
Palliative Care Coverage across European National Health Systems: Proposal of a Synthetic Indicator

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Primary Indicators and Data
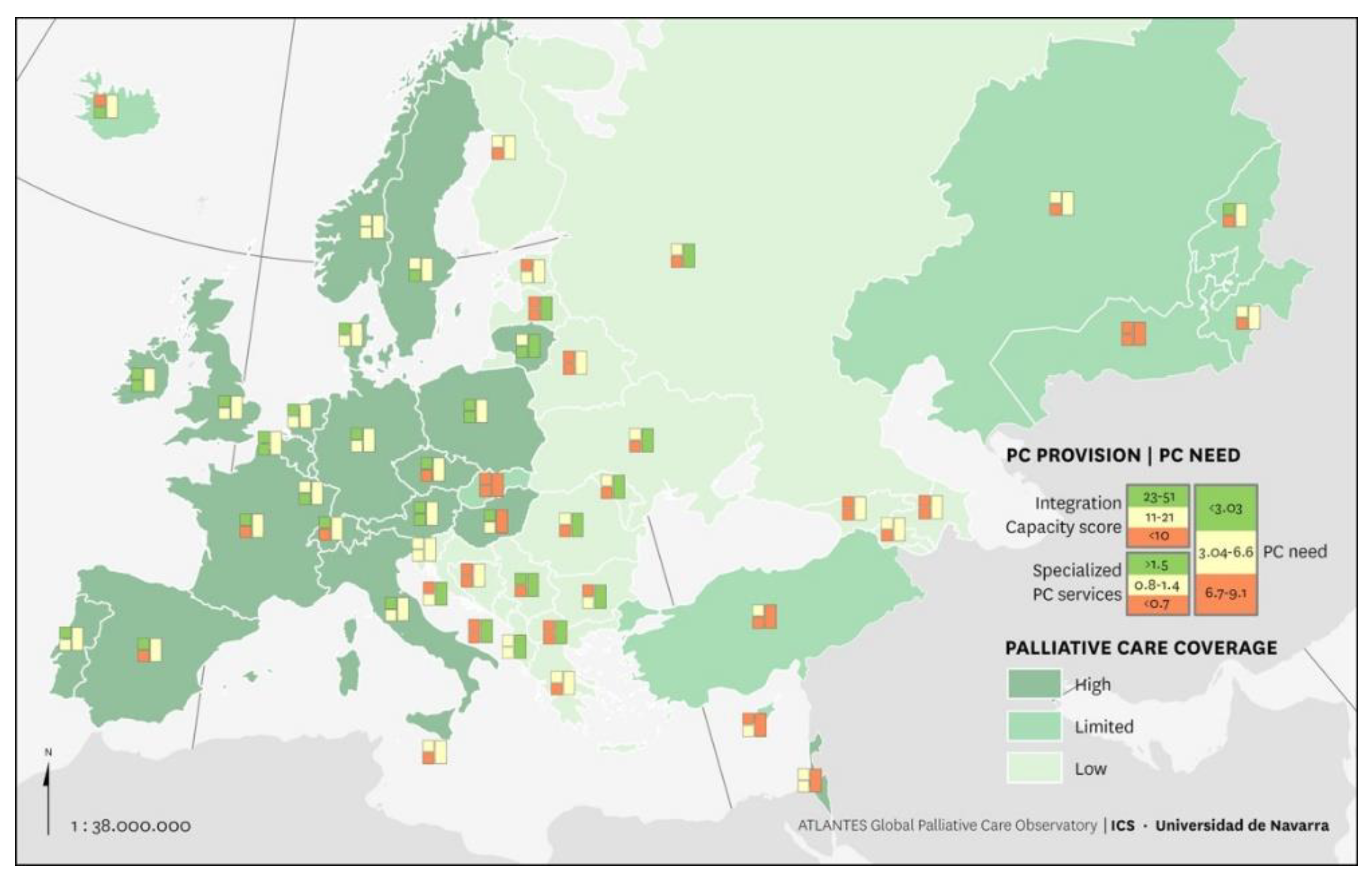
- Specialized palliative care services (SSPC) refers to the total number of reported specialized services per 100,000 inhabitants [13].
