
Socio-Economic Determinants of Health Literacy in High School Students: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey
2.2. General Health Literacy Index and Sub-Indices
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Group
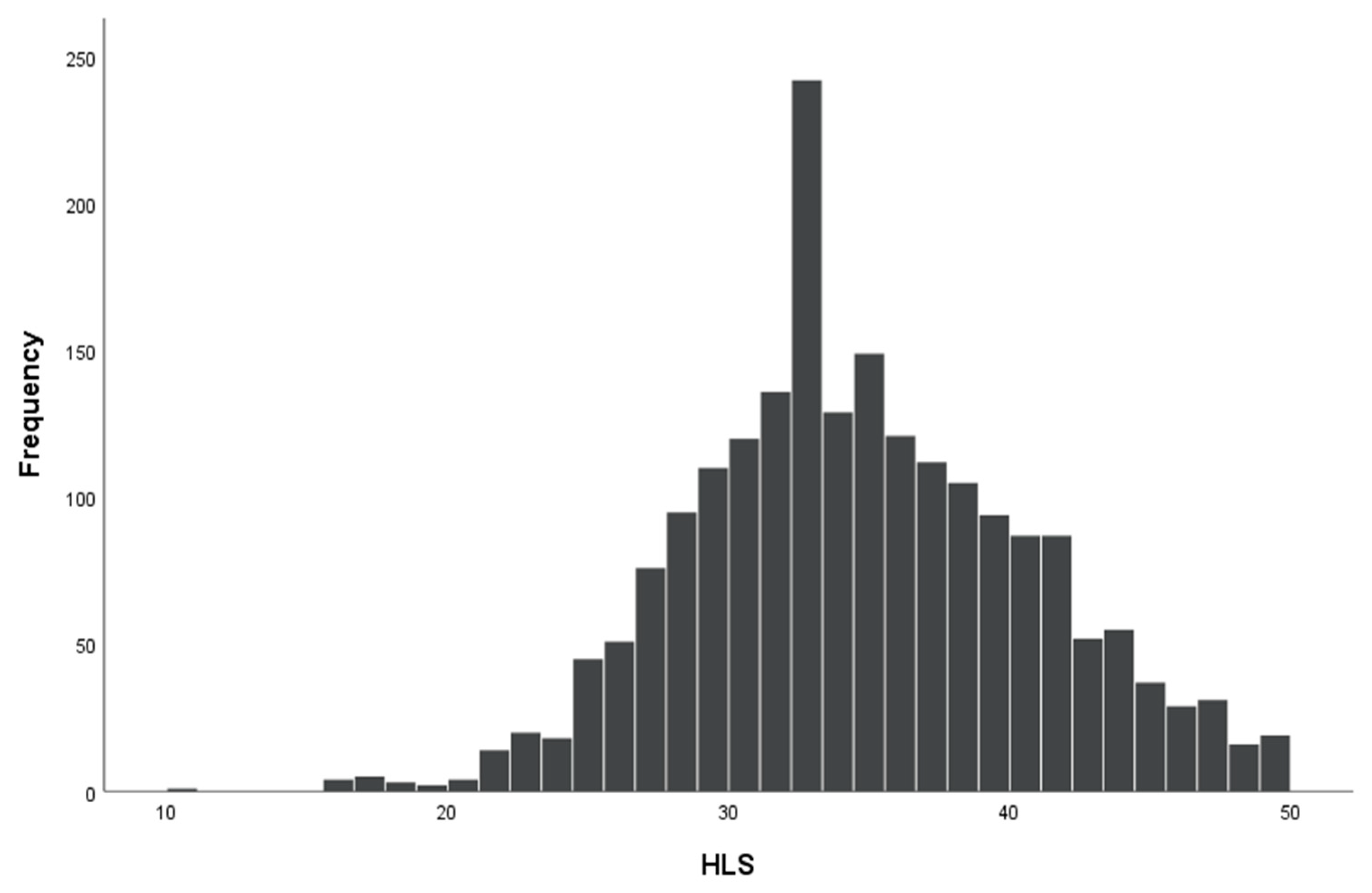
3.2. Health Literacy
3.3. Predictors of Sub-Indices of Health Literacy
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nutbeam, D.; Kickbusch, I. Health Promotion Glossary. Health Promot. Int. 1998, 13, 349–364. [Google Scholar] [CrossRef]
- Zaben, K.; Khalil, A. Health Literacy, Self-Care Behavior and Quality of Life in Acute Coronary Syndrome Patients: An Integrative Review. Open J. Nurs. 2019, 9, 383–395. [Google Scholar] [CrossRef] [Green Version]
- Duplaga, M. Determinants and Consequences of Limited Health Literacy in Polish Society. Int. J. Environ. Res. Public Health 2020, 17, 642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Humphrys, E.; Burt, J.; Rubin, G.; Emery, J.D.; Walter, F.M. The Influence of Health Literacy on the Timely Diagnosis of Symptomatic Cancer: A Systematic Review. Eur. J. Cancer Care 2019, 28, e12920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, K.; Pelikan, J.J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health Literacy in Europe: Comparative Results of the European Health Literacy Survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Shanghai Declaration on Promoting Health in the 2030 Agenda for Sustainable Development. Health Promot. Int. 2017, 32, 7–8. [Google Scholar] [CrossRef] [Green Version]
- Olives, T.; Patel, R.; Patel, S.; Hottinger, J.; Miner, J.R. Health Literacy of Adults Presenting to an Urban ED. Am. J. Emerg. Med. 2011, 29, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Rikard, R.V.; Thompson, M.S.; McKinney, J.; Beauchamp, A. Examining Health Literacy Disparities in the United States: A Third Look at the National Assessment of Adult Literacy (NAAL). BMC Public Health 2016, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toçi, E.; Burazeri, G.; Myftiu, S.; Sørensen, K.; Brand, H. Health Literacy in a Population-Based Sample of Adult Men and Women in a South Eastern European Country. J. Public Health 2016, 38, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Ozkan, S.; Dikmen, A.; Tuzun, H.; Karakaya, K. Prevalence and Determiners of Health Literacy in Turkey. Eur. J. Public Health 2016, 26. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, S.; Takamura, H.; Okumura, M. Sentiment Classification Using Word Sub-Sequences and Dependency Sub-Trees. In Pacific-Asia Conference on Knowledge Discovery and Data Mining; Springer: Berlin/Heidelberg, Germany, 2005; Volume 3518, pp. 301–311. [Google Scholar]
- Duong, T.V.; Aringazina, A.; Baisunova, G.; Nurjanah; Pham, T.V.; Pham, K.M.; Truong, T.Q.; Nguyen, K.T.; Oo, W.M.; Mohamad, E.; et al. Measuring Health Literacy in Asia: Validation of the HLS-EU-Q47 Survey Tool in Six Asian Countries. J. Epidemiol. 2017, 27, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Altin, S.V.; Finke, I.; Kautz-Freimuth, S.; Stock, S. The Evolution of Health Literacy Assessment Tools: A Systematic Review. BMC Public Health 2014, 14, 1207. [Google Scholar] [CrossRef] [Green Version]
- Okan, O.; Lopes, E.; Bollweg, T.M.; Bröder, J.; Messer, M.; Bruland, D.; Bond, E.; Carvalho, G.S.; Sørensen, K.; Saboga-Nunes, L.; et al. Generic Health Literacy Measurement Instruments for Children and Adolescents: A Systematic Review of the Literature. BMC Public Health 2018, 18, 166. [Google Scholar] [CrossRef] [Green Version]
