
Impact of the COVID-19 Pandemic on Palliative Care in Cancer Patients in Spain

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
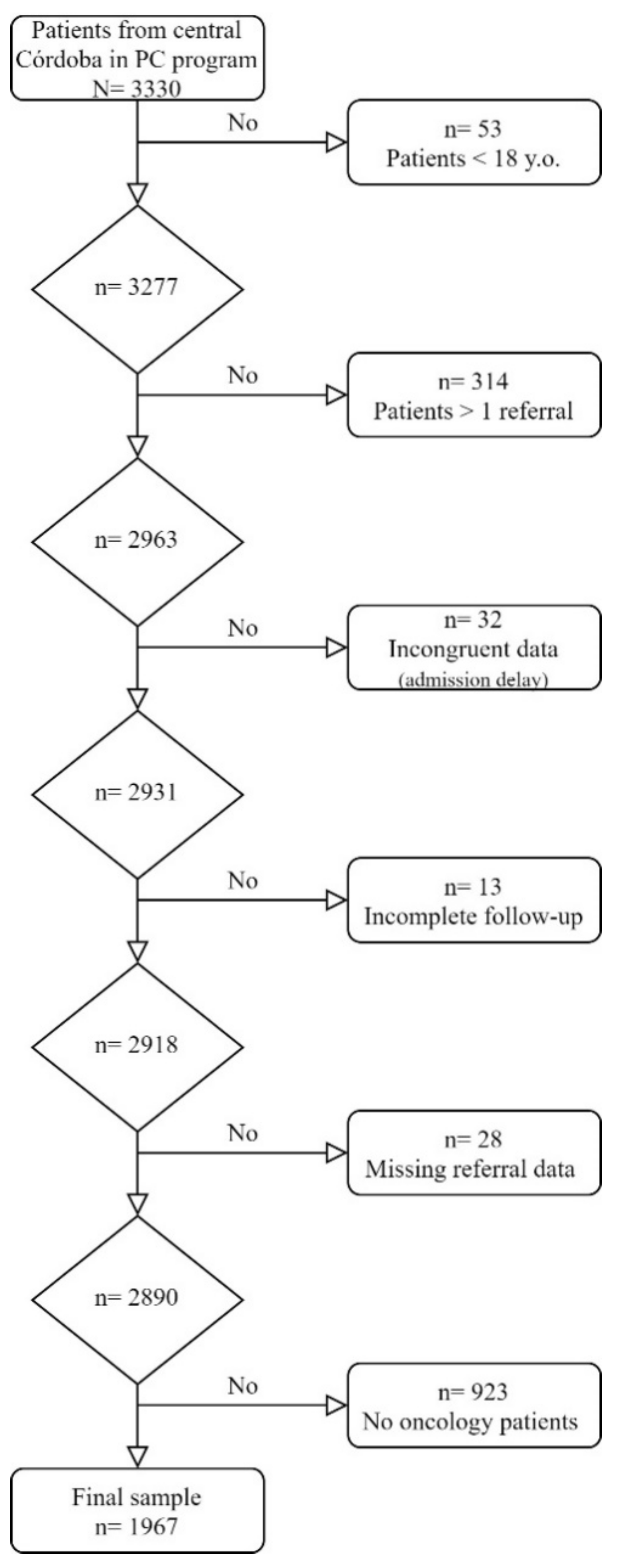
2.2. Sample and Procedure
2.3. Data Analysis
2.4. Ethical Statements
3. Results
3.1. Patients’ Socio-Demographic Data
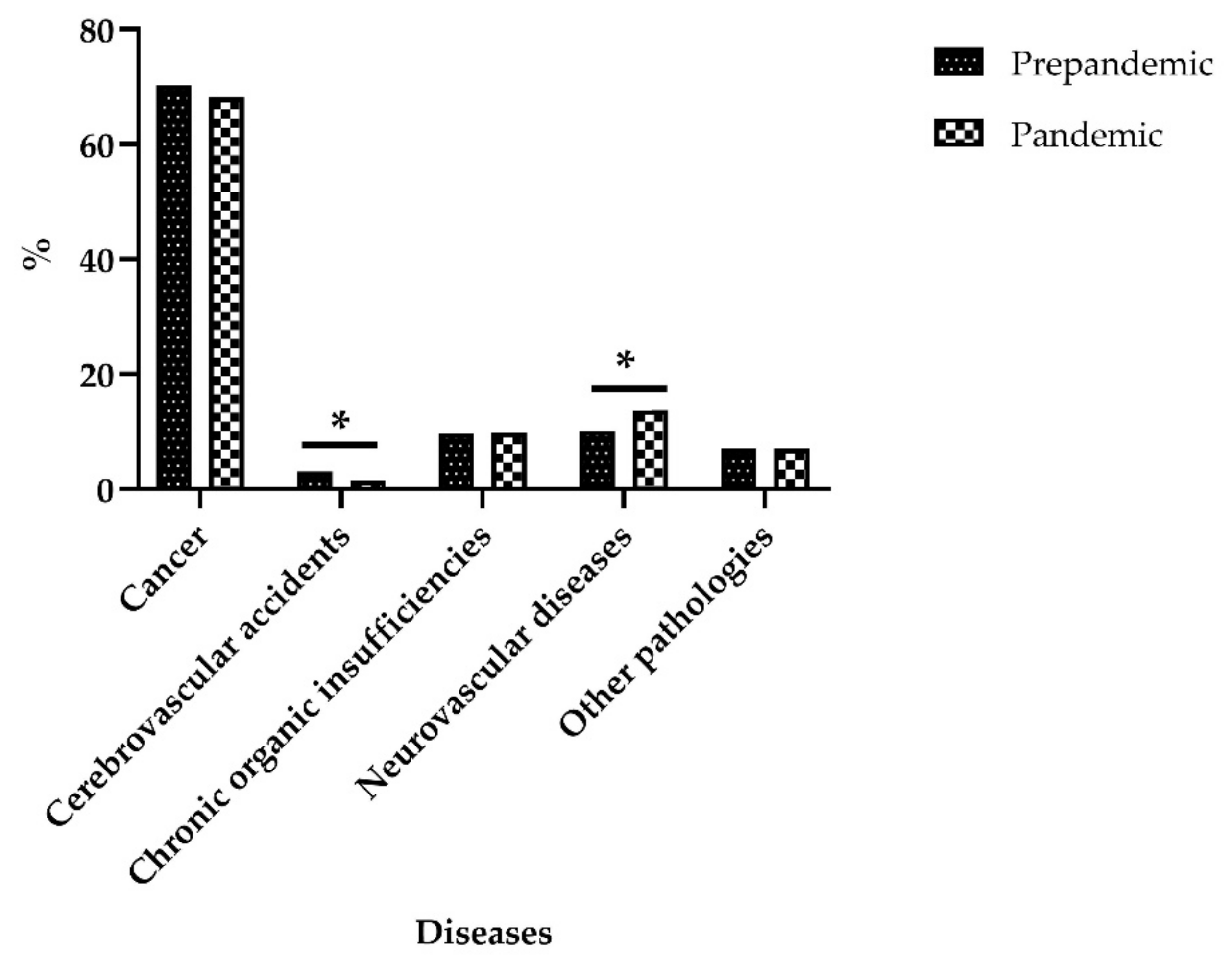
3.2. Patients’ Clinical Situation
3.3. Healthcare Provided
Risk and Survival Analysis for the Permanence of Patients in the Program
3.4. Degree of Patients’ Knowledge and Preferences
4. Discussion
4.1. Patients’ Socio-Demographic Data
4.2. Patients’ Clinical Situation
4.3. Healthcare Provided
4.4. Degree of Patients’ Knowledge and Preferences
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Organización Médica Colegial of Spain (OMC). Código de Dentología Médica: Guía de Ética Médica; Organización Médica Colegial of Spain: Madrid, Spain, 2011. [Google Scholar]
- Allert, G.; Blasszauer, B.; Boyd, K.; Callahan, D. The goals of medicine: Setting new priorities. Hastings Cent. Rep. 1996, 26, S1. [Google Scholar]
- Emmerich, N. Leadership in palliative medicine: Moral, ethical and educational. BMC Med. Ethics 2018, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Palliative Care. 2020. Available online: https://www.who.int/es/news-room/fact-sheets/detail/palliative-care (accessed on 20 July 2021).
- Hodiamont, F.; Jünger, S.; Leidl, R.; Maier, B.O.; Schildmann, E.; Bausewein, C. Understanding complexity—the palliative care situation as a complex adaptive system. BMC Health Serv. Res. 2019, 19, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wynne, K.J.; Petrova, M.; Coghlan, R. Dying individuals and suffering populations: Applying a population-level bioethics lens to palliative care in humanitarian contexts: Before, during and after the COVID-19 pandemic. J. Med. Ethics 2020, 46, 514–525. [Google Scholar] [CrossRef]
- Rosa, W. Access to palliative care as public health priority-Yes, you heard me right. Public Health Nurs. 2017, 34, 513–514. [Google Scholar] [CrossRef] [PubMed]
- A Powell, R.; Schwartz, L.; Nouvet, E.; Sutton, B.; Petrova, M.; Marston, J.; Munday, D.; Radbruch, L. Palliative care in humanitarian crises: Always something to offer. Lancet 2017, 389, 1498–1499. [Google Scholar] [CrossRef]
- Chapman, M.; Russell, B.; Philip, J. Systems of Care in Crisis: The Changing Nature of Palliative Care during COVID-19. J. Bioethical Inq. 2020, 17, 761–765. [Google Scholar] [CrossRef]
- Park, M.; Cook, A.R.; Lim, J.T.; Sun, Y.; Dickens, B.L. A Systematic Review of COVID-19 Epidemiology Based on Current Evidence. J. Clin. Med. 2020, 9, 967. [Google Scholar] [CrossRef] [Green Version]
