
Access to Assistive Technology during the COVID-19 Global Pandemic: Voices of Users and Families

 , , ,
, , ,
Abstract
:1. Introduction
- What are the experiences of AT users during the COVID-19 pandemic in relation to AT access and service delivery?
- What are the implications of the COVID-19 pandemic for AT systems strengthening?
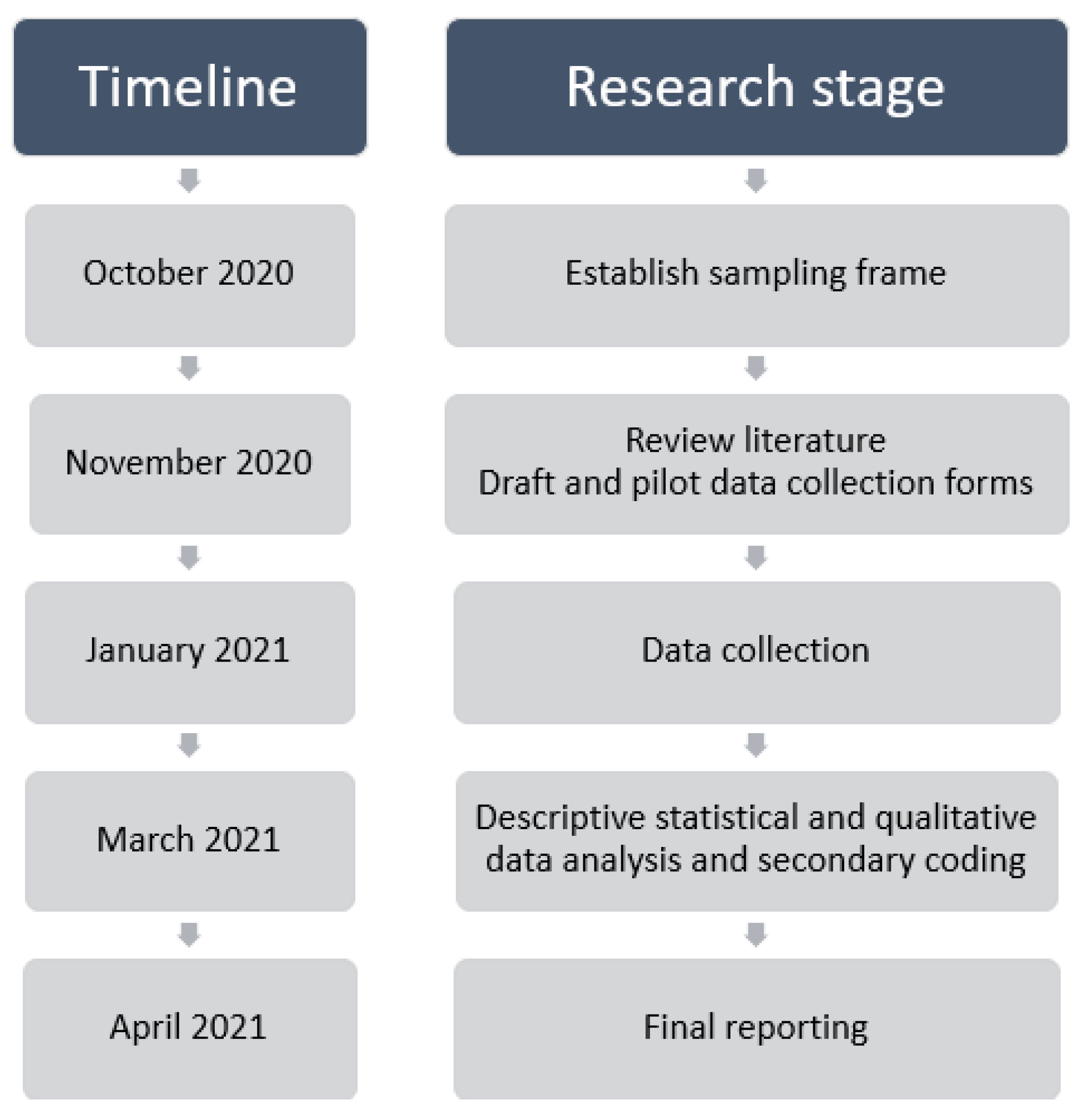
2. Methods
2.1. Research Design
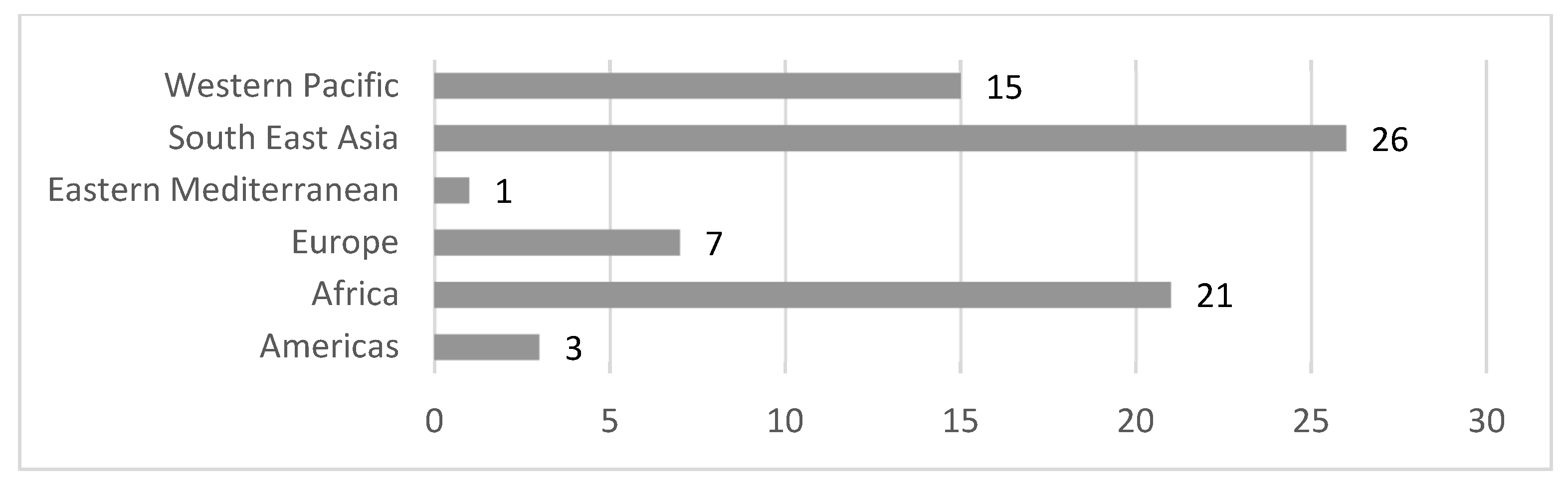
2.2. Sample
2.3. Data Collection
2.4. Data Analysis
2.4.1. Managing the Data
2.4.2. Approach to Analysis
2.4.3. Analysis Process
3. Results
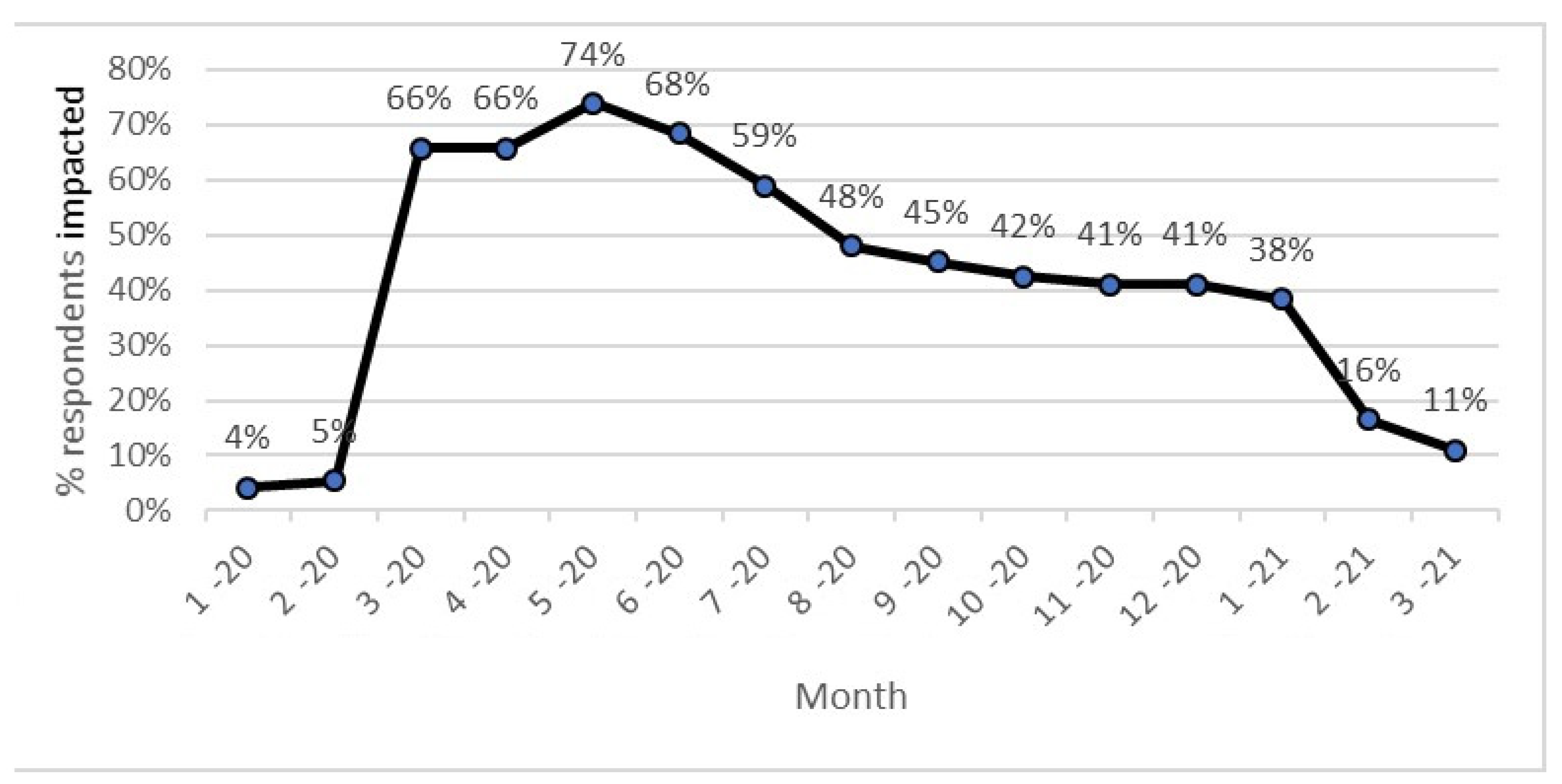
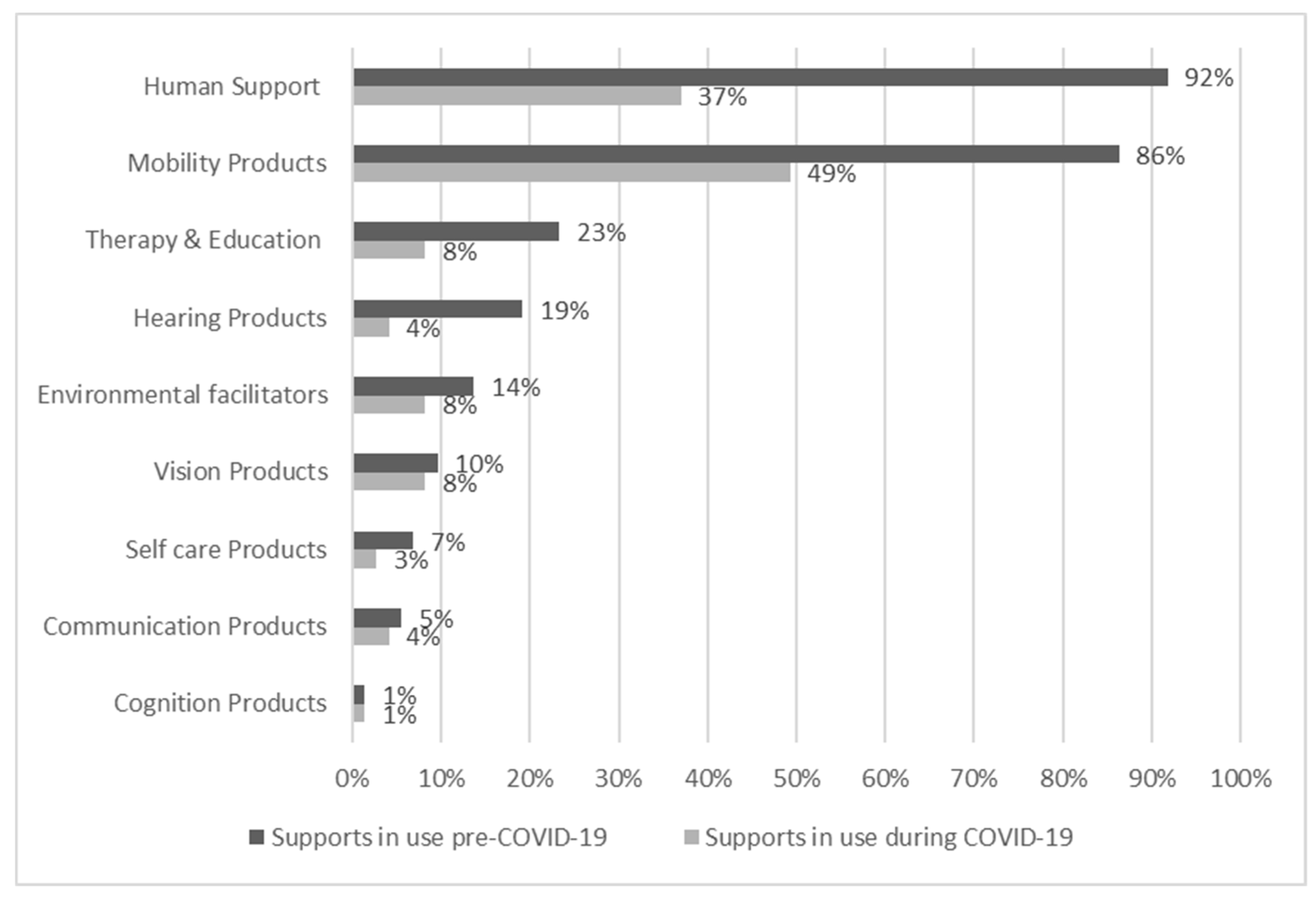
3.1. Descriptive Statistics
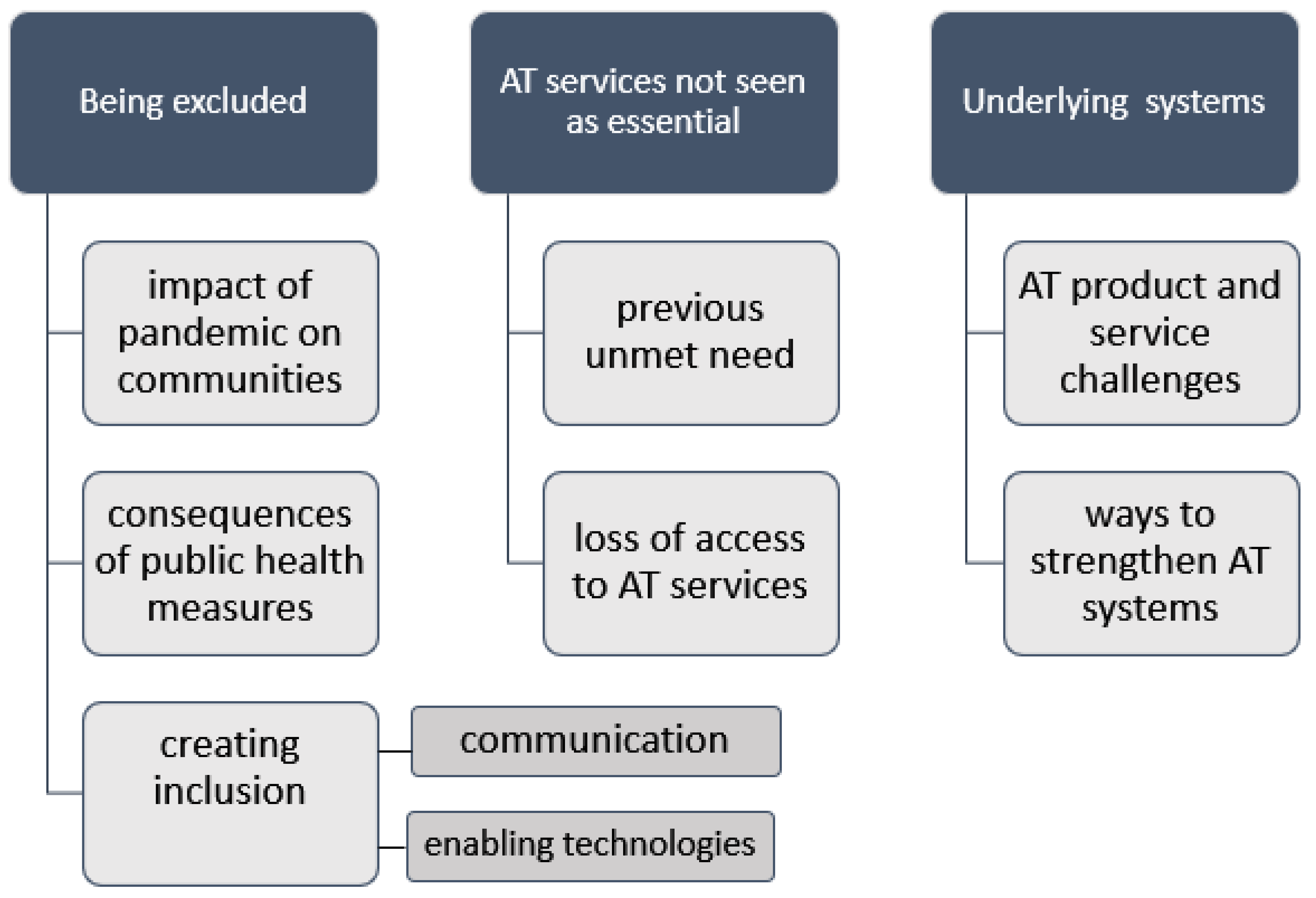
3.2. Qualitative Results
3.2.1. Being Excluded
Due to COVID-19, the close down of therapy service physically, (his) condition deteriorated. (SU51, Bangladesh)
Field worker could no longer hold and play with me. (SU40, Cameroon)
‘The community has the fear of assisting those in need for fear of getting infected with COVID-19.’ (SU19, Kenya)
‘There’s a bit of mistrust in the community because everyone was afraid.’ (SU50, Benin)
We decided to move to the farms where we did all the activities there and we came back at the evening, we had to lock L and her young sister inside because we couldn’t bring them there. (SU45, Tanzania)
‘lack of political will to be disability inclusive in their COVID-19 program.’ (SU52, Malawi)
There were not much activity in the communities or in the village that included person with disability. (SU62, Fiji)
The community stopped including me or I feel left out when they don’t understand the impact of the pandemic towards hard of hearing person. Like the use of pen and paper. They are lazy to write and never understand that pen and paper is my way of communication. (SU57, Philippines)
Even during times when restrictions had eased for the wider community, I still felt excluded as I had to follow strict policies because of my disability and the Government rules about group living. (SU66, Australia)
Due to social distancing, (he) couldn’t play outside. The situation affected (his) mental health. (SU53, Bangladesh)
I need someone to hold me when I stand. This made me not able to be supported by someone when I stand up due to social distancing. My helper couldn’t come close to me. (SU52, Malawi)
[Self isolation had a] clear impact on my quality of life-I had a letter from the Government to self isolate and am trying to follow this-but it is hard to be positive especially in the last 2 months! I have not been out of the house for a year now! (SU13, UK)
Sometimes, I miss my friends from another village and even from the same village. As I am mostly 90 years old, my daughter doesn’t want me to go outside during COVID-19 to protect me from the virus. (SU42, Myanmar)
The hardest thing for E was to (not) go to class because he likes to socialize with other children, but as a measure of the family we decided not to send them to their classes anymore. (SU46, Nicaragua)
The game center where he met many friends was closed down, resulting in him being left alone most of the times. (SU68, Zimbabwe)
We have strict guidance so this framed my daily life choices. (SU06, UK)
In COVID time fear is in every person or in society. Lockdown imposed and police not allowed anyone to go out for anything. No one supported us because we are living in remote area in small village. (SU14, India)
…it was locked down family that lost employment to support person with disabilities-had issues in buying diapers, etc. (SU62, Fiji)
Q could not go to the provincial hospital or annual health check and getting new arm brace during COVID-19. (SU72, Vietnam)
