
Oral Health-Related Quality of Life in Adolescents as Measured with the Child-OIDP Questionnaire: A Systematic Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Selection Process
2.4. Data Collection Process and Variables
2.5. Risk of Bias in Individual Studies and Quality Assessment

{kind=link}
| Author Year Country | Study’s Aim | Sample Selection Method Sample Size (n) | Age Range Sex (%) | Questionnaire (OHRQoL) Completion Mode Administration Context | Type of Intervention | Sample’s Inclusion and Exclusion Criteria | Results (Impact Prevalence; Mean C-OIDP Score) | Quality of Study (FLC 3.0/ STROBE Cross-Sectional Studies) |
|---|---|---|---|---|---|---|---|---|
| Alzahrani et al., 2019 Saudi Arabia [26] | To examine the associations between the OHRQoL based on the Child-OIDP index and the different oral diseases among Saudi schoolchildren living in the Albaha region of Saudi Arabia. | Two-stage randomized sampling technique n = 349 | 12–15 years old Male: 100 | C-OIDP Interview Three intermediate schools | Questionnaire Oral clinical examination | Inclusion: Physically and mentally fit for this study; parent’s written informed consent. Exclusion: Histories of antibiotic therapy and/or systemic diseases during the previous three months; female schoolchildren. | Impact prevalence: 75.1% Mean C-OIDP score: 2.5 | Medium/18 |
| Bakhtiar et al. 2014 Iran [27] | To assess the association between OHRQoL and clinical oral health measures among mid-level school children in the city of Kerman, Southeast of Iran and also, answer this question whether the status of oral health can modify OIDP index in adolescents. | Random Cluster Sample n = 400 | 11–13 years-old Male: 46.75 Female: 53.25 | C-OIDP Self-completed part Interview Mid-level schools | Questionnaire Oral clinical examination | Exclusion: serious medical problem and any condition influencing on their quality-of-life and also their oral health like orthodontic treatment. | Impact prevalence: 82% Mean C-OIDP score: 10.2 C-OIDP score: 7.1 | Medium/16 |
| Basavaraj et al., 2014 India [28] | To investigate whether a relationship exists between specific clinical dental measures and OHRQoL using the Child-OIDP index among children attending various schools located in Modinagar, India. | Two-stage cluster sampling technique n = 900 | 12 and 15 years old Male: 67 Female: 33 576 (64%): 12 years (385: males, 191: females) 324 (36%): 15 years (218: males, 106: females) | C-OIDP Interviewer-administered Six public and ten private middle and high schools | Questionnaire Oral clinical examination | Inclusion: 12 and 15 years old, attending various schools in Modinagar. Exclusion: Systemic diseases and on antibiotic therapy in the previous six months. | Impact prevalence: 60% Mean C-OIDP score: 2.49 | High/20 |
| Castro et al., 2011 Brazil [29] | To assess the association between OHRQoL, measured through the Child-OIDP, and demographic characteristics, self-reported oral problems and clinical oral health measures among 11- to 12-year-old schoolchildren in the city of Rio de Janeiro, Brazil. | Probabilistic sample with complex design n = 571 | 11–12 years old Male: 38.6 Female: 61.4 | C-OIDP Self-administrated part (refers to list of pathologies) Face-to-face interview part Six to seven years of public education | Questionnaire Oral clinical examination | Inclusion: Year 6 and 7 classes, 11 and 12 years old, both sexes, formally enrolled in the public educational system of the city of Rio de Janeiro, parent’s informed consent. | Impact prevalence: 88.7% Mean C-OIDP score: 7.1 | Medium/16 |