- Vallath, N.; Damani, A.; Ghoshal, A.; Salins, N.; Bhatnagar, S.; Sanghavi, P.R.; Viswanath, V.; Ostwal, S.; Chinchalkar, G. Approaches and best practices for managing cancer pain within the constraints of the COVID-19 pandemic in India. Indian J. Palliat. Care 2020, 26, S106. [Google Scholar] [CrossRef]
- Rogers, J.E.B.; Constantine, L.A.; Thompson, J.M.; Mupamombe, C.T.; Vanin, J.M.; Navia, R.O. COVID-19 Pandemic Impacts on U.S. Hospice Agencies: A National Survey of Hospice Nurses and Physicians. Am. J. Hosp. Palliat. Med. 2021, 38, 521–527. [Google Scholar] [CrossRef]
- AlWaheidi, S.; Sullivan, R.; A Davies, E. Additional challenges faced by cancer patients in Gaza due to COVID-19. Ecancermedicalscience 2020, 14, ed100. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, J.; Castro, L.; Rêgo, G.; Nunes, R. Burnout Determinants among Nurses Working in Palliative Care during the Coronavirus Disease 2019 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3358. [Google Scholar] [CrossRef] [PubMed]
- Büntzel, J.; Klein, M.; Keinki, C.; Walter, S.; Büntzel, J.; Hübner, J. Oncology services in corona times: A flash interview among German cancer patients and their physicians. J. Cancer Res. Clin. Oncol. 2020, 146, 2713–2715. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.; Sachdeva, S.; Parekh, T.; Desai, R. COVID-19 and Cancer: Lessons from a Pooled Meta-Analysis. JCO Glob. Oncol. 2020, 6, 557–559. [Google Scholar] [CrossRef] [PubMed]
- Blinderman, C.D.; Adelman, R.; Kumaraiah, D.; Pan, C.X.; Palathra, B.C.; Kaley, K.; Trongone, N.; Spillane, K. A Comprehensive Approach to Palliative Care during the Coronavirus Pandemic. J. Palliat. Med. 2021, 24, 1017–1022. [Google Scholar] [CrossRef]
- Fausto, J.; Hirano, L.; Lam, D.; Mehta, A.; Mills, B.; Owens, D.; Perry, E.; Curtis, J.R. Creating a Palliative Care Inpatient Response Plan for COVID-19—The UW Medicine Experience. J. Pain Symptom Manag. 2020, 60, e21–e26. [Google Scholar] [CrossRef]
- De Gatta Sánchez, D.F. Real Decreto 463/2020, de 14 de marzo, por el que se declara el estado de alarma para la gestión de la situación de crisis sanitaria ocasionada por el covid-19 y sus prórrogas. Ars Iuris Salmant. 2020, 8, 192–199. [Google Scholar]
- Martin-Roselló, M.L.; Fernández-López, A.; Sanz-Amores, R.; Gómez-García, R.; Vidal-España, F.; Cia-Ramos, R. IDC-Pal: Instrumento Diagnóstico de la Complejidad en Cuidados Paliativos. 2014. Available online: http://www.juntadeandalucia.es/salud/IDCPal (accessed on 19 August 2021).
- Karnofsky, D.A.; Abelmann, W.H.; Craver, L.F.; Burchenal, J.H. The use of the nitrogen mustards in the palliative treatment of carcinoma-with particular reference to bronchogenic carcinoma. Cancer 1948, 1, 634–656. [Google Scholar] [CrossRef]
