
An Evaluation of Natural Environment Interventions for Informal Cancer Caregivers in the Community


Abstract
:1. Introduction
1.1. Theoretical Underpinnings
1.2. Background
2. Materials and Methods
2.1. Stage 1: Identification of the Research Question and Eligibility Criteria
2.2. Stage 2: Identification of Relevant Publications
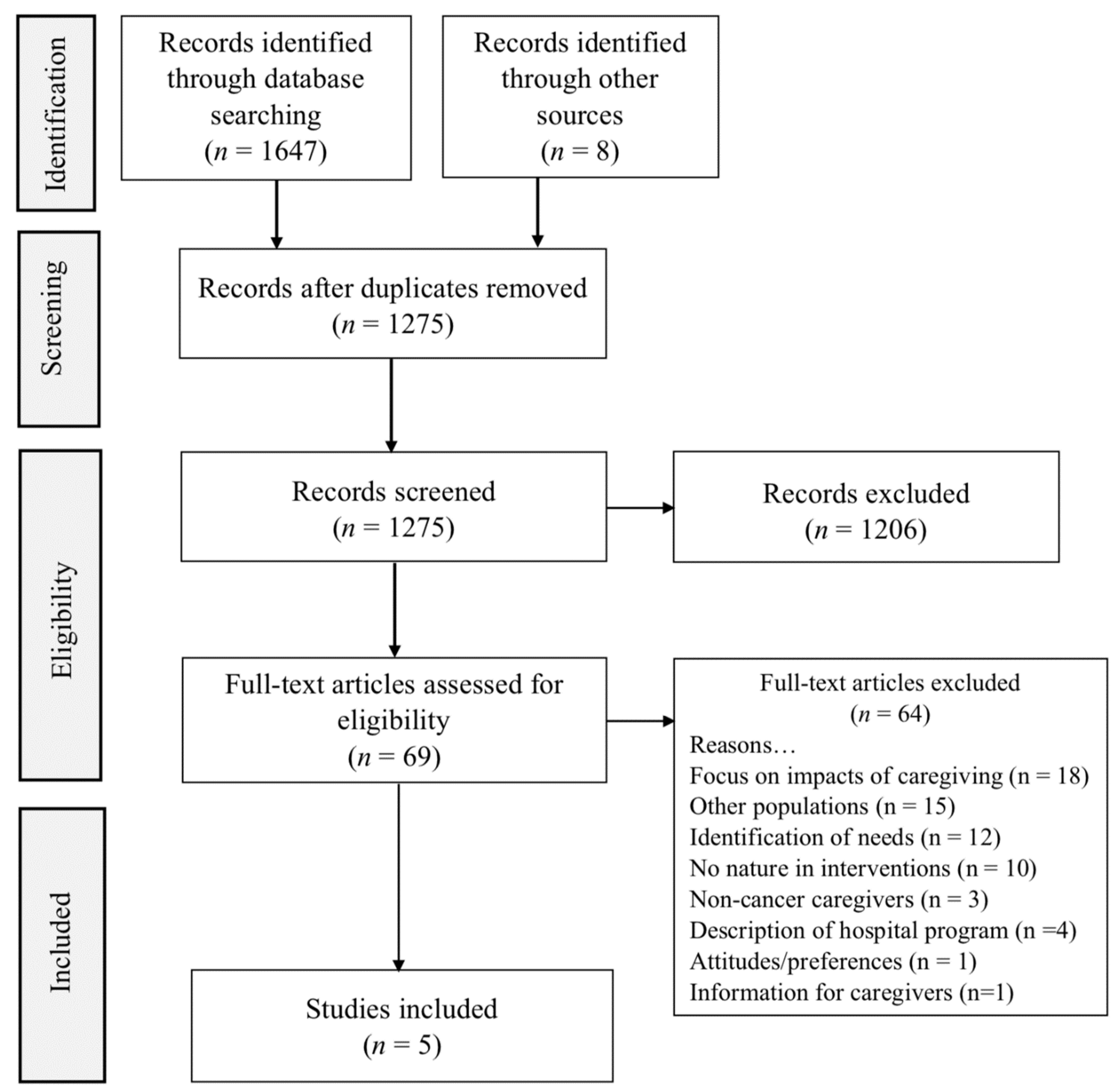
2.3. Stage 3: Selection of Publications
3. Results
3.1. Stage 4 and 5: Charting the Data and Collating, Summarizing, and Reporting the Results
3.2. Summary
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Robinson, J.M.; Jorgensen, A.; Cameron, R.; Brindley, P. Let nature be thy medicine: A socioecological exploration of green prescribing in the UK. Int. J. Environ. Res. Public Health 2020, 17, 3460. [Google Scholar] [CrossRef]
- Romito, F.; Goldzweig, G.; Cormio, C.; Hagedoorn, M.; Andersen, B.L. Informal caregiving for cancer patients. Cancer 2013, 119, 2160–2169. [Google Scholar] [CrossRef] [Green Version]
- Lambert, S.D.; Ould Brahim, L.; Morrison, M.; Girgis, A.; Yaffe, M.; Belzile, E.; Clayberg, K.; Robinson, J.; Thorne, S.; Bottorff, J.L.; et al. Priorities for caregiver research in cancer care: An international Delphi survey of caregivers, clinicians, managers, and researchers. Supportive Care Cancer 2019, 27, 805–817. [Google Scholar] [CrossRef]
- Lambert, S.D.; Girgis, A. Unmet supportive care needs among informal caregivers of patients with cancer: Opportunities and challenges in informing the development of interventions. Asia-Pac. J. Oncol. Nurs. 2017, 4, 136–139. [Google Scholar] [CrossRef]
- Kent, E.E.; Rowland, J.H.; Northouse, L.; Litzelman, K.; Chou, W.Y.; Shelburne, N.; Timura, C.; O’Mara, A.; Huss, K. Caring for caregivers and patients: Research and clinical priorities for informal cancer caregiving. Cancer 2016, 122, 1987–1995. [Google Scholar] [CrossRef]
- Ferrell, B.R.; Kravitz, K.; Borneman, T.; Friedmann, E.T. Family caregivers: A qualitative study to better understand the quality-of-life concerns and needs of this population. Clin. J. Oncol. Nurs. 2018, 22, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Northouse, L.L.; Katapodi, M.C.; Song, L.; Zhang, L.; Mood, D.W. Interventions with family caregivers of cancer patients: Meta-analysis of randomized trials. CA A Cancer J. Clin. 2010, 60, 317–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AARP; National Alliance for Caregiving. Caregiving in the U.S. 2020; AARP: Washington, DC, USA; National Alliance for Caregiving: Washington, DC, USA, 2020. [Google Scholar]
- Wyatt, G.; Lehto, R.H.; Sender, J. The prevalence and types of complementary and integrative health therapies used by caregivers of patients with cancer. Semin. Oncol. Nurs. 2019, 35, 342–347. [Google Scholar] [CrossRef] [PubMed]
- Thana, K.; Lehto, R.; Sikorskii, A.; Wyatt, G. Informal caregiver burden for solid tumor cancer patients: A review and future directions. Psychol. Health 2021, 1–23. [Google Scholar] [CrossRef]
- Frambes, D.; Given, B.; Lehto, R.; Wyatt, G.; Sikorskii, A. Informal caregivers of cancer patients: Review of interventions, care activities, and outcomes. West. J. Nurs. Res. 2018, 40, 1069–1097. [Google Scholar] [CrossRef]
- Brant, J.M.; Silbermann, M. Global perspective on palliative care for cancer patients: Not all countries are the same. Curr. Oncol. Rep. 2021, 23, 60. [Google Scholar] [CrossRef]
