
Isotemporal Substitution Analysis of Accelerometer-Derived Sedentary Behavior and Physical Activity on Cardiometabolic Health in Korean Adults: A Population-Based Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Accelerometer Measures of Physical Activity and Sedentary Behaviors
2.3. Blood Sample Test
2.4. Cardiometabolic Risk Factors
2.5. Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kelli, H.M.; Kassas, I.; Lattouf, O.M. Cardio metabolic syndrome: A global epidemic. J. Diabetes Metab. 2015, 6, 2–14. [Google Scholar] [CrossRef] [Green Version]
- Aguilar, M.; Bhuket, T.; Torres, S.; Liu, B.; Wong, R.J. Prevalence of the metabolic syndrome in the United States, 2003–2012. JAMA 2015, 313, 1973–1974. [Google Scholar] [CrossRef]
- Van Vliet-Ostaptchouk, J.V.; Nuotio, M.-L.; Slagter, S.N.; Doiron, D.; Fischer, K.; Foco, L.; Gaye, A.; Gögele, M.; Heier, M.; Hiekkalinna, T. The prevalence of metabolic syndrome and metabolically healthy obesity in Europe: A collaborative analysis of ten large cohort studies. BMC Endocr. Disord. 2014, 14, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.-H.; Lee, S.-H.; Shin, K.-S.; Son, D.-Y.; Kim, S.-H.; Joe, H.; Yoo, B.-W.; Hong, S.-H.; Cho, C.-Y.; Shin, H.-S. The change of metabolic syndrome prevalence and its risk factors in Korean adults for decade: Korea national health and nutrition examination survey for 2008–2017. Korean J. Fam. Pract. 2020, 10, 44–52. [Google Scholar] [CrossRef]
- Ranasinghe, P.; Mathangasinghe, Y.; Jayawardena, R.; Hills, A.; Misra, A. Prevalence and trends of metabolic syndrome among adults in the asia-pacific region: A systematic review. BMC Public Health 2017, 17, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, S.; Rohatgi, A.; Ayers, C.R.; Willis, B.L.; Haskell, W.L.; Khera, A.; Drazner, M.H.; de Lemos, J.A.; Berry, J.D. Cardiorespiratory fitness and classification of risk of cardiovascular disease mortality. Circulation 2011, 123, 1377–1383. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.W.; Popkin, B.M. Time use and physical activity: A shift away from movement across the globe. Obes. Rev. 2012, 13, 659–680. [Google Scholar] [CrossRef] [Green Version]
- Seguin, R.; Buchner, D.M.; Liu, J.; Allison, M.; Manini, T.; Wang, C.-Y.; Manson, J.E.; Messina, C.R.; Patel, M.J.; Moreland, L. Sedentary behavior and mortality in older women: The women’s health initiative. Am. J. Prev. Med. 2014, 46, 122–135. [Google Scholar] [CrossRef] [Green Version]
- Ding, D.; Mutrie, N.; Bauman, A.; Pratt, M.; Hallal, P.R.; Powell, K.E. Physical activity guidelines 2020: Comprehensive and inclusive recommendations to activate populations. Lancet 2020, 396, 1780–1782. