
Developmental Dental Defects in Permanent Teeth Resulting from Trauma in Primary Dentition: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
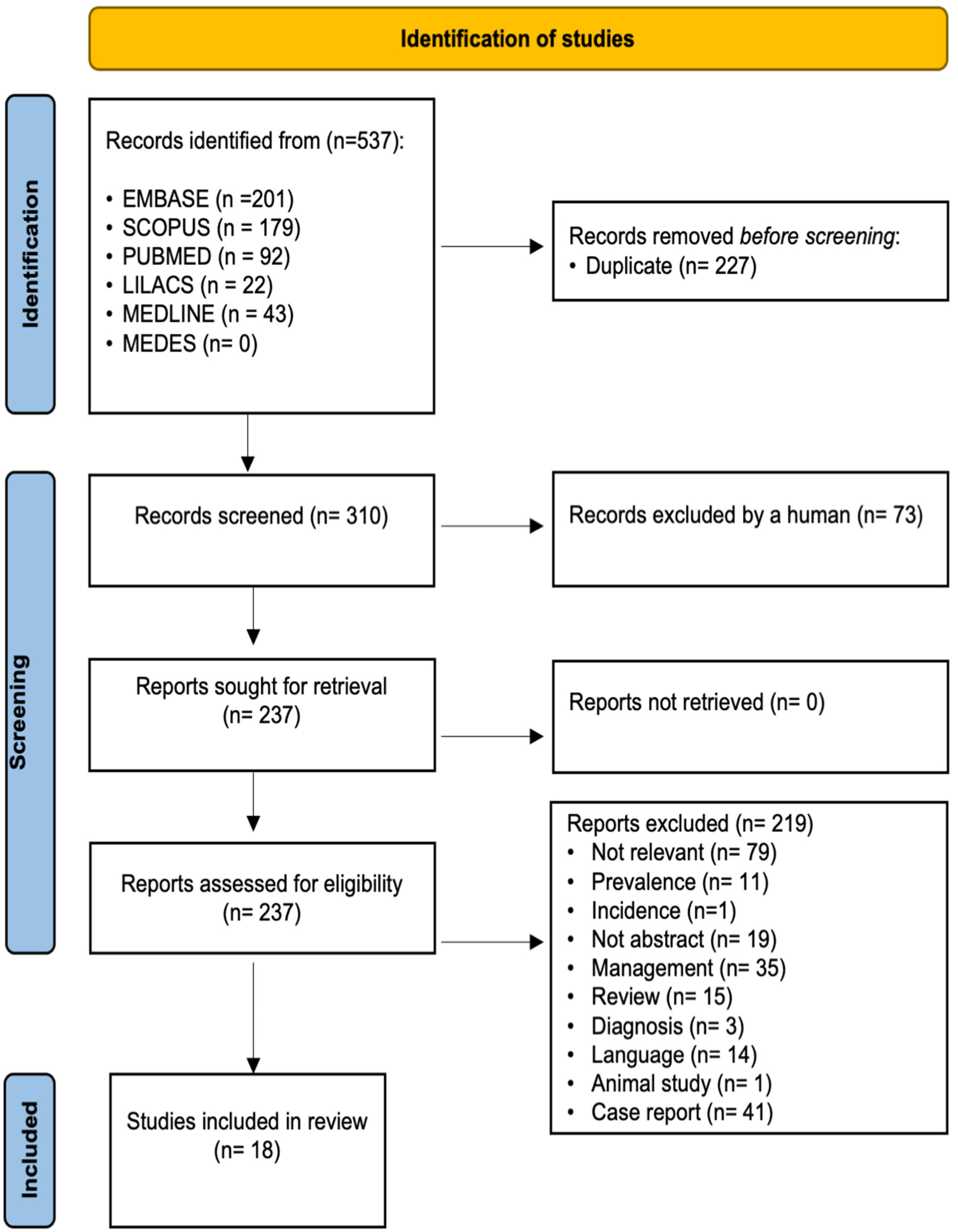
2. Materials and Methods
3. Results
Consequences in Permanent Dentition in High Quality Articles
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Mendoza-Mendoza, A.; Iglesias-Linares, A.; Yañez-Vico, R.M.; Abalos-Labruzzi, C. Prevalence and Complications of Trauma to the Primary Dentition in a Subpopulation of Spanish Children in Southern Europe. Dent. Traumatol. 2015, 31, 144–149. [Google Scholar] [CrossRef]
- Akin, A.; Uysal, S.; Cehreli, Z.C. Segmental Alveolar Process Fracture Involving Primary Incisors: Treatment and 24-Month Follow Up. Dent. Traumatol. 2011, 27, 63–66. [Google Scholar] [CrossRef] [PubMed]
- Soares, F.C.; Cardoso, M.; Bolan, M. Association between Trauma to Primary Incisors and Crown Alterations in Permanent Successors. Braz. Dent. J. 2014, 25, 332–335. [Google Scholar] [CrossRef]
- da Silva Assuņão, L.R.; Ferelle, A.; Iwakura, M.L.H.; Cunha, R.F. Effects on Permanent Teeth after Luxation Injuries to the Primary Predecessors: A Study in Children Assisted at an Emergency Service. Dent. Traumatol. 2009, 25, 165–170. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Ravn, J.J. The Effect of Traumatic Injuries to Primary Teeth on Their Permanent Successors: II. A Clinical and Radiographic Follow-up Study of 213 Teeth. Eur. J. Oral Sci. 1971, 79, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Altun, C.; Cehreli, Z.C.; Güven, G.; Acikel, C. Traumatic Intrusion of Primary Teeth and Its Effects on the Permanent Successors: A Clinical Follow-up Study. Oral. Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 493–498. [Google Scholar] [CrossRef]