- Resources in other areas of the health system: Integration Capacity Score (ICS) refers to an indicator synthesizing PC activity in pediatrics, cardiology, oncology, primary care, long-term care, and volunteering. This score has a maximum value of 53 points and allows the classification of countries at a high level (score from 53–23), middle level (score from 22–11), and low level (<10 points) [2].
- The standardized need for palliative care for each country refers to the total number of patients who died due to SHS per 100,000 inhabitants in 2017. The burden of serious health-related suffering was based on the Lancet Commission report [18], using base mortality rates for 17 conditions from the WHO World European Mortality Database (EMD) [19].
2.2. Synthetic Coverage Indicator
2.3. External Validation
2.4. Patient and Public Involvement Statement
3. Results
3.1. Country Coverage Level (CCL)
3.2. External Validation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Assessing the Development of Palliative Care Worldwide: A Set of Actionable Indicators [Internet]. Available online: https://www.who.int/publications/i/item/9789240033351 (accessed on 5 October 2021).
- Sánchez-Cárdenas, M.A.; Garralda, E.; Arias-Casais, N.S.; Sastoque, E.R.B.; Van Steijn, D.; Moine, S.; Murray, S.A.; Centeno, C. Palliative care integration indicators: An European regional analysis. BMJ Support. Palliat. Care 2021. [Google Scholar] [CrossRef] [PubMed]
- Arias, N.; Garralda, E.; De Lima, L.; Rhee, J.Y.; Centeno, C. Global Palliative Care and Cross-National Comparison: How Is Palliative Care Development Assessed? J. Palliat. Med. 2019, 22, 580–590. [Google Scholar] [CrossRef] [PubMed]
- Wright, M.; Wood, J.; Lynch, T.; Clark, D. Mapping Levels of Palliative Care Development: A Global View. J. Pain Symptom Manag. 2008, 35, 469–485. [Google Scholar] [CrossRef] [PubMed]
- Lynch, T.; Connor, S.; Clark, D. Mapping Levels of Palliative Care Development: A Global Update. J. Pain Symptom Manag. 2013, 45, 1094–1106. [Google Scholar] [CrossRef] [PubMed]
- The Economist Intelligent Unit: The 2015 Quality of Death Index: Ranking Palliative Care Across the World. London, 2015. Available online: http://www.lienfoundation.org/sites/default/files/2015%20Quality%20of%20Death%20Report.pdf (accessed on 5 October 2021).
