
Do Cognitive Abilities Influence Physical and Mental Fatigue in Patients with Chronic Pain after Walking According to a Clinical Guideline for Physical Exercise?

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Walking Pattern
2.2.2. Chronic Pain Acceptance Questionnaire (CPAQ)
2.2.3. Cognitive Fusion
2.2.4. Mental and Physical Fatigue
2.2.5. Socio-Demographic and Clinical Data
2.3. Procedure
2.4. Statistical Analysis
3. Results
3.1. Descriptive Analysis and Correlations of the Variables under Study
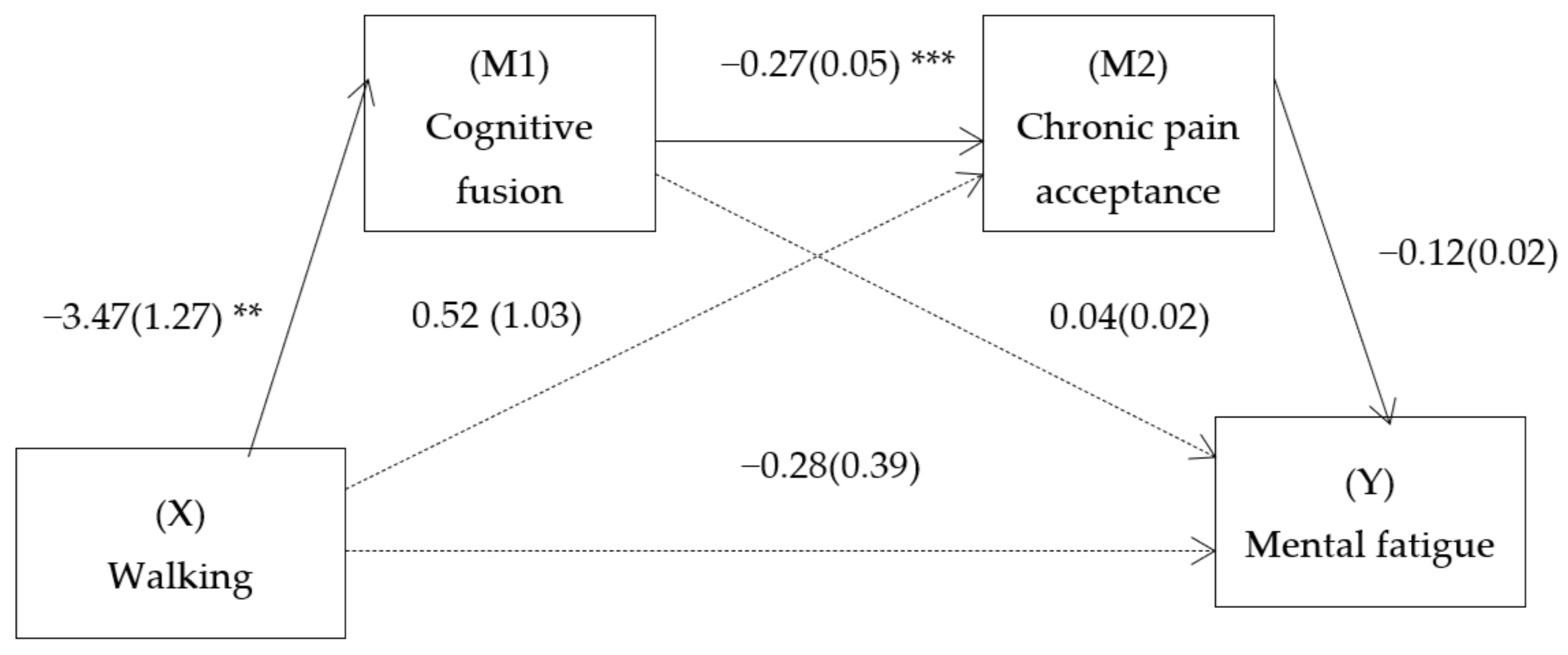
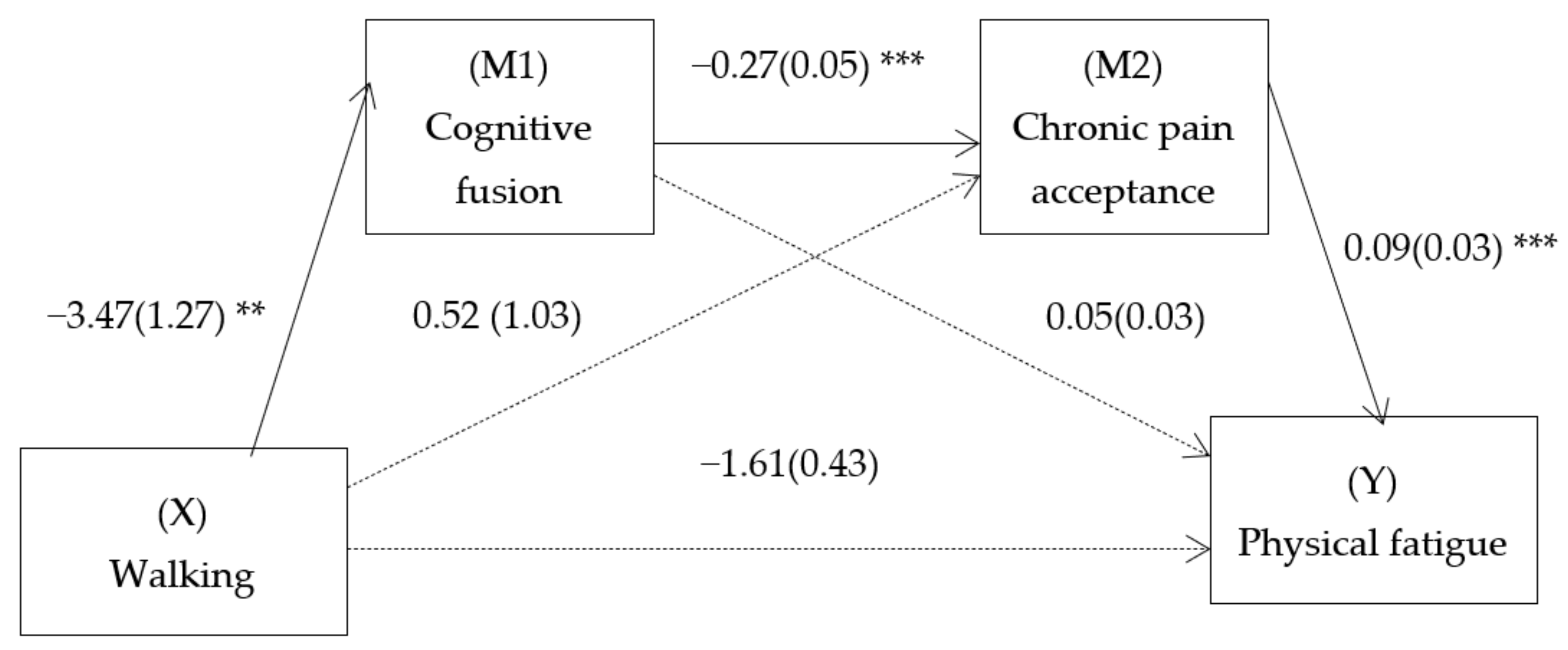
3.2. SMM Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Busch, A.J.; Webber, S.C.; Brachaniec, M.; Bidonde, J.; Bello-Haas, V.D.; Danyliw, A.D.; Overend, T.J.; Richards, R.S.; Sawant, A.; Schachter, C.L. Exercise Therapy for Fibromyalgia. Curr. Pain Headache Rep. 2011, 15, 358–367. [Google Scholar] [CrossRef] [Green Version]
- Bidonde, J.; Busch, A.; Bath, B.; Milosavljevic, S. Exercise for Adults with Fibromyalgia: An Umbrella Systematic Review with Synthesis of Best Evidence. Curr. Rheumatol. Rev. 2014, 10, 45–79. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; et al. EULAR revised recommendations for the management of fibromyalgia. Ann. Rheum. Dis. 2017, 76, 318–328. [Google Scholar] [CrossRef]
- Gusi, N.; Parraca, J.; Adsuar, J.; Olivares, P. Physical exercise and Fibromyalgia. In Guía de ejercicios físicos para personas con Fibromialgia; Penacho, A., Rivera, J., Pastor, M.A., Gusi, N., Eds.; Asociación Divulgación Fibromialgia: Vitoria, 2009; pp. 39–56. [Google Scholar]
- López-Roig, S.; Pastor, M.A.; Peñacoba, C.; Lledó, A.; Sanz, Y.; Velasco, F. Prevalence and predictors of unsupervised walking and physical activity in a community population of women with fibromyalgia. Rheumatol. Int. 2016, 36, 1127–1133. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Baños, Y.; Pastor-Mira, M.-Á.; Lledó, A.; López-Roig, S.; Peñacoba, C.; Sánchez-Meca, J. Do women with fibromyalgia adhere to walking for exercise programs to improve their health? Systematic review and meta-analysis. Disabil. Rehabil. 2018, 40, 2475–2487. [Google Scholar] [CrossRef] [PubMed]
