
Oral Hygiene Practices and Knowledge among Adolescents Aged between 15 and 17 Years Old during Fixed Orthodontic Treatment: Multicentre Study Conducted in France

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site and Population
2.2. Ethics
2.3. Measurement Tool
2.4. Statistical Method
3. Results
3.1. Patient Characteristics
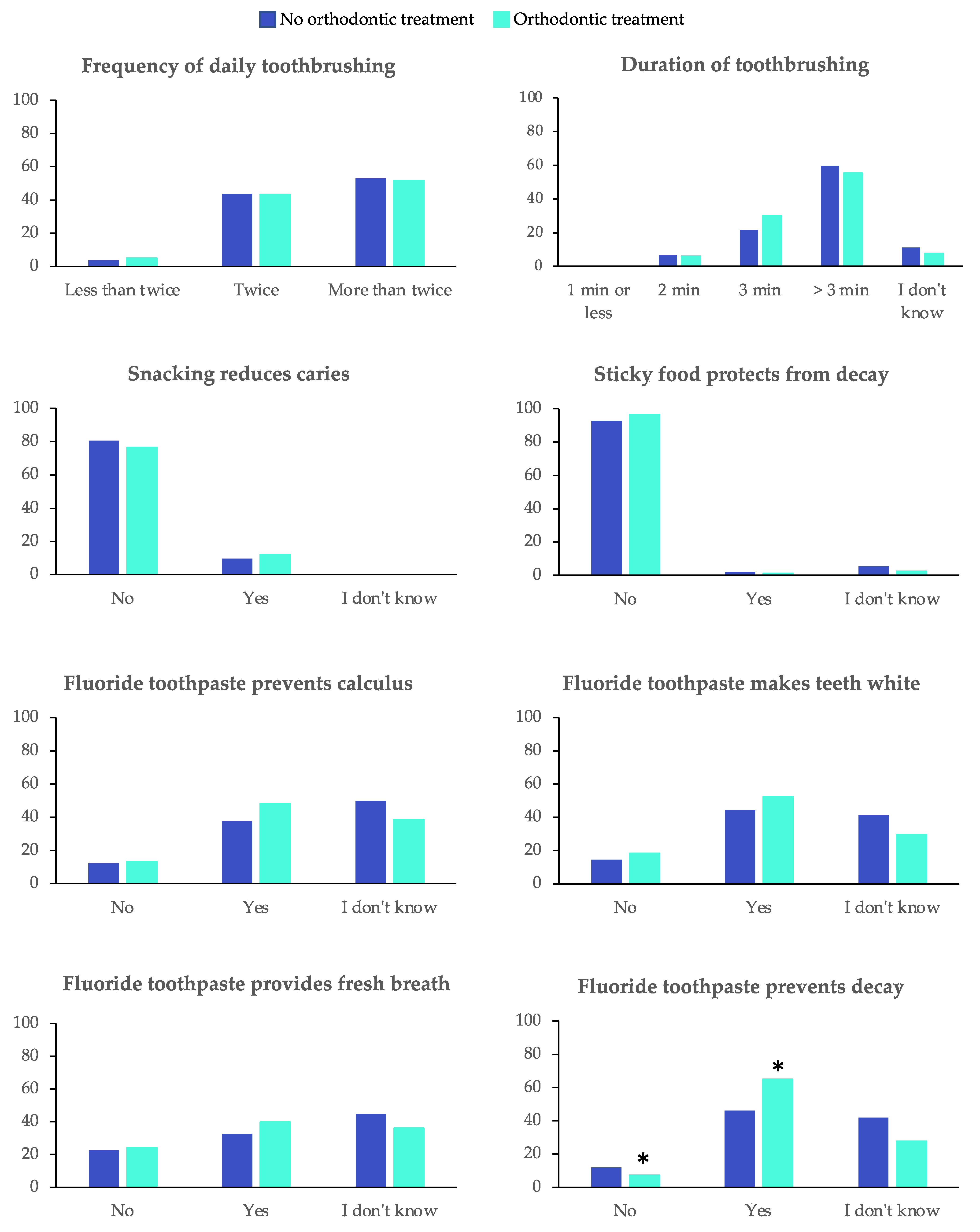
3.2. Assessment of Adolescents’ Knowledge regarding Prevention of Oral Diseases
3.3. Assessment of Adolescents’ Attitudes and Practices towards Oral Health
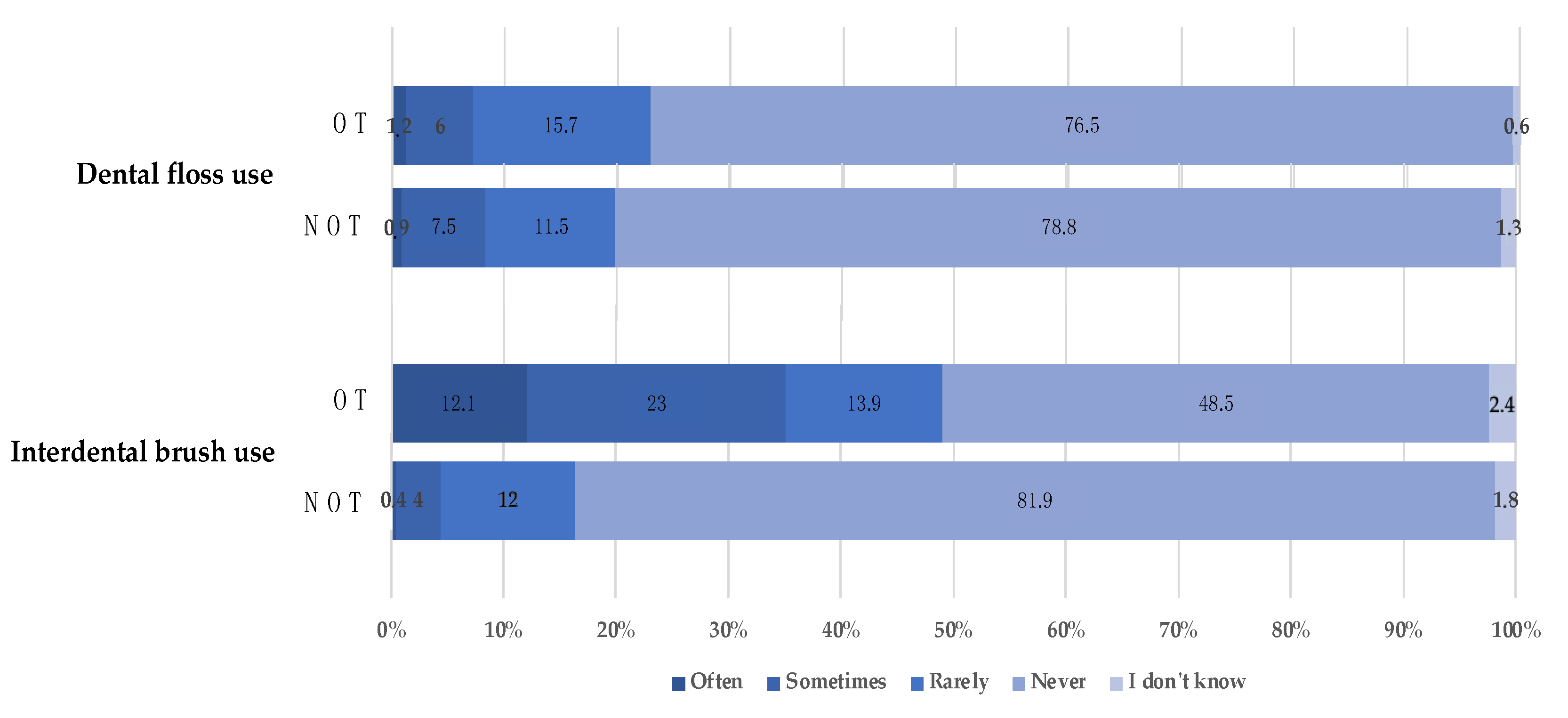
3.3.1. Oral Hygiene Habits
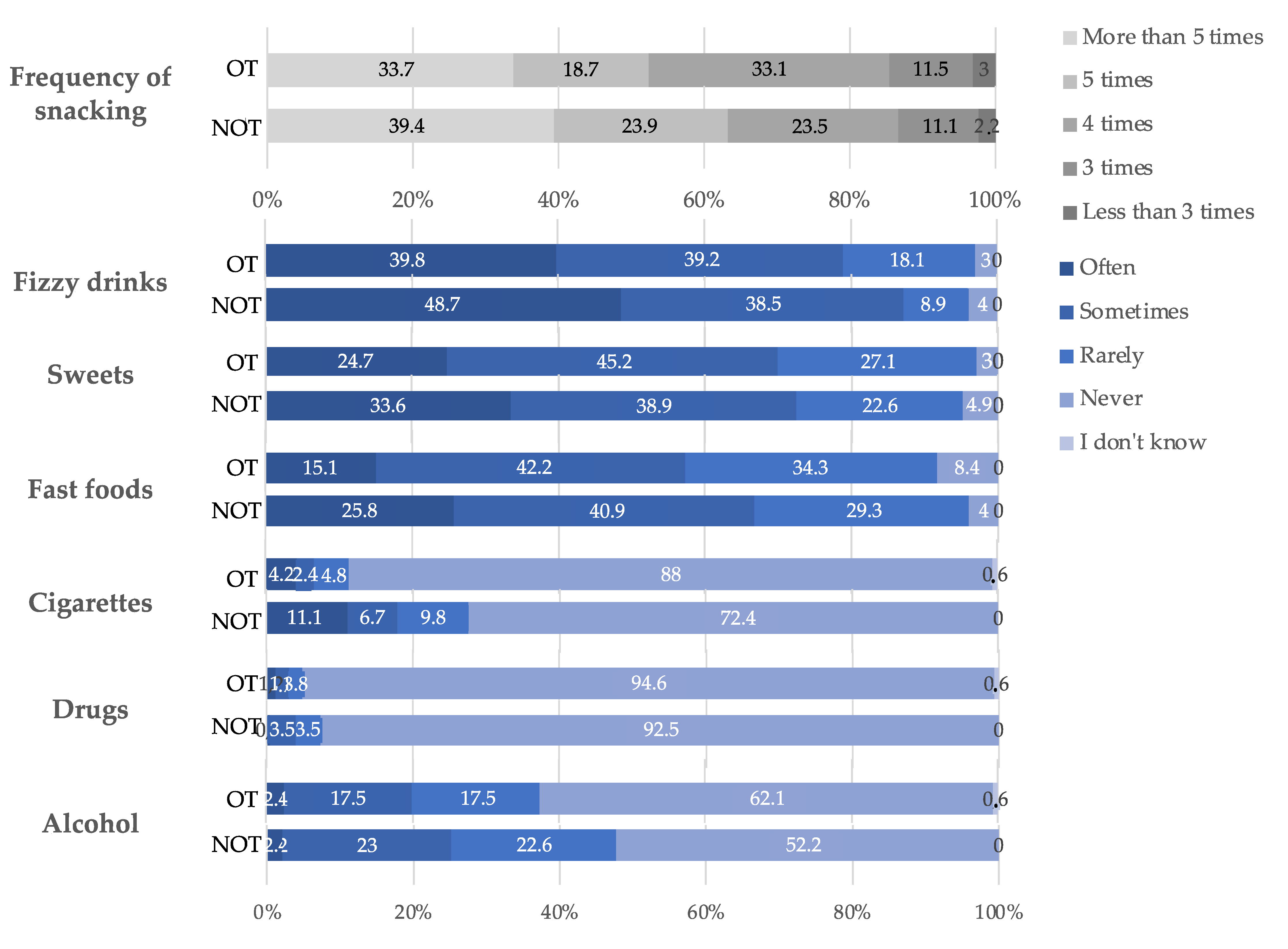
3.3.2. Nutrition and Harmful Habits
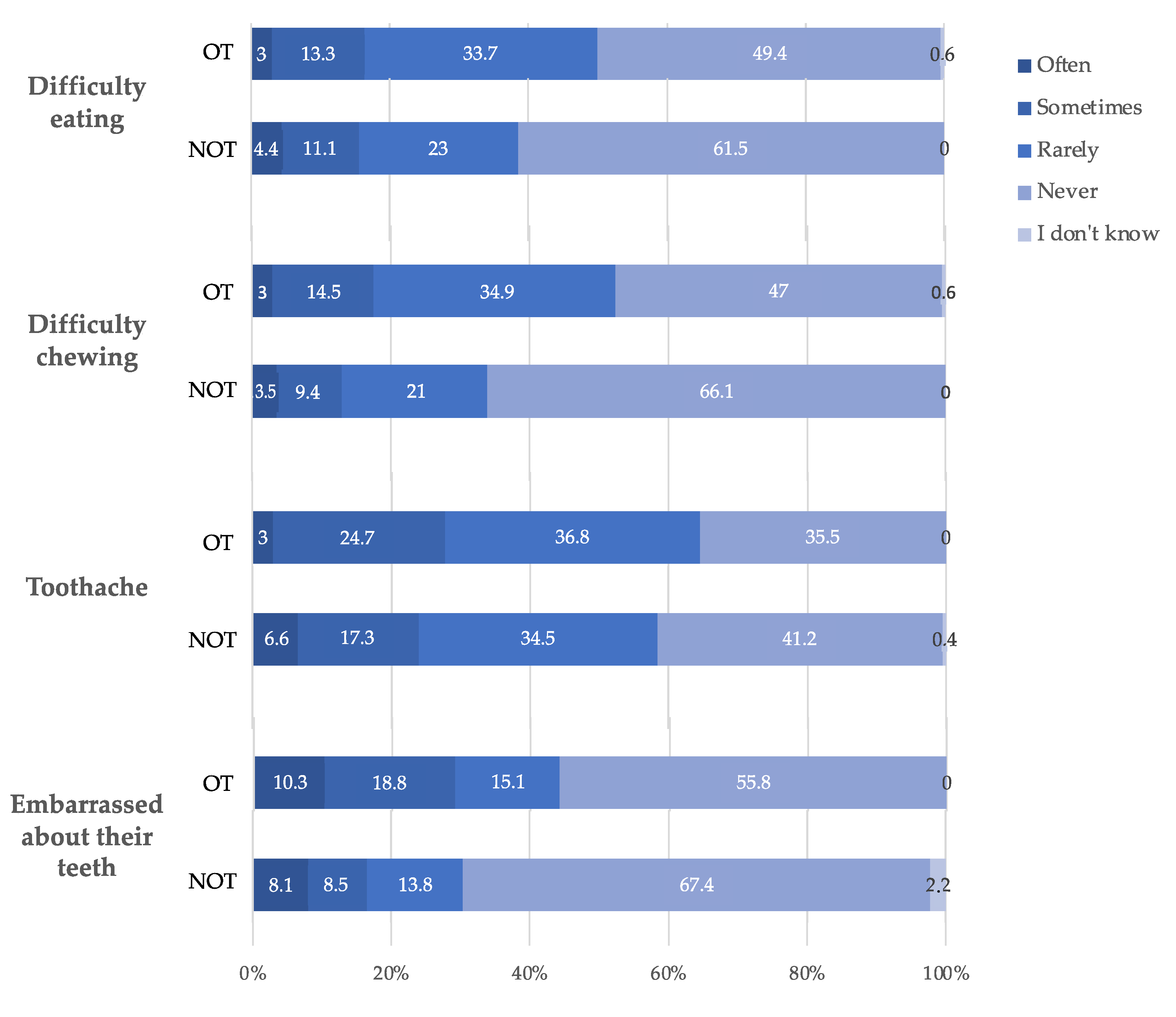
3.4. Self-Perception of Oral and General Health
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Petersen, P.E. The World Oral Health Report 2003: Continuous Improvement of Oral Health in the 21st Century—The Approach of the WHO Global Oral Health Programme. Community Dent. Oral Epidemiol. 2003, 31, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.L.; Vann, W.F.; Kotch, J.B.; Pahel, B.T.; Lee, J.Y. Impact of Poor Oral Health on Children’s School Attendance and Performance. Am. J. Public Health 2011, 101, 1900–1906. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Bernabé, E.; Dahiya, M.; Bhandari, B.; Murray, C.J.L.; Marcenes, W. Global Burden of Untreated Caries: A Systematic Review and Metaregression. J. Dent. Res. 2015, 94, 650–658. [Google Scholar] [CrossRef]
- Califano, J.V.; AAP. AAPD Periodontal Diseases of Children and Adolescents. Pediatr. Dent. 2005, 27, 189–196. [Google Scholar] [PubMed]