- Stjernswärd, J.; Foley, K.M.; Ferris, F.D. The Public Health Strategy for Palliative Care. J. Pain Symptom Manag. 2007, 33, 486–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osman, H.; Rihan, A.; Garralda, E.; Rhee, J.Y.; Pons-Izquierdo, J.J.; Lima, L.; Tfayli, A.; Centeno, C. Atlas of Palliative Care in the Eastern Mediterranean Region; IAHPC Press: Houston, TX, USA, 2017. [Google Scholar]
- Rhee, J.Y.; Luyirika, E.; Namisango, E.; Powell, R.A.; Garralda, E.; Pons-Izquierdo, J.J.; Lima, L.; Centeno, C. APCA Atlas of Palliative Care in Africa; AHPC Press: Houston, TX, USA, 2017. [Google Scholar]
- Pastrana, T.; Torres, I.; De Lima, L. Palliative care development in Latin America: An analysis using macro indicators. Palliat. Med. 2014, 28, 1231–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centeno-Cortes, C.; Lynch, T.; Donea, O.; Rocafort, J. EAPC Atlas of Palliative Care in Europe 2013-Full Edition; EAPC Press: Milan, Italy, 2013. [Google Scholar]
- Sharkey, L.; Loring, B.; Cowan, M.; Riley, L.; Krakauer, E.L. National palliative care capacities around the world: Results from the World Health Organization Noncommunicable Disease Country Capacity Survey. Palliat. Med. 2018, 32, 106–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arias-Casais, N.; López-Fidalgo, J.; Garralda, E.; Pons, J.J.; Rhee, J.Y.; Lukas, R.; De Lima, L.; Centeno, C. Trends analysis of specialized palliative care services in 51 countries of the WHO European region in the last 14 years. Palliat. Med. 2020, 34, 1044–1056. [Google Scholar] [CrossRef] [PubMed]
- Callaway, M.V.; Connor, S.; Foley, K.M. World Health Organization Public Health Model: A Roadmap for Palliative Care Development. J. Pain Symptom Manag. 2018, 55, S6–S13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, J.; Barnes, A.; Gardiner, C. Reframing Global Palliative Care Advocacy for the Sustainable Development Goal Era: A Qualitative Study of the Views of International Palliative Care Experts. J. Pain Symptom Manag. 2018, 56, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.A.; Alkema, L.; Black, R.E.; Boerma, J.T.; Collins, G.; Ezzati, M.; Grove, J.T.; Hogan, D.R.; Hogan, M.C.; Horton, R.; et al. Guidelines for Accurate and Transparent Health Estimates Reporting: The GATHER statement. Lancet 2016, 388, e19–e23. [Google Scholar] [CrossRef] [Green Version]