There were many restrictions in the area (travel, transportation, crowd gathering, etc.). This has caused the centre that the child is attending to have closed… socio-educational support is made difficult by the absence of a sign language facilitator, because the little girl does not use articulated language. (SU36, Benin)
During isolation at home my father and brother spent more time with me. (SU40, Cameroon)
His parents stayed at home and spent more time to teach (him). (SU71, Vietnam)
People with disabilities were not a high priority to get PPE, or even considered, sometimes. (SU61, Australia)
Yes like mask, soap and sanitizer, but we could not managed to afford because of poor economic status. (SU45, Tanzania)
The social distancing impacted my services negatively. When I communicated with people wearing masks, I had to lean closer to the people to hear and understand what they were saying. In a normal scenario, I would lip-read and communicate. In addition, I had to deal with background noise. However, if I stood close enough, I would be able to understand the other person, despite the mask. Considering the COVID-19 guidelines (social distancing), this is probably a Catch-22 situation. (SU12, India)
Masks made it difficult for me to lip read as people wore masks over their mouth, and I sometimes had to request them to remove their masks while maintaining social distancing which often wasn’t comfortable. (SU10, India)
Masks has been helpful. However, it causes communication barrier. If only transparent facemasks are allowed to be worn. (SU57, Philippines)
Good neighbors and family love sharing our resources together. (SU34, Cameroon)
Psycho-social support of volunteers. (SU05, Ukraine)
Family solidarity…Disabilities Organizations in Rwanda keep me inform(ed) and involve me in helping others. (SU26, Rwanda)
We have supported our neighbors in this COVID time because we are living in remote area in small village. One time we have received food from local government officials. (SU24, India)
Because everyone is feeling socially isolated now (not just me), they are moving to this. So the burden of dealing with social isolation doesn’t fall just on me, as its more equal, the burden is shared, and I don’t just feel its me and my needs making this happen. (SU61, Australia)
There are some times when the people from health… come to ask for persons with disabilities for inclusion on some COVID relief programs. (SU68, Zimbabwe)
He had unmet need for a hearing device pre COVID. This was provided thanks to an inclusive COVID-19 response program and will transform his difficulties hearing and communicating during his social activities. However, due to COVID-19, social activities have been abolished and Mbah W feels unsafe going outside. (SU16, Indonesia)
Health and support systems should have a preparedness plan that gives a special focus to poor families with a member(s) with disabilities prior to incidents such as COVID-19… When there is no such plans, in times like these when we compete for limited resources, our type of families are easily forgotten in everything. (SU44, Tanzania)
Consultation with disability sector planning and ways forwards so when it done it’s done for all. (SU62, Fiji)
I feel included in social activities that are now available to me online and can be viewed flexibly when I’m awake, instead of at set times when I am too tired. (SU61, Australia)
I love to play table tennis and enjoy life to the fullest (now) participation has become all online activities. (SU23, India)