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.; Altenburg, T.M.; Chinapaw, M.J. Sedentary behavior research network (SBRN)–terminology consensus project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M.T.; Hamilton, D.G.; Zderic, T.W. Role of low energy expenditure and sitting in obesity, metabolic syndrome, type 2 diabetes, and cardiovascular disease. Diabetes 2007, 56, 2655–2667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henson, J.; Yates, T.; Biddle, S.J.; Edwardson, C.L.; Khunti, K.; Wilmot, E.G.; Gray, L.J.; Gorely, T.; Nimmo, M.A.; Davies, M.J. Associations of objectively measured sedentary behaviour and physical activity with markers of cardiometabolic health. Diabetologia 2013, 56, 1012–1020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilmot, E.G.; Edwardson, C.L.; Achana, F.A.; Davies, M.J.; Gorely, T.; Gray, L.J.; Khunti, K.; Yates, T.; Biddle, S.J. Sedentary time in adults and the association with diabetes, cardiovascular disease and death: Systematic review and meta-analysis. Diabetologia 2012, 55, 2895–2905. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med. Sci. Sports Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Tanabe, K.; Yokoyama, N.; Zempo, H.; Kuno, S. Objectively measured light-intensity lifestyle activity and sedentary time are independently associated with metabolic syndrome: A cross-sectional study of Japanese adults. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.C.; Howe, G.R.; Kushi, L.H. Adjustment for total energy intake in epidemiologic studies. Am. J. Clin. Nutr. 1997, 65, 1220S–1228S. [Google Scholar] [CrossRef]
- Mekary, R.A.; Ding, E.L. Analysis of television viewing and physical activity using time substitution models. Arch. Intern. Med. 2010, 170, 1173–1174. [Google Scholar]
- Fishman, E.I.; Steeves, J.A.; Zipunnikov, V.; Koster, A.; Berrigan, D.; Harris, T.A.; Murphy, R. Association between objectively measured physical activity and mortality in NHANES. Med. Sci. Sports Exerc. 2016, 48, 1303. [Google Scholar] [CrossRef] [Green Version]
- Aggio, D.; Smith, L.; Hamer, M. Effects of reallocating time in different activity intensities on health and fitness: A cross sectional study. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Healy, G.N.; Winkler, E.A.; Brakenridge, C.L.; Reeves, M.M.; Eakin, E.G. Accelerometer-derived sedentary and physical activity time in overweight/obese adults with type 2 diabetes: Cross-sectional associations with cardiometabolic biomarkers. PLoS ONE 2015, 10, e0119140. [Google Scholar] [CrossRef]
- Huh, J.H.; Kang, D.R.; Jang, J.-Y.; Shin, J.-H.; Kim, J.Y.; Choi, S.; Cho, E.J.; Park, J.-S.; Sohn, I.S.; Jo, S.-H. Metabolic syndrome epidemic among Korean adults: Korean survey of Cardiometabolic Syndrome. Atherosclerosis 2018, 277, 47–52. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CDC/National Center for Health Statistics. National Health and Nutrition Examination Survey 2013–2014, Physical Activity Monitor Data Documentation, Codebook, and Frequencies. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2013-2014/PAXDAY_H.htm (accessed on 27 March 2021).