- Coolidge, T.; Heima, M.; Johnson, E.K.; Weinstein, P. The Dental Neglect Scale in Adolescents. BMC Oral Health 2009, 9, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Ghutaimel, H.; Riba, H.; Al-Kahtani, S.; Al-Duhaimi, S. Common Periodontal Diseases of Children and Adolescents. Int. J. Dent. 2014, 2014, 850674. [Google Scholar] [CrossRef] [PubMed]
- Agustsdottir, H.; Gudmundsdottir, H.; Eggertsson, H.; Jonsson, S.H.; Gudlaugsson, J.O.; Saemundsson, S.R.; Eliasson, S.T.; Arnadottir, I.B.; Holbrook, W.P. Caries Prevalence of Permanent Teeth: A National Survey of Children in Iceland Using ICDAS. Community Dent. Oral Epidemiol. 2010, 38, 299–309. [Google Scholar] [CrossRef]
- Fleming, E.; Afful, J. Prevalence of Total and Untreated Dental Caries Among Youth: United States, 2015–2016. NCHS Data Brief 2018, 307, 1–8. [Google Scholar]
- Olczak-Kowalczyk, D.; Gozdowski, D.; Kaczmarek, U. Oral Health in Polish Fifteen-Year-Old Adolescents. Oral Health Prev. Dent. 2019, 17, 139–146. [Google Scholar] [CrossRef]
- Jordao, L.M.R.; Vasconcelos, D.N.; Moreira, R.D.S.; Freire, M.D.C.M. Individual and Contextual Determinants of Periodontal Health in 12-Year-Old Schoolchildren in a Brazilian Capital City. Int. J. Dent. 2012, 2012, 325475. [Google Scholar] [CrossRef] [Green Version]
- Das, U.M.; Vadakkekuttical, R.J.; Kanakkath, H.; Shankunni, S.P. Dental Health Awareness, Attitude, and Dental Health-Care Seeking Practices as Risk Indicators for the Prevalence of Periodontal Disease among 15–17-Year-Old School Children in Kozhikode District, Kerala, India. J. Indian Soc. Periodontol. 2017, 21, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Albandar, J.M.; Rams, T.E. Global Epidemiology of Periodontal Diseases: An Overview. Periodontol. 2000 2002, 29, 7–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brukiene, V.; Aleksejuniene, J. Theory-Based Oral Health Education in Adolescents. Stomatologija 2010, 12, 3–9. [Google Scholar] [PubMed]