All the services that were meaningful to me were all closed. However, my exercise physiologist and my drama group started to offer video link appointments or group activities. I did not have the technology or internet to access these, and I needed help to learn how to use this… I was still able to participate in my drama group sessions with my classmates, friends and trainers through a virtual environment. It is undoubtedly true that this iPad and internet connection, has become an important part of my daily activities since the beginning of the pandemic. I believe having a stable and economical internet plan is essential for me to fully participate in meaningful activities and essential services. (SU66, Australia)
The self-isolation impacted me positively because I could explore calls via Zoom and Teams. Using Teams, Zoom, and headphones enables me to focus more on my speech, and understand people clearly. Online calls have actually proved to be an advantage because I must rely on just one sense-hearing. This has made me more sensitive and empathetic to others’ voices, honing my abilities along the way. (SU13, UK)
This hit me hard because I’m a people person. I love people. For instance, one of the girls in the service is in a home, and I ring her once a week: because it helps her and it helps me. I feel better after talking to her on the phone. (SU55, Ireland)
(She) was not able to use computer at home, (had) untrained caregivers …had a lot of communication problem because of the absence of special communication board. (SU60, Tanzania)
Q and her family members stayed at home during the social distancing period. She studied online from home. Her school updated lessons to students via parents mobile phone. (SU72, Vietnam)
Occupational therapy student input was all online, and the students did lots of work identifying options for streaming for interests. I was also able to access a live Facebook stream of puppy raising … Technology reliant on internet connection was an issue as I am on a low income and could not afford a high data plan. (SU65, Australia)
During COVID I reduced my participation in [classroom competitions] as it becomes a bit difficult to communicate effectively over a call as compared to communication in person.... Access to good internet service helped, also, I am a persistent person, I don’t give up easily. (SU10, India)
I have tried to keep my Muslim Group going as many really wanted support. Possibly no one really thought how much we rely on AT until we have these restrictions—it certainly made me think once my hearing started to deteriorate; I just need to be patient to get the new equipment. With hearing aids and the hearing clinic I can run my home, engage in discussions and online meetings with my hearing aids-otherwise I would not be able to be active. (SU06, UK)
Last March, I felt isolated but soon after we had the virtual service running so it wasn’t that bad, but it took a lot of figuring out, together: staff and service owners worked on this together. (SU55, Ireland)
3.2.2. AT Services Not Seen as Essential
(COVID-19 related restrictions have) influenced my life. First by taking the others away from me a little, then the closure of the border…destroyed my mother’s small trade that allowed her to take care of my basic needs. (SU50, Benin)
…we were hearing from the radio, that we were advised to wash our hands with running water and for us we couldn’t able to manage it because we don’t have a source of water and for our neighbors that had water they were not allowing us to fetch it because they were afraid of contacting the disease. (SU45, Tanzania)
Daily life is very stressful (she) can no longer creep on the floor for fear of touching the virus. (she) need(s) a wheelchair or [crutches] that can keep (her) from the floor. (She) can no longer play with friends at school. No more visits to the physiotherapist. We needed mask and hand sanitizers. (she) was afraid going out. We are afraid of visiting the hospital. (SU34, Cameroon)