- Trost, S.G.; Pate, R.R.; Freedson, P.S.; Sallis, J.F.; Taylor, W.C. Using objective physical activity measures with youth: How many days of monitoring are needed? Med. Sci. Sports Exerc. 2000, 32, 426–431. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Im, J.-S.; Choi, Y.-H. Objectively measured sedentary behavior and moderate-to-vigorous physical activity on the health-related quality of life in US adults: The national health and nutrition examination survey 2003–2006. Qual. Life Res. 2017, 26, 1315–1326. [Google Scholar] [CrossRef] [PubMed]
- National Institutes of Health. SAS Programs for Analyzing NHANES 2003-2004 Accelerometer Data. Available online: https://epi.grants.cancer.gov/nhanes-pam/ (accessed on 27 March 2021).
- Bennie, J.A.; Ding, D.; Khan, A.; Stamatakis, E.; Biddle, S.J.; Kim, J. Run, lift, or both? Associations between concurrent aerobic–muscle strengthening exercise with adverse cardiometabolic biomarkers among Korean adults. Eur. J. Prev. Cardiol. 2020, 27, 738–748. [Google Scholar] [CrossRef] [PubMed]
- An, K.O.; Kim, J. Associations between handgrip strength with adverse cardiometabolic health among representative Korean adults. Int. J. Environ. Res. Public Health 2019, 17, 269. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Tanabe, K.; Yokoyama, N.; Zempo, H.; Kuno, S. Association between physical activity and metabolic syndrome in middle-aged Japanese: A cross-sectional study. BMC Public Health 2011, 11, 1–8. [Google Scholar] [CrossRef] [Green Version]
- De la Cámara, M.A.; Pardos-Sevilla, A.I.; Jiménez-Fuente, A.; Hubler-Figueiró, T.; d’Orsi, E.; Rech, C.R. Associations of mutually exclusive categories of physical activity and sedentary time with metabolic syndrome in older adults: An isotemporal substitution approach. J. Aging Phys. Act. 2021, 1, 1–9. [Google Scholar] [CrossRef]
- Kim, J. Association between meeting physical activity guidelines and mortality in Korean adults: An 8-year prospective study. J. Exerc. Nutr. Biochem. 2017, 21, 23. [Google Scholar] [CrossRef]
- Matthews, C.E.; Keadle, S.K.; Troiano, R.P.; Kahle, L.; Koster, A.; Brychta, R.; Van Domelen, D.; Caserotti, P.; Chen, K.Y.; Harris, T.B.; et al. Accelerometer-measured dose-response for physical activity, sedentary time, and mortality in US adults. Am. J. Clin. Nutr. 2016, 104, 1424–1432. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Tanabe, K.; Yoshizawa, Y.; Yokoyama, N.; Suga, Y.; Kuno, S. Lifestyle-based physical activity intervention for one year improves metabolic syndrome in overweight male employees. Tohoku J. Exp. Med. 2013, 229, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ford, E.S.; Caspersen, C.J. Sedentary behaviour and cardiovascular disease: A review of prospective studies. Int. J. Epidemiol. 2012, 41, 1338–1353. [Google Scholar] [CrossRef] [PubMed]
- Lerma, N.L.; Cho, C.C.; Swartz, A.M.; Miller, N.E.; Keenan, K.G.; Strath, S.J. Isotemporal substitution of sedentary behavior and physical activity on function. Med. Sci. Sports Exerc. 2018, 50, 792. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Yin, X.; Li, Y.; Bi, C.; Li, M.; Yang, X.; Zhang, T.; Zhang, F.; Cao, J.; Guo, Y. Isotemporal substitution of sedentary behavior for physical activity on cardiorespiratory fitness in children and adolescents. Medicine 2020, 99, e21367. [Google Scholar] [CrossRef]