- Marques, S.R.L.; Lemos, S.M.A. Health Literacy Assessment Instruments: Literature Review. Audiol. Commun. Res. 2017, 22, e1757. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Zeng, H.; Shen, Y.; Zhang, F.; Sharma, M.; Lai, W.; Zhao, Y.; Tao, G.; Yuan, J.; Zhao, Y. Assessment Tools for Health Literacy among the General Population: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 1711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perry, E.L. Health Literacy in Adolescents: An Integrative Review. J. Spec. Pediatr. Nurs. 2014, 19, 210–218. [Google Scholar] [CrossRef]
- Davis, T.C.; Wolf, M.S.; Arnold, C.L.; Byrd, R.S.; Long, S.W.; Springer, T.; Estela, K.; Bocchini, J.A. Development and Validation of the Rapid Estimate of Adolescent Literacy in Medicine (REALM-Teen): A Tool to Screen Adolescents for below-Grade Reading in Health Care Settings. Pediatrics 2006, 118, e1707–e1714. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Kondilis, B.K.; Patelarou, E.; Akrivos, P.D.; Falagas, M.E. Health Literacy and Sources of Health Education among Adolescents in Greece. Int. J. Adolesc. Med. Health 2009, 21, 179–186. [Google Scholar] [CrossRef]
- Röthlin, F.; Pelikan, J.; Ganahl, K. Die Gesundheitskompetenz von 15-Jährigen Jugendlichen in Österreich; Abschlussbericht Der Österreichischen Gesundheitskompetenz Jugendstudie Im Auftrag Des Hauptverbands Der Österreichischen Sozialversicherungsträger (HVSV); Ludwig Boltzmann Gesellschaft GmbH: Vienna, Austria, 2013. [Google Scholar]
- Driessnack, M.; Chung, S.; Perkhounkova, E.; Hein, M. Using the “Newest Vital Sign” to Assess Health Literacy in Children. J. Pediatr. Health Care 2014, 28, 165–171. [Google Scholar] [CrossRef]
- Bröder, J.; Okan, O.; Bauer, U.; Bruland, D.; Schlupp, S.; Bollweg, T.M.; Saboga-Nunes, L.; Bond, E.; Sørensen, K.; Bitzer, E.M.; et al. Health Literacy in Childhood and Youth: A Systematic Review of Definitions and Models. BMC Public Health 2017, 17. [Google Scholar] [CrossRef]
- Wu, A.D.; Begoray, D.L.; MacDonald, M.; Higgins, J.W.; Frankish, J.; Kwan, B.; Fung, W.; Rootman, I. Developing and Evaluating a Relevant and Feasible Instrument for Measuring Health Literacy of Canadian High School Students. Health Promot. Int. 2021, 25, 444–452. [Google Scholar] [CrossRef] [Green Version]
- Dehghankar, L.; Panahi, R.; Kekefallah, L.; Hosseini, N.; Hasannia, E. The Study of Health Literacy and Its Related Factors among Female Students at High Schools in Qazvin. J. Health Lit. 2019, 4, 18–26. [Google Scholar]
- Lam, L.T.; Yang, L. Is Low Health Literacy Associated with Overweight and Obesity in Adolescents: An Epidemiology Study in a 12–16 Years Old Population, Nanning, China, 2012. Arch. Public Health 2014, 72, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, A.; Eckert, T.L.; Zaso, M.J.; Scott-Sheldon, L.A.J.; Vanable, P.A.; Carey, K.B.; Ewart, C.K.; Carey, M.P. Associations between Health Literacy and Health Behaviors among Urban High Schoolers. J. Sch. Health 2017, 87, 885. [Google Scholar] [CrossRef] [PubMed]
- Sansom-Daly, U.M.; Lin, M.; Robertson, E.G.; Wakefield, C.E.; McGill, B.C.; Girgis, A.; Cohn, R.J. Health Literacy in Adolescents and Young Adults: An Updated Review. J. Adolesc. Young Adult Oncol. 2016, 5, 106–118. [Google Scholar] [CrossRef] [PubMed]