| Do et al., 2020 Vietnam [30] | To assess the impact of oral health problems on daily activities of 12- and 15-year-old children in Can Tho. | Cluster sampling of probability proportional to size n = 809 n = 407 children of 12 years old n = 402 children of 15 years old | 12–15 years old Sex: Not stated | C-OIDP Self-administrated part (refers to list of pathologies) Questionnaire: Interview administrated under the guidance and interpretation of the investigators Ten secondary schools (six schools in urban and four in rural areas) | Questionnaire | Inclusion: 12–15 years old, informed consent, year 6 to 9 classes. | Impact prevalence: 87–78.6% Mean C-OIDP score: 9.1–5.6 | High/17 |
| Dumitrache et al., 2009 Romania [31] | To assess the prevalence and severity of the oral health impact on the quality of life of schoolchildren in Bucharest using the Child-OIDP index. | Random selection n = 413 | 11–13 years old Male: 47 Female: 53 | C-OIDP interview administrated Six schools | Questionnaire Oral clinical examination | Inclusion: 11–13 years, randomly selected from six schools from the six-city district, parents’ and school officials’ written consent. | Impact prevalence: 57.4% Mean C-OIDP score: Not stated | Low/14 |
| Kumar et al., 2015 India [32] | To evaluate the psychometric properties of the Hindi version of the Child-OIDP and to estimate the oral impacts on daily performance in 12–15-year-old public and private schoolchildren. This article also aimed to determine the prevalence of dental caries in this age group. | Two-stage stratified cluster random sampling n = 690 | 12–15 years old Male: 50.724 Female: 49.28 | C-OIDP Self-administrated Four private and four public schools | Questionnaire Oral clinical examination | Inclusion: Present on the day of examination. Exclusion: Not willing to participate, absent, suffering from any systemic disease that contradicts oral examination. | Impact prevalence: 36.5% Mean C-OIDP score for eating: 2.5 | Medium/17 |
| Moreno Ruiz et al., 2014 Chile [33] | To evaluate the oral health-related quality of life using the Child-OIDP index in schoolchildren from 11–14 years old in Licantén, 2013. | Sample selection method not stated n = 203 | 11–14 years old Male: 48.3 Female: 52.7 | C-OIDP Self-administrated The only school and high school | Questionnaire | Inclusion: Between first grade and fifth grade. | Impact prevalence: 68% Mean C-OIDP score: 6.92 | Medium/15 |
| Paredes- Martínez et al., 2014 Peru [34] | To determine how oral conditions impact the quality of life related to oral health (HRQL) in a group of 11 and 12-year-old schoolchildren from the district of San Juan de Miraflores, Lima, in 2013. | Sample selection method not stated n = 169 | 11–12 years old Male: 49.7 Female: 50.3 | C-OIDP Self-completion: List of pathologies Interview administered Educational institution | Questionnaire | Inclusion: 11 and 12-year-old schoolchildren, apparently healthy, both sexes, with authorization from the educational institution, parents’ and children’s informed consent. Exclusion: Uncorrected visual and hearing disabilities. | Impact prevalence: 100% Mean C-OIDP score: Not stated | Medium/16 |
| Pavithran et al., 2020 India [35] | To assess and compare the oral health status and impact of oral diseases on daily activities among 12 to 15-year-old institutionalized orphans and non-orphan children in Bengaluru. | Simple random sampling technique for orphanage participants. Convenience selection for non-orphanage participants. n = 420 | 12–15 years old Male orphans: 51 Female orphans: 49 Male non–orphans: 50.5 Female non–orphans: 49.5 | C-OIDP Guided interviews 15 orphanages and 15 government schools | Questionnaire Oral clinical examination | Inclusion: Orphans aged 12–15 years old, consent by institutional authorities; non–orphans aged 12–15 years old with parent/guardian’s informed consent. Exclusion: Any long–standing systemic disease, physical disability, or mixed dentition. | Impact prevalence: 76.3% orphans, 65.7% non-orphans Mean C-OIDP score: 3.9 orphans, 2.8 non-orphans | High/18 |
