
Caries Risk Assessment Using the Caries Management by Risk Assessment (CAMBRA) Protocol among the General Population of Sakaka, Saudi Arabia—A Cross-Sectional Study

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, Q.; van Palenstein Helderman, W. Caries experience variables as indicators in caries risk assessment in 6–7-year-old Chinese children. J. Dent. 2006, 34, 676–681. [Google Scholar] [CrossRef]
- Suneja, E.S.; Suneja, B.; Tandon, B.; Philip, N.I. An overview of caries risk assessment: Rationale, risk indicators, risk assessment methods, and risk-based caries management protocols. Indian J. Dent. Sci. 2017, 9, 210. [Google Scholar] [CrossRef]
- Brantley, C.F.; Bader, J.D.; Shugars, D.A.; Nesbit, S.P. Does the cycle of rerestoration lead to larger restorations? J. Am. Dent. Assoc. 1995, 126, 1407–1413. [Google Scholar] [CrossRef] [PubMed]
- Mejàre, I.; Axelsson, S.; Dahlën Ga Espelid, I.; Norlund, A.; Tranæus, S.; Twetman, S. Caries risk assessment. A systematic review. Acta Odontol. Scand. 2014, 72, 81–91. [Google Scholar] [CrossRef]
- Bratthall, D.; Hänsel Petersson, G. Cariogram–a multifactorial risk assessment model for a multifactorial disease. Community Dent. Oral Epidemiol. 2005, 33, 256–264. [Google Scholar] [CrossRef]
- Senneby, A.; Mejàre, I.; Sahlin, N.-E.; Svensäter, G.; Rohlin, M. Diagnostic accuracy of different caries risk assessment methods. A systematic review. J. Dent. 2015, 43, 1385–1393. [Google Scholar] [CrossRef]
- Holgerson, P.L.; Twetman, S.; Stecksèn-Blicks, C. Validation of an age-modified caries risk assessment program (Cariogram) in preschool children. Acta Odontol. Scand. 2009, 67, 106–112. [Google Scholar] [CrossRef]
- Featherstone, J.D. The caries balance: The basis for caries management by risk assessment. Oral Health Prev. Dent. 2004, 2, 259–264. [Google Scholar]
- Chaffee, B.W.; Cheng, J.; Featherstone, J.D. Non-operative anti-caries agents and dental caries increment among adults at high caries risk: A retrospective cohort study. BMC Oral Health 2015, 15, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Featherstone, J.D.; Crystal, Y.O.; Alston, P.; Chaffee, B.W.; Doméjean, S.; Rechmann, P.; Zhan, L.; Ramos-Gomez, F. A Comparison of Four Caries Risk Assessment Methods. Front. Oral Health 2021, 2, 15. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.D.; Domejean-Orliaguet, S.; Jenson, L.; Wolff, M.; Young, D.A. Caries risk assessment in practice for age 6 through adult. CDA 2007, 35, 703. [Google Scholar]
- Sudhir, K.M.; Kanupuru, K.K.; Fareed, N.; Mahesh, P.; Vandana, K.; Chaitra, N.T. CAMBRA as a Tool for Caries Risk Prediction Among 12-to 13-year-old Institutionalised Children-A Longitudinal Follow-up Study. Oral Health Prev. Dent. 2016, 14, 355–362. [Google Scholar] [PubMed]
- Almusawi, M.; Gosadi, I.; Abidia, R.; Almasawi, M.; Khan, H. Potential risk factors for dental caries in Type 2 diabetic patients. Int. J. Dent. Hyg. 2018, 16, 467–475. [Google Scholar] [CrossRef]
- Mu, M. Caries Risk Assessment and its Association with Socio-demographic Factors among General Population of Lahore, Pakistan. Biomedica 2019, 35, 131. [Google Scholar]
- Khallaf, Y.S.; Hafez, S.; Shaalan, O.O. Evaluation of ICCMS versus CAMBRA Caries Risk Assessment Models Acquisition on Treatment Plan in Young Adult Population: A Randomized Clinical Trial. Clin. Cosmet. Investig. Dent. 2021, 13, 293. [Google Scholar] [CrossRef] [PubMed]