- Zubrod, C.G.; Schneiderman, M.; Frei, E.; Brindley, C.; Gold, G.L.; Shnider, B.; Oviedo, R.; Gorman, J.; Jones, R.; Jonsson, U.; et al. Appraisal of methods for the study of chemotherapy of cancer in man: Comparative therapeutic trial of nitrogen mustard and triethylene thiophosphoramide. J. Chronic Dis. 1960, 11, 7–33. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Rajan, S.; Chakrabarti, D.; Akhtar, N.; Kumar, V.; Verma, M. Searching for answers: Cancer care during the COVID pandemic. Clin. Epidemiology Glob. Health 2021, 10, 100696. [Google Scholar] [CrossRef]
- Sociedad Española de Oncología Médica (SEOM). Las cifras del cáncer en España. 2021. Available online: https://seom.org/ (accessed on 15 August 2021).
- Kuhlen, R.; Winklmair, C.; Schmithausen, D.; Schick, J.; Scriba, P. The Effects of the COVID-19 Pandemic and Lockdown on Routine Hospital Care for Other Illnesses. Dtsch. Aerzteblatt Online 2020, 117, 488–489. [Google Scholar] [CrossRef]
- Reichardt, P.; Bollmann, A.; Hohenstein, S.; Glass, B.; Untch, M.; Reichardt, A.; Amrein, D.; Kuhlen, R. Decreased Incidence of Oncology Admissions in 75 Helios Hospitals in Germany during the COVID-19 Pandemic. Oncol. Res. Treat. 2021, 44, 71–75. [Google Scholar] [CrossRef] [PubMed]
- AlShehery, M.Z.; Duraisamy, B.; Zaidi, A.R.Z.; AlShehry, N.F.; Zaidi, F.Z.; Rababah, A.A.; Assiri, A.A.; AlGhamdi, M.S.; Al Mutair, A.; Al-Omari, A. COVID-19 and Palliative Care Services: Comparative Patterns of Inpatient, Outpatient, and Consultation Services in a Tertiary Care Center in Riyadh. Cureus 2020, 12, e11996. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Hammoudi, A.; Marliot, G.; De Courreges, A.; Cucchi, M.; Mirabel, X.; Leblanc, E.; Lartigau, E. Major impact of COVID-19 national containment on activities in the French northern comprehensive cancer center. Med Oncol. 2021, 38, 1–5. [Google Scholar] [CrossRef]
- Chou, Y.-C.; Yen, Y.-F.; Feng, R.-C.; Wu, M.-P.; Lee, Y.-L.; Chu, D.; Huang, S.-J.; Curtis, J.R.; Hu, H.-Y. Impact of the COVID-19 Pandemic on the Utilization of Hospice Care Services: A Cohort Study in Taiwan. J. Pain Symptom Manag. 2020, 60, e1–e6. [Google Scholar] [CrossRef]
- Sanghavi, P.; Singh, M.; Patel, B.; Umrania, R.; Chishi, K.; Ghoghari, M. Experience of palliative care services at tertiary comprehensive cancer center during COVID-19 lockdown phase: An analytical original study. Indian J. Palliat. Care 2020, 26, S27. [Google Scholar] [CrossRef]
- Rhee, J.; Grant, M.; Detering, K.; Clayton, J.; Arthurs, K. Dying still matters in the age of COVID-19. Aust. J. Gen. Pr. 2020, 49, 28. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Significantly Impacts Health Services for Noncommunicable Diseases. 2020. Available online: https://www.who.int/news/item/01-06-2020-covid-19-significantly-impacts-health-services-for-noncommunicable-diseases (accessed on 10 August 2021).