This really affected G and our life in the way that we could not receive the services that we wanted. We wanted wheelchair but up to now we have not received, we wanted repair/maintenance of CP Chair but we did not receive timely service. G needs regular medication in the hospital but we received so little attention from health staff from April-July 2020. We also restricted our movements to hospitals in fear of COVID-19. (SU39, Tanzania)
My daily life is so complicated because the facilities I use are not friendly e.g., normal books with small font size, untrained personnel and un recommended baby walker for mobility purposes. (SU60, Tanzania)
I couldn’t able to go for hearing aid repair = I couldn’t able to hear (so) Since I couldn’t able to hear family and myself struggle in communicating day-to-day activities. I have to manage on physical prompting which takes very long time to understand. (SU43, India)
3.2.3. Underlying Systems
Income generation support to parents, repair of hearing aid. Accessibility of assistive devices, transportation, livelihood support. (SU43, India)
Improve accessibility and affordability of medical health and services, including the assistive products and especially for the older persons with disabilities. (SU19, Kenya)
4. Discussion
4.1. People
4.2. Policy
4.3. Products
4.4. Personnel
4.5. Provision
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Rapid Evidence Review
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| About Me | |
|---|---|
| My name and the place I live: | Free text responses |
| If you choose, tell us about you and your life | |
| Life before COVID-19 | |
| List the assistive products and services that you used before COVID-19 | |
| Before COVID-19, were there other supports that you needed that you didn’t have? | |
| Before COVID-19, did you have any difficulty accessing assistive products and services? | |
| The next questions are about your participation before COVID-19 Before COVID-19, did you: | |
| Take care of yourself? | |
| Do tasks at home, for yourself and others? | |
| Participate in other activities (Examples: work, study, fun, community) | |
| Access assistive technology services (Examples: Assessment, maintenance, repairs, training) | |
| Life now, during COVID-19 | |
| What months did COVID-19 impact your access to services? Tick all that apply | |
| 2020 January; February; March; April; May; June; July; August; September; October; November; December 2021 January; February; March | |
| List the assistive products and services that you used now, during COVID-19 Examples: Individual supports (e.g., assistive products or home adaptations): Support people (e.g., caregivers, family, paid helpers): Societal supports (e.g., accessible transport) | |
| What is your daily life like with these supports? | |
| Do you need any other supports to live your daily life | |
| Are there any barriers to accessing assistive products and services? | |
| During COVID-19, what is different about how you: | |
| Take care of yourself | |
| Do tasks at home, for yourself and others? | |
| Participate in other activities (Examples: work, study, fun, community) | |
| Access assistive technology services (Examples: Assessment, maintenance, repairs, training) | |
| What do you think most impacted your services? (either in a good or bad way) | |
| Social distancing | |
| Self-isolation | |
| The region where I live was locked down | |
| The services I use were closed | |
| I was at risk of contracting COVID-19 | |
| Important people around me were contracting COVID-19 | |
| There was a need for new equipment to be safe, like masks | |
| I didn’t feel safe going outside | |
| My community stopped including me | |
| Fear of being denied access to services | |
| Fear my products might be taken away for use by others (for example, a ventilator or other respiratory device) | |