- Farsi, N.; Merdad, L.; Mirdad, S. Caries risk assessment in preschool children in Saudi Arabia. Oral Health Prev. Dent. 2013, 11, 271–280. [Google Scholar] [PubMed]
- Chaudhary, F.A.; Ahmad, B.; Bashir, U. Dental health status and oral health behaviours of patients with facial burn in Pakistan. BMC Oral Health 2019, 19, 1–10. [Google Scholar] [CrossRef]
- Chaudhary, F.A.; Ahmad, B.; Javed, M.Q.; Yakub, S.S.; Arjumand, B.; Khan, A.M.; Mustafa, S. The Relationship of Orofacial Pain and Dental Health Status and Oral Health Behaviours in Facial Burn Patients. Pain Res. Manag. 2021, 2021, 5512755. [Google Scholar] [CrossRef]
- Maheswari, S.U.; Raja, J.; Kumar, A.; Seelan, R.G. Caries management by risk assessment: A review on current strategies for caries prevention and management. J. Pharm. Bioallied Sci. 2015, 7, S320. [Google Scholar]
- Doméjean, S.; White, J.M.; Featherstone, J. Validation of the CDA CAMBRA caries risk assessment—A six-year retrospective study. J. Calif. Dent. Assoc. 2011, 39, 709–715. [Google Scholar]
- Featherstone, J.; Chaffee, B. The evidence for caries management by risk assessment (CAMBRA®). Adv. Dent. Res. 2018, 29, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Featherstone, J.; White, J.; Hoover, C.; Rapozo-Hilo, M.; Weintraub, J.; Wilson, R.; Zhan, L.; Gansky, S. A randomized clinical trial of anticaries therapies targeted according to risk assessment (caries management by risk assessment). Caries Res. 2012, 46, 118–129. [Google Scholar] [CrossRef] [Green Version]
- Chaudhary, F.A.; Ahmad, B.; Sinor, M.Z. The severity of facial burns, dental caries, periodontal disease, and oral hygiene impact oral health-related quality of life of burns victims in Pakistan: A cross-sectional study. BMC Oral Health 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, F.A.; Ahmad, B. The relationship between psychosocial distress and oral health status in patients with facial burns and mediation by oral health behaviour. BMC Oral Health 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Muhson, Z.N.; Thabit, S.; Al-ward, F.S.; Al Shatari, S.A. Caries risk assessment of a sample of children attending preventive specialized dental center in Al Resafa, Baghdad. J. Baghdad Coll. Dent. 2020, 32, 17–24. [Google Scholar] [CrossRef]
- Rechmann, P.; Chaffee, B.; Rechmann, B.; Featherstone, J. Changes in caries risk in a practice-based randomized controlled trial. Adv. Dent. Res. 2018, 29, 15–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- da Silva Jorge, V.C.; Câmara, J.V.F.; da Silveira Pereira, G.D.; Barbosa, I.F.; de Carvalho Vianna, R.F.; de Campos, P.R.B.; Fried, H.; Groisman, S. Evaluation of caries risk in pre-school children using the CAMBRA protocol and CAST index. Braz. J. Dev. 2021, 7, 26944–26954. [Google Scholar] [CrossRef]
- Al-Shammery, A.R. Caries experience of urban and rural children in Saudi Arabia. J. Public Health Dent. 1999, 59, 60–64. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Groups | Number (%) |
|---|---|---|
| Gender | Male | 82 (51.2) |
| Female | 78 (48.8) | |
| Age groups (years) | Group I (6 to 19 years) | 0 |
| Group II (20 to 29 years) | 42 (26.2) | |
| Group III (30 to 39 years) | 42 (26.2) | |
| Group IV (40 to 49 years) | 46 (28.8) | |
| Group V (50 to 59 years) | 16 (10.0) | |
| Group VI (above 60 years) | 14 (8.8) | |
| Residence | Rural | 51 (31.9) |
| Urban | 109 (68.1) | |
| Education | Primary school and below = 1 | 45 (28.1) |
| Secondary school = 2 | 54 (33.7) | |