- Cueto Urbina, A.; Ávila Rivera, C.; González Ríos, J. Traumatismos Dentoalveolares Que Afectan a Las Estructuras de Soporte de Los Dientes Temporales y Sus Efectos En Los Sucesores Definitivos. Int. J. Odontostomatol. 2012, 6, 379–383. [Google Scholar] [CrossRef] [Green Version]
- de Fátima Guedes de Amorim, L.; Estrela, C.; da Costa, L.R.R.S. Effects of Traumatic Dental Injuries to Primary Teeth on Permanent Teeth—A Clinical Follow-up Study. Dent. Traumatol. 2011, 27, 117–121. [Google Scholar] [CrossRef] [PubMed]
- Tsurumachi, T.; Hirano, Y.; Hira, A.; Aida, Y.; Ogiso, B. Developmental Disturbance of a Mandibular Central Incisor Following Trauma to the Primary Predecessor. J. Oral Sci. 2015, 57, 157–160. [Google Scholar] [CrossRef] [Green Version]
- Lenzi, M.M.; da Silva Fidalgo, T.K.; Luiz, R.R.; Maia, L.C. Trauma in Primary Teeth and Its Effect on the Development of Permanent Successors: A Controlled Study. Acta. Odontol. Scand. 2019, 77, 76–81. [Google Scholar] [CrossRef]
- Carvalho, V.; Jacomo, D.R.; Campos, V. Frequency of Intrusive Luxation in Deciduous Teeth and Its Effects. Dent. Traumatol. 2010, 26, 304–307. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G. Systematic Reviews of Evaluations of Prognostic Variables. Syst. Rev. Health Care Meta-Anal. 2008, 323, 228–247. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Szymańska-Jachimczak, E.I. Acute mechanical injuries to deciduous teeth, their effect on tooth germs of permanent teeth, therapeutic procedures. Czas. Stomatol. 1972, 25, 537–543. [Google Scholar]
- Demir, P.; Guler, C.; Kizilci, E.; Keskin, G. Survival of Avulsed Permanent Incisors in Children Following Delayed Replantation. Niger. J. Clin. Pract. 2020, 23, 631–637. [Google Scholar]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. 2000. Available online: http://www3.med.unipmn.it/dispense_ebm/2009-2010/Corso%20Perfezionamento%20EBM_Faggiano/NOS_oxford.pdf (accessed on 4 January 2022).