| Vélez- Vásquez et al., 2019 Ecuador [36] | To associate the level of dental caries experience with the level of impact of oral conditions on the quality of life related to oral health. | Random sample n = 118 | 11–12 years old Male: 47.45 Female: 52.54 | C-OIDP Interview Educational institutions | Questionnaire Oral clinical examination | Inclusion: 11- and 12-year-old schoolchildren from the educational centers of the parish of Machángara from Cuenca, Ecuador in 2017. | Impact prevalence: 88.1% Mean C-OIDP score: not stated | High/19 |
| Alves et al., 2015 Brazil [37] | To use normative methods to compare dental caries need with the socio-dental approach in 12-year-old adolescents according to family’s living conditions in a deprived community in Brazil. | Random sampling technique n = 159 | 12 years old Male: 49.1 Female: 50.9 | C-OIDP CS-C-OIDP Self-administration Face-to-face Primary healthcare (PHC) | Questionnaires Oral clinical examination | Inclusion: Living in the areas covered by the primary healthcare system of the Manguinhos community for at least six months. Exclusion: Unable to answer the questionnaire. | Impact prevalence (Generic C-OIDP): 76.1% Impact prevalence (CS-Child–OIDP): 64.8% Mean C-OIDP score: 9.66 (generic) Mean C-OIDP score: 10.95 (specific) | Medium/17 |
| Bernabé et al., 2007 Peru [38] | To determine the prevalence, intensity and extent of the impacts of oral problems in a sample of Peruvian 11–12-year-old schoolchildren, and to compare the intensity and extent of the impacts by the type of self-perceived oral problem. | Random selection n = 805 | 11–12 years old Male: 48.8 Female: 51.2 | C-OIDP Individual face-to-face interview First question self-administrated (refers to list of pathologies) Four public schools linked to a health center | Questionnaire | Inclusion: 11–12-year-olds; parental consent letter; child’s written consent. | Impact prevalence: 82.0% Mean C-OIDP score: 7.8 | Medium/15 |
| Del Castillo- López et al., 2014 Peru [39] | To determine the impact of oral conditions on HRQL, through the Child-OIDP index, in 11- and 12-year-old schoolchildren from the Canchaque and San Miguel de El Faique districts of the Huancabamba province, from the rural area of Piura, in 2010. | Sample selection method not stated n = 150 | 11–12 years old Male: 89 Female: 61 | C-OIDP Self-administrated part Face-to-face interview part Six public educational Institutions (EIs) | Questionnaire | Inclusion: 11–12 years old, healthy students, both sexes, parents’ and children’s signed informed consent. | Impact prevalence: 88.7% Mean C-OIDP score: 7.05 | Medium/17 |
| Marcelo- Inguza et al., 2015 Peru [40] | To measure the impact of oral conditions on the Quality of Life Related to Health (OHRQoL) in schoolchildren aged 11–12 years in the urban-marginal area of Pachacutec-Ventanilla, Callao, Lima in 2013. | Sample selection method not stated n = 132 | 11–12 years old Male: 44 Female: 56 | C-OIDP Self-administrated part (refers to list of pathologies) Face-to-face interview part Primary or secondary level of an educational institution | Questionnaire | Inclusion: 11 and 12 years old, both sexes, parents’ and children’s informed consent, apparently healthy and without any chronic systemic alteration. | Impact prevalence: 100% Mean C-OIDP score: 9.71 | High/17 |
| Naidoo et al., 2013 South Africa [41] | To assess the prevalence, extent and intensity of oral impacts and their relation to perceived clinical conditions in a sample of primary school children in South Africa. | Random sampling method n = 1665 | 11–13 years old Male: 47 Female: 54 | C-OIDP Face-to-face interview 26 primary schools | Questionnaire Oral clinical examination | Inclusion: 11–13 years old, 26 primary schools from amongst all those in the Ugu district, Kwazulu Natal (KZN), South Africa. | Impact prevalence: 36.2% Mean C-OIDP score: Not stated | Medium/18 |