- Arias-Casais, N.; Garralda, E.; Rhee, J.Y.; de Lima, L.; Pons, J.J.; Clark, D.; Hasselaar, J.; Ling, J.; Mosoiu, D.; Centeno, C.; et al. EAPC Atlas of Palliative Care in Europe 2019; EAPC Press: Vilvoorde, Belgium, 2019; pp. 1–197. [Google Scholar]
- Knaul, F.M.; E Farmer, P.; Krakauer, E.L.; De Lima, L.; Bhadelia, A.; Kwete, X.J.; Arreola-Ornelas, H.; Gómez-Dantés, O.; Rodriguez, N.M.; Alleyne, G.A.O.; et al. Alleviating the access abyss in palliative care and pain relief—an imperative of universal health coverage: The Lancet Commission report. Lancet 2018, 391, 1391–1454. [Google Scholar] [CrossRef]
- WHO; Geneva, S. Projections of Mortality and Causes of Death, 2016 to 2060. Available online: http://www.who.int/healthinfo/global_burden_disease/projections/en/ (accessed on 12 October 2020).
- Clark, D.; Baur, N.; Clelland, D.; Garralda, E.; Lopez-Fidalgo, J.; Connor, S.; Centeno, C. Mapping Levels of Palliative Care Development in 198 Countries: The Situation in 2017. J. Pain Symptom Manag. 2020, 59, 794–807.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radbruch, L.; Payne, S. White paper on standards and norms for hospice and palliative care in Europe: Part 1. Eur. J. Palliat. Care. 2009, 17, 22–33. [Google Scholar]
- World Bank. World Bank Country and Lending Groups—World Bank Data Help Desk; The World Bank: Washington, DC, USA, 2020; pp. 1–8. [Google Scholar]
- Ferrell, B.R.; Temel, J.S.; Temin, S.; Alesi, E.R.; Balboni, T.A.; Basch, E.M.; Firn, J.I.; Paice, J.A.; Peppercorn, J.M.; Phillips, T.; et al. Integration of Palliative Care Into Standard Oncology Care: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2017, 35, 96–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, L.; Geller, T.P.; Baruah, R.; Beattie, J.M.; Boyne, J.; de Stoutz, N.; Di Stolfo, G.; Lambrinou, E.; Skibelund, A.K.; Uchmanowicz, I.; et al. Integration of a palliative approach into heart failure care: A European Society of Cardiology Heart Failure Association position paper. Eur. J. Hear. Fail. 2020, 22, 2327–2339. [Google Scholar] [CrossRef] [PubMed]
- Ewert, B.; Hodiamont, F.; van Wijngaarden, J.; Payne, S.; Groot, M.; Hasselaar, J.; Menten, J.; Radbruch, L. Building a taxonomy of integrated palliative care initiatives: Results from a focus group. BMJ Support. Palliat. Care 2016, 6, 14–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woitha, K.; Garralda, E.; Martin-Moreno, J.M.; Clark, D.; Centeno, C. Ranking of Palliative Care Development in the Countries of the European Union. J. Pain Symptom Manag. 2016, 52, 370–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Country | SSPC | ICS | Need PC |