| Bachelor = 3 | 35 (21.9) | |
| Diploma = 4 | 12 (7.5) | |
| Master = 5 | 10 (6.3) | |
| PhD = 6 | 4 (2.5) |
| Disease Indicators | N (%) |
|---|---|
| Visible cavities or radiographic penetration of the dentin | 112 (70.0) |
| Radiographic approximal enamel lesions (not in dentin) | 111 (69.4) |
| White spots on smooth surfaces | 114 (71.3) |
| Restorations in last three years | 89 (55.6) |
| Risk Factors | |
| Visible heavy plaque on teeth | 132 (82.5) |
| Frequent snack (> 3 × daily between meals) | 107 (66.9) |
| Deep pits and fissures | 110 (68.8) |
| Recreational drug use | 45 (28.1) |
| Inadequate saliva flow by observation | 33 (20.6) |
| Saliva reducing factors (medications/radiation/systemic) | 17 (10.6) |
| Exposed roots | 30 (18.8) |
| Orthodontic appliances | 43 (26.9) |
| Protective Factors | |
| Home/work/school is a fluoridated community | 39 (24.4) |
| Fluoride toothpaste at least once daily | 148 (92.5) |
| Fluoride toothpaste at least 2 × daily | 68 (42.5) |
| Fluoride mouth rinse (0.05% NaF) daily | 8 (5.0) |
| Fluoride varnish in last six months | 12 (7.5) |
| Chlorhexidine prescribed/used one week each of last six months | 38 (23.8) |
| Xylitol gum/lozenges 4 × daily last six months | 14 (8.8) |
| Calcium and phosphate paste during last six months | 4 (2.5) |
| Caries Risk | p-Value | |||
|---|---|---|---|---|
| High | Moderate | |||
| N (%) | N (%) | |||
| Age group | 6 to 19 years | 22 (52.4) | 20 (47.6) | <0.001 |
| 20 to 29 years | 39 (92.9) | 3 (7.1) | ||
| 30 to 39 years | 45 (97.8) | 1 (2.2) | ||
| 40 to 49 years | 16 (100.0) | 0 | ||
| 50 to 59 years | 14 (100.0) | 0 | ||
| Gender | Males | 71 (86.6) | 11(13.4) | 0.66 |
| Females | 65 (83.3) | 13 (16.7) | ||
| Resident | Rural | 48 (94.1) | 3 (5.9) | 0.032 |
| Urban | 88 (80.7) | 21 (19.3) | ||
| Education | Primary | 27 (60.0) | 18 (40.0) | <0.001 |
| Secondary | 53 (98.1) | 1 (1.9) | ||
| Bachelor | 30 (85.7) | 5 (14.3) | ||
| Diploma | 12 (100.0) | 0 | ||
| Masters | 10 (100.0) | 0 | ||
| PhD | 4 (100.0) | 0 | ||
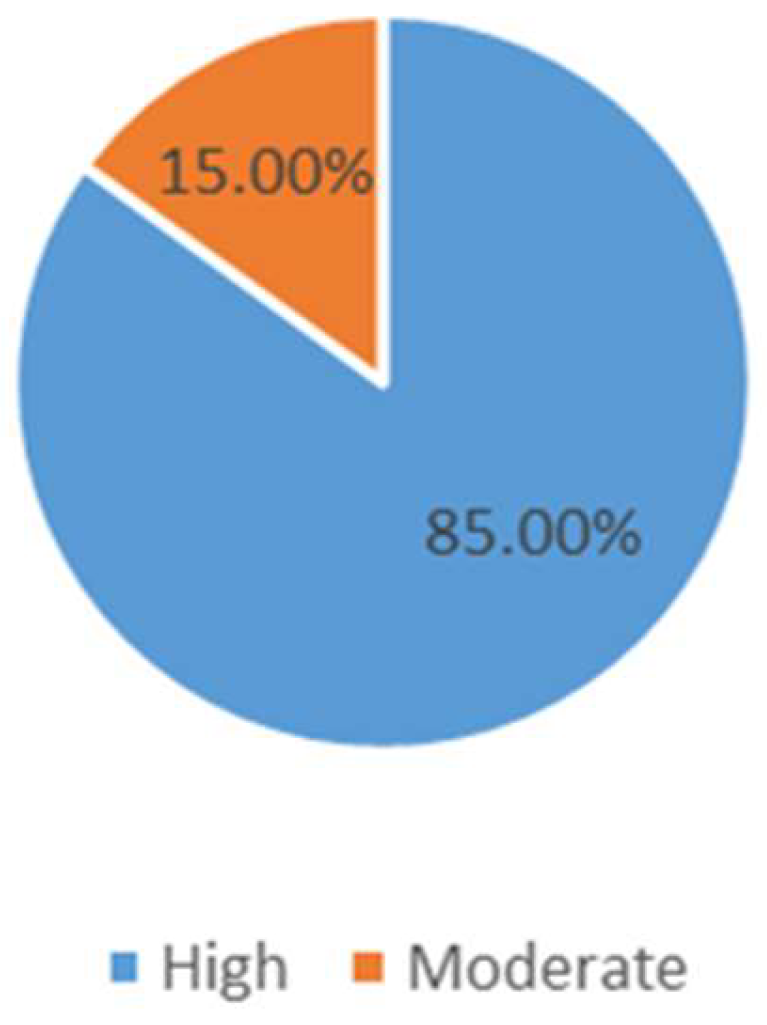
| Total | 136 (85.0) | 24 (15.0) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iqbal, A.; Khattak, O.; Chaudhary, F.A.; Onazi, M.A.A.; Algarni, H.A.; AlSharari, T.; Alshehri, A.; Mustafa, M.; Issrani, R.; Alghamdi, E.Y.M.; et al. Caries Risk Assessment Using the Caries Management by Risk Assessment (CAMBRA) Protocol among the General Population of Sakaka, Saudi Arabia—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 1215. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031215
Iqbal A, Khattak O, Chaudhary FA, Onazi MAA, Algarni HA, AlSharari T, Alshehri A, Mustafa M, Issrani R, Alghamdi EYM, et al. Caries Risk Assessment Using the Caries Management by Risk Assessment (CAMBRA) Protocol among the General Population of Sakaka, Saudi Arabia—A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1215. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031215
Chicago/Turabian StyleIqbal, Azhar, Osama Khattak, Farooq Ahmad Chaudhary, Meshal Aber Al Onazi, Hmoud Ali Algarni, Thani AlSharari, Abdullah Alshehri, Mohammed Mustafa, Rakhi Issrani, Ebtehal Yanallah Mohamed Alghamdi, and et al. 2022. "Caries Risk Assessment Using the Caries Management by Risk Assessment (CAMBRA) Protocol among the General Population of Sakaka, Saudi Arabia—A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 3: 1215. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031215