- Yu, J.; Ouyang, W.; Chua, M.L.K.; Xie, C. SARS-CoV-2 Transmission in Patients with Cancer at a Tertiary Care Hospital in Wuhan, China. JAMA Oncol. 2020, 6, 1108–1110. [Google Scholar] [CrossRef] [Green Version]
- Petrova, D.; Pérez-Gómez, B.; Pollán, M.; Sánchez, M.-J. Implications of the COVID-19 pandemic for cancer in Spain. Med. Clin. 2020, 155, 263. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.-Y.; Desai, A.; Lopes, G.D.L.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Montero-Oleas, N.; Puente-Vallejo, R.; León-Micheli, B.; Imbaquingo-Cabrera, A.; Silva, M.; Gamarra, E.; Álvarez-Rodas, B.; Segovia, N.; Aldaz-Roldan, P.; Nuñez-Silva, C.; et al. Reducing the impact of COVID-19 on radiation oncology units of developing countries: A rapid review and expert consensus. Medwave 2020, 20, e8012. [Google Scholar] [CrossRef] [PubMed]
- Richards, M.; Anderson, M.; Carter, P.; Ebert, B.L.; Mossialos, E. The impact of the COVID-19 pandemic on cancer care. Nat. Rev. Cancer 2020, 1, 565–567. [Google Scholar] [CrossRef] [PubMed]
- Shankar, A.; Saini, D.; Roy, S.; Jarrahi, A.M.; Chakraborty, A.; Bharti, S.J.; Taghizadeh-Hesary, F. Cancer Care Delivery Challenges Amidst Coronavirus Disease-19 (COVID-19) Outbreak: Specific Precautions for Cancer Patients and Cancer Care Providers to Prevent Spread. Asian Pac. J. Cancer Prev. 2020, 21, 569–573. [Google Scholar] [CrossRef]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.Q.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef]
- Robilotti, E.V.; Babady, N.E.; Mead, P.A.; Rolling, T.; Perez-Johnston, R.; Bernardes, M.; Bogler, Y.; Caldararo, M.; Figueroa, C.J.; Glickman, M.S.; et al. Determinants of COVID-19 disease severity in patients with cancer. Nat. Med. 2020, 26, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- European Society for Medical Oncology (ESMO). Cancer Patient Management during the COVID-19 Pandemic. 2020. Available online: https://www.esmo.org/guidelines/cancer-patient-management-during-the-covid-19-pandemic (accessed on 7 August 2021).
- Graboyes, E.M.; Kompelli, A.R.; Neskey, D.M.; Brennan, E.; Nguyen, S.; Sterba, K.R.; Warren, G.W.; Hughes-Halbert, C.; Nussenbaum, B.; Day, T.A. Association of Treatment Delays with Survival for Patients with Head and Neck Cancer: A Systematic Review. JAMA Otolaryngol. Neck Surg. 2019, 145, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Kutikov, A.; Weinberg, D.S.; Edelman, M.; Horwitz, E.M.; Uzzo, R.G.; Fisher, R.I. A War on Two Fronts: Cancer Care in the Time of COVID-19. Ann. Intern. Med. 2020, 172, 756–758. [Google Scholar] [CrossRef] [Green Version]
- Amaddeo, G.; Brustia, R.; Allaire, M.; Lequoy, M.; Hollande, C.; Regnault, H.; Blaise, L.; Ganne-Carrié, N.; Séror, O.; Larrey, E.; et al. Impact of COVID-19 on the management of hepatocellular carcinoma in a high-prevalence area. JHEP Rep. 2021, 3, 100199. [Google Scholar] [CrossRef]
- Sigorski, D.; Sobczuk, P.; Osmola, M.; Kuć, K.; Walerzak, A.; Wilk, M.; Ciszewski, T.; Kopeć, S.; Hryń, K.; Rutkowski, P.; et al. Impact of COVID-19 on anxiety levels among patients with cancer actively treated with systemic therapy. ESMO Open 2020, 5, e000970. [Google Scholar] [CrossRef]
- Miller, J.; Maeda, Y.; Au, S.; Gunn, F.; Porteous, L.; Pattenden, R.; MacLean, P.; Noble, C.L.; Glancy, S.; Dunlop, M.G.; et al. Short-term outcomes of a COVID-adapted triage pathway for colorectal cancer detection. Color. Dis. 2021, 23, 1639–1648. [Google Scholar] [CrossRef]
- Beltran-Aroca, C.M.; González-Tirado, M.; Girela-López, E. Ethical issues in primary care during the coronavirus (SARS-CoV-2) pandemic. Semergen 2020, 47, 122–130. [Google Scholar] [CrossRef]
- Temel, J.S.; Greer, J.A.; Muzikansky, A.; Gallagher, E.R.; Admane, S.; Jackson, V.A.; Dahlin, C.M.; Blinderman, C.D.; Jacobsen, J.; Pirl, W.; et al. Early Palliative Care for Patients with Metastatic Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2010, 363, 733–742. [Google Scholar] [CrossRef] [Green Version]
- Smith, T.; Temin, S.; Alesi, E.R.; Abernethy, A.P.; Balboni, T.A.; Basch, E.M.; Ferrell, B.R.; Loscalzo, M.; Meier, D.E.; Paice, J.; et al. American Society of Clinical Oncology Provisional Clinical Opinion: The Integration of Palliative Care Into Standard Oncology Care. J. Clin. Oncol. 2012, 30, 880–887. [Google Scholar] [CrossRef] [PubMed]
- De Salud, C.; de Andalucía, J. Plan Andaluz de Cuidados Paliativos: 2008–2012. Available online: https://www.juntadeandalucia.es/organismos/saludyfamilias.html (accessed on 20 August 2021).