- Ryan, D.J.; Wullems, J.A.; Stebbings, G.K.; Morse, C.I.; Stewart, C.E.; Onambele-Pearson, G.L. Using isotemporal substitution to predict the effects of changing physical behaviour on older adults’ cardio-metabolic profiles. PLoS ONE 2019, 14, e0224223. [Google Scholar] [CrossRef] [Green Version]
- Moura, B.P.; Rufino, R.L.; Faria, R.C.; Amorim, P.R.S. Effects of isotemporal substitution of sedentary behavior with light-intensity or moderate-to-vigorous physical activity on cardiometabolic markers in male adolescents. PLoS ONE 2019, 14, e0225856. [Google Scholar] [CrossRef]
- Galmes-Panades, A.M.; Varela-Mato, V.; Konieczna, J.; Wärnberg, J.; Martínez-González, M.; Salas-Salvadó, J.; Corella, D.; Schröder, H.; Vioque, J.; Alonso-Gómez, Á.M.; et al. Isotemporal substitution of inactive time with physical activity and time in bed: Cross-sectional associations with cardiometabolic health in the PREDIMED-Plus study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 137. [Google Scholar] [CrossRef] [Green Version]
- Chomistek, A.K.; Henschel, B.; Eliassen, A.H.; Mukamal, K.J.; Rimm, E.B. Frequency, type, and volume of leisure-time physical activity and risk of coronary heart disease in young women. Circulation 2016, 134, 290–299. [Google Scholar] [CrossRef] [Green Version]
- Oja, P. Dose response between total volume of physical activity and health and fitness. Med. Sci. Sports Exerc. 2001, 33 (Suppl. 6), S428–S437. [Google Scholar] [CrossRef] [Green Version]
- Wolff-Hughes, D.L.; Fitzhugh, E.C.; Bassett, D.R.; Churilla, J.R. Total activity counts and bouted minutes of moderate-to-vigorous physical activity: Relationships with cardiometabolic biomarkers using 2003–2006 NHANES. J. Phys. Act. Health 2015, 12, 694–700. [Google Scholar] [CrossRef]
- Bassett, D.R.; Troiano, R.P.; McClain, J.J.; Wolff, D.L. Accelerometer-based physical activity: Total volume per day and standardized measures. Med. Sci. Sports Exerc. 2015, 47, 833–838. [Google Scholar] [CrossRef] [PubMed]
- Lakka, T.A.; Laaksonen, D.E. Physical activity in prevention and treatment of the metabolic syndrome. Appl. Physiol. Nutr. Metab. 2007, 32, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Brien, S.E.; Katzmarzyk, P.T. Physical activity and the metabolic syndrome in Canada. Appl. Physiol. Nutr. Metab. 2006, 31, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Boulé, N.G.; Bouchard, C.; Tremblay, A. Physical fitness and the metabolic syndrome in adults from the Quebec family study. Can. J. Appl. Physiol. 2005, 30, 140–156. [Google Scholar] [CrossRef]
- Yang, X.; Telama, R.; Hirvensalo, M.; Mattsson, N.; Viikari, J.S.; Raitakari, O.T. The longitudinal effects of physical activity history on metabolic syndrome. Med. Sci. Sports Exerc. 2008, 40, 1424–1431. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Overall (n = 2197) | Male (n = 826) | Female (n = 1371) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Age [years] a | 48.92 | ± 0.33 | 50.23 | ± 0.55 | 48.14 | ± 0.40 | 0.002 |