- Silk, H.; Kwok, A. Addressing Adolescent Oral Health: A Review. Pediatr. Rev. 2017, 38, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.T.; Corrêa, J.D.; Silva, T.A. The Oral Microbiota Is Modified by Systemic Diseases. J. Dent. Res. 2019, 98, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Lamont, R.J. Beyond the Red Complex and into More Complexity: The Polymicrobial Synergy and Dysbiosis (PSD) Model of Periodontal Disease Etiology. Mol. Oral Microbiol. 2012, 27, 409–419. [Google Scholar] [CrossRef] [Green Version]
- Lamont, R.J.; Hajishengallis, G. Polymicrobial Synergy and Dysbiosis in Inflammatory Disease. Trends Mol. Med. 2015, 21, 172–183. [Google Scholar] [CrossRef] [Green Version]
- Tanner, A.C.R.; Kressirer, C.A.; Rothmiller, S.; Johansson, I.; Chalmers, N.I. The Caries Microbiome: Implications for Reversing Dysbiosis. Adv. Dent. Res. 2018, 29, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Hajishengallis, G. Immunomicrobial Pathogenesis of Periodontitis: Keystones, Pathobionts, and Host Response. Trends Immunol. 2014, 35, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Inquimbert, C.; Bourgeois, D.; Bravo, M.; Viennot, S.; Tramini, P.; Llodra, J.C.; Molinari, N.; Dussart, C.; Giraudeau, N.; Carrouel, F. The Oral Bacterial Microbiome of Interdental Surfaces in Adolescents According to Carious Risk. Microorganisms 2019, 7, 319. [Google Scholar] [CrossRef] [Green Version]
- Tarannum, F.; Faizuddin, M.; Swamy, S.; Hemalata, M. Efficacy of a New Interdental Cleaning Aid. J. Indian Soc. Periodontol. 2012, 16, 375–380. [Google Scholar] [CrossRef] [PubMed]