- Von Arx, T. Developmental Disturbances of Permanent Teeth Following Trauma to the Primary Dentition. Aust. Dent. J. 1993, 38, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J.O.; Ravn, J.J. Enamel Changes in Permanent Teeth after Trauma to Their Primary Predecessors. Eur. J. Oral Sci. 1973, 81, 203–209. [Google Scholar] [CrossRef]
- Odersjö, M.L.; Koch, G. Developmental Disturbances in Permanent Successors after Intrusion Injuries to Maxillary Primary Incisors. Eur. J. Paediatr. Dent. 2001, 2, 165–172. [Google Scholar]
- Sennhenn-Kirchner, S.; Jacobs, H.G. Traumatic Injuries to the Primary Dentition and Effects on the Permanent Successors—A Clinical Follow-up Study. Dent. Traumatol. 2006, 22, 237–241. [Google Scholar] [CrossRef]
- do Espirito Santo Jacomo, D.R.; Campos, V. Prevalence of Sequelae in the Permanent Anterior Teeth after Trauma in Their Predecessors: A Longitudinal Study of 8 Years. Dent. Traumatol. 2009, 25, 300–304. [Google Scholar] [CrossRef]
- Bardellini, E.; Amadori, F.; Pasini, S.; Majorana, A. Dental Anomalies in Permanent Teeth after Trauma in Primary Dentition. J. Clin. Pediatr. Dent. 2017, 41, 5–9. [Google Scholar] [CrossRef] [PubMed]
- De Amorim, C.S.; Americano, G.C.A.; Moliterno, L.F.M.; de Marsillac, M.D.W.S.; Andrade, M.R.T.C.; Campos, V. Frequency of Crown and Root Dilaceration of Permanent Incisors after Dental Trauma to Their Predecessor Teeth. Dent. Traumatol. 2018, 34, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Christophersen, P.; Freund, M.; Harild, L. Avulsion of Primary Teeth and Sequelae on the Permanent Successors. Dent. Traumatol. 2005, 21, 320–323. [Google Scholar] [CrossRef] [PubMed]
- Martioli, G.; Venante, H.S.; Santin, G.C.; de Salles, C.L.F.; Maciel, S.M.; de Fracasso, M.L.C. Dental Trauma and Itssequelae in Deciduous and Permanent Teeth-Longitudinal Study. Acta Sci.-Health Sci. 2019, 41, e34030. [Google Scholar] [CrossRef]
- Andreasen, J.O.; Andreasen, F.M.; Andersson, L. Textbook and Color Atlas of Traumatic Injuries to the Teeth. Stomatol. Edu. J. 2019, 6, 279. [Google Scholar] [CrossRef]


{kind=link}
| Study | Country | Study Design | Criteria ** | Total Score | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Selection | Comparability | Outcome and Exposure | |||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||||
| Von Arx and Colleagues, 1993 [17] | Switzerland | Cross-sectional | X | X | X | X | X | X | X | 7 | |
| Odersjö and Colleagues, 2001 [19] | Sweden | Cross-sectional | X | X | X | X | X | 5 | |||
| Christophersen and Colleagues, 2005 [24] | Denmark | Cross- sectional | X | X | X | X | 4 | ||||
| Sennhenn-Kirchner and Colleagues, 2006 [20] | Germany | Cohort | X | X | X | X | 4 | ||||
| Altun and Colleagues, 2009 [6] | Turkey | Cross-sectional | X | X | X | X | X | X | 6 | ||
| Da Silva Assunção and Colleagues, 2009 [4] | Brazil | Cross- sectional | X | X | X | X | X | 5 | |||
| Ribeiro do Espírito Santo and Colleagues, 2009 [21] | Brazil | Cross-sectional | X | X | X | X | X | 5 | |||
| Carvalho and Colleagues, 2010 [11] | Brazil | Cross-sectional | X | X | X | X | X | X | 6 | ||
| Guedes de Amorim and Colleagues, 2010 [8] | Brazil | Cross-sectional | X | X | X | X | X | 5 | |||
| Cueto Urbina and Colleagues, 2012 [7] | Chile | Cross-sectional | X | X | X | X | X | 5 | |||
| Soares and Colleagues, 2014 [3] | Brazil | Cross-sectional | X | X | X | 3 | |||||
| Mendoza-Mendoza and Colleagues, 2014 [1] | Spain | Cross-sectional | X | X | X | X | X | X | 6 | ||
| Bardellini and Colleagues, 2017 [22] | Italy | Cross-sectional | X | X | X | X | X | 5 | |||
| Silva de Amorim and Colleagues, 2018 [23] | Brazil | Cross-sectional | X | X | X | X | X | 5 | |||
| Graziele Martioli and Colleagues, 2019 [25] | Brazil | Cohort | X | X | X | X | X | 5 | |||
