults in Nursing Homes and Other Residential Aged Care Facilities: A Systematic Review. Int. J. Geriatr. Psychiatry 2017, 32, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Comer, J.S.; Blanco, C.; Hasin, D.S.; Liu, S.M.; Grant, B.F.; Turner, J.B.; Olfson, M. Health-Related Quality of Life across the Anxiety Disorders. J. Clin. Psychiatry 2010, 71. [Google Scholar] [CrossRef] [PubMed]
- Stelmach-Mardas, M.; Mardas, M.; Iqbal, K.; Tower, R.J.; Boeing, H.; Piorunek, T. Quality of Life, Depression and Dietary Intake in Obstructive Sleep Apnea Patients. Health Qual. Life Outcomes 2016, 14, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trevizan, F.B.; de Oliveira Santos Miyazaki, M.C.; Silva, Y.L.W.; Roque, C.M.W. Quality of Life, Depression, Anxiety and Coping Strategies after Heart Transplantation. Braz. J. Cardiovasc. Surg. 2017, 32, 162–170. [Google Scholar] [CrossRef] [Green Version]
- de Andrade de Lima, C.; de Oliveira, R.C.; de Oliveira, S.A.G.; da Silva, M.A.S.; de Andrade Lima, A.; Andrade, M.S.; Pinho, C.M. Quality of life, anxiety and depression in patients with chronic obstructive pulmonary disease. Rev. Bras. Enferm. 2020, 73 (Suppl. 1), e20190423. [Google Scholar] [CrossRef]
- Geraldo José Cunha, Â.; Zbonik Mendes, A.; Dias Wanderley de Carvalho, F.; Aparecida Ribeiro de Paula, M.; Gonçalves Brasil, T. The Impact of Asthma on Quality of Life and Anxiety: A Pilot Study. J. Asthma 2019, 56, 680–685. [Google Scholar] [CrossRef]
- Korkmaz, S.; Kazgan, A.; Çekiç, S.; Tartar, A.S.; Balcı, H.N.; Atmaca, M. The Anxiety Levels, Quality of Sleep and Life and Problem-Solving Skills in Healthcare Workers Employed in COVID-19 Services. J. Clin. Neurosci. 2020, 80, 131–136. [Google Scholar] [CrossRef]
- Gan, G.G.; Yuen, L.H. Anxiety, Depression and Quality of Life of Medical Students in Malaysia. Med. J. Malays. 2019, 74, 57–61. [Google Scholar]
- Kaneko, Y.; Mouri, T.; Seto, Y.; Nishioka, N.; Yoshimura, A.; Yamamoto, C.; Harita, S.; Chihara, Y.; Tamiya, N.; Yamada, T.; et al. The Quality of Life of Patients with Suspected Lung Cancer before and after Bronchoscopy and the Effect of Mirtazapine on the Depressive Status. Intern. Med. 2020, 59, 1605–1610. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Fujimoto, K.; Ishiwata, T.; Kasai Id, H.; Terada, J.; Shionoya, Y.; Ikari, J.; Kawata, N.; Tada, Y.; Tsushima, K.; Tatsumi, K. Identification of Factors during Bronchoscopy That Affect Patient Reluctance to Undergo Repeat Examination: Questionnaire Analysis after Initial Bronchoscopy. PLoS ONE 2018, 13, e0208495. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Analyzed Variable | Mean ± SD or % |
|---|---|
| Sex (% of men) | 39% |
| Age (years) | 54.2 ± 16.9 |
| Range: 19–87 | |
| BMI (kg/m2) | 24.6 ± 4.8 |
| Range: 16.1–37.4 | |
| BMI (kg/m2) categories (%) | |
| <18.5 (Underweight) | 10.6% |
| 18.5–24.9 (Healthy weight) | 42.6% |
| 25.0–29.9 (Overweight) | 32.8% |
| ≥30.0 (Obesity) | 14.0% |
| Level of education (%) | |
| Primary school | 29.0% |
| High school | 35.5% |
| University degree | 35.5% |
| Place of living (%) | |
| Village | 34.7% |
| Cities < 50,000 inhabitants | 11.3% |
| Cities 50,000 ≤ inhabitants < 100,000 | 15.3% |
| Cities ≥ 100,000 inhabitants | 38.7% |
| Inpatients/outpatients (%) | 28.2/71.8% |
| Previous FVB (%) | |
| No | 51% |
| Yes | 49% |
| Previous endoscopy—sedation type (%) | |
| Local sedation | 17% |
| Deep sedation | 83% |
| Comorbidities (%) | 55.6% |
| No of comorbidities | Mean within 2.5 (range: 1–10) |
| No of comorbidities | |
| Charlson Comorbidity Index for all patients | 2.35 ± (2.39) (range 0–11) |
| Depression and Anxiety Scores | Mean ± SD; Range or % |
|---|---|
| BDI-II total score: | 9.2 ± 8.6; 0 to 46 |
| BDI-II (%): | |