- Wise, J. Covid-19: Cancer mortality could rise at least 20% because of pandemic, study finds. BMJ 2020, 369, m1735. [Google Scholar] [CrossRef]
- Webster, P. Virtual health care in the era of COVID-19. Lancet 2020, 395, 1180–1181. [Google Scholar] [CrossRef]
- De Angelis, R.; Sant, M.; Coleman, M.; Francisci, S.; Baili, P.; Pierannunzio, D.; Trama, A.; Visser, O.; Brenner, H.; Ardanaz, E.; et al. Cancer survival in Europe 1999–2007 by country and age: Results of EUROCARE-5—A population-based study. Lancet Oncol. 2014, 15, 23–34. [Google Scholar] [CrossRef]
- Arnold, M.; Rutherford, M.; Bardot, A.; Ferlay, J.; Andersson, T.M.-L.; Myklebust, T.Å.; Tervonen, H.; Thursfield, V.; Ransom, D.; Shack, L.; et al. Progress in cancer survival, mortality, and incidence in seven high-income countries 1995–2014 (ICBP SURVMARK-2): A population-based study. Lancet Oncol. 2019, 20, 1493–1505. [Google Scholar] [CrossRef] [Green Version]
- Haase, K.R.; Kain, D.; Merchant, S.; Booth, C.; Koven, R.; Brundage, M.; Galica, J. Older survivors of cancer in the COVID-19 pandemic: Reflections and recommendations for future care. J. Geriatr. Oncol. 2021, 12, 461–466. [Google Scholar] [CrossRef] [PubMed]
- Pendyala, P.; Goglia, A.G.; Mattes, M.D.; Grann, A.; Huang, D.; Wagman, R.T.; Yehia, Z.A.; Yoon, J.; Ennis, R.D. Impact of the Coronavirus Disease of 2019 Pandemic on Radiation Oncology Clinical Decision Making in a High-Prevalence Environment. Adv. Radiat. Oncol. 2021, 6, 100680. [Google Scholar] [CrossRef] [PubMed]
- Wentlandt, K.; Seccareccia, D.; Kevork, N.; Workentin, K.; Blacker, S.; Grossman, D.; Zimmermann, C. Quality of Care and Satisfaction with Care on Palliative Care Units. J. Pain Symptom Manag. 2016, 51, 184–192. [Google Scholar] [CrossRef] [Green Version]
- Cabañero-Martínez, M.; Nolasco, A.; Melchor, I.; Fernández-Alcántara, M.; Cabrero-García, J. Place of death of people with conditions needing palliative care in the different regions of Spain. An. Sist. Sanit. Navar. 2020, 43, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Babarro, A.; Bruera, E.; Varela-Cerdeira, M.; Boya-Cristia, M.J.; Madero, R.; Torres, I.; De Castro, J.; González-Barón, M. Can This Patient Be Discharged Home? Factors Associated with At-Home Death among Patients With Cancer. J. Clin. Oncol. 2011, 29, 1159–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutiérrez-Sánchez, D.; Gómez-García, R.; Roselló, M.L.M.; Cuesta-Vargas, A.I. The Quality of Dying and Death of Advanced Cancer Patients in Palliative Care and Its Association with Place of Death and Quality of Care. J. Hosp. Palliat. Nurs. 2021, 23, 264–270. [Google Scholar] [CrossRef]
- Nitola-Mendoza, L.; Centeno, C. Place of death of patients receiving palliative care: Can we reverse the trend of dying in hospitals? An. Sist. Sanit. Navar. 2021, 44, 125–126. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Babarro, A.; Astray-Mochales, J.; Domínguez-Berjón, F.; Gènova-Maleras, R.; Bruera, E.; Díaz-Mayordomo, A.; Cortes, C.C. The association between in-patient death, utilization of hospital resources and availability of palliative home care for cancer patients. Palliat. Med. 2013, 27, 68–75. [Google Scholar] [CrossRef]
- Strang, P.; Hedman, C.; Adlitzer, H.; Schultz, T. Dying from cancer with COVID-19: Age, sex, socio-economic status, and comorbidities. Acta Oncol. 2021, 60, 1–6. [Google Scholar] [CrossRef]
- Arias-Casais, N.; López-Fidalgo, J.; Garralda, E.; Pons, J.J.; Rhee, J.Y.; Lukas, R.; De Lima, L.; Centeno, C. Trends analysis of specialized palliative care services in 51 countries of the WHO European region in the last 14 years. Palliat. Med. 2020, 34, 1044–1056. [Google Scholar] [CrossRef]
- Ali, M.; Capel, M.; Jones, G.; Gazi, T. The importance of identifying preferred place of death. BMJ Support. Palliat. Care 2019, 9, 84–91. [Google Scholar] [CrossRef]