| BMI [kg/m2] | 23.80 | ± 0.07 | 24.47 | ± 0.11 | 23.39 | ± 0.09 | <0.001 |
| Waist circumference [cm] | 80.95 | ± 0.21 | 85.68 | ± 0.30 | 78.10 | ± 0.24 | <0.001 |
| Systolic blood pressure [mmHg] | 116.72 | ± 0.35 | 120.08 | ± 0.51 | 114.69 | ± 0.45 | <0.001 |
| Diastolic blood pressure [mmHg] | 74.60 | ± 0.21 | 77.32 | ± 0.35 | 72.96 | ± 0.25 | <0.001 |
| Fasting blood glucose [mg/dL] | 99.48 | ± 0.50 | 102.75 | ± 0.86 | 97.50 | ± 0.61 | <0.001 |
| Hemoglobin A1c [%] | 5.69 | ± 0.02 | 5.74 | ± 0.03 | 5.66 | ± 0.02 | 0.020 |
| HDL cholesterol [mg/dL] | 51.83 | ± 0.26 | 47.48 | ± 0.39 | 54.45 | ± 0.33 | <0.001 |
| Triglyceride [mg/dL] | 127.02 | ± 2.41 | 154.19 | ± 5.18 | 110.65 | ± 2.16 | <0.001 |
| Total cholesterol [mg/dL] | 190.44 | ± 0.76 | 188.68 | ± 1.27 | 191.50 | ± 0.94 | 0.071 |
| Cardiometabolic risk factors [numbers] | 2.09 | ± 0.03 | 2.33 | ± 0.05 | 1.94 | ± 0.04 | <0.001 |
| Sedentary time (min/day) | 465.45 | ± 3.47 | 465.93 | ± 5.79 | 465.16 | ± 4.33 | 0.914 |
| Light intensity activity (min/day) | 216.23 | ± 1.95 | 203.00 | ± 3.23 | 224.21 | ± 2.42 | <0.001 |
| Lifestyle activity (min/day) | 79.42 | ± 1.18 | 80.35 | ± 2.00 | 78.86 | ± 1.45 | 0.537 |
| MVPA (min/day) | 32.63 | ± 0.73 | 38.51 | ± 1.31 | 29.09 | ± 0.84 | <0.001 |
| Wear time (min/day) | 793.74 | ± 4.63 | 787.80 | ± 7.47 | 797.31 | ± 5.90 | 0.320 |
| Education level [n (%)] b | |||||||
| <High School | 551 | (25.08) | 180 | (21.79) | 371 | (27.06) | 0.020 |
| High School | 807 | (36.73) | 312 | (37.77) | 495 | (36.11) | |
| >High School | 839 | (38.19) | 334 | (40.44) | 505 | (36.83) | |
| Household income [n (%)] | |||||||
| Q1 | 275 | (12.52) | 84 | (10.17) | 191 | (13.93) | 0.029 |
| Q2 | 605 | (27.54) | 230 | (27.85) | 375 | (27.35) | |
| Q3 | 674 | (30.68) | 249 | (30.15) | 425 | (31.0) | |
| Q4 | 643 | (29.27) | 263 | (31.84) | 380 | (27.72) | |
| Alcohol consumption [n (%)] | |||||||
| Never | 575 | (26.17) | 128 | (15.5) | 447 | (32.6) | <0.001 |
| Once a week | 1209 | (55.03) | 422 | (51.09) | 787 | (57.4) | |
| 2–3 times/week | 300 | (13.65) | 195 | (23.61) | 105 | (7.66) | |
| ≥4 times/week | 113 | (5.14) | 81 | (9.81) | 32 | (2.33) | |
| Smoking status [n (%)] | |||||||
| Never | 1547 | (70.41) | 276 | (33.41) | 1271 | (92.71) | <0.001 |
| Former | 389 | (17.71) | 340 | (41.16) | 49 | (3.57) | |
| Current | 261 | (11.88) | 210 | (25.42) | 51 | (3.72) | |
| Overall (n = 2197) | Male (n = 826) | Female (n = 1371) | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Abdominal obesity [n (%)] | 530 | (24.12) | 238 | (28.81) | 292 | (21.30) | <0.001 |
| High blood pressure [n (%)] | 761 | (34.64) | 364 | (44.07) | 397 | (28.96) | <0.001 |
| High fasting glucose [n (%)] | 712 | (32.41) | 342 | (41.40) | 370 | (26.99) | <0.001 |
| High hemoglobin A1c [n (%)] | 178 | (8.10) | 78 | (9.44) | 100 | (7.29) | 0.074 |
| High TG [n (%)] | 576 | (26.22) | 311 | (37.65) | 265 | (19.33) | 0.004 |
| Low HDL [n (%)] | 747 | (34.00) | 199 | (24.09) | 548 | (39.97) | <0.001 |