| Nordin et al., 2019 Malaysia [42] | To assess the oral health status, oral health behaviors and OHRQoL among 11–12-year-old OA children in the Cameron Highlands (CH), Malaysia, and to identify factors associated with their OHRQoL. | Sample selection method not stated n = 227 | 11–12 years old Male: 51.5 Female 48.5 | C-OIDP Self-administrated Primary schoolchildren | Questionnaire Oral clinical examination | Exclusion: Absent and without informed consent. | Impact prevalence: 58.6% Mean C-OIDP score: 5.45 | High/17 |
| Reinoso- Vintimilla et al. 2017 Ecuador [43] | Evaluate the impact of oral conditions in quality of life in children between 11 to 12 years old of schools at Sayausí, Cuenca, Ecuador. | Sample selection method not stated n = 359 | 11–12 years-old Male: 52.37 Female: 47.63 | C-OIDP Interview administrated List of pathologies: self-administrated Church’s school | Questionnaire | Inclusion: 11 and 12 years old, in apparent good general health, both sexes, with informed assent, parents informed consent. Exclusion: who did not wish to collaborate and with physical disabilities | Impact prevalence: 98,8% Mean C-OIDP score: not stated | Medium/15 |
| Simangwa et al. 2020 Tanzania [44] | To estimate the prevalence of oral impacts and to identify important clinical- and socio-demographic covariates. In addition, this study compares Maasai and non-Maasai adolescents regarding any association of socio- demographic and clinical covariates with oral impacts on daily performances. | One-stage cluster sample design n = 906 | 12–17 years-old Male: 43.9 Female: 56.1 | C-OIDP Face- to- face interviews 23 Rural public Primary schools | Questionnaire Oral clinical examination | Inclusion: 12 to 14 years old attending rural public primary schools of Monduli and Longido districts. Exclusion: attending urban and private primary schools, absents, difficulties in learning. | Impact prevalence: 15.8% Mean C-OIDP score: not stated | High/18 |
| Amalia et al., 2017 Indonesia [45] | To examine the association between SBDP performance and OHRQoL in primary schoolchildren, while also considering the impact of untreated caries and sociodemographic factors. | Convenience sample n = 1906 | 12 years old Male: 54 Female: 46 | CS-C-OIDP Interview Primary public and private schools | Questionnaire Oral clinical examination | Inclusion: All 12-year-olds from both primary public and private schools. Exclusion: No written informed consent; absent children. | Eating impact prevalence: 42.4% −38.6% Impact prevalence related to caries: 56% Impact prevalence (global): Not stated Mean C-OIDP score: 1.6–6.8 | Medium/16 |
| Athira et al., 2015 India [46] | To determine the association, if any, between OHRQoL measured using the C-OIDP index and clinical oral health measures among 12–17-year-old children of South Bangalore. | Random sampling technique n = 504 | 12–17 years old Male: 48 Female: 52 | C-OIDP Self-administration Five schools | Questionnaire Oral clinical examination | Inclusion: 12–17 years old, males and females, who can read and are ready to answer the questions, fulfill the research criteria, and consent to participate in the study. Exclusion: Did not cooperate with clinical exam; systemic disease. | Eating C-OIDP: 6.9 Impact prevalence: 43.1% Mean C-OIDP score: Not stated | Low/16 |
| Bianco et al., 2009 Italy [47] | To use an oral health-related quality of life (OHRQoL) measure, the Child-Oral Impact on Daily Performance (Child-OIDP), to assess the prevalence, characteristics and severity of oral impacts on health and daily activities in secondary schoolchildren, and to identify determinants such as children’s sociodemographic profile, oral hygiene habits, nutrition practices and oral health conditions, such as dental caries, periodontal diseases and orthodontics, that can predict oral impacts. | Random selection n = 530 | 11–16 years old Male: 47.4 Female: 52.6 | C-OIDP Interview Secondary schools | Questionnaire Oral clinical examination | Inclusion: 11–16-year-olds; parental consent form. | Impact prevalence: 66.8% Mean C-OIDP score: 1.9 | High/18 |