- Fleary, S.A.; Joseph, P.; Pappagianopoulos, J.E. Adolescent Health Literacy and Health Behaviors: A Systematic Review. J. Adolesc. 2018, 62, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Wallston, K.A.; Wallston, B.S.; DeVellis, R. Development of the Multidimensional Health Locus of Control (MHLC) Scales. Health Educ. Behav. 1978, 6, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Pelikan, J.M.; Röthlin, F.; Ganahl, K. Measuring Comprehensive Health Literacy in General Populations: Validation of Instrument, Indices and Scales of the HLS-EU Study. In Proceedings of the 6th Annual Health Literacy Research Conference, Rockville, MD, USA, 3–4 November 2014. [Google Scholar]
- Reid, A.L.; Porter, K.J.; You, W.; Kirkpatrick, B.M.; Yuhas, M.; Vaught, S.S.; Zoellner, J.M. Low Health Literacy Is Associated With Energy-Balance-Related Behaviors, Quality of Life, and BMI Among Rural Appalachian Middle School Students: A Cross-Sectional Study. J. Sch. Health 2021, 91, 608–616. [Google Scholar] [CrossRef]
- Chi, X.; Liang, K.; Chen, S.T.; Huang, Q.; Huang, L.; Yu, Q.; Jiao, C.; Guo, T.; Stubbs, B.; Hossain, M.M.; et al. Mental Health Problems among Chinese Adolescents during the COVID-19: The Importance of Nutrition and Physical Activity. Int. J. Clin. Health Psychol. 2021, 21, 100218. [Google Scholar] [CrossRef]
- Wright, L.J.; Williams, S.E.; van Zanten, J.J.C.S.V. Physical Activity Protects Against the Negative Impact of Coronavirus Fear on Adolescent Mental Health and Well-Being During the COVID-19 Pandemic. Front. Psychol. 2021, 12, 737. [Google Scholar] [CrossRef] [PubMed]
- Ruíz-Roso, M.B.; de Carvalho Padilha, P.; Matilla-Escalante, D.C.; Brun, P.; Ulloa, N.; Acevedo-Correa, D.; Ferreira Peres, W.A.; Martorell, M.; Bousquet Carrilho, T.R.; De Oliveira Cardoso, L.; et al. Changes of Physical Activity and Ultra-Processed Food Consumption in Adolescents from Different Countries during Covid-19 Pandemic: An Observational Study. Nutrients 2020, 12, 2289. [Google Scholar] [CrossRef]
- Zenic, N.; Taiar, R.; Gilic, B.; Blazevic, M.; Maric, D.; Pojskic, H.; Sekulic, D. Levels and Changes of Physical Activity in Adolescents during the COVID-19 Pandemic: Contextualizing Urban vs. Rural Living Environment. Appl. Sci. 2020, 10, 3997. [Google Scholar] [CrossRef]
- Bates, L.C.; Zieff, G.; Stanford, K.; Moore, J.B.; Kerr, Z.Y.; Hanson, E.D.; Gibbs, B.B.; Kline, C.E.; Stoner, L. COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep. Children 2020, 7, 138. [Google Scholar] [CrossRef] [PubMed]
- Rossi, L.; Behme, N.; Breuer, C. Physical Activity of Children and Adolescents during the COVID-19 Pandemic—A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 11440. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, D.; Ostojic, D.; Decelis, A.; Castro-Piñero, J.; Jezdimirovic, T.; Drid, P.; Ostojic, L.; Gilic, B. The Impact of Scholastic Factors on Physical Activity Levels during the COVID-19 Lockdown: A Prospective Study on Adolescents from Bosnia and Herzegovina. Children 2021, 8, 877. [Google Scholar] [CrossRef]
- Manganello, J.A. Health Literacy and Adolescents: A Framework and Agenda for Future Research. Health Educ. Res. 2008, 23, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Nielsen-Bohlman, L.; Panzer, A.; Kindig, D. Health Literacy: A Prescription to End Confusion; Nielsen-Bohlman, L., Panzer, A.M., Kindig, D.A., Eds.; National Academies Press: Washington, DC, USA, 2004; ISBN 978-0-309-28332-8. [Google Scholar]