- Barton, J.; Pretty, J. What is the best dose of nature and green exercise for improving mental health? A multi-study analysis. Environ. Sci. Technol. 2010, 44, 3947–3955. [Google Scholar] [CrossRef]
- Northouse, L.L. Helping patients and their family caregivers cope with cancer. Oncol. Nurs. Forum 2012, 39, 500–506. [Google Scholar] [CrossRef]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Kaplan, S. Meditation, restoration, and the management of mental fatigue. Environ. Behav. 2001, 33, 480–506. [Google Scholar] [CrossRef] [Green Version]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Berto, R. The role of nature in coping with psycho-physiological stress: A literature review on restorativeness. Behav. Sci. 2014, 4, 394–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thana, K.; Sikorskii, A.; Lehto, R.; Given, C.; Wyatt, G. Burden and psychological symptoms among caregivers of patients with solid tumor cancers. Eur. J. Oncol. Nurs. 2021, 52, 101979. [Google Scholar] [CrossRef]
- O’Brien, L.; Morris, J.; Stewart, A. Engaging with peri-urban woodlands in England: The contribution to people’s health and well-being and implications for future management. Int. J. Environ. Res. Public Health 2014, 11, 6171–6192. [Google Scholar] [CrossRef] [Green Version]
- Britton, E.; Kindermann, G.; Domegan, C.; Carlin, C. Blue care: A systematic review of blue space interventions for health and wellbeing. Health Promot. Int. 2020, 35, 50–69. [Google Scholar] [CrossRef] [Green Version]
- Kondo, M.C.; Fluehr, J.M.; McKeon, T.; Branas, C.C. Urban green space and its impact on human health. Int. J. Environ. Res. Public Health 2018, 15, 445. [Google Scholar] [CrossRef] [Green Version]
- Valtchanov, D.; Ellard, C.G. Cognitive and affective responses to natural scenes: Effects of low-level visual properties on preference, cognitive load and eye-movements. J. Environ. Psychol. 2015, 43, 184–195. [Google Scholar] [CrossRef]
- Cutillo, A.; Rathore, N.; Reynolds, N.; Hilliard, L.; Haines, H.; Whelan, K.; Madan-Swain, A. A literature review of nature-based therapy and its application in cancer care. J. Ther. Hortic. 2015, 25, 3–15. [Google Scholar]
- Fried, G.; Wichrowski, M. Horticulture therapy: A psychosocial treatment option at the Stephen D. Hassenfeld Children’s Center for Cancer and Blood Disorders. Prim. Psychiatry 2008, 15, 73–77. [Google Scholar]
- Taft, S.B. Therapeutic horticulture for people living with cancer: The Healing Gardens program at Lifeline in Seattle. J. Ther. Hortic. 2004, 15, 16. [Google Scholar]
- Adevi, A.A.; Lieberg, M. Stress rehabilitation through garden therapy: A caregiver perspective on factors considered most essential to the recovery process. Urban For. Urban Green. 2012, 11, 51–58. [Google Scholar] [CrossRef]
- Gemmill, R.; Cooke, L.; Williams, A.C.; Grant, M. Informal caregivers of hematopoietic cell transplant patients: A review and recommendations for interventions and research. Cancer Nurs. 2011, 34, E13–E21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environ. Res. 2018, 166, 628–637. [Google Scholar] [CrossRef]
- Shuda, Q.; Bougoulias, M.E.; Kass, R. Effect of nature exposure on perceived and physiologic stress: A systematic review. Complementary Ther. Med. 2020, 53, 102514. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Lavin, J.; Lavin, C.; Bai, X.; Mastropaolo, S.; Feldman, D. Determining the effect of group flower arranging sessions on caregiver self-efficacy stress levels in an in-patient hospice. OMEGA-J. Death Dying 2020, 30222819900441. [Google Scholar] [CrossRef] [PubMed]