| Yetkiner et al., 2014 Turkey [48] | (1) To determine orthodontic treatment need, self-esteem and OHRQoL of primary schoolchildren, and (2) To investigate possible influences of orthodontic treatment need on OHRQoL and self-esteem. | Sample selection method not stated n = 219 | 13–14 years old Male: 51.60 Female: 48.40 | C-OIDP Self-administrated The sixth year of primary public school | Questionnaire Oral clinical examination | Inclusion: 13–14 years, no history of previous orthodontic treatment, with informed consent. | Impact prevalence: 69.9% Mean C-OIDP score for eating: 3 | Medium/18 |
3. Results
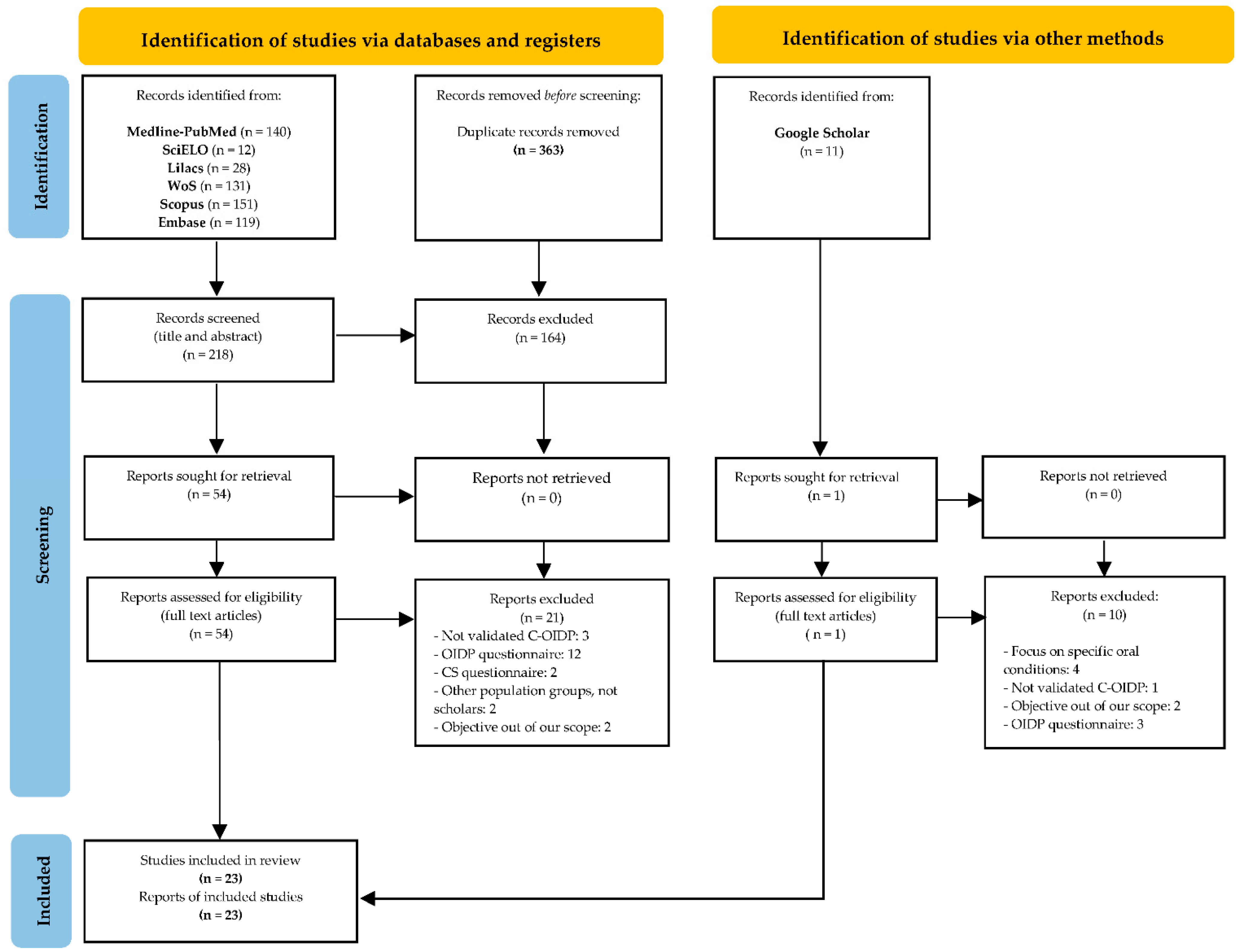
3.1. Study Selection and Flow Diagram
3.2. Qualitative Synthesis
3.2.1. Population (P)
3.2.2. Intervention (I) (Child-OIDP Questionnaire)
3.2.3. Outcome (O)
3.3. Risk of Bias within Studies and Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Hescot, P. The New Definition of Oral Health and Relationship between Oral Health and Quality of Life. Chin. J. Dent. Res. 2017, 20, 189–192. [Google Scholar] [CrossRef] [PubMed]
- OHCHR; WHO. The Right to Health. Fact Sheet No. 31; United Nations Press: Geneva, Switzerland, 2008. [Google Scholar]
- Sischo, L.; Broder, H.L. Oral health-related quality of life: What, why, how, and future implications. J. Dent. Res. 2011, 90, 1264–1270. [Google Scholar] [CrossRef] [Green Version]
- Thomson, W.M.; Broder, H.L. Oral Health-Related Quality of Life in Children and Adolescents. Pediatric Clin. N. Am. 2018, 65, 1073–1084. [Google Scholar] [CrossRef] [PubMed]
- Gabardo, M.C.L.; Moysés, S.T.; Moysés, S.J. Self-Rating of oral health according to the Oral Health Impact Profile and associated factors: A systematic review. Rev. Panam. Salud Pública 2013, 33, 439–445. [Google Scholar]
- Bennadi, D.; Reddy, C.V.K. Oral health related quality of life. J. Int. Soc. Prev. Community Dent. 2013, 3, 1–6. [Google Scholar] [CrossRef]
- Locker, D.; Allen, F. What do measures of ‘oral health-related quality of life’ measure? Community Dent. Oral Epidemiol. 2007, 35, 401–411. [Google Scholar] [CrossRef]
- Montero, J.; Bravo, M.; Vicente, M.P.; Galindo, M.P.; López, J.F.; Albaladejo, A. Dimensional structure of the oral health-related quality of life in healthy Spanish workers. Health Qual. Life Outcomes 2010, 21, 8–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atchison, K.A.; Dolan, T.A. Development of the Geriatric Oral Health Assessment Index. J. Dent. Educ. 1990, 54, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Leão, A.; Sheiham, A. The development of a socio-dental measure of dental impacts on daily living. Community Dent. Health 1996, 13, 22–26. [Google Scholar] [PubMed]
- Adulyanon, S.; Sheiham, A. Oral Impacts on Daily Performances. In Measuring Oral Health and Quality of Life; Slade, G.D., Ed.; University of North Carolina: Chapel Hill, NC, USA, 1997; pp. 151–160. [Google Scholar]
- Montero, J.; Bravo, M.; Albaladejo, A. Validation of two complementary oral-health related quality of life indicators (OIDP and OSS 0-10) in two qualitatively distinct samples of the Spanish population. Health Qual. Life Outcomes 2008, 6, 101. [Google Scholar] [CrossRef] [Green Version]
- Patil, S.; Kahtani, A.A.; Baeshen, H.A.; Alamir, A.W.; Khan, S.; Bhandi, S.; Hosmani, J.; Raj, A.T.; Gadbail, A.; Gondivkar, S.; et al. Face Validity and Psychometric Evaluation of the Available Oral Health-related Quality of Life Instruments: A Systematic Review. Oral Health Prev. Dent. 2020, 18, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Jokovic, A.; Locker, D.; Stephens, M.; Kenny, D.; Tompson, B.; Guyatt, G. Validity and reliability of a questionnaire for measuring child oral-health-related quality of life. J. Dent. Res. 2002, 81, 459–463. [Google Scholar] [CrossRef]