- Bronfenbrenner, U. The Ecology of Human Development: Experiments by Nature and Design; Harvard University Press: Cambridge, MA, USA, 1979. [Google Scholar]
- Guo, S.; Naccarella, L.; Yu, X.; Armstrong, R.; Browne, G.; Shi, Y.; Davis, E. Health Literacy and Its Mediating Role in Predicting Health Behaviors Among Chinese Secondary Students. Asia-Pac. J. Public Health 2021, 33, 76–83. [Google Scholar] [CrossRef]
- Bröder, J.; Okan, O.; Bauer, U.; Bollweg, T.M.; Bruland, D.; Pinheiro, P. Child and Youth Health Literacy: A Conceptual Analysis and Proposed Target-Group-Centred Definition. Int. J. Environ. Res. Public Health 2019, 16, 3417. [Google Scholar] [CrossRef] [Green Version]
- Thomas, Y.; Srinivasan, R. Emerging Shifts in Learning Paradigms—From Millenials to the Digital Natives. Int. J. Appl. Eng. Res. 2016, 5, 3616–3618. [Google Scholar]
- Domanska, O.M.; Firnges, C.; Bollweg, T.M.; Sørensen, K.; Holmberg, C.; Jordan, S. Do Adolescents Understand the Items of the European Health Literacy Survey Questionnaire (HLS-EU-Q47)—German Version? Findings from Cognitive Interviews of the Project “Measurement of Health Literacy Among Adolescents” (MOHLAA) in Germany. Arch. Public Health 2018, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| HL Index | Cronbach-α Coefficient | Guttman Split-Half Coefficient |
|---|---|---|
| AI-HL | 0.831 | 0.750 |
| UI-HL | 0.812 | 0.762 |
| ApI-HL | 0.851 | 0.802 |
| UsI-HL | 0.814 | 0.690 |
| HC-HL | 0.856 | 0.790 |
| DP-HL | 0.875 | 0.752 |
| HP-HL | 0.889 | 0.824 |
| General HL | 0.950 | 0.882 |
| Variable | Categories | % | n |
|---|---|---|---|
| Gender | female | 66.3 | 1457 |
| male | 33.7 | 741 | |
| Class at school | I class | 37.0 | 809 |
| II class | 28.8 | 630 | |
| III or IV class | 34.2 | 748 | |
| Type of school | general education | 82.3 | 1829 |
| providing vocational training | 17.7 | 393 | |
| Education level of mother | primary or vocational | 24.5 | 540 |
| secondary | 37.4 | 825 | |
| University education | 38.2 | 844 | |
| Education level of father | primary or vocational | 40.1 | 540 |
| secondary | 33.1 | 825 | |
| University education | 26.8 | 844 | |
| Marital status of parents | married | 86.6 | 1918 |
| divorced or in separation | 10.2 | 227 | |
| one or both parents | 3.2 | 71 | |
| Number of household members | <3 household members | 4.2 | 93 |
| 3 | 16.7 | 370 | |
| 4 | 33.3 | 734 | |
| 5 | 22.1 | 487 | |
| 6 | 13.3 | 294 | |
| 7 | 5.7 | 126 | |
| >7 | 4.7 | 103 | |
| Place of residence | rural | 51.5 | 1142 |
| urban ≤ 10,000 | 6.0 | 132 | |
| urban > 10,000 to 200,000 | 19.3 | 427 | |
| urban > 200,000 | 23.2 | 515 | |
| Size of accommodation | ≤50 m2 | 9.7 | 213 |
| >50 m2–70 m2 | 15.4 | 339 | |
| >70 m2–90 m2 | 11.6 | 255 | |
| >90 m2 | 63.3 | 1393 | |
| Monthly expenses on mobile phone | <5 PLN | 5.1 | 112 |
| 5–<10 PLN | 6.6 | 144 | |
| 10–<30 PLN | 32.6 | 716 | |
| 30–<50 PLN | 34.0 | 747 | |
| ≥50 PLN | 21.7 | 475 | |
| Receiving external support | no | 45.4 | 972 |
| yes | 54.6 | 1170 | |
| Self-assessed economic situation | very bad, bad or average | 13.8 | 305 |
| good | 53.4 | 1177 | |
| very good | 32.8 | 722 | |
| Number of books at home | ≤25 | 12.4 | 272 |
| 26–50 | 17.9 | 393 | |
| 51–100 | 27.5 | 605 | |
| 101–500 | 32.7 | 719 | |
| >500 | 9.5 | 209 | |
| Weekly duration of Internet use | ≥2 h | 9.1 | 202 |
| >2–7 h | 20.4 | 454 | |
| >7–14 h | 18.3 | 405 | |