| Study | Country | Study Design | Criteria ** | Total Score | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Selection | Comparability | Outcome and Exposure | |||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||||
| Andreasen and Colleagues, 1971 [5] | Denmark | Case-control | X | X | X | X | X | X | 6 | ||
| Andreasen and Colleagues, 1972 [18] | Denmark | Case-control | X | X | X | X | X | X | X | 7 | |
| Machado Lenzi and Colleagues, 2018 [10] | Brazil | Case-control | X | X | X | X | X | X | X | 7 | |
| Study | Study Participants | Most Affected Teeth | Type of Primary Teeth Trauma | Most Damaging Trauma | Time When Trauma Occurred | Age at Dental Examination | Consequences in Permanent Dentition | Sequelae Prevalence | p Value |
|---|---|---|---|---|---|---|---|---|---|
| Von Arx and Colleagues, 1992 [17] | 114 children (70 boys, 44 girls) 255 traumatized primary teeth Age 0–7 years | Central upper primary incisors (n = 161, 63%) | Intrusion (15%) Avulsion (18%) Partial luxation (40%) Subluxation (18%) Crow and root fractures with exposed pulp (3%) Crow and root fractures without exposed pulp (6%) | Intrusion (54% of cases developed malformations) | Mean age at the time of the trauma was 3.6 years old | Mean age at the time of re-examination 8.7 years | Enamel hypoplasia (68%) Crown dilaceration (17%) Root malformation (10%) Odontoma-like teeth (5%) | 23% (n = 33) | p value NP |
| Altun and Colleagues, 2009 [6] | 78 children (41 boys, 37 girls) 138 traumatized primary incisors Age 12–48 months | Maxillary incisors (93.47%, with right central primary incisors accounting for 41.3%) | Intrusion | Intrusion | Most injuries occurred between 13 and 36 months | Mean age 22.32 ± 9.72 months | Enamel hypoplasia (39 teeth, 28.3%) Crown/root deformation (23 teeth, 16.7%) Ectopic eruption (23 teeth, 16.7%) | 53.6% (n = 74) | NS correlation between age of intrusion and frequency of subsequent developmental disturbances. (p > 0.05) |
| Carvalho and Colleagues, 2010 [11] | 307 children (169 boys, 138 girls) 753 traumatized anterior deciduous teeth Age between 0–10 years old | Right central primary incisor (35.2% TI) (47.3% PI) | Intrusion (n = 221, 29.3%) | Intrusion | Children with ages from 1 to 4 years old were the most affected | NP | Discoloration of enamel TI (11.7%, n = 15) PI (12.9%, n = 12) Enamel hypoplasia TI (7.8%, n = 10) PI (15.1%, n = 14) Crown dilaceration TI (2.3%, n = 3) PI (3.2%, n = 3) Root dilaceration TI (1.6%, n = 2) PI (3.2%, n = 3) Eruption disturbances TI (6.3%, n = 8) PI (12.9%, n = 12) Sequestration of permanent tooth germ TI (0,8%, n = 1) PI (0%, n = 0) | 68.8% (n = 84) | NS Correlation between the age of intrusion and the developmental disturbances on permanent teeth (p = 0.140) |
| Mendoza-Mendoza and Colleagues, 2014 [1] | 879 children 191 had traumatic injury to the primary dentition (101 boys, 90 girls) Age 1–7 years old | Upper central primary incisors (86.9%) | Subluxation (47.29%) Intrusion (23.15%) Avulsion (13.63%) Lateral luxation (9.35%) Extrusive luxation (5.9%) Hard tissue lesion (31.64%) | Intrusion | Most common age range for injuries in deciduous teeth was 1–3 years old | 43 children: 1 year old 57 children: 2 years old 42 children: 3 years old 22 children: 4 years old 27 children: 5 years old or more. | Hypoplasia (2 cases) Hypomineralization (2 cases) Delayed eruption (2 Case) Others (2 cases) | 4.5 % | p value NP |
| Study | Study Participants | Most Affected Teeth | Kind of Primary Teeth Trauma | Most Damaging Trauma | Time when Trauma Occurred | Age at Dental Examination | Consequences in Permanent Dentition | Sequelae Prevalence | p Value |
|---|---|---|---|---|---|---|---|---|---|