- Filstrup, S.L.; Briskie, D.; Da Fonseca, M.; Lawrence, L.; Wandera, A.; Inglehart, M.R. Early childhood caries and quality of life: Child and parent perspectives. Pediatric Dent. 2003, 25, 431–440. [Google Scholar]
- Broder, H.L.; McGrath, C.; Cisneros, G.J. Questionnaire development: Face validity and item impact testing of the Child Oral Health Impact Profile. Community Dent. Oral Epidemiol. 2007, 35 (Suppl. 1), 8–19. [Google Scholar] [CrossRef]
- Gherunpong, S.; Tsakos, G.; Sheiham, A. Developing and evaluating an oral health-related quality of life index for children; the CHILD-OIDP. Community Dent. Health 2004, 21, 161–169. [Google Scholar]
- Tubert-Jeannin, S.; Pegon-Machat, E.; Gremeau-Richard, C.; Lecuyer, M.; Tsakos, G. Validation of a French version of Child-OIDP index. Eur. J. Oral Sci. 2005, 113, 355–362. [Google Scholar] [CrossRef]
- Yusuf, H.; Gherunpong, S.; Tsakos, G.; Sheiham, A. Validation of an English version of Child-OIDP index, an oral health related quality of life measure for children. Health Qual. Life Outcomes 2006, 1, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mtaya, M.; Astrøm, A.N.; Tsakos, G. Applicability of an abbreviated version of the Child-OIDP inventory among primary schoolchildren in Tanzania. Health Qual. Life Outcomes 2007, 13, 40. [Google Scholar] [CrossRef] [Green Version]
- Martinicorena, F.J.C.; Gallardo, E.R.; Oses, J.A.; Bravo, M.; Tsakos, G. Adaptation and validation for Spain of the Child-Oral Impact on Daily Performance (C-OIDP) for use with adolescents. Med. Oral Patol. Oral Cirugía Bucal 2010, 15, 106–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pentapati, K.C.; Yeturu, S.K.; Siddiq, H.A. A reliability generalization meta-analysis of Child Oral Impacts on Daily Performances (C-OIDP) questionnaire. J. Oral Biol. Craniofacial Res. 2020, 10, 776–781. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- De Argumedo, M.L.; Reviriego, E.; Gutiérrez, A.; Bayón, J.C. Actualización del Sistema de Trabajo Compartido para Revisiones Sistemáticas de la Evidencia Científica y Lectura Crítica (Plataforma FLC 3.0). Ministerio de Sanidad, Servicios Sociales e Igualdad. Servicio de Evaluación de Tecnologías Sanitarias del País Vasco 2017. Informes de Evaluación de Tecnologías Sanitarias: OSTEBA. Available online: https://www.ser.es/wp-content/uploads/2018/04/Informe-OSTEBA.-FLC-3.0.pdf (accessed on 1 December 2021).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzahrani, A.A.H.; Alhassan, E.M.; Albanghali, M.A. Association between oral diseases and impact on daily performance among male Saudi schoolchildren. Clin. Exp. Dent. Res. 2019, 5, 655–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bakhtiar, M.; Mohammadi, T.M.; Hajizamani, A.; Vossoughi, M. Association of Oral Health Indicators with Quality-of-Life Related to Oral Health among Iranian Adolescent. J. Int. Oral Health 2014, 6, 5–9. [Google Scholar] [CrossRef] [Green Version]
- Basavaraj, P.; Sunil, M.K.; Nagarajappa, R.; Ashish, S.; Ramesh, G. Correlation between oral health and Child-OIDP Index in 12-and 15-year-old children from Modinagar, India. Asia Pac. J. Public Health 2014, 26, 390–400. [Google Scholar] [CrossRef]
- Castro, R.A.L.; Portela, M.C.; Leão, A.T.; Vasconcellos, M.T.L. Oral health-related quality of life of 11- and 12-year-old public school children in Rio de Janeiro. Community Dent. Oral Epidemiol. 2011, 39, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Do, H.G.; Truong, K.N.; Pham, D.H.; Ngo, L.T.Q.; Tran, H.T.; Doan, N. Oral Impacts on Daily Performances of Children 12 and 15-Year-Old in Can Tho City. In Proceedings of the 7TH International Conference on the Development of Biomedical Engineering in Vietnam (BME7), Ho Chi Minh City, Vietnam, 27–29 June 2018; Van Toi, V., Le, T.Q., Ngo, H.T., Nguyen, T.H., Eds.; Springer: Singapore, 2020; pp. 585–589. [Google Scholar] [CrossRef]