- Ng, E.; Lim, L.P. An Overview of Different Interdental Cleaning Aids and Their Effectiveness. Dent. J. 2019, 7, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourgeois, D.; Saliasi, I.; Llodra, J.C.; Bravo, M.; Viennot, S.; Carrouel, F. Efficacy of Interdental Calibrated Brushes on Bleeding Reduction in Adults: A 3-Month Randomized Controlled Clinical Trial. Eur. J. Oral Sci. 2016, 124, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, D.; Bravo, M.; Llodra, J.-C.; Inquimbert, C.; Viennot, S.; Dussart, C.; Carrouel, F. Calibrated Interdental Brushing for the Prevention of Periodontal Pathogens Infection in Young Adults—A Randomized Controlled Clinical Trial. Sci. Rep. 2019, 9, 15127. [Google Scholar] [CrossRef] [Green Version]
- Baskaradoss, J.K. Relationship between Oral Health Literacy and Oral Health Status. BMC Oral Health 2018, 18, 1–6. [Google Scholar] [CrossRef]
- Berkman, N.D.; Davis, T.C.; McCormack, L. Health Literacy: What Is It? J. Health Commun. 2010, 15 (Suppl. 2), 9–19. [Google Scholar] [CrossRef]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low Health Literacy and Health Outcomes: An Updated Systematic Review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef]
- Paulander, J.; Axelsson, P.; Lindhe, J. Association between Level of Education and Oral Health Status in 35-, 50-, 65- and 75-Year-Olds. J. Clin. Periodontol. 2003, 30, 697–704. [Google Scholar] [CrossRef]
- El Osta, N.; Pichot, H.; Soulier-Peigue, D.; Hennequin, M.; Tubert-Jeannin, S. Validation of the Child Oral Health Impact Profile (COHIP) French Questionnaire among 12 Years-Old Children in New Caledonia. Health Qual. Life Outcomes 2015, 13, 176. [Google Scholar] [CrossRef] [Green Version]
- Himida, T.; Promise, U. School-Based Dental Sealant Programmes May Be Effective in Caries Prevention. Evid. Based Dent. 2017, 18, 13–14. [Google Scholar] [CrossRef]