- Brinkman-Stoppelenburg, A.; Rietjens, J.A.; Van Der Heide, A. The effects of advance care planning on end-of-life care: A systematic review. Palliat. Med. 2014, 28, 1000–1025. [Google Scholar] [CrossRef]
- Mohammed, T.; Ali, I.; Desai, A. COVID-19 in Older Individuals with Cancer: Problem and Potential Solutions. Cancer Investig. 2021, 39, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Wallace, C.L.; Wladkowski, S.; Gibson, A.; White, P. Grief during the COVID-19 Pandemic: Considerations for Palliative Care Providers. J. Pain Symptom Manag. 2020, 60, e70–e76. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patients’ socio-demographic data | Gender | Male/Female |
| Age | Years | |
| Main caregiver | FDR 1; SDR 2; other relatives; professionals | |
| Clinical situation of patient | Cancer | Type of oncological process |
| Metastasis | Presence or absence | |
| Complexity [20] | Non-complex situation; complex; highly complex discharge | |
| Reason for leaving program | Discharge; death | |
| Karnofsky Performance Status scale (KPS) | Ability to perform routine tasks (0–100) | |
| Eastern Cooperative Oncology Group scale (ECOG) | Cancer patient’s quality of life (0–5) | |
| Health care provided | Referred from | Primary care; outpatient care; inpatient care; emergency care and other |
| CMU 3 of origin | Type of CMU | |
| Derivation priority | Normal; Urgent; Preferential | |
| Place of death | Home; general hospital; PC hospital; emergency ward; others | |
| Total delay | Time from patient referral to PC to inclusion in program (days) | |
| Length of stay in program (patient’s survival) | Time from patient being attended to patient leaving program (days) | |
| Degree of patient’s knowledge and preferences | Advance vital directives | Document registered by patient (yes/no) |
| Knowledge of patient and family | Degree of patient’s knowledge of real situation (not informed; partial; full knowledge; not applicable) | |
| Assessment of patient and family | Degree of assessment and understanding of patient’s situation (not informed; partial; full knowledge; not applicable) |
| Scale | Points | Description |
|---|---|---|
| Karnofsky Performance Status scale 1 (KPS) [21] | 0 | Dead |
| 10 | Moribund | |
| 20 | Completely bedridden, very sick, hospital admission necessary; active support treatment necessary | |
| 30 | Severely disabled; hospital admission indicated, and active supportive treatment given | |
| 40 | Disabled, requires special care and assistance. Bedridden for over half the day. | |
| 50 | Requires considerable assistance and frequent medical. Bedridden for less than half the day. | |
| 60 | Requires occasional assistance but is able to care for most personal needs | |
| 70 | Cares for self; unable to carry on normal activity or do active work | |
| 80 | Able to perform normal activity with effort; some signs and symptoms of disease | |
| 90 | Able to carry on normal activity; minor signs and symptoms of disease | |
| 100 | Normal, no complaints, no evidence of disease | |
| Eastern Cooperative Oncology Group scale 2 (ECOG) [22] | 0 | Completely asymptomatic, fully able to do work and everyday activities |
| 1 | Shows symptoms that do not prevent them from doing their work or everyday activities | |
| 2 | Unable to carry out any work activities, with symptoms which force them to stay in bed for several hours a day | |
| 3 | Confined to bed or chair for more than half the day due to the existence of symptoms | |
| 4 | Totally confined to bed or chair all day and needing help with all everyday activities | |
| 5 | Dying or will die within hours |
| Pre-Pandemic | Pandemic | p-Value | |
|---|---|---|---|
| n = 1219 (%) | n = 748 (%) | ||
| Gender | 0.027 | ||
| Males | 743 (61%) | 418 (55.8%) | |