- McCullough, A.; Ruehrdanz, A.; Jenkins, M.A.; Gilmer, M.J.; Olson, J.; Pawar, A.; Holley, L.; Sierra-Rivera, S.; Linder, D.E.; Pichette, D.; et al. Measuring the effects of an animal-assisted intervention for pediatric oncology patuents and their parents: A multisite randomized controlled trial. J. Pediatric Oncol. Nurs. 2018, 35, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Carrion-Plazza, A.; Jaen, J.; Montoya-Castilla, I. HabitApp: New play technologies in pediatric cancer to improve the psychosocial state of patients and caregivers. Front. Psychol. 2020, 11, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, K. The Impact of Complementary Therapies on Cancer Patient Caregivers’ Quality of Life. Ph.D. Thesis, California State University, Long Beach, CA, USA, 2016. [Google Scholar]
- Sun, V.; Raz, D.J.; Kim, J.Y.; Melstrom, L.; Hite, S.; Varatkar, G.; Fong, Y. Barriers and facilitators of adherence to a perioperative physical activity intervention for older adults with cancer and their family caregivers. J. Geriatr. Oncol. 2019, 11, 256–262. [Google Scholar] [CrossRef] [Green Version]
- White, M.P.; Yeo, N.L.; Vassiljev, P.; Lundstedt, R.; Wallergård, M.; Albin, M.; Lõhmus, M. A prescription for “nature”—the potential of using virtual nature in therapeutics. Neuropsychiatr. Dis. Treat. 2018, 14, 3001–3013. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Publications | Sample (Age, Sex, Race, Any Co-Morbid Conditions If Mentioned) | Design (Type of Study) | Type of Intervention | Patient Cancer Diagnosis | Measures Used | Study Outcomes |
|---|---|---|---|---|---|---|
| Carrion-Plaza, et al. (2020). HabitApp: New play technologies in pediatric cancer to improve the psychosocial state of patients and caregivers | 39 Spanish pediatric oncology patients and 39 caregivers (61% female, n = 24); age range 30–64 years. | Controlled mixed methods pre-post study consisting of 30-minute sessions with pre, during (10 min, 20 min), and post evaluations. Qualitative data were collected during the observation period. | Evaluate use of the HabitApp technological play therapy, a mobile application that permits the observation of animals in their personal habitats from around the world using remote video cameras. | Patients were hematology-oncology patients undergoing cancer treatments—bone marrow transplantation (not at terminal phase). | Observational ad hoc measurement scale (affection, nervousness, proximity to child, reactions, interest, satisfaction) 0–3 ratings; state-trait anxiety inventory; somatic complaints list; positive and Negative experience scale; Mood scale (fear, sadness, happiness, anger); State-Trait Depression Inventory. | Caregivers demonstrated significant improvements in psychosocial factors of affection, proximity, interest, and satisfaction. There were smiling faces and laughter, relaxed conversation, and storytelling between patients and their caregivers. |