- Nihtila, A.; West, N.; Lussi, A.; Bouchard, P.; Ottolenghi, L.; Senekola, E.; Llodra, J.C.; Viennot, S.; Bourgeois, D. Oral Health Behavior and Lifestyle Factors among Overweight and Non-Overweight Young Adults in Europe: A Cross-Sectional Questionnaire Study. Healthcare 2016, 4, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malinowska-Cieślik, M.; Mazur, J.; Nałęcz, H.; Małkowska-Szkutnik, A. Social and Behavioral Predictors of Adolescents’ Positive Attitude towards Life and Self. Int. J. Environ. Res. Public. Health 2019, 16, 4404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahengbam, P.P.; Kshetrimayum, N.; Wahengbam, B.S.; Nandkeoliar, T.; Lyngdoh, D. Assessment of Oral Health Knowledge, Attitude and Self-Care Practice Among Adolescents—A Statewide Cross-Sectional Study in Manipur, Northeastern India. J. Clin. Diagn. Res. JCDR 2016, 10, ZC65–ZC70. [Google Scholar] [CrossRef] [PubMed]
- Blaggana, A.; Grover, V.; Anjali; Kapoor, A.; Blaggana, V.; Tanwar, R.; Kaur, H.; Haneet, R.K. Oral Health Knowledge, Attitudes and Practice Behaviour among Secondary School Children in Chandigarh. J. Clin. Diagn. Res. JCDR 2016, 10, ZC01–ZC06. [Google Scholar] [CrossRef]
- Graça, S.R.; Albuquerque, T.S.; Luis, H.S.; Assunção, V.A.; Malmqvist, S.; Cuculescu, M.; Slusanschi, O.; Johannsen, G.; Galuscan, A.; Podariu, A.C.; et al. Oral Health Knowledge, Perceptions, and Habits of Adolescents from Portugal, Romania, and Sweden: A Comparative Study. J. Int. Soc. Prev. Community Dent. 2019, 9, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Al-Qahtani, S.M.; Razak, P.A.; Khan, S.D. Knowledge and Practice of Preventive Measures for Oral Health Care among Male Intermediate Schoolchildren in