| Lack of information about COVID | |
| Lack of information about changes in how assistive products and services can be accessed | |
| Fear of creating a burden on the system | |
| Inability to travel to the place providing products and services | |
| Other | |
| Addressing the challenges | |
| What qualities/attributes about you and your family, have helped you manage the impacts of COVID-19? | |
| What have other organisations done that has helped you throughout this time? Example: civil society organisations, government? | |
| What do you think could have been helpful, but was not done? | |
| How could our health and support systems be better prepared in the future? | |
References
- de Witte, L.; Steel, E.; Gupta, S.; Ramos, V.D.; Roentgen, U. Assistive technology provision: Towards an international framework for assuring availability and accessibility of affordable high-quality assistive technology. Disabil. Rehabil. Assist. Technol. 2018, 13, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Tebbutt, E.; Brodmann, R.; Borg, J.; MacLachlan, M.; Khasnabis, C.; Horvath, R.E. Assistive products and the Sustainable Development Goals (SDGs). Glob. Health 2016, 12, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, J.; Lindström, A.; Larsson, S. Assistive technology in developing countries: A review from the perspective of the Convention on the Rights of Persons with Disabilities. Prosthet. Orthot. Int. 2011, 35, 20–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khasnabis, C.; Mirza, Z.; MacLachlan, M. Opening the GATE to inclusion for people with disabilities. Lancet 2015, 386, 2229–2230. [Google Scholar] [CrossRef]
- Groce, N.; Kett, M.; Lang, R.; Trani, J.-F. Disability and Poverty: The need for a more nuanced understanding of implications for development policy and practice. Third World Q. 2011, 32, 1493–1513. [Google Scholar] [CrossRef]
- Emerson, E.; Madden, R.; Graham, H.; Llewellyn, G.; Hatton, C.; Robertson, J. The health of disabled people and the social determinants of health. Public Health 2011, 125, 145–147. [Google Scholar] [CrossRef] [PubMed]
- Layton, N.; Bell, D.; Borg, J.; Steel, E.; Maclachlan, M.; Tebbutt, E.; Khasnabis, C.; Swaminathan, S. Assistive technology as a pillar of universal health coverage: Qualitative analysis of stakeholder responses to the world health assembly resolution on assistive technology. Disabil. Rehabil. Assist. Technol. 2020, 15, 825–831. [Google Scholar] [CrossRef]
- Austin, V.; Holloway, C.; Ossul Vermehren, I.; Dumbuya, A.; Barbareschi, G.; Walker, J. “Give Us the Chance to Be Part of You, We Want Our Voices to Be Heard”: Assistive Technology as a Mediator of Participation in (Formal and Informal) Citizenship Activities for Persons with Disabilities Who Are Slum Dwellers in Freetown, Sierra Leone. Int. J. Environ. Res. Public Health 2021, 18, 5547. [Google Scholar] [CrossRef]
- Graham, L.; Moodley, J.; Selipsky, L. The disability–poverty nexus and the case for a capabilities approach: Evidence from Johannesburg, South Africa. Disabil. Soc. 2013, 28, 324–337. [Google Scholar] [CrossRef]
- Verduzco-Gutierrez, M.; Lara, A.M.; Annaswamy, T.M. When Disparities and Disabilities Collide: Inequities during the COVID-19 Pandemic. PM&R 2021, 13, 412–414. [Google Scholar]
- Andrews, E.E.; Ayers, K.B.; Brown, K.S.; Dunn, D.S.; Pilarski, C.R. No body is expendable: Medical rationing and disability justice during the COVID-19 pandemic. Am. Psychol. 2021, 76, 451–461. [Google Scholar] [CrossRef]
- WHO. Policy Brief: Access to Assistive Technology; World Health Organisation: Geneva, Switzerland, 2020; Available online: https://www.who.int/phi/implementation/assistive_technology/phi_gate/en/ (accessed on 22 August 2021).