- Dumitrache, M.A.; Comes, C.; Teodorescu, E.; Dumitraşcu, L.; Cuculescu, M.; Ionescu, E. Life quality related to oral health of schoolchildren from Bucharest. Rev. Romana Bioet. 2009, 7, 169–178. [Google Scholar]
- Kumar, S.; Kumar, A.; Badiyani, B.; Kumar, A.; Basak, D.; Ismai, L.M.B. Oral health impact, dental caries experience, and associated factors in 12–15-year-old school children in India. Int. J. Adolesc. Med. Health 2017, 29. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, X.M.; Abara, C.V.; Cartes-Velásquez, R. Impacto de la salud bucal en la calidad de vida de escolares de 11 a 14 años, Licantén, 2013 TT—Oral health impact on the quality of life of 11 to 14 years-old schoolchildren, Licantén, 2013. Rev. Clin. Periodoncia Implantol. Rehabil. Oral 2014, 7, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Paredes-Martínez, E.R.; Díaz-Pizán, M.E. Impacto de las condiciones bucales sobre la calidad de vida en escolares del Distrito de San Juan de Miraflores. Lima, Perú TT—Impact of oral conditions on the quality of life in schoolchildren in San Juan de Miraflores. Lima, Perú. Rev. Estomatol. Hered. Internet 2014, 24, 171–177. [Google Scholar] [CrossRef]
- Pavithran, V.K.; Murali, R.; Krishna, M.; Shamala, A.; Yalamalli, M.; Kumar, A.V.; Raina, R. Impact of oral diseases on daily activities among 12- To 15-year-old institutionalized orphan and non-orphan children in Bengaluru city: A cross-sectional analytical study. Indian J. Dent. Res. Internet 2020, 31, 396–402. [Google Scholar] [CrossRef] [PubMed]
- Vélez-Vásquez, V.A.; Villavicencio-Caparó, E.; Cevallos-Romero, S.; Del Castillo-López, C. Impacto de la experiencia de caries en la calidad de vida relacionada a la salud bucal; Machángara, Ecuador TT—Impact of caries experience on quality of life related to bucal health, Machángara, Ecuador. Rev. Estomatol. Hered. Internet 2019, 29, 203–212. [Google Scholar] [CrossRef]
- Alves, F.N.; de Andrade, C.L.; Vettore, M.V. Planning oral health care using the sociodental approach and the index of family living conditions: A cross-sectional study in Brazilian adolescents. BMC Res. Notes 2015, 8, 588. [Google Scholar] [CrossRef] [Green Version]
- Bernabé, E.; Tsakos, G.; Sheiham, A. Intensity and extent of oral impacts on daily performances by type of self-perceived oral problems. Eur. J. Oral Sci. 2007, 115, 111–116. [Google Scholar] [CrossRef] [PubMed]
- Del Castillo-López, C.; Evangelista-Alva, A.; Sánchez-Borjas, P. Impacto de las condiciones bucales sobre la calidad de vida en escolares de ámbito rural, Piura, Perú TT—Impact of oral conditions on the quality of life in rural schoolchildren, Piura, Peru. Rev. Estomatológica Hered. Internet 2014, 24, 220–228. [Google Scholar] [CrossRef]
- Marcelo-Ingunza, J.; del Castillo-López, C.; Evangelista-Alva, A.; Sánchez-Borjas, P. Calidad de vida relacionada a la salud bucal en escolares de ámbito urbano-marginal TT—Oral Health Related Quality of Life in school children of urban-marginal area. Rev. Estomatológica Hered. Internet 2015, 25, 194–204. [Google Scholar] [CrossRef]
- Naidoo, S.; Sheiham, A.; Tsakos, G. The relation between oral impacts on daily performances and perceived clinical oral conditions in primary school children in the Ugu District, Kwazulu Natal, South Africa. S. Afr. Dent. J. 2013, 68, 214–218. [Google Scholar]
- Nordin, E.A.B.; Shoaib, L.A.; Yusof, Z.Y.M.; Manan, N.M.; Othman, S.A. Oral health-related quality of life among 11–12year old indigenous children in Malaysia. BMC Oral Health 2019, 19, 152. [Google Scholar] [CrossRef] [Green Version]