| >14–21 h | 16.3 | 361 | |
| >21–35 h | 16.0 | 354 | |
| >35 h | 19.9 | 440 | |
| Health literacy | inadequate | 4.6 | 96 |
| problematic | 36.8 | 766 | |
| sufficient | 45.2 | 942 | |
| excellent | 13.4 | 278 |
| Variable | Categories | OR | 95% CI | p | aOR | a95% CI | p |
|---|---|---|---|---|---|---|---|
| Gender | female * | ||||||
| male | 0.87 | 0.72–1.05 | 0.143 | ||||
| Class at school | I class * | ||||||
| II class | 1.03 | 0.82–1.28 | 0.818 | ||||
| III or IV class | 1.22 | 0.99–1.51 | 0.059 | ||||
| Type of school | GE * | ||||||
| with VT | 1.15 | 0.92–1.45 | 0.216 | ||||
| Education level of mother # | primary or vocational * | ||||||
| secondary | 0.97 | 0.78–1.22 | 0.821 | 0.93 | 0.72–1.21 | 0.934 | |
| University | 0.73 | 0.58–0.92 | 0.007 | 0.74 | 0.55–0.98 | 0.038 | |
| Education level of father # | primary or vocational * | ||||||
| secondary | 1.10 | 0.89–1.35 | 0.381 | 1.32 | 1.04–1.67 | 0.022 | |
| University | 0.80 | 0.64–0.99 | 0.047 | 1.12 | 0.84–1.50 | 0.424 | |
| Marital status of parents | married * | ||||||
| divorced or separated | 1.10 | 0.83–1.46 | 0.514 | ||||
| one or both parents | 1.04 | 0.64–1.70 | 0.865 | ||||
| Number of household members | <3 household members * | ||||||
| 3 | 1.20 | 0.74–1.94 | 0.461 | ||||
| 4 | 1.10 | 0.70–1.74 | 0.684 | ||||
| 5 | 1.18 | 0.73–1.89 | 0.497 | ||||
| 6 | 1.21 | 0.74–1.98 | 0.452 | ||||
| 7 | 1.16 | 0.65–2.04 | 0.620 | ||||
| >7 | 1.35 | 0.74–2.44 | 0.326 | ||||
| Place of residence | rural * | ||||||
| urban ≤ 10,000 | 0.96 | 0.65–1.40 | 0.826 | ||||
| urban > 10,000 to 200,000 | 0.97 | 0.76–1.22 | 0.767 | ||||
| urban > 200,000 | 1.06 | 0.85–1.31 | 0.622 | ||||
| Size of accommodation # | ≤50 m2 * | ||||||
| >50 m2–70 m2 | 0.93 | 0.65–1.33 | 0.686 | 1.08 | 0.73–1.58 | 0.714 | |
| >70 m2–90 m2 | 0.58 | 0.39–0.85 | 0.005 | 0.66 | 0.43–0.998 | 0.049 | |
| >90 m2 | 0.74 | 0.54–0.99 | 0.045 | 0.92 | 0.66–1.28 | 0.920 | |
| Monthly expenses on mobile phone # | ≤5 PLN * | ||||||
| >5–10 PLN | 0.63 | 0.37–1.06 | 0.082 | 0.64 | 0.37–1.12 | 0.116 | |
| >10–30 PLN | 0.80 | 0.52–1.21 | 0.286 | 0.85 | 0.55–1.33 | 0.481 | |
| >30–50 PLN | 0.79 | 0.52–1.20 | 0.277 | 0.89 | 0.58–1.39 | 0.612 | |
| >50 PLN | 0.62 | 0.40–0.95 | 0.030 | 0.70 | 0.44–1.11 | 0.126 | |
| Receiving external support # | no * | ||||||
| yes | 0.81 | 0.68–0.97 | 0.021 | 0.88 | 0.73–1.07 | 0.198 | |
| Self-assessed economic situation # | worse than good * | ||||||
| good | 0.59 | 0.46–0.77 | 0.000 | 0.65 | 0.49–0.86 | 0.003 | |
| very good | 0.37 | 0.28–0.49 | 0.000 | 0.43 | 0.32–0.59 | <0.001 | |
| Number of books at home # | ≤25 * | ||||||
| 26–50 | 1.24 | 0.89–1.72 | 0.196 | 1.19 | 0.84–1.68 | 0.331 | |
| 51–100 | 1.03 | 0.76–1.39 | 0.870 | 1.03 | 0.75–1.42 | 0.861 | |
| 101–500 | 1.03 | 0.76–1.38 | 0.866 | 1.11 | 0.80–1.53 | 0.530 | |
| >500 | 0.66 | 0.44–0.98 | 0.038 | 0.79 | 0.52–1.21 | 0.278 | |
| Weekly duration of Internet use | not more than 2 h * | ||||||
| >2–7 h | 1.12 | 0.79–1.59 | 0.518 | ||||
| >7–14 | 1.23 | 0.86–1.75 | 0.259 | ||||
| >14–21 | 1.18 | 0.82–1.69 | 0.381 | ||||
| >21–35 | 0.90 | 0.62–1.30 | 0.566 | ||||
| >35 h | 1.22 | 0.86–1.74 | 0.259 |
| Variable | Categories | AI-HL | UI-HL | ||
|---|---|---|---|---|---|
| B(SE) | p | B(SE) | p | ||
| Gender | male vs. female | 0.96 (0.32) | 0.002 | −0.10 (0.32) | 0.763 |
| Class at school | I class * | ||||
| II class | 0.28 (0.38) | 0.449 | 0.7 (0.37) | 0.062 | |