- Scherer, M.J. It is time for the biopsychosocialtech model. Disabil. Rehabil. Assist. Technol. 2020, 15, 363–364. [Google Scholar] [CrossRef] [PubMed]
- MacLachlan, M.; McVeigh, J.; Cooke, M.; Ferri, D.; Holloway, C.; Austin, V.; Javadi, D. Intersections Between Systems Thinking and Market Shaping for Assistive Technology: The SMART (Systems-Market for Assistive and Related Technologies) Thinking Matrix. Int. J. Environ. Res. Public Health 2018, 15, 2627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Assembly (Ed.) Resolution on Improving Access to Assistive Technology. In A71/21; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Desmond, D.; Layton, N.; Bentley, J.; Boot, F.H.; Borg, J.; Dhungana, B.M.; Gallagher, P.; Gitlow, L.; Gowran, R.J.; Groce, N.; et al. Assistive technology and people: A position paper from the first global research, innovation and education on assistive technology (GREAT) summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 437–444. [Google Scholar] [CrossRef] [Green Version]
- Smith, R.O.; Scherer, M.; Cooper, R.; Bell, D.; Hobbs, D.A.; Pettersson, C.; Seymour, N.; Borg, J.; Johnson, M.J.; Lane, J.P.; et al. Assistive technology products: A position paper from the first global research, innovation, and education on assistive technology (GREAT) summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 473–485. [Google Scholar] [CrossRef] [Green Version]
- Smith, E.M.; Gowran, R.J.; Mannan, H.; Donnelly, B.; Alvarez, L.; Bell, D.; Contepomi, S.; Ennion, L.; Hoogerwerf, E.J.; Howe, T.; et al. Enabling appropriate personnel skill-mix for progressive realization of equitable access to assistive technology. Disabil. Rehabil. Assist. Technol. 2018, 13, 445–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLachlan, M.; Banes, D.; Bell, D.; Borg, J.; Donnelly, B.; Fembek, M.; Ghosh, R.; Gowran, R.; Hannay, E.; Hiscock, D.; et al. Assistive technology policy: A position paper from the first global research, innovation, and education on assistive technology (GREAT) summit. Disabil. Rehabil. Assist. Technol. 2018, 13, 454–466. [Google Scholar] [CrossRef] [Green Version]
- Layton, N.; Borg, J. (Eds.) Global perspectives on assistive technology. In Proceedings of the GReAT Consultation, Geneva, Switzerland, 22–23 August 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Smith, E.; Rizzo Battistela, L.; Contepomi, S.; Gowran, R.; Kankipati, P.; Layton, N.; MacDonald, R.; Nleya, C.; Delgado Ramos, V.; Rios Rincon, A.; et al. Measuring Met and Unmet Assistive Technology Needs at the National Level: Comparing National Database Collection Tools across Eight Case Countries. Available online: https://researchbank.swinburne.edu.au/items/9cc4fe9f-1282-4c17-9c39-0bfe32d8ce89/1/ (accessed on 22 August 2021).
- World Health Organisation. Coronavirus Disease (COVID-19) Pandemic 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 22 August 2021).
- Armitage, R.; Nellums, L.B. The COVID-19 response must be disability inclusive. Lancet Public Health 2020, 5, e257. [Google Scholar] [CrossRef] [Green Version]
- Humanity and Inclusion. Needs Assessment Impact of COVID-19 on People with Disabilities and their Families in Jordan. April 2020. Humanity & Inclusion. Available online: https://data2.unhcr.org/en/documents/details/75872 (accessed on 22 August 2021).