- Reinoso-Vintimilla, N.; Del Castillo-López, C. Calidad de vida relacionada a la salud bucal en escolares de Sayausí, Cuenca Ecuador TT—Quality of life related to the oral health in school from Sayausí, Cuenca Ecuador. Rev. Estomatol. Hered. 2017, 27, 227–234. [Google Scholar] [CrossRef] [Green Version]
- Simangwa, L.D.; Johansson, A.K.; Johansson, A.; Minja, I.K.; Astrom, A.N.; Åstrøm, A.N. Oral impacts on daily performances and its socio-demographic and clinical distribution: A cross-sectional study of adolescents living in Maasai population areas, Tanzania. Health Qual. Life Outcomes 2020, 18, 181. [Google Scholar] [CrossRef]
- Amalia, R.; Schaub, R.M.H.; Stewart, R.E.; Widyanti, N.; Groothoff, J.W. Impact of school-based dental program performance on the oral health-related quality of life in children. J. Investig. Clin. Dent. 2017, 8, e12179. [Google Scholar] [CrossRef]
- Athira, S.; Jayakumar, H.L.; Chandra, M.; Gupta, T.; Dithi, C.; Anand, P.J.S. Oral Health-Related Quality of Life of School Children Aged 12–17 Years According to the Child-Oral Impacts on Daily Performances Index and the Impact of Oral Health Status on Index Scores. Int. J. Prev. Public Health Sci. 2015, 1, 25–30. [Google Scholar] [CrossRef]
- Bianco, A.; Fortunato, L.; Nobile, C.G.A.; Pavia, M. Prevalence and determinants of oral impacts on daily performance: Results from a survey among school children in Italy. Eur. J. Public Health 2010, 20, 595–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yetkiner, E.; Vardar, C.; Ergin, E.; Yücel, C.; Ersin, N.K. Orthodontic Treatment Need, Self-Esteem, and Oral Health-Related Quality of Life Assessment of Primary Schoolchildren: A Cross-Sectional Pilot Study. Turk. J. Orthod. 2014, 26, 182–189. [Google Scholar] [CrossRef] [Green Version]
- Petersen, P.E.; Baez, R.J. World Health Organization. In Oral Health Surveys: Basic Methods, 5th ed.; WHO Press: Geneva, Switzerland, 2013; ISBN 978-92-4-154864-9. [Google Scholar]
- Adunola, F.; Garcia, I.; Iafolla, T.; Boroumand, S.; Silveira, M.L.; Adesanya, M.; Dye, B.A. Self-perceived oral health, normative need, and dental services utilization among dentate adults in the United States: National Health and Nutrition Examination Survey (NHANES) 2011–2014. J. Public Health Dent. 2019, 79, 79–90. [Google Scholar] [CrossRef]

| Criteria | Inclusion | Exclusion |
|---|---|---|
| 1. Study design | Cross-sectional studies | Systematic reviews, metanalysis, literature reviews, case-control studies, case-series, cohort’s studies, reports, papers, conference proceedings |
| 2. Population | Adolescents | Adults |
| 3. Population age range | 11–18 years-old | <11-years-old >18-years-old |
| 4. Administered questionnaire | C-OIDP/OIDP | Other oral health-related quality of life-validated questionnaires |
| 5. Year of publication | Last 17 years (2005–2021) | <2005 |
| 6. Language | English, Spanish | Other languages |
| 7. Publication type | Original articles, full-text | Not original articles, abstracts |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alvarez-Azaustre, M.P.; Greco, R.; Llena, C. Oral Health-Related Quality of Life in Adolescents as Measured with the Child-OIDP Questionnaire: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 12995. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182412995
Alvarez-Azaustre MP, Greco R, Llena C. Oral Health-Related Quality of Life in Adolescents as Measured with the Child-OIDP Questionnaire: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(24):12995. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182412995
Chicago/Turabian StyleAlvarez-Azaustre, María Paloma, Rossana Greco, and Carmen Llena. 2021. "Oral Health-Related Quality of Life in Adolescents as Measured with the Child-OIDP Questionnaire: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 24: 12995. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182412995