| High total cholesterol [n (%)] | 1078 | (49.07) | 389 | (47.09) | 689 | (50.26) | 0.151 |
| Adverse cardiometabolic risk factors, ≥3 [n (%)] | 817 | (37.19) | 372 | (45.04) | 445 | (32.46) | <0.001 |
| Adverse cardiometabolic risk factors, ≥4 [n (%)] | 420 | (19.12) | 184 | (22.28) | 236 | (17.21) | 0.004 |
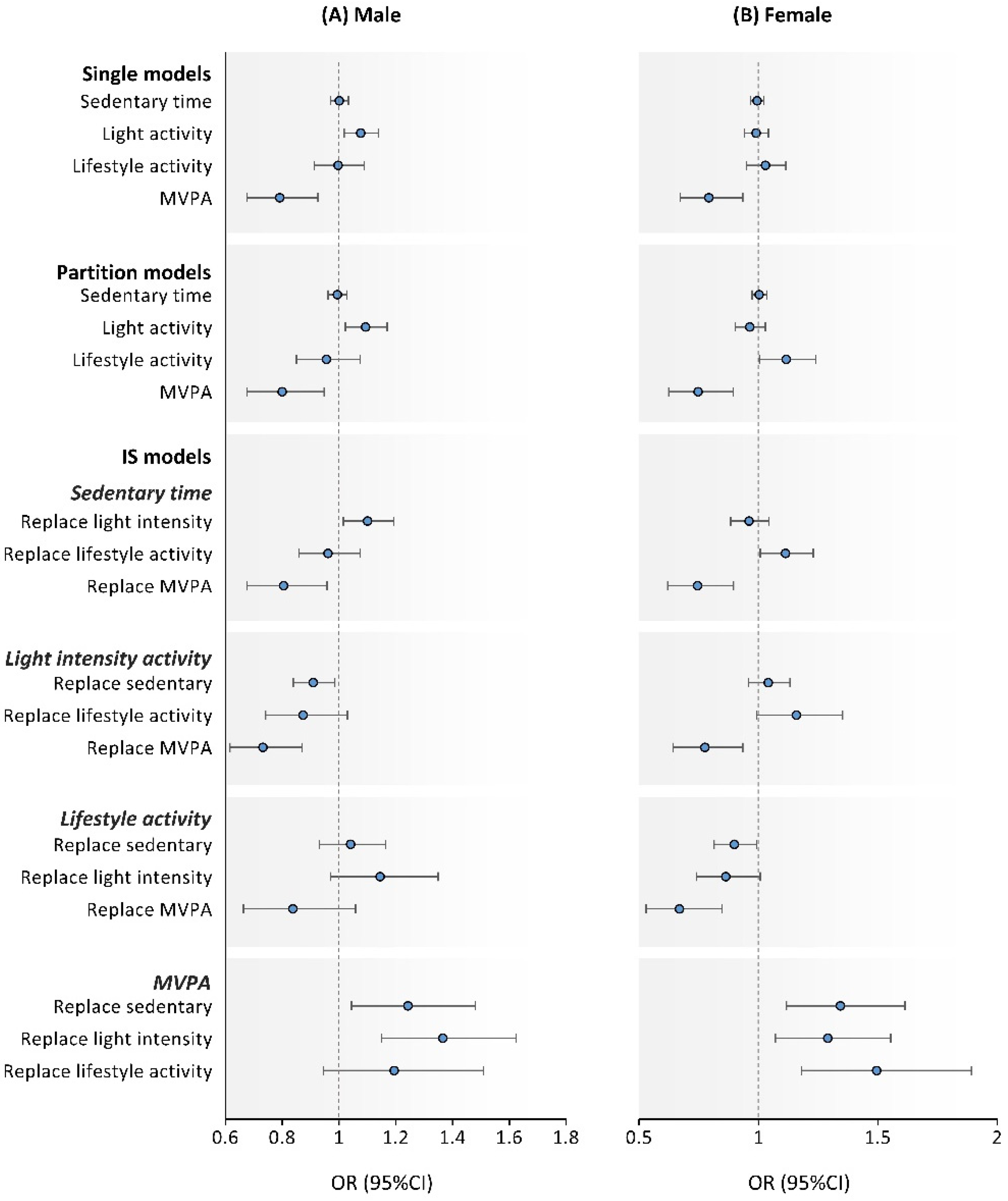
| Sedentary Time | Light Intensity Activity | Lifestyle Activity | MVPA | |||||
|---|---|---|---|---|---|---|---|---|
| OR | (95%CI) | OR | (95%CI) | OR | (95%CI) | OR | (95%CI) | |
| Single model | 0.99 | (0.98, 1.01) | 1.01 | (0.98, 1.04) | 1.01 | (0.96, 1.06) | 0.89 | (0.81, 0.97) |
| Partition model | 0.99 | (0.98, 1.01) | 1.00 | (0.97, 1.04) | 1.02 | (0.96, 1.10) | 0.87 | (0.80, 0.96) |
| IS models | ||||||||
| Replace sedentary | Dropped | 0.99 | (0.94, 1.04) | 0.97 | (0.91, 1.03) | 1.14 | (1.04, 1.25) | |
| Replace light intensity | 1.01 | (0.96, 1.06) | Dropped | 0.98 | (0.89, 1.08) | 1.15 | (1.05, 1.26) | |
| Replace lifestyle activity | 1.03 | (0.97, 1.10) | 1.02 | (0.93, 1.12) | Dropped | 1.17 | (1.03, 1.33) | |
| Replace MVPA | 0.88 | (0.80, 0.97) | 0.87 | (0.79, 0.96) | 0.85 | (0.75, 0.97) | Dropped | |
| Sedentary Time | Light Intensity Activity | Lifestyle Activity | MVPA | |||||
|---|---|---|---|---|---|---|---|---|
| OR | (95%CI) | OR | (95%CI) | OR | (95%CI) | OR | (95%CI) | |
| Single model | 0.99 | (0.97, 1.01) | 1.03 | (0.99, 1.06) | 1.02 | (0.96, 1.08) | 0.79 | (0.70, 0.88) |
| Partition model | 0.99 | (0.97, 1.01) | 1.02 | (0.97, 1.07) | 1.05 | (0.97, 1.13) | 0.76 | (0.68, 0.86) |
| IS models | ||||||||
| Replace sedentary | Dropped | 0.97 | (0.92, 1.03) | 0.95 | (0.88, 1.02) | 1.30 | (1.14, 1.47) | |
| Replace light intensity | 1.03 | (0.97, 1.09) | Dropped | 0.97 | (0.87, 1.09) | 1.33 | (1.18, 1.51) | |
| Replace lifestyle activity | 1.05 | (0.98, 1.13) | 1.03 | (0.92, 1.15) | Dropped | 1.37 | (1.16, 1.61) | |
| Replace MVPA | 0.77 | (0.68, 0.87) | 0.75 | (0.66, 0.85) | 0.73 | (0.62, 0.86) | Dropped | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, J.; Kim, H.; Kim, J. Isotemporal Substitution Analysis of Accelerometer-Derived Sedentary Behavior and Physical Activity on Cardiometabolic Health in Korean Adults: A Population-Based Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 11102. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111102
Ma J, Kim H, Kim J. Isotemporal Substitution Analysis of Accelerometer-Derived Sedentary Behavior and Physical Activity on Cardiometabolic Health in Korean Adults: A Population-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(21):11102. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111102
Chicago/Turabian StyleMa, Jiameng, Hyunshik Kim, and Junghoon Kim. 2021. "Isotemporal Substitution Analysis of Accelerometer-Derived Sedentary Behavior and Physical Activity on Cardiometabolic Health in Korean Adults: A Population-Based Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 21: 11102. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111102