- Peñacoba, C.; Pastor, M.-Á.; López-Roig, S.; Velasco, L.; Lledo, A. Walking Beliefs in Women With Fibromyalgia: Clinical Profile and Impact on Walking Behavior. Clin. Nurs. Res. 2017, 26, 632–650. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Baños, Y.; Pastor, M.-Á.; Velasco, L.; López-Roig, S.; Peñacoba, C.; Lledo, A.; Rodríguez, C. To walk or not to walk: Insights from a qualitative description study with women suffering from fibromyalgia. Rheumatol. Int. 2016, 36, 1135–1143. [Google Scholar] [CrossRef]
- Slade, S.C.; Patel, S.; Underwood, M.; Keating, J.L. What Are Patient Beliefs and Perceptions About Exercise for Nonspecific Chronic Low Back Pain? Clin. J. Pain 2014, 30, 995–1005. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Norton, S.; McCracken, L.M. Change in “Self-as-Context” (“Perspective-Taking”) Occurs in Acceptance and Commitment Therapy for People With Chronic Pain and Is Associated With Improved Functioning. J. Pain 2017, 18, 664–672. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, S.A.; Pinto-Gouveia, J.; Gillanders, D.; Castilho, P. Pain and Depressive Symptoms: Exploring Cognitive Fusion and Self-Compassion in a Moderated Mediation Model. J. Psychol. Interdiscip. Appl. 2019, 153, 173–186. [Google Scholar] [CrossRef] [PubMed]
- Gillanders, D.T.; Bolderston, H.; Bond, F.W.; Dempster, M.; Flaxman, P.E.; Campbell, L.; Kerr, S.; Tansey, L.; Noel, P.; Ferenbach, C.; et al. The Development and Initial Validation of the Cognitive Fusion Questionnaire. Behav. Ther. 2014, 45, 83–101. [Google Scholar] [CrossRef] [Green Version]
- Romero-Moreno, R.; Losada, A.; Fernández-Fernández, V.; Márquez-González, M.; Gillanders, D. Cognitive fusion in dementia caregiving: Psychometric properties of the spanish version of the “cognitive fusion questionnaire”. Behav. Psychol. Psicol. Conduct. 2014, 22, 117–132. [Google Scholar]
- Esteve, R.; Ramírez-Maestre, C.; López-Martínez, A.E. Adjustment to chronic pain: The role of pain acceptance, coping strategies, and pain-related cognitions. Ann. Behav. Med. 2007, 33, 179–188. [Google Scholar] [CrossRef]
- Écija, C.; Luque-Reca, O.; Suso-Ribera, C.; Catala, P.; Peñacoba, C. Associations of Cognitive Fusion and Pain Catastrophizing with Fibromyalgia Impact through Fatigue, Pain Severity, and Depression: An Exploratory Study Using Structural Equation Modeling. J. Clin. Med. 2020, 9, 1763. [Google Scholar] [CrossRef]