| No or minimal depression | 73.5% |
| Mild depression | 16.5% |
| Moderate depression | 6.7% |
| Severe depression | 3.3% |
| STAI-S | |
| Score: | 41.9 ± 10.4; 21 to 72 |
| STAI-T | |
| Score: | 41.7 ± 8.6; 21 to 70 |
| Analyzed Variable | STAI-State | STAI-Trait | ||||
|---|---|---|---|---|---|---|
| r | p-Value | r2 | r | p-Value | r2 | |
| BDI-II | ||||||
| Total score | 0.39 | <0.0001 | 0.14 | 0.65 | <0.0001 | 0.46 |
| No or minimal depression | −0.25 | 0.0072 | 0.13 | −0.58 | <0.0001 | 0.42 |
| Mild depression | 0.25 | 0.0072 | 0.07 | 0.49 | <0.0001 | 0.18 |
| Moderate depression | 0.12 | 0.1851 | 0.03 | 0.18 | 0.0474 | 0.16 |
| Severe depression | 0.13 | 0.1739 | 0.02 | 0.29 | 0.0015 | 0.04 |
| Quality of Life a | ||||||
| Physical health (D1) | −0.43 | <0.0001 | 0.26 | −0.41 | <0.0001 | 0.27 |
| Psychological (D2) | −0.39 | <0.0001 | 0.14 | −0.52 | <0.0001 | 0.21 |
| Social relationship (D3) | −0.15 | 0.0966 | 0.03 | −0.40 | <0.0001 | 0.13 |
| Environment (D4) | −0.25 | 0.0064 | 0.06 | −0.47 | <0.0001 | 0.19 |
| Total QOL | −0.39 | <0.0001 | 0.2 | −0.57 | <0.0001 | 0.38 |
| Analyzed Parameters | STAI-S Classification | STAI-T Classification | ||||||
|---|---|---|---|---|---|---|---|---|
| STAI Score (Points) | ≤35 | 36–45 | ≥46 | p-Value | ≤35 | 36–45 | ≥46 | p-Value |
| Sex (Female/Male) | 18F/14M | 33F/19M | 21F/12M | 11F/15M | 40F/20M | 21F/13M | ||
| Age (years) | 51.3 (18.6) | 52.4 (15.5) | 60.3 (16.7) | 0.0432 | 47.8 (16.6) | 54.6 (16.1) | 60.8 (14.0) | 0.0285 |
| BMI (kg/m2) | 23.76 (4.6) | 24.74 (4.9) | 25.32 (4.2) | 0.4886 | 24.3 (5.0) | 24.2 (4.6) | 27.1 (4.9) | 0.0675 |
| CCI | 1.56 (1.50) | 2.6 (2.5) | 2.7 (2.4) | 0.1514 | 1.3 (1.1) | 2.6 (2.5) | 2.7 (2.6) | 0.0405 |
| BDI-II | ||||||||
| Total score | 6.8 (6.1) | 7.9 (6.3) | 13.9 (10.0) | 0.0009 | 2.9 (2.8) | 7.6 (5.7) | 17.2 (8.7) | <0.0001 |
| Quality of Life a | ||||||||
| Physical health (D1) | 23.7 (2.8) | 21.9 (2.6) | 19.8 (3.5) | <0.0001 | 23.3 (3.4) | 22.1 (2.7) | 19.6 (3.0) | 0.0006 |
| Psychological (D2) | 22.1 (2.8) | 20.7 (2.9) | 19.0 (4.1) | 0.0011 | 23.1 (1.9) | 20.8 (2.7) | 18.6 (4.8) | <0.0001 |
| Social relationship (D3) | 11.7 (1.9) | 10.8 (2.4) | 11.0 (2.0) | 0.1469 | 12.4 (1.6) | 10.9 (2.3) | 10.6 (2.3) | 0.0015 |
| Environment (D4) | 31.2 (5.5) | 29.6 (6.2) | 28.1 (4.9) | 0.0242 | 33.9 (4.5) | 29.2 (5.4) | 27.8 (6.4) | 0.0002 |
| Total QOL | 95.5 (11.2) | 89.0 (11.6) | 83.3 (11.4) | <0.0001 | 98.8 (11.6) | 89.5 (10.3) | 81.8 (11.2) | <0.0001 |
| Depression risk % | 15.6 | 29.6 | 54.5 | 0.0016 | 3.8 | 20.0 | 76.5 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brajer-Luftmann, B.; Mardas, M.; Stelmach-Mardas, M.; Lojko, D.; Batura-Gabryel, H.; Piorunek, T. Association between Anxiety, Depressive Symptoms, and Quality of Life in Patients Undergoing Diagnostic Flexible Video Bronchoscopy. Int. J. Environ. Res. Public Health 2021, 18, 10374. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910374
Brajer-Luftmann B, Mardas M, Stelmach-Mardas M, Lojko D, Batura-Gabryel H, Piorunek T. Association between Anxiety, Depressive Symptoms, and Quality of Life in Patients Undergoing Diagnostic Flexible Video Bronchoscopy. International Journal of Environmental Research and Public Health. 2021; 18(19):10374. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910374
Chicago/Turabian StyleBrajer-Luftmann, Beata, Marcin Mardas, Marta Stelmach-Mardas, Dorota Lojko, Halina Batura-Gabryel, and Tomasz Piorunek. 2021. "Association between Anxiety, Depressive Symptoms, and Quality of Life in Patients Undergoing Diagnostic Flexible Video Bronchoscopy" International Journal of Environmental Research and Public Health 18, no. 19: 10374. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910374