| III or IV class | −0.54 (0.36) | 0.125 | 0.14 (0.36) | 0.690 | |
| Type of school | with VT vs. GE | −0.30 (0.39) | 0.437 | −1.18 (0.39) | 0.002 |
| Education level of mother | secondary * | ||||
| primary or voc. | 0.16 (0.39) | 0.682 | 0.11 (0.39) | 0.785 | |
| University | 1.15 (0.34) | 0.001 | 1.13 (0.34) | 0.001 | |
| Education level of father | primary or voc. * | ||||
| secondary | −0.03 (0.35) | 0.939 | −0.64 (0.35) | 0.070 | |
| University | 0.88 (0.37) | 0.019 | 0.91 (0.37) | 0.014 | |
| Marital status of parents | married * | ||||
| div. or in sep. | −0.79 (0.49) | 0.107 | −0.14 (0.49) | 0.775 | |
| one or both parents deceased | −0.35 (0.83) | 0.672 | 0.39 (0.84) | 0.641 | |
| Number of household members | 4 * | ||||
| <3 | 0.12 (0.79) | 0.876 | 0.38 (0.77) | 0.625 | |
| 3 | −0.11 (0.45) | 0.805 | −0.12 (0.44) | 0.788 | |
| 5 | −0.35 (0.41) | 0.399 | −0.26 (0.41) | 0.521 | |
| 6 | −0.33 (0.49) | 0.502 | 0.01 (0.49) | 0.992 | |
| 7 | −0.37 (0.68) | 0.585 | −0.69 (0.68) | 0.314 | |
| >7 | 0.09 (0.73) | 0.898 | −0.08 (0.76) | 0.920 | |
| Place of residence | rural * | ||||
| urban ≤ 10,000 | 0.47 (0.65) | 0.467 | 0.33 (0.64) | 0.607 | |
| urban > 10,000 to 200,000 | −0.07 (0.40) | 0.869 | 0.17 (0.40) | 0.671 | |
| urban >200,000 | −0.37 (0.37) | 0.325 | 0.49 (0.37) | 0.186 | |
| Size of accommodation | ≤50 m2 * | ||||
| >50 m2–70 m2 | −0.86 (0.61) | 0.159 | 0.01 (0.61) | 0.989 | |
| >70 m2–90 m2 | 0.96 (0.58) | 0.097 | 0.7 (0.58) | 0.226 | |
| >90 m2 | 0.96 (0.42) | 0.021 | 0.35 (0.42) | 0.405 | |
| Monthly expenses on mobile phone | 30–<50 PLN * | ||||
| <5 PLN | −1.49 (0.74) | 0.044 | −1.47 (0.71) | 0.039 | |
| 5–<10 PLN | 0.64 (0.64) | 0.320 | 0.37 (0.63) | 0.556 | |
| 10–<30 PLN | 0.05 (0.37) | 0.889 | −0.13 (0.37) | 0.733 | |
| from 50 PLN | 1 (0.41) | 0.014 | 0.07 (0.41) | 0.868 | |
| Receiving external support | yes vs. no | 0.28 (0.3) | 0.358 | 0.6 (0.3) | 0.050 |
| Self-assessed economic situation | good | ||||
| worse than good | −1.44 (0.44) | 0.001 | −0.38 (0.45) | 0.400 | |
| very good | 2.01 (0.33) | <0.001 | 1.36 (0.33) | <0.001 | |
| Number of books at home | 101–500 * | ||||
| ≤25 | 0.16 (0.50) | 0.751 | −0.53 (0.5) | 0.295 | |
| 26–50 | −0.75 (0.44) | 0.089 | −0.79 (0.44) | 0.071 | |
| 51–100 | −0.01 (0.39) | 0.984 | −0.29 (0.38) | 0.457 | |
| >500 | 0.93 (0.55) | 0.088 | 1.57 (0.55) | 0.004 | |
| Weekly duration of Internet use | >2–7 h * | ||||
| ≤2 h | 0.61 (0.59) | 0.300 | 0.51 (0.59) | 0.385 | |
| >7–14 | −0.36 (0.48) | 0.453 | −0.52 (0.48) | 0.281 | |
| >14–21 | −0.04 (0.50) | 0.943 | −0.16 (0.5) | 0.752 | |
| >21–35 | 0.77 (0.50) | 0.120 | 0.15 (0.5) | 0.768 | |
| >35 h | 0.37 (0.47) | 0.429 | −0.13 (0.47) | 0.790 | |
| Variable | Categories | ApI-HL | UsI-HL | ||
|---|---|---|---|---|---|
| B(SE) | p | B(SE) | p | ||
| Gender | male vs. female | 0.7 (0.35) | 0.045 | 0.22 (0.33) | 0.495 |
| Class at school | I class * | ||||
| II class | 0.28 (0.41) | 0.500 | −0.04 (0.39) | 0.912 | |
| III or IV class | 0.05 (0.39) | 0.895 | −0.67 (0.37) | 0.067 | |
| Type of school | with VT vs. GE | −0.20 (0.43) | 0.645 | −0.05 (0.4) | 0.904 |
| Education level of mother | secondary * | ||||
| primary or voc. | −0.17 (0.43) | 0.692 | 0.08 (0.40) | 0.833 | |
| University | 1.19 (0.38) | 0.002 | 0.99 (0.35) | 0.005 | |
| Education level of father | primary or voc. * | ||||
| secondary | −0.72 (0.39) | 0.066 | −0.21 (0.36) | 0.573 | |