| Lavin, et al. (2020). Determining the effect of group flower arranging sessions on caregiver self-efficacy and stress levels in an in-patient hospice | n = 71 family caregivers of patients in patient end of life care. (n = 38; 54.3%) were 51 to 76 years old. Majority of the participants (n = 65; 92.9%) were females and (n = 5, 7.1%) were males. Participants self-identified as Hispanic (n = 33, 41.7%), Caucasian (n = 22, 31.4%),African American (n = 14, 20%), and Asian (n = 1, 1.4%). | Mixed methods pre-post design. | Participation in a ‘flowers for healing’ class that taught participants how to arrange flowers. Participants shared their flower arrangement with the patient they cared for. | Terminally ill hospice patients. Type of diagnosis not described although cancer caregiving is alluded to in the literature review. | The revised scale for Caregiving self-efficacy; Likert scale (0–5) used to evaluate stress level, sleep, appetite and eating habits, mood, memory, and sense of wellbeing. Participant satisfaction open-ended comments for future changes and recommendations. | n = 55 caregivers did not complete the self-efficacy post-test due to needing to get back to the patient. However, stress levels were significantly decreased in the overall sample. Of those who completed self-efficacy pre- and post-intervention (n = 17), there was significant improvement in scores. Qualitative data indicated very positive experience (n = 57 reported positive emotions such as relaxation, calming, healing); n = 16 identified less worry, reflection; positive sensory experience identified by n = 7. |
| McCullough, t al. (2018). Measuring the effects of an animal-assisted intervention for pediatric oncology patients and their parents: a multisite randomized controlled trial | 106 primary parent caregivers (n = 60 in intervention group, n = 46 in control condition). 92.5% (n = 98) primary caregivers were mothers; most of sample ranged between 26–45 years (80%). 67% (n = 71) Caucasian; 8% (n = 8) African-American; 14% (n = 15) Hispanic; 6% (n = 6) Other; 6% (n = 6) not reported. | Parallel group randomized trial. | Evaluated the effects of an animal-assisted intervention on stress, anxiety, and health-related quality of life in children with cancer and their parents in five U.S. pediatric hospital sites. Intervention occurred in cancer outpatient setting once per week over 4 months approximately depending on cancer treatment schedules. Sessions average 24 min in length. | Children (n = 106) were 3–17 years with newly diagnosed cancers (previous 6 weeks); Cancers included lymphomas (n = 13, 12%); osteosarcoma (n = 6, 6%); Wilms’ tumor 8% (n = 8) neuroblastoma (n = 2, 2%); sarcomas (n = 7, 7%); other (n = 15, 14%). | Pediatric Inventory for Parents used to measure stress; 2 items including 4 subscales: communication; emotional functioning, role functioning, medical care. State-Trait Anxiety Inventory (2 20-item scales). | Parents in the intervention group had significant reduction in overall parenting stress post-intervention as compared to the control group (p = 0.008). Parents in the intervention group had significant reductions in stressful communications over time (p = 0.004), frequency of stressful events related to medical care (p = .023), and reduced emotional distress (p = 0.002). There were no significant differences in state or trait anxiety pre-post intervention between the groups with increased state anxiety noted in both groups (p < 0.001). |