- Peñacoba, C.; Ecija, C.; Velasco, L.; Catala, P.; Suso-Ribera, C. The paradox of wellbeing: What happens among women with fibromyalgia? Aging Ment. Health 2021, 1–8. [Google Scholar] [CrossRef]
- Catala, P.; Lopez-Roig, S.; Ecija, C.; Suso-Ribera, C.; Peñacoba Puente, C. Why do some people with severe chronic pain adhere to walking prescriptions whilst others won’t? A cross-sectional study exploring clinical and psychosocial predictors in women with fibromyalgia. Rheumatol. Int. 2021, 41, 1479–1484. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; DaSilva, P.; Skillicorn, B.; Doherty, R. The Cognitive Fusion Questionnaire. Clin. J. Pain 2014, 30, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Haugmark, T.; Hagen, K.B.; Smedslund, G.; Zangi, H.A. Mindfulness- and acceptance-based interventions for patients with fibromyalgia—A systematic review and meta-analyses. PLoS ONE 2019, 14, e0221897. [Google Scholar] [CrossRef] [PubMed]
- Catalá, P.; Blanco, S.; Perez-Calvo, S.; Luque-Reca, O.; Bedmar, D.; Peñacoba, C. Does the Rural Environment Influence Symptomatology and Optimize the Effectiveness of Disease Acceptance? A Study Among Women With Fibromyalgia. Front. Psychol. 2021, 12, 658974. [Google Scholar] [CrossRef]
- Wicksell, R.K.; Kemani, M.; Jensen, K.; Kosek, E.; Kadetoff, D.; Sorjonen, K.; Ingvar, M.; Olsson, G.L. Acceptance and commitment therapy for fibromyalgia: A randomized controlled trial. Eur. J. Pain 2013, 17, 599–611. [Google Scholar] [CrossRef] [PubMed]
- Tangen, S.F.; Helvik, A.-S.; Eide, H.; Fors, E.A. Pain acceptance and its impact on function and symptoms in fibromyalgia. Scand. J. Pain 2020, 20, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, L.; Velasco, L.; Blanco, S.; Catala, P.; Pastor-Mira, M.Á.; Peñacoba, C. Perfectionism, maladaptive beliefs and anxiety in women with fibromyalgia. An explanatory model from the conflict of goals. Pers. Individ. Dif. 2022, 184, 111165. [Google Scholar] [CrossRef]