| University | 0.70 (0.41) | 0.090 | 0.31 (0.39) | 0.426 | |
| Marital status of parents | married * | ||||
| div or in sep. | −0.06 (0.54) | 0.906 | −0.48 (0.5) | 0.340 | |
| one or both parents deceased | −0.13 (0.93) | 0.890 | −0.09 (0.87) | 0.920 | |
| Number of household members | 4 * | ||||
| <3 | 0.95 (0.84) | 0.259 | 0 (0.79) | 0.999 | |
| 3 | 0.29 (0.49) | 0.557 | 0.05 (0.46) | 0.921 | |
| 5 | −0.22 (0.45) | 0.623 | −0.51 (0.42) | 0.226 | |
| 6 | −0.19 (0.54) | 0.723 | 0.03 (0.50) | 0.952 | |
| 7 | −0.55 (0.75) | 0.463 | −0.17 (0.71) | 0.814 | |
| >7 | 0.44 (0.83) | 0.598 | −0.23 (0.78) | 0.768 | |
| Place of residence | rural | ||||
| urban ≤ 10,000 | 0.35 (0.72) | 0.625 | −0.35 (0.67) | 0.598 | |
| urban > 10,000 to 200,000 | −0.30 (0.44) | 0.495 | −0.05 (0.41) | 0.909 | |
| urban > 200,000 | −0.11 (0.41) | 0.797 | −0.06 (0.38) | 0.871 | |
| Size of accommodation | ≤50 m2 * | ||||
| >50 m2–70 m2 | −0.09 (0.68) | 0.894 | 0.23 (0.64) | 0.713 | |
| >70 m2–90 m2 | 1.25 (0.64) | 0.052 | 0.91 (0.6) | 0.127 | |
| >90 m2 | 0.67 (0.47) | 0.151 | 0.93 (0.44) | 0.033 | |
| Monthly expenses on mobile phone | 30–<50 PLN * | ||||
| <5 PLN | −0.89 (0.79) | 0.262 | −2.11 (0.75) | 0.005 | |
| 5–<10 PLN | 0.39 (0.7) | 0.578 | −0.12 (0.66) | 0.855 | |
| 10–<30 PLN | −0.24 (0.4) | 0.545 | −0.28 (0.38) | 0.458 | |
| from 50 PLN | 1.04 (0.45) | 0.021 | 0.81 (0.42) | 0.056 | |
| Receiving external support | yes vs. no | 0.77 (0.34) | 0.023 | 0.54 (0.32) | 0.086 |
| Self-assessed economic situation | good * | ||||
| worse than good | −1.35 (0.49) | 0.006 | −1.28 (0.46) | 0.005 | |
| very good | 2.25 (0.36) | <0.001 | 2.24 (0.34) | <0.001 | |
| Number of books at home | 101–500 * | ||||
| ≤25 | 0.27 (0.55) | 0.625 | 0.31 (0.52) | 0.551 | |
| 26–50 | −0.82 (0.48) | 0.089 | −0.23 (0.45) | 0.612 | |
| 51–100 | −0.03 (0.43) | 0.939 | <0.001 (0.40) | 0.999 | |
| >500 | 2.26 (0.61) | <0.001 | 1.48 (0.57) | 0.010 | |
| Weekly duration of Internet use | >2–7 h * | ||||
| ≤2 h | 0.39 (0.66) | 0.552 | −0.2 (0.61) | 0.745 | |
| >7–14 | −0.56 (0.53) | 0.285 | −0.5 (0.49) | 0.311 | |
| >14–21 | −0.57 (0.55) | 0.294 | −0.62 (0.51) | 0.226 | |
| >21–35 | 0.51 (0.55) | 0.354 | −0.33 (0.51) | 0.517 | |
| >35 h | 0.12 (0.52) | 0.813 | −0.16 (0.49) | 0.740 | |
| Variable | Categories | HC-HL | DP-HL | HP-HL | |||
|---|---|---|---|---|---|---|---|
| B(SE) | p | B(SE) | p | B(SE) | p | ||
| Gender | male vs. female | 0.07 (0.29) | 0.818 | 0.62 (0.35) | 0.073 | 0.68 (0.35) | 0.051 |
| Class at school | I class * | ||||||
| II class | 0.36 (0.34) | 0.290 | 0.18 (0.41) | 0.661 | 0.11 (0.41) | 0.786 | |
| III or IV class | −0.03 (0.32) | 0.923 | 0.09 (0.39) | 0.817 | −0.93 (0.39) | 0.017 | |
| Type of school | with VT vs. GE | −0.54 (0.35) | 0.123 | −0.67 (0.42) | 0.112 | 0.04 (0.43) | 0.924 |
| Education level of mother | secondary * | ||||||
| primary or voc. | 0.12 (0.35) | 0.733 | 0.08 (0.43) | 0.856 | 0.03 (0.43) | 0.949 | |
| University | 0.65 (0.31) | 0.035 | 1.53 (0.37) | <0.001 | 1.19 (0.38) | 0.002 | |
| Education level of father | primary or voc. * | ||||||
| secondary | −0.4 (0.32) | 0.211 | −0.52 (0.38) | 0.179 | −0.34 (0.39) | 0.374 | |
| University | 0.64 (0.34) | 0.057 | 1.29 (0.41) | 0.002 | 0.35 (0.41) | 0.401 | |
| Marital status of parents | married * | ||||||
| div or in sep. | −0.23 (0.44) | 0.592 | −0.85 (0.53) | 0.109 | 0.2 (0.53) | 0.706 | |
| one or both parents deceased | −0.53 (0.76) | 0.483 | −0.19 (0.96) | 0.842 | 0.95 (0.93) | 0.307 | |