| Sun, et al. (2020). Barriers and facilitators of adherence to a perioperative physical activity intervention for older adults with cancer and their family caregivers | 34 patient-caregiver dyads. Caregivers were 59% female; 82% Caucasian, and 53% were employed. | Qualitative study of the barriers and facilitators to the walking intervention. The caregivers were trained to serve as the patients coach and participated in walking with their patient during the intervention time period. | Evaluation of barriers and facilitators to a physical activity intervention. The peri-operative physical activity intervention was aimed at building the patients physical and psychological function pre-surgery. The dyadic sessions consisted of one-on-one coaching via 5 videoconference and telephone sessions that were delivered pre-surgery, during hospitalization, and 2–4 weeks following surgery. | Lung (n = 18; mean age 74 years) and gastrointestinal (n = 16; mean age 71 years) cancers. | Data were derived from the physical therapy/occupational therapy notes that were taken during baseline, session 1 before surgery, and inpatient encounter post-surgery. | Family caregivers noted barriers were: co-morbid conditions (pain, arthritis), allergies and sensitivities to walking outdoors, family obligations and work responsibilities, MD appointments, busy schedule, weather, and uneven walking surfaces. Facilitators to outdoor activity included patient wanting to hike in mountains twice weekly; encouragement from patient and benefit such as reduced anxiety. |
| Turner (2016). The impact of complementary therapies on cancer patient caregivers’ quality of life | Data were evaluated on 120 users of therapies and 120 non-user cancer caregivers from a large cancer center. Complementary therapy users were primarily female (68%), Caucasian (82%), college educated (64%), and living with a partner (71%). | Secondary analysis of cross-sectional data that compared quality of life data between cancer caregivers who did vs. those who did not participate in cancer center complementary therapies program. | Complementary therapy classes offered to the cancer patients and their caregivers were divided into healing (art, gardening, movement, music, photography, and writing) and fitness (aquatic therapy, cycling, pilates, strength and fitness, walking, and yoga). | Cancer patients at large cancer center. | 51-item quality of life survey (36 quality of life questions; 15 demographic items) with a single open-ended question about the impact of complementary therapies. User data from records about complementary therapy usage. | Complementary therapy uses reported significantly better scores on relationship with others, mental functioning, emotional state, and attitude toward life as compared to non-complementary therapy users. 40% of the use (highest reported along with arts program) were hope blooms gardening. 20% of users also participated in walking and cycling. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lehto, R.H.; Wyatt, G.; Sender, J.; Miller, S.E. An Evaluation of Natural Environment Interventions for Informal Cancer Caregivers in the Community. Int. J. Environ. Res. Public Health 2021, 18, 11124. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111124
Lehto RH, Wyatt G, Sender J, Miller SE. An Evaluation of Natural Environment Interventions for Informal Cancer Caregivers in the Community. International Journal of Environmental Research and Public Health. 2021; 18(21):11124. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111124
Chicago/Turabian StyleLehto, Rebecca H., Gwen Wyatt, Jessica Sender, and Sara E. Miller. 2021. "An Evaluation of Natural Environment Interventions for Informal Cancer Caregivers in the Community" International Journal of Environmental Research and Public Health 18, no. 21: 11124. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111124