- Lazarus, K.U.; Oluwole, D.A. Demographic factors, attitude and knowledge of persons with special needs towards COVID-19 in Nigeria: Implications for counselling and social policy. Emerald Open Res. 2020, 2, 55. [Google Scholar] [CrossRef]
- Pettinicchio, D.; Maroto, M.; Chai, L.; Lukk, M. Findings from an online survey on the mental health effects of COVID-19 on Canadians with disabilities and chronic health conditions. Disabil. Health J. 2021, 14, 101085. [Google Scholar] [CrossRef]
- Qi, F.; Hu, L. Including people with disability in the COVID-19 outbreak emergency preparedness and response in China. Disabil. Soc. 2020, 35, 848–853. [Google Scholar] [CrossRef] [Green Version]
- Shakespeare, T.; Watson, N.; Brunner, R.; Cullingworth, J.; Hameed, S.; Scherer, N.; Pearson, C.; Reichenberger, V. Disabled People in Britain and the Impact of the COVID-19 Pandemic. Soc. Policy Adm. 2021, 1–15, epub ahead of print. [Google Scholar] [CrossRef]
- Siette, J.; Siette, J.; Dodds, L.; Seaman, K.; Wuthrich, V.; Johnco, C.; Earl, J.; Dawes, P.; Westbrook, J.I. The impact of COVID- 19 on the quality of life of older adults receiving community- based aged care. Aust. J. Ageing 2021, 40, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Faccioli, S.; Lombardi, F.; Bellini, P.; Costi, S.; Sassi, S.; Pesci, M.C.; Kazatchkine, M.; De Courcelles, S. How Did Italian Adolescents with Disability and Parents Deal with the COVID-19 Emergency? Int. J. Environ. Res. Public Health 2021, 18, 1687. [Google Scholar] [CrossRef] [PubMed]
- Stillman, M.D.; Capron, M.; Alexander, M.; Di Giusto, M.L.; Scivoletto, G. COVID-19 and spinal cord injury and disease: Results of an international survey. Spinal Cord Ser. Cases 2020, 6, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizzo, J.-R.; Beheshti, M. COVID-19 and Visual Disability: Can’t Look and Now Don’t Touch. PM&R 2021, 13, 415–421. [Google Scholar]
- Dianito, A.; Espinosa, J.; Duran, J.; Tus, J. A Glimpse into the Lived Experiences and Challenges Faced of PWD Students towards Online Learning in the Philippines Amidst COVID-19 Pandemic. Int. J. Adv. Res. Innov. Ideas Educ. 2021, 7, 1206–1230. [Google Scholar]
- Guptha, J.; Madaan, P.; Gulati, S. COVID-19: Implications for Children With Special Needs. J. ReAttach Ther. Dev. Divers. 2021, 3, 1–3. [Google Scholar] [CrossRef]
- Mont, D.; Layton, N.; Puli, L.; Gupta, S.; Manlappaz, A.; Shae, K.; Tebbutt, E.; Calvo, I. Assistive Technology and Support Services During the CovidCOVID-19 global pandemic: The Roles of Government and Civil Society in Fulfilling the Social Contract. Int. J. Environ. Res. Public Health. (under review).
- Puli, L.; Layton, N.; Mont, D.; Shae, K.; Calvo, I.; Hill, K.; Callaway, L.; Tebbutt, E.; Manlapaz, A.; Groenewegen, I.; et al. Assistive technology provider experiences during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10477. [Google Scholar] [CrossRef] [PubMed]
- Booth, A.; Hannes, K.; Harden, A.; Noyes, J.; Harris, J.; Tong, A. COREQ (Consolidated Criteria for Reporting Qualitative Studies), in Guidelines for Reporting Health Research: A User’s Manual; Moher, D., Altman, D., Schulz, K., Simera, I., Wager, E., Eds.; Wiley Blackwell: Oxford, UK, 2014; pp. 214–226. [Google Scholar]
- Braun, V.; Clarke, V.; Weate, P. Using Thematic Analysis in sport and Exercise Research. In Routledge Handbook of Qualitative Research in Sport and Exercise; Smith, B., Sparkes, A., Eds.; Routledge: London, UK, 2019; pp. 191–205. [Google Scholar]
- Braun, V.; Clarke, V.; Hayfield, N.; Terry, G. Thematic Analysis. In Handbook of Research Methods in Health Social Sciences; Liamputtong, P., Ed.; Springer Nature: Singapore, 2018; pp. 1–18. [Google Scholar]
- Krefting, L. Rigor in Qualitative Research: The Assessment of Trustworthiness. Am. J. Occup. Ther. 1991, 45, 214–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centre for Disease Control. Social Distancing. 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/social-distancing.html. (accessed on 22 August 2021).
- Lund, E.M.; Forber-Pratt, A.J.; Wilson, C.; Mona, L.R. The COVID-19 pandemic, stress, and trauma in the disability community: A call to action. Rehabil. Psychol. 2020, 65, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Anik, M.E.I.; Rahman, S.; Ataullah, A.H.M.; Rahman, M.M. Effect of Anxiety and Fear on Neurorehabilitation Services in COVID-19. SVOA Neurol. 2021, 2, 4–5. [Google Scholar]
- Kuper, H.; Banks, L.M.; Bright, T.; Davey, C.; Shakespeare, T. Disability-inclusive COVID-19 response: What it is, why it is important and what we can learn from the United Kingdom’s response. Wellcome Open Res. 2020, 5, 79. [Google Scholar] [CrossRef]
- Banks, L.M.; Davey, C.; Shakespeare, T.; Kuper, H. Disability-inclusive responses to COVID-19: Lessons learnt from research on social protection in low- and middle-income countries. World Dev. 2021, 137, 105178. [Google Scholar] [CrossRef] [PubMed]
- Smith, E.M.; Toro Hernandez, M.L.; Ebuenyi, I.D.; Syurina, E.V.; Barbareschi, G.; Best, K.L.; Danemayer, J.; Oldfrey, B.; Ibrahim, N.; Holloway, C.; et al. Assistive Technology Use and Provision During COVID-19: Results from a Rapid Global Survey. Int. J. Health Policy Manag. 2020, X, 1–10. [Google Scholar] [CrossRef]
- Smith, E.M.; MacLachlan, M.; Ebuenyi, I.D.; Holloway, C.; Austin, V. Developing inclusive and resilient systems: COVID-19 and assistive technology. Disabil. Soc. 2020, 36, 1–4. [Google Scholar] [CrossRef]
- Mintrom, M.; O’Connor, R. The importance of policy narrative: Effective government responses to COVID-19. Policy Des. Pract. 2020, 3, 205–227. [Google Scholar] [CrossRef]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Zhang, C.; Boyle, C.; Smith, M.; Phillips, J.P. Fair Allocation of Scarce Medical Resources in the Time of COVID-19. N. Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef] [PubMed]
- Surya, N.; Srivastava, A.; Nagda, T.; Palande, D.; Someshwar, H. Education, Training, and Practices of Neurorehabilitation in India During the COVID-19 Pandemic. Front. Neurol. 2021, 12, 626399. [Google Scholar] [CrossRef]
- Ramos Ataide, C.E.; Gonçalves Matos, A., Jr.; Araújo Dias, L.H.; Ferreira Farias, L.; Monteiro de Vasconcelos Filho, C.R.; Zanona, A. Occupational therapy productions in times of pandemic: A systematic review of occupational therapeutic actions against the new coronavirus (COVID-19) epidemic. Eur. PMC 2021, 10, 75. [Google Scholar]
- Piquet, V.; Luczak, C.; Seiler, F.; Monaury, J.; Martini, A.; Ward, A.B.; Bayle, N. Do Patients with COVID-19 Benefit from Rehabilitation? Functional outcomes of the first 100 patients in a COVID-19 rehabilitation unit. Arch. Phys. Med. Rehabil. 2021, 102, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Araten-Bergman, T.; Shpigelman, C.N. Staying connected during COVID-19: Family engagement with adults with developmental disabilities in supported accommodation. Res. Dev. Disabil. 2021, 108, 103812. [Google Scholar] [CrossRef] [PubMed]
- HelpAge International. Access to Age-Assistive Technology: A Resilience Building Measure for Older People; HelpAge International: Chiang Mai, Thailand, 2020. [Google Scholar]