Abha, Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prasai Dixit, L.; Shakya, A.; Shrestha, M.; Shrestha, A. Dental Caries Prevalence, Oral Health Knowledge and Practice among Indigenous Chepang School Children of Nepal. BMC Oral Health 2013, 13, 20. [Google Scholar] [CrossRef] [Green Version]
- Jensen, O.; Gabre, P.; Sköld, U.M.; Birkhed, D. Fluoride Toothpaste and Toothbrushing; Knowledge, Attitudes and Behaviour among Swedish Adolescents and Adults. Swed. Dent. J. 2011, 35, 203–213. [Google Scholar]
- Al-Darwish, M.S. Oral Health Knowledge, Behaviour and Practices among School Children in Qatar. Dent. Res. J. 2016, 13, 342–353. [Google Scholar] [CrossRef]
- Aljohani, S.R.; Alsaggaf, D.H. Adherence to Dietary Advice and Oral Hygiene Practices Among Orthodontic Patients. Patient Prefer. Adherence 2020, 14, 1991–2000. [Google Scholar] [CrossRef]
- Pandey, V.; Chandra, S.; Dilip Kumar, H.P.; Gupta, A.; Bhandari, P.P.; Rathod, P. Impact of Dental Neglect Score on Oral Health among Patients Receiving Fixed Orthodontic Treatment: A Cross-Sectional Study. J. Int. Soc. Prev. Community Dent. 2016, 6, 120–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anuwongnukroh, N.; Dechkunakorn, S.; Kanpiputana, R. Oral Hygiene Behavior during Fixed Orthodontic Treatment. Dentistry 2017, 7, 1–5. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | No Orthodontic Treatment (n = 266) | Orthodontic Treatment (n = 166) | p-Value (Chi-square) | |
|---|---|---|---|---|
| Age | Years (Mean ± SD) | 16.48 ± 0.53 | 16.38 ± 0.49 | |
| Gender | Males (%) | 56.6 | 53.6 | 0.552 |
| Females (%) | 43.4 | 46.4 | ||
| Father’s occupation | Farm worker/Shopkeeper (%) | 11.1 | 10.3 | 0.129 |
| Executive/Company manager (%) | 24.8 | 30.7 | ||
| Administration (%) | 17.7 | 9.6 | ||