|---|---|---|---|
| The Netherlands | 0.9 | 51 | 4.7 |
| UK | 1.3 | 47 | 5.5 |
| Germany | 1.1 | 43 | 5.9 |
| Switzerland | 1.0 | 40 | 5.1 |
| Belgium | 1.7 | 38 | 5.1 |
| Czech Rep. | 0.6 | 36 | 5.9 |
| Denmark | 0.9 | 36 | 5.4 |
| Italy | 0.9 | 36 | 5.8 |
| Poland | 1.5 | 35 | 5.5 |
| Spain | 0.6 | 35 | 4.9 |
| Austria | 2.2 | 34 | 5.1 |
| France | 1.0 | 33 | 4.4 |
| Kyrgyzstan | 0.2 | 26 | 3.7 |
| Hungary | 1.1 | 25 | 7.9 |
| Ireland | 1.9 | 25 | 5.5 |
| Portugal | 0.9 | 25 | 5.9 |
| Serbia | 0.2 | 23 | 8.7 |
| Albania | 0.9 | 21 | 6.7 |
| Romania | 0.6 | 21 | 9.1 |
| Israel | 1.4 | 20 | 2.6 |
| Lithuania | 1.7 | 19 | 7.9 |
| Sweden | 1.6 | 19 | 5.0 |
| Armenia | 0.2 | 17 | 6.1 |
| Greece | 0.0 | 17 | 6.1 |
| Luxembourg | 1.8 | 17 | 3.8 |
| Norway | 1.2 | 15 | 4.4 |
| Slovenia | 1.1 | 15 | 5.8 |
| Moldova | 0.5 | 14 | 7.7 |
| Russian Fed. | 0.2 | 14 | 7.4 |
| Turkey | 0.2 | 14 | 3.2 |
| Finland | 0.7 | 13 | 5.8 |
| Tajikistan | 0.1 | 13 | 3.8 |
| Ukraine | 0.1 | 13 | 8.3 |
| Kazakhstan | 0.1 | 12 | 4.8 |
| Malta | 0.4 | 11 | 4.4 |
| Belarus | 0.2 | 10 | 6.6 |
| Cyprus | 0.9 | 10 | 2.5 |
| Latvia | 0.6 | 10 | 8.4 |
| Slovakia | 0.0 | 10 | 0.2 |
| Georgia | 0.6 | 9 | 5.6 |
| Bulgaria | 1.4 | 8 | 10 |
| Croatia | 0.8 | 8 | 7.6 |
| Estonia | 1.4 | 8 | 6.6 |
| Azerbaijan | 0.0 | 6 | 6.0 |
| Bosnia & H. | 0.1 | 6 | 6.0 |
| Iceland | 1.5 | 6 | 3.5 |
| Macedonia | 0.3 | 6 | 6.8 |
| Montenegro | 0.0 | 3 | 8.4 |
| Uzbekistan | 0.0 | 3 | 2.5 |
| Mean | 0.79 | 19.92 | 5.69 |
| Std. Dev. | 0.60 | 12.45 | 1.92 |
| Kurtosis | −0.830 | −0.397 | 0.494 |
| Skewness | 0.383 | 0.758 | −0.197 |
| Country Coverage Level | Specialized PC Services | Integrated Resources in the Health System | PC Need | Countries | |||
|---|---|---|---|---|---|---|---|
| N° Services per 100,000 | Integration Capacity Score (ICS) | Deceased Patients with SHS per 100,000 Inhabitants, Year | n = 49 | ||||
| Level | Mean (Range) | Level | Mean (Range) | Level | Mean (Range) | n (%) | |
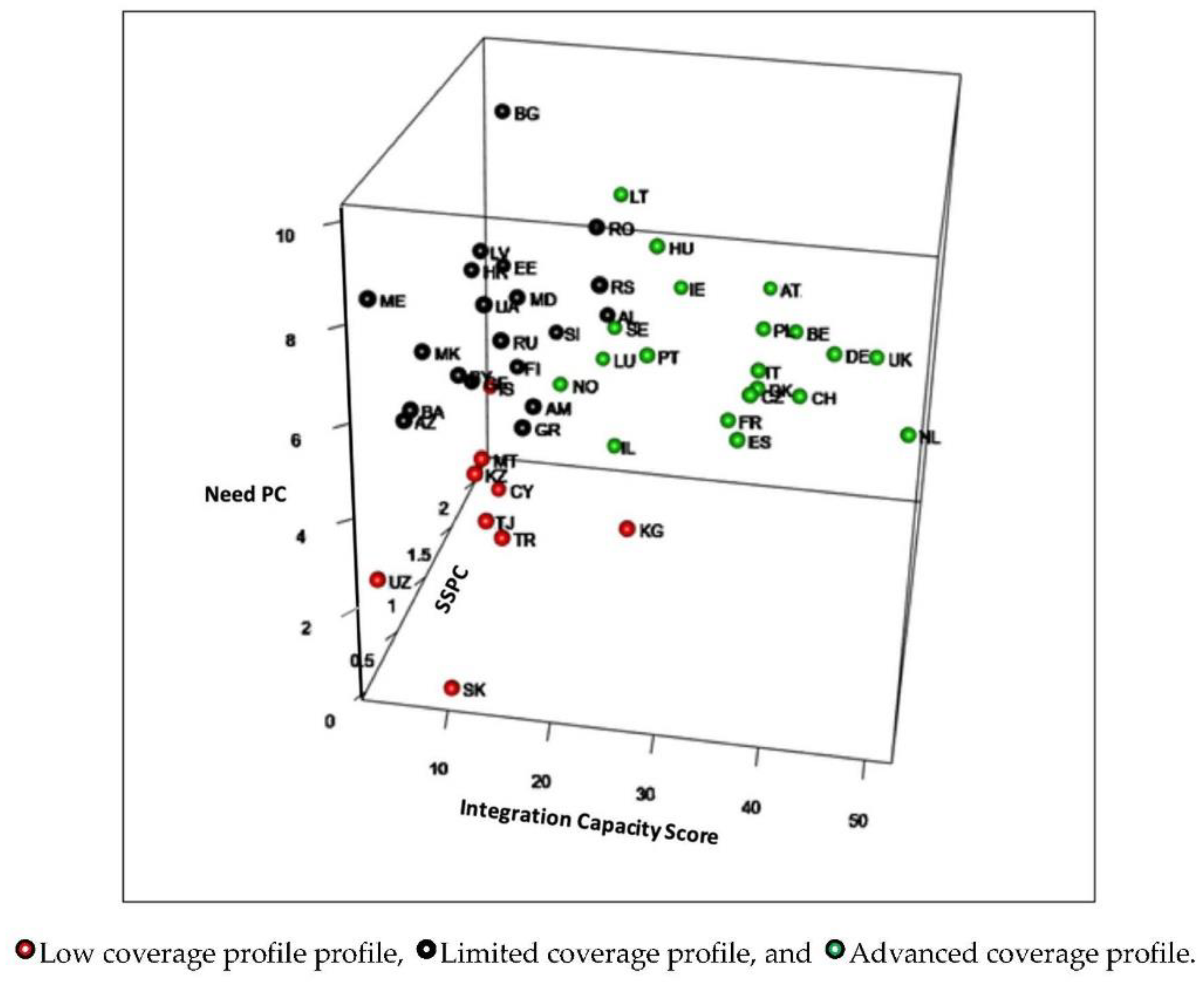
| Advanced Coverage profile | ↑ | 1.27 (0.6–2.2) | ↑ | 31.45 (15–51) | ↓ | 5.32 (2.6–7.9) | 20 (41) |
| Limited Coverage profile | ↓ | 0.38 (0–1.5) | ↓ | 11.67 (3–26) | ↓↓ | 3.18 (0.2–4.8) | 9 (18) |
| Low Coverage profile | ↓ | 0.50 (0–1.4) | ↓ | 12.10 (3–23) | ↑↑ | 7.19 (5.6–10) | 20 (41) |