| Number of household members | 4 * | ||||||
| <3 | 0.25 (0.7) | 0.718 | 0.8 (0.86) | 0.352 | 0.75 (0.86) | 0.383 | |
| 3 | −0.12 (0.4) | 0.769 | 0.08 (0.49) | 0.874 | 0.17 (0.49) | 0.727 | |
| 5 | −0.54 (0.37) | 0.146 | −0.08 (0.45) | 0.862 | −0.12 (0.45) | 0.793 | |
| 6 | 0.08 (0.44) | 0.861 | −0.1 (0.53) | 0.845 | −0.23 (0.54) | 0.675 | |
| 7 | −0.53 (0.61) | 0.384 | −0.14 (0.75) | 0.854 | −0.03 (0.75) | 0.968 | |
| >7 | −0.13 (0.69) | 0.850 | 0.18 (0.81) | 0.826 | 0.60 (0.83) | 0.465 | |
| Place of residence | rural * | ||||||
| urban ≤ 10,000 | 0.05 (0.59) | 0.933 | 0.37 (0.71) | 0.606 | 0.2 (0.71) | 0.780 | |
| urban > 10,000 to 200,000 | 0.07 (0.36) | 0.851 | −0.03 (0.44) | 0.940 | −0.25 (0.44) | 0.561 | |
| urban >200,000 | 0.12 (0.33) | 0.730 | −0.03 (0.41) | 0.939 | −0.25 (0.41) | 0.535 | |
| Size of accommodation | ≤50 m2 * | ||||||
| >50 m2–70 m2 | 0.72 (0.55) | 0.193 | −1.17 (0.67) | 0.08 | −0.56 (0.68) | 0.408 | |
| >70 m2–90 m2 | 1.47 (0.52) | 0.005 | 0.37 (0.63) | 0.554 | 0.70 (0.63) | 0.268 | |
| >90 m2 | 0.92 (0.38) | 0.015 | 0.39 (0.46) | 0.407 | 0.56 (0.46) | 0.226 | |
| Monthly expenses on mobile phone | 30–<50 PLN * | ||||||
| <5 PLN | −1.02 (0.65) | 0.115 | −1.24 (0.8) | 0.121 | −2.41 (0.79) | 0.002 | |
| 5–<10 PLN | 0.53 (0.58) | 0.357 | 0.79 (0.7) | 0.263 | 0.1 (0.70) | 0.883 | |
| 10–<30 PLN | −0.41 (0.33) | 0.218 | 0.19 (0.4) | 0.646 | −0.36 (0.40) | 0.365 | |
| from 50 PLN | 0.76 (0.37) | 0.040 | 0.69 (0.45) | 0.124 | 0.69 (0.45) | 0.124 | |
| Receiving external support | yes vs. no | 0.68 (0.27) | 0.014 | 0.52 (0.33) | 0.118 | 0.31 (0.33) | 0.360 |
| Self-assessed economic situation | good * | ||||||
| worse than good | −0.56 (0.4) | 0.163 | −1.27 (0.48) | 0.009 | −1.77 (0.48) | <0.001 | |
| very good | 1.87 (0.29) | <0.001 | 1.95 (0.36) | <0.001 | 1.89 (0.36) | <0.001 | |
| Number of books at home | 101–500 * | ||||||
| ≤25 | −0.59 (0.45) | 0.187 | −0.20 (0.55) | 0.714 | 0.80 (0.55) | 0.147 | |
| 26–50 | −0.68 (0.40) | 0.088 | −1.10 (0.48) | 0.021 | −0.45 (0.48) | 0.349 | |
| 51–100 | −0.21 (0.35) | 0.547 | −0.46 (0.42) | 0.282 | 0.47 (0.42) | 0.267 | |
| >500 | 1.47 (0.50) | 0.003 | 1.60 (0.60) | 0.007 | 1.51 (0.6) | 0.012 | |
| Weekly duration of Internet use | >2–7 h * | ||||||
| ≤2 h | 0.48 (0.53) | 0.373 | 0.14 (0.65) | 0.827 | 0.80 (0.65) | 0.216 | |
| >7–14 | −0.47 (0.43) | 0.278 | 0.06 (0.51) | 0.900 | −0.64 (0.53) | 0.226 | |
| >14–21 | −0.13 (0.45) | 0.771 | −0.54 (0.53) | 0.309 | −0.69 (0.54) | 0.205 | |
| >21–35 | 0.24 (0.45) | 0.591 | −0.28 (0.55) | 0.608 | 0.03 (0.54) | 0.952 | |
| >35 h | 0.13 (0.42) | 0.763 | 0.58 (0.55) | 0.291 | 0.20 (0.52) | 0.703 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duplaga, M.; Grysztar, M. Socio-Economic Determinants of Health Literacy in High School Students: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 12231. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212231
Duplaga M, Grysztar M. Socio-Economic Determinants of Health Literacy in High School Students: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(22):12231. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212231
Chicago/Turabian StyleDuplaga, Mariusz, and Marcin Grysztar. 2021. "Socio-Economic Determinants of Health Literacy in High School Students: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 22: 12231. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182212231