- Dailey, D.L.; Frey-Law, L.; Vance, C.; Rakel, B.A.; Merriwether, E.N.; Darghosian, L.; Golchha, M.; Geasland, K.M.; Spitz, R.; Crofford, L.; et al. Perceived function and physical performance are associated with pain and fatigue in women with fibromyalgia. Arthritis Res. Ther. 2016, 18, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grape, H.E.; Solbrække, K.N.; Kirkevold, M.; Mengshoel, A.M. Tiredness and fatigue during processes of illness and recovery: A qualitative study of women recovered from fibromyalgia syndrome. Physiother. Theory Pract. 2017, 33, 31–40. [Google Scholar] [CrossRef]
- Humphrey, L.; Arbuckle, R.; Mease, P.; Williams, D.A.; Samsoe, B.D.; Gilbert, C. Fatigue in fibromyalgia: A conceptual model informed by patient interviews. BMC Musculoskelet. Disord. 2010, 11, 216. [Google Scholar] [CrossRef] [Green Version]
- Vincent, A.; Benzo, R.P.; Whipple, M.O.; McAllister, S.J.; Erwin, P.J.; Saligan, L.N. Beyond pain in fibromyalgia: Insights into the symptom of fatigue. Arthritis Res. Ther. 2013, 15, 221. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, F.; Smythe, H.A.; Yunus, M.B.; Bennett, R.M.; Bombardier, C.; Goldenberg, D.L.; Tugwell, P.; Campbell, S.M.; Abeles, M.; Clark, P.; et al. The american college of rheumatology 1990 criteria for the classification of fibromyalgia. Arthritis Rheum. 1990, 33, 160–172. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodero, B.; García-Campayo, J.; Casanueva, B.; del Hoyo, Y.L.; Serrano-Blanco, A.; Luciano, J. V Veaselaircdhation of the Spanish version of the Chronic Pain Acceptance Questionnaire (CPAQ) for the assessment of acceptance in fibromyalgia. Health Qual. Life Outcomes 2010, 8, 37. [Google Scholar] [CrossRef] [Green Version]
- Luque-Reca, O.; Gillanders, D.; Catala, P.; Peñacoba, C. Psychometric properties of the Cognitive Fusion Questionnaire in females with fibromyalgia. Curr. Psychol. 2021, 1–11. [Google Scholar] [CrossRef]
- Munguía-Izquierdo, D.; Segura-Jimenez, V.; Camiletti-Moiron, D.; Pulido-Martos, M.; Álvarez-Gallardo, I.C.; Romero, A.; Aparicio, V.A.; Carbonell-Baeza, A.; Delgado-Fernández, M. Multidimensional fatigue inventory: Spanish adaptation and psychometric properties for fibromyalgia patients. The Al-andalus study. Clin. Exp. Rheumatol. 2012, 30, 94–102. [Google Scholar]
- IBM Corp IBM SPSS Statistics for Windows, version 22. IBM Corp.: Armonk, NY, USA, 2017.