| Employee/Manual worker (%) | 29.6 | 37.4 | ||
| Unemployed/Disabled/Deceased (%) | 7.5 | 7.2 | ||
| Unknown (%) | 9.3 | 4.8 | ||
| Mother’s occupation | Farm worker/Shopkeeper (%) | 5.7 | 3.6 | 0.060 |
| Executive/Company manager (%) | 15.9 | 22.3 | ||
| Administration (%) | 29.7 | 23.5 | ||
| Employee/Manual worker (%) | 21.7 | 32.5 | ||
| Unemployed/Disabled/Deceased (%) | 19.5 | 15.7 | ||
| Unknown (%) | 7.5 | 2.4 | ||
| Any medical aid | No (%) | 29.7 | 18.7 | 0.013 |
| Yes (%) | 70.3 | 81.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Inquimbert, C.; Clement, C.; Couatarmanach, A.; Tramini, P.; Bourgeois, D.; Carrouel, F. Oral Hygiene Practices and Knowledge among Adolescents Aged between 15 and 17 Years Old during Fixed Orthodontic Treatment: Multicentre Study Conducted in France. Int. J. Environ. Res. Public Health 2022, 19, 2316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042316
Inquimbert C, Clement C, Couatarmanach A, Tramini P, Bourgeois D, Carrouel F. Oral Hygiene Practices and Knowledge among Adolescents Aged between 15 and 17 Years Old during Fixed Orthodontic Treatment: Multicentre Study Conducted in France. International Journal of Environmental Research and Public Health. 2022; 19(4):2316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042316
Chicago/Turabian StyleInquimbert, Camille, Celine Clement, Antoine Couatarmanach, Paul Tramini, Denis Bourgeois, and Florence Carrouel. 2022. "Oral Hygiene Practices and Knowledge among Adolescents Aged between 15 and 17 Years Old during Fixed Orthodontic Treatment: Multicentre Study Conducted in France" International Journal of Environmental Research and Public Health 19, no. 4: 2316. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042316