| Andreasen and Colleagues, 1971 [5] | TG: 103 patients 213 traumatized primary teeth CG: Contralateral permanent successors 26 children 33 teeth Age 0–9 years old | Maxillary central primary incisors (n = 131) | Subluxation: 35 primary teeth Intrusive luxation: 36 primary teeth Extrusive luxation: 76 primary teeth Exarticulation: 27 primary teeth No information: 39 primary teeth | Intrusion (69%, n = 25) | 62 children: 0 to 2 years old 43 children: 3 to 4 years old 88 children: 5 to 6 years old 20 children: 7 to 9 years old | NP | White or yellow- brown discoloration of enamel (23%) White or yellow-brown discoloration of enamel and circular enamel hypoplasia (12%) Crown dilaceration (3%) Lateral root angulation or dilaceration (1%) Partial or complete arrest of root formation (2%) Not disturbances (59%) | TG: 41% (n = 88) | p ≤ 0.05 |
| Andreasen and Colleagues, 1973 [18] | Main material: 487 children (251 boys, 236 girls) TG: 147 children NTG: 340 children CG: 111 children (51 boys, 60 girls) Age 9–17 years old | Only anterior teeth were included | Luxations and fractures | NP | NP | NP | Internal white enamel hypoplasia < 0.5mm TG: 19.7% NTG: 21.2% Internal white enamel hypoplasia ≥ 0.5mm TG: 19.0% NTG: 13.5% Internal white and yellow-brown enamel hypoplasia TG: 2.7% NTG:1.8% External white enamel hypoplasia TG: 3.4% NTG:2.3% External white and yellow-brown enamel hypoplasia TG: 5.4% NTG:0.6% White and/or yellow-brown discoloration of enamel and horizontal enamel hypoplasia TG: 2.0% NTG:0.6% Generalized internal or external white enamel hypoplasia TG: 5.4% NTG: 5.3% | Main material: TG: 57.8% NTG:45.3% | p ≤ 0.05 |
| Machado Lenzi and Colleagues, 2018 [10] | 124 children TG: (permanent teeth whose antecessor had suffered dental trauma): 214 primary teeth CG: (teeth of the same child whose antecessor had not suffered dental trauma): 247 primary teeth Age 0–8 years old | Upper central primary incisors (n = 172, 80%) | Intrusion (38.7%) Concussion (14%) Lateral luxation (11%) Avulsion (11%) Subluxation (7.8%) Extrusion (4.6%) Enamel fracture (3%) Root fracture (3%) Enamel dentin fracture with pulp exposure (1.5%) | Intrusion (55.8% of cases developed malformations) | Enamel fracture mainly for the 2–3 years age group Enamel dentin fracture without pulp exposure mostly for the 1–2 years age group Enamel dentin fracture with pulp exposure mainly for the 3–5 years age group Root fracture mostly for the 4–5 years age group | <1 year: 1 child 1 year: 8 children 2 year: 49 children 3 year: 35 children 4 year: 22 children 5 year: 54 children 6 year: 28 children 7 year: 14 children 8 year: 3 children | Discoloration of enamel CG (5.7%) TG (11.2%) Enamel hypoplasia CG (1.2%) TG (9.8%) Crown dilaceration CG (0%) TG (0.9%) Odontoma-like formation CG (0%) TG (0.5%) Root dilacerations CG (0.4%) TG (0.9 %) Partial arrest of root formations CG (0%) TG (0.5%) Sequestration of tooth germ CG (0%) TG (0.5%) Eruption disturbance CG (0%) TG (4.7%) | TG: 28.9% (n = 62) |
<0.001 for intrusion <0.001 age < 1 year |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caeiro-Villasenín, L.; Serna-Muñoz, C.; Pérez-Silva, A.; Vicente-Hernández, A.; Poza-Pascual, A.; Ortiz-Ruiz, A.J. Developmental Dental Defects in Permanent Teeth Resulting from Trauma in Primary Dentition: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 754. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020754
Caeiro-Villasenín L, Serna-Muñoz C, Pérez-Silva A, Vicente-Hernández A, Poza-Pascual A, Ortiz-Ruiz AJ. Developmental Dental Defects in Permanent Teeth Resulting from Trauma in Primary Dentition: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(2):754. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020754
Chicago/Turabian StyleCaeiro-Villasenín, Lucía, Clara Serna-Muñoz, Amparo Pérez-Silva, Ascensión Vicente-Hernández, Andrea Poza-Pascual, and Antonio José Ortiz-Ruiz. 2022. "Developmental Dental Defects in Permanent Teeth Resulting from Trauma in Primary Dentition: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 2: 754. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19020754