- Hayes, A. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Press: New York, NY, USA, 2013. [Google Scholar]
- Hu, L.; Bentler, P. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternative. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Baron, R.; Kenny, D. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Turk, D.C.; Wilson, H.D.; Cahana, A. Treatment of chronic non-cancer pain. Lancet 2011, 377, 2226–2235. [Google Scholar] [CrossRef]
- Betina Nishishinya, M.; Rivera, J.; Alegre, C.; Alejandra Pereda, C. Non pharmacologic and alternative treatments in fibromyalgia. Med. Clin. 2006, 127, 295–299. [Google Scholar] [CrossRef]
- Cabral, C.M.N.; Miyamoto, G.C.; Franco, K.F.M.; Bosmans, J.E. Economic evaluations of educational, physical, and psychological treatments for fibromyalgia: A systematic review with meta-analysis. Pain 2021, 162, 2331–2345. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy; The Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Hayes, S.C.; Luoma, J.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and commitment therapy: Model, processes, and outcomes. In The Act in Context—The Canonical Papers of Steven C. Hayes; Routledge: New York, NY, USA, 2016; pp. 249–279. [Google Scholar] [CrossRef]
- McCracken, L.M.; Morley, S. The Psychological Flexibility Model: A Basis for Integration and Progress in Psychological Approaches to Chronic Pain Management. J. Pain 2014, 15, 221–234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Aranda, A.; Barceló-Soler, A.; Andrés-Rodríguez, L.; Peñarrubia-María, M.T.; Tuccillo, R.; Borraz-Estruch, G.; García-Campayo, J.; Feliu-Soler, A.; Luciano, J.V. Description and narrative review of well-established and promising psychological treatments for fibromyalgia. Mindfulness Compassion 2017, 2, 112–129. [Google Scholar] [CrossRef]
- Peñacoba, C.; Pastor-Mira, M.Á.; Suso-Ribera, C.; Catalá, P.; Nardi-Rodríguez, A.; López-Roig, S. Activity Patterns and Functioning. A Contextual–Functional Approach to Pain Catastrophizing in Women with Fibromyalgia. Int. J. Environ. Res. Public Health 2021, 18, 5394. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, S.R.; Tully, M.A.; Ryan, B.; Bleakley, C.M.; Baxter, G.D.; Bradley, J.M.; McDonough, S.M. Walking Exercise for Chronic Musculoskeletal Pain: Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2015, 96, 724–734e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terrier, P.; Praz, C.; Le Carré, J.; Vuistiner, P.; Léger, B.; Luthi, F. Influencing walking behavior can increase the physical activity of patients with chronic pain hospitalized for multidisciplinary rehabilitation: An observational study. BMC Musculoskelet. Disord. 2019, 20, 188. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Psychosocial Characteristics | |
|---|---|
| Walking, n (%) | |
| Yes | 132 (57.1) |
| No | 95 (41.1) |
| Cognitive fusion, mean (SD) | 33.31 (9.61) |
| Chronic Pain Acceptance, mean (SD) | 18.93 (7.84) |
| Mental fatigue, mean (SD) | 15.25 (3.15) |
| Physical fatigue, mean (SD) | 15.21 (3.39) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catala, P.; Gutierrez, L.; Écija, C.; Serrano del Moral, Á.; Peñacoba, C. Do Cognitive Abilities Influence Physical and Mental Fatigue in Patients with Chronic Pain after Walking According to a Clinical Guideline for Physical Exercise? Int. J. Environ. Res. Public Health 2021, 18, 13148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413148
Catala P, Gutierrez L, Écija C, Serrano del Moral Á, Peñacoba C. Do Cognitive Abilities Influence Physical and Mental Fatigue in Patients with Chronic Pain after Walking According to a Clinical Guideline for Physical Exercise? International Journal of Environmental Research and Public Health. 2021; 18(24):13148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413148
Chicago/Turabian StyleCatala, Patricia, Lorena Gutierrez, Carmen Écija, Ángel Serrano del Moral, and Cecilia Peñacoba. 2021. "Do Cognitive Abilities Influence Physical and Mental Fatigue in Patients with Chronic Pain after Walking According to a Clinical Guideline for Physical Exercise?" International Journal of Environmental Research and Public Health 18, no. 24: 13148. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182413148