| Females | 476 (39%) | 330 (44.2%) | |
| Age (years) | 0.574 | ||
| Median [IQR] 1 | 75.69 [64.98–83.73] | 75.61 [65.25–84.67] | |
| Caregivers | |||
| FDR 2 | 1020 (83.7%) | 657 (88%) | 0.008 |
| SDR 3 | 57 (4.7%) | 43 (5.7%) | |
| OR 4 | 104 (8.5%) | 37 (5%) | |
| Professionals | 38 (3.1%) | 11 (1.3%) |
| Pre-Pandemic | Pandemic | p-Value | |
|---|---|---|---|
| n = 1219 (%) | n = 748 (%) | ||
| Type of cancer | 0.242 | ||
| Lung | 270 (22.2%) | 136 (18.2%) | |
| Intracranial | 37 (3%) | 21 (2.8%) | |
| Haematological | 63 (5.2%) | 39 (5.2%) | |
| Prostate | 41 (3.4%) | 27 (3.6%) | |
| Urinary Tract | 83 (6.8%) | 58 (7.8%) | |
| Colorectal | 207 (17%) | 138 (18.5%) | |
| Breast | 78 (6.4%) | 52 (6.9%) | |
| Head-neck | 63 (5.2%) | 23 (3.1%) | |
| Genitals | 72 (5.9%) | 51 (6.8%) | |
| Oesophagus-stomach | 87 (7.1%) | 48 (6.4%) | |
| Liver | 49 (4%) | 33 (4.4%) | |
| Pancreas-bile ducts | 122 (10%) | 78 (10.4%) | |
| Bone | 1 (0.1%) | 4 (0.6%) | |
| Others | 45 (3.7%) | 40 (5.3%) | |
| Presence of metastasis | 0.156 | ||
| Yes | 469 (38.5%) | 313 (41.8%) | |
| Complexity | 0.020 | ||
| Not complex | 800 (65.6%) | 459 (61.3%) | |
| 1 complex element | 151 (12.4%) | 70 (9.3%) | |
| Several complex elements | 33 (2.7%) | 19 (2.6%) | |
| Highly complex | 235 (19.3%) | 200 (26.8%) | |
| KPS 1 (points) | 0.141 | ||
| 10 | 22 (1.8%) | 21 (2.8%) | |
| 20 | 61 (5%) | 26 (3.5%) | |
| 30 | 168 (13.8%) | 70 (9.3%) | |
| 40 | 261 (21.4%) | 153 (20.4%) | |
| 50 | 464 (38.1%) | 318 (42.5%) | |
| 60 | 191 (15.7%) | 121 (16.2%) | |
| 70 | 27 (2.2%) | 17 (2.3%) | |
| 80 | 11 (0.9%) | 17 (2.3%) | |
| 90 | 9 (0.7%) | 1 (0.2%) | |
| 100 | 5 (0.4%) | 4 (0.5%) | |
| ECOG 2 (points) | <0.001 | ||
| 0 | 12 (1%) | 0 (0%) | |
| 1 | 40 (3.3%) | 13 (1.7%) | |
| 2 | 631 (51.8%) | 186 (24.8%) | |
| 3 | 333 (27.2%) | 389 (52.1%) | |
| 4 | 191 (15.7%) | 153 (20.5%) | |
| 5 | 12 (1%) | 7 (0.9%) | |
| Reason for ending program | <0.001 | ||
| Discharge | 7 (0.6%) | 22 (2.9%) | |
| Death | 1212 (99.4%) | 726 (97.1%) |
| Pre-Pandemic | Pandemic | p-Value | |
|---|---|---|---|
| n = 1219 (%) | n = 748 (%) | ||
| Referral from | <0.001 | ||
| Primary care | 201 (16.5%) | 80 (10.7%) | |
| Outpatient care | 539 (44.2%) | 312 (41.7%) | |
| Inpatient care | 474 (38.9%) | 348 (46.5%) | |
| Emergency and other | 5 (0.4%) | 8 (1.1%) | |
| CMU 1 | 0.326 | ||
| Cardiology | 5 (0.4%) | 1 (0.2%) | |
| Plastic surgery | 4 (0.2%) | 3 (0.6%) | |
| General surgery | 44 (3.6%) | 24 (3.2%) | |
| Thoracic surgery | 0 (0%) | 1 (0.2%) | |
| Digestive | 126 (10.3%) | 74 (9.9%) | |
| Pain unit | 0 (0%) | 1 (0.2%) | |
| Gynaecology | 6 (0.5%) | 13 (1.7%) | |
| Home hospital treatment | 0 (0%) | 1 (0.2%) | |
| Haematology | 51 (4.2%) | 31 (4.1%) | |
| Infectious diseases | 2 (0.2%) | 1 (0.2%) | |
| Maxillofacial surgery | 6 (0.5%) | 2 (0.3%) | |
| Internal medicine | 121 (9.9%) | 79 (10.7%) | |
| Nephrology | 2 (0.2%) | 1 (0.2%) | |
| Neurosurgery | 13 (1.1%) | 8 (1.1%) | |
| Pneumology | 67 (5.5%) | 26 (3.5%) | |
| Neurology | 6 (0.5%) | 4 (0.6%) | |
| Oncology | 701 (57.5%) | 427 (57.2%) | |
| ENT 2 | 4 (0.3%) | 5 (0.9%) | |
| Oncology RT | 23 (1.9%) | 17 (2.3%) | |
| Interventional X-ray 3 | 0 (0%) | 1 (0.2%) | |
| Traumatology | 1 (0.1%) | 0 (0%) | |
| UCI | 2 (0.2%) | 0 (0%) | |
| Emergencies | 2 (0.2%) | 0 (0%) | |
| Urology | 32 (2.6%) | 23 (3.2%) | |
| Priority | 0.153 | ||
| Normal (no priority) | 1108 (90.9%) | 663 (88.7%) | |
| Urgent (priority 1) | 16 (1.3%) | 8 (1.1%) | |
| Preferential (priority 2) | 95 (7.8%) | 76 (10.2%) | |
| Delay (days) | 0.016 | ||
| Average [IQR] 4 | 1 [0–0] | 1 [0–0] | |
| Place of death | n = 1212 | n = 726 | <0.001 |
| Home | 609 (50.3%) | 422 (58.1%) | |
| General hospital | 165 (13.6%) | 110 (15.2%) | |
| Palliative hospital | 404 (33.3%) | 184 (25.3%) | |
| Emergencies | 17 (1.4%) | 8 (1.1%) | |