| Country Development Level | Country | World Map of Palliative Care 2019 Level 1 |
|---|---|---|
| Advanced Coverage: countries with high scores on ICS, SSPC and low PC needs | The Netherlands | 4b |
| UK | 4b | |
| Germany | 4b | |
| Switzerland | 4a | |
| Belgium | 4b | |
| Czech Rep. | 4a | |
| Denmark | 4b | |
| Italy | 4b | |
| Poland | 4b | |
| Spain | 4b | |
| Austria | 4a | |
| France | 4b | |
| Hungary | 4a | |
| Ireland | 4b | |
| Portugal | 4b | |
| Israel | 4b | |
| Lithuania | 4b | |
| Sweden | 4b | |
| Luxembourg | 3b | |
| Norway | 4b | |
| Limited Coverage: countries with low levels of need and low ICS and SSPC scores | Kyrgyzstan | 3b |
| Turkey | 3b | |
| Tajikistan | 3b | |
| Kazakhstan | 4a | |
| Malta | 3b | |
| Cyprus | 3b | |
| Slovakia | 4a | |
| Iceland | 4b | |
| Uzbekistan | 2 | |
| Low Coverage: Countries with high levels of need and low levels of ICS and SSPC | Serbia | 3b |
| Albania | 3b | |
| Romania | 4b | |
| Armenia | 3a | |
| Greece | 3a | |
| Slovenia | 3b | |
| Moldova | 3a | |
| Russian Fed. | 4a | |
| Finland | 3b | |
| Ukraine | 4a | |
| Belarus | 3b | |
| Latvia | 4a | |
| Georgia | 4a | |
| Bulgaria | 3b | |
| Croatia | 3 | |
| Estonia | 3a | |
| Azerbaijan | 3b | |
| Bosnia & H. | 3a | |
| Macedonia | 3b | |
| Montenegro | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Cárdenas, M.A.; Garralda, E.; Benítez, E.; Arias-Casais, N.; van Steijn, D.; Centeno, C. Palliative Care Coverage across European National Health Systems: Proposal of a Synthetic Indicator. Int. J. Environ. Res. Public Health 2021, 18, 10753. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010753
Sánchez-Cárdenas MA, Garralda E, Benítez E, Arias-Casais N, van Steijn D, Centeno C. Palliative Care Coverage across European National Health Systems: Proposal of a Synthetic Indicator. International Journal of Environmental Research and Public Health. 2021; 18(20):10753. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010753
Chicago/Turabian StyleSánchez-Cárdenas, Miguel Antonio, Eduardo Garralda, Edgar Benítez, Natalia Arias-Casais, Danny van Steijn, and Carlos Centeno. 2021. "Palliative Care Coverage across European National Health Systems: Proposal of a Synthetic Indicator" International Journal of Environmental Research and Public Health 18, no. 20: 10753. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010753