| Negative Impacts |  | Aspect of Life during COVID-19 |  | Positive Impacts |
|---|---|---|---|---|
| Life During a Pandemic |
| ||
| Lockdown |
| ||
| Physical Distancing |
| ||
| Personal Protective Equipment |
| ||
| AT Users’ Perspectives on Public Health Messaging | Communication Principles for More Inclusive Public Health Messaging | |
|---|---|---|
| Difficulties | Solutions | |
| Timing and complexity: ‘There is a lot but it is changing quickly, so feel a bit confused at times’ (SU13, UK) I see the communication is so muddled and confusing-so needs to be clearer guidance. See the messaging needs to be clearer for us all and also to be able to share our concerns and give suggestions. (SU13, UK) Accessibility: (accessible (braille) materials are not available for reading on COVID) (SU54, India) …not in a format that can be used by all disabilities (SU52, Malawi) It wasn’t translated in my local language (SU70, Zimbabwe) AT service specific information: Lack of information about changes in how assistive products and services can be accessed (SU16, Indonesia) The support systems should inform us to stock up on hearing aid batteries, and in case of a faulty hearing aid, the support system should provide us with a contact number so that the hearing aid can be repaired or replaced (SU12, India) | Regular, prompt and local: Information received through daily media briefs by the Ministry of Health (SU19, Kenya) The village administrator explained deeply about COVID-19 news and preventive measures … daily by using loudspeaker (SU42, Myanmar) In our living area, local authorities promptly update information about the COVID pandemic, which helps us to keep aware of protecting our family (SU72, Vietnam) Access and accessibility: I have a television set and a radio: therefore, getting information especially through radio in vernacular language (SU03, Kenya) (need to) improve the use of visual audio media and social networks (SU27, Nicaragua) Accuracy: Give to the people the truth about COVID-19 and how people can immunize themselves. Give to people accurate information and give them basic knowledge in health issues especially persons with disabilities (SU26, Rwanda) | Make use of multiple and diverse opportunities, platforms and networks to disseminate regular, reliable and transparent public health messages across local areas and languages. Public health messages should be accessible for all including people with vision, hearing, cognition or communication access needs. Provide specific messaging for people who use AT regarding how changes will impact them and actions they can take. |
| Perspectives of People Who Use AT on Service Access | Principles for Sustaining AT Services | |
|---|---|---|
| Examples of Difficulties | Examples of Solutions | |
| Access to services and service personnel: Assessment (was) remote, then access to therapies with extreme protective and health measures…but the remote follow-ups were inoperative (SU37, Nicaragua) Many businesses were closed and it was difficult to get an appointment and if you did-do you really want to go? (SU18, Kenya) There was restriction in accessing service centres and I had also fear of getting infected (SU53, Bangladesh) My orthotics need to be renewed because I have grew up a little bit (SU50, Benin) Rehabilitation services … were stopped hence no services related to assistive devices and services were rendered (SU45, Tanzania) I was not allowed to go to some services, and many couldn’t come to me. Physio, OT students and OT, and masseuse weren’t allowed to visit (SU65, Australia) Issues of supply and repair: I can’t control on my urine and stool, so I have to use urine bag every time but in COVID time we were face many problem in getting it (SU27, India) The lockdown caused hearing aid centers to close and thus, we can’t avail the services and maintenance for our hearing aids. We can’t even buy batteries (SU57, Philippines) N’s hearing aids couldn’t be repaired so she refused to wear it sometimes as the family couldn’t adjust in a right way (SU67, Vietnam) I used to go center for repair and maintenance and sometimes as follow up once or twice in a month… Due to locked down it was closed for certain times until the service provider got safety measures (SU21, Nepal) | Telehealth and regular contact: ... so I used zoom where possible but it was not always suitable (SU65, Australia) I was in touch with service provider through telecommunication so when the situation was under control I got access to service center (SU21, Nepal) The telehealth policy was only for rural people but has been expanded to everybody and this has helped a lot. Its worrying that this might go away afterwards (SU61, Australia) I used e-appointments and video-calling for minor prosthetic issues (SU23, India) I can access online and if anything needs to be sent to me, {Provider] organize for it to be delivered. If I just need advice, AT are on the end of the phone (SU55, Ireland) I was in touch with service provider through telecommunication so when the situation was under control I got access to service center (SU21, Nepal) Stocking up: During COVID-19, I ensured that I stocked up on hearing aid batteries (SU12, India) AT Services opened with protection measures: Services are open but ‘must follow health safety protocol’ (SU72, Vietnam) | Use telehealth including zoom consultations and telephone contact to bridge service gaps, support regular contact between AT users and service providers and reduce access barriers. Where internet and delivery services operate well, online ordering systems can support access to consumables and spare parts. AT services require access to training for personnel and equipment to ensure adequate infection control measures, reducing the risk of face-to-face contact for all involved. |
| Recommendations |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Layton, N.; Mont, D.; Puli, L.; Calvo, I.; Shae, K.; Tebbutt, E.; Hill, K.D.; Callaway, L.; Hiscock, D.; Manlapaz, A.; et al. Access to Assistive Technology during the COVID-19 Global Pandemic: Voices of Users and Families. Int. J. Environ. Res. Public Health 2021, 18, 11273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111273
Layton N, Mont D, Puli L, Calvo I, Shae K, Tebbutt E, Hill KD, Callaway L, Hiscock D, Manlapaz A, et al. Access to Assistive Technology during the COVID-19 Global Pandemic: Voices of Users and Families. International Journal of Environmental Research and Public Health. 2021; 18(21):11273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111273
Chicago/Turabian StyleLayton, Natasha, Daniel Mont, Louise Puli, Irene Calvo, Kylie Shae, Emma Tebbutt, Keith D. Hill, Libby Callaway, Diana Hiscock, Abner Manlapaz, and et al. 2021. "Access to Assistive Technology during the COVID-19 Global Pandemic: Voices of Users and Families" International Journal of Environmental Research and Public Health 18, no. 21: 11273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111273