| Others | 17 (1.4%) | 2 (0.3%) |
| Pre-Pandemic | Pandemic | p-Value | ||
|---|---|---|---|---|
| Referral from | ECOG 1 (points) | n = 1219 (%) | n = 748 (%) | |
| Primary care n = 281 | 0 | 2 (1%) | 0 (0%) | <0.001 |
| 1 | 7 (3.5%) | 0 (0%) | ||
| 2 | 114 (56.7%) | 19 (23.8%) | ||
| 3 | 33 (16.4%) | 43 (53.8%) | ||
| 4 | 45 (22.4%) | 15 (18.8%) | ||
| 5 | 0 (0%) | 3 (3.8%) | ||
| Outpatient care n = 851 | 0 | 6 (1.1%) | 0 (0%) | <0.001 |
| 1 | 22 (4.1%) | 6 (1.9%) | ||
| 2 | 298 (55.3%) | 94 (30.1%) | ||
| 3 | 143 (26.5%) | 164 (52.6%) | ||
| 4 | 68 (12.6%) | 45 (14.4%) | ||
| 5 | 2 (0.4%) | 3 (1%) | ||
| Inpatient care n = 822 | 0 | 4 (0.8%) | 0 (0%) | <0.001 |
| 1 | 10 (2.1%) | 7 (2%) | ||
| 2 | 215 (45.4%) | 66 (19%) | ||
| 3 | 157 (33.1%) | 182 (52.3%) | ||
| 4 | 78 (16.5%) | 93 (26.7%) | ||
| 5 | 10 (2.1%) | 0 (0%) | ||
| Emergency and other n = 13 | 0 | 0 (0%) | 0 (0%) | 0.325 |
| 1 | 1 (20%) | 0 (0%) | ||
| 2 | 4 (80%) | 7 (87.5%) | ||
| 3 | 0 (0%) | 0 (0%) | ||
| 4 | 0 (0%) | 0 (0%) | ||
| 5 | 0 (0%) | 1 (12.5%) |
| HR 1 | 95% CI 2 | p-Value | |
|---|---|---|---|
| Pandemic | |||
| Pre-pandemic (reference) | |||
| Pandemic | 0.99 | 0.82–1.20 | 0.931 |
| Age (decades/years) | 0.89 | 0.84–0.95 | <0.001 |
| Gender | |||
| Male (reference) | |||
| Female | 0.79 | 0.67–0.93 | 0.005 |
| Presence of metastasis | |||
| No (reference) | |||
| Yes | 1.48 | 1.25–1.75 | <0.001 |
| KPS 3 | 0.84 | 0.78–0.91 | <0.001 |
| ECOG 4 | 1.16 | 1.02–1.31 | 0.024 |
| Referral from | |||
| Primary care (reference) | |||
| Outpatient care | 0.74 | 0.59–0.94 | 0.012 |
| Inpatient care | 1.00 | 0.78–1.27 | 0.968 |
| Emergencies and other | 0.99 | 0.23–4.18 | 0.988 |
| Priority | |||
| Normal (reference) | |||
| Urgent | 8.11 | 2.96–22.18 | <0.001 |
| Preferential | 1.38 | 1.06–1.81 | 0.017 |
| Pre-Pandemic | Pandemic | p-Value | |
|---|---|---|---|
| n = 1219 (%) | n = 748 (%) | ||
| ADLW 1 registered | 1.000 | ||
| Yes | 13 (1.1%) | 7 (1%) | |
| Patient’s knowledge | 0.192 | ||
| Not informed | 161 (13.2%) | 93 (12.4%) | |
| Partial knowledge | 375 (30.8%) | 276 (36.9%) | |
| Full knowledge | 683 (56%) | 379 (50.7%) | |
| Patient’s assessment | <0.001 | ||
| Not informed | 166 (13.6%) | 90 (12%) | |
| Partial knowledge | 66 (5.4%) | 31 (4.2%) | |
| Full knowledge | 658 (54%) | 511 (68.3%) | |
| Not known/Not applicable | 329 (27%) | 116 (15.5%) | |
| Family’s knowledge | 0.351 | ||
| Not informed | 1 (0.1%) | 4 (0.6%) | |
| Partial knowledge | 30 (2.5%) | 29 (3.9%) | |
| Full knowledge | 1176 (96.5%) | 706 (94.4%) | |
| Not known/Not applicable | 11 (0.9%) | 8 (1.1%) | |
| Family’s assessment | 0.683 | ||
| Not informed | 76 (6.2%) | 54 (7.2%) | |
| Partial knowledge | 29 (2.4%) | 10 (1.4%) | |
| Full knowledge | 1100 (90.2%) | 673 (90%) | |
| Not known/Not applicable | 15 (1.2%) | 10 (1.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beltran-Aroca, C.M.; Ruiz-Montero, R.; Llergo-Muñoz, A.; Rubio, L.; Girela-López, E. Impact of the COVID-19 Pandemic on Palliative Care in Cancer Patients in Spain. Int. J. Environ. Res. Public Health 2021, 18, 11992. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182211992
Beltran-Aroca CM, Ruiz-Montero R, Llergo-Muñoz A, Rubio L, Girela-López E. Impact of the COVID-19 Pandemic on Palliative Care in Cancer Patients in Spain. International Journal of Environmental Research and Public Health. 2021; 18(22):11992. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182211992
Chicago/Turabian StyleBeltran-Aroca, Cristina M., Rafael Ruiz-Montero, Antonio Llergo-Muñoz, Leticia Rubio, and Eloy Girela-López. 2021. "Impact of the COVID-19 Pandemic on Palliative Care in Cancer Patients in Spain" International Journal of Environmental Research and Public Health 18, no. 22: 11992. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182211992