
Cost-Effectiveness of PET/CT Surveillance Schedules to Detect Distant Recurrence of Resected Stage III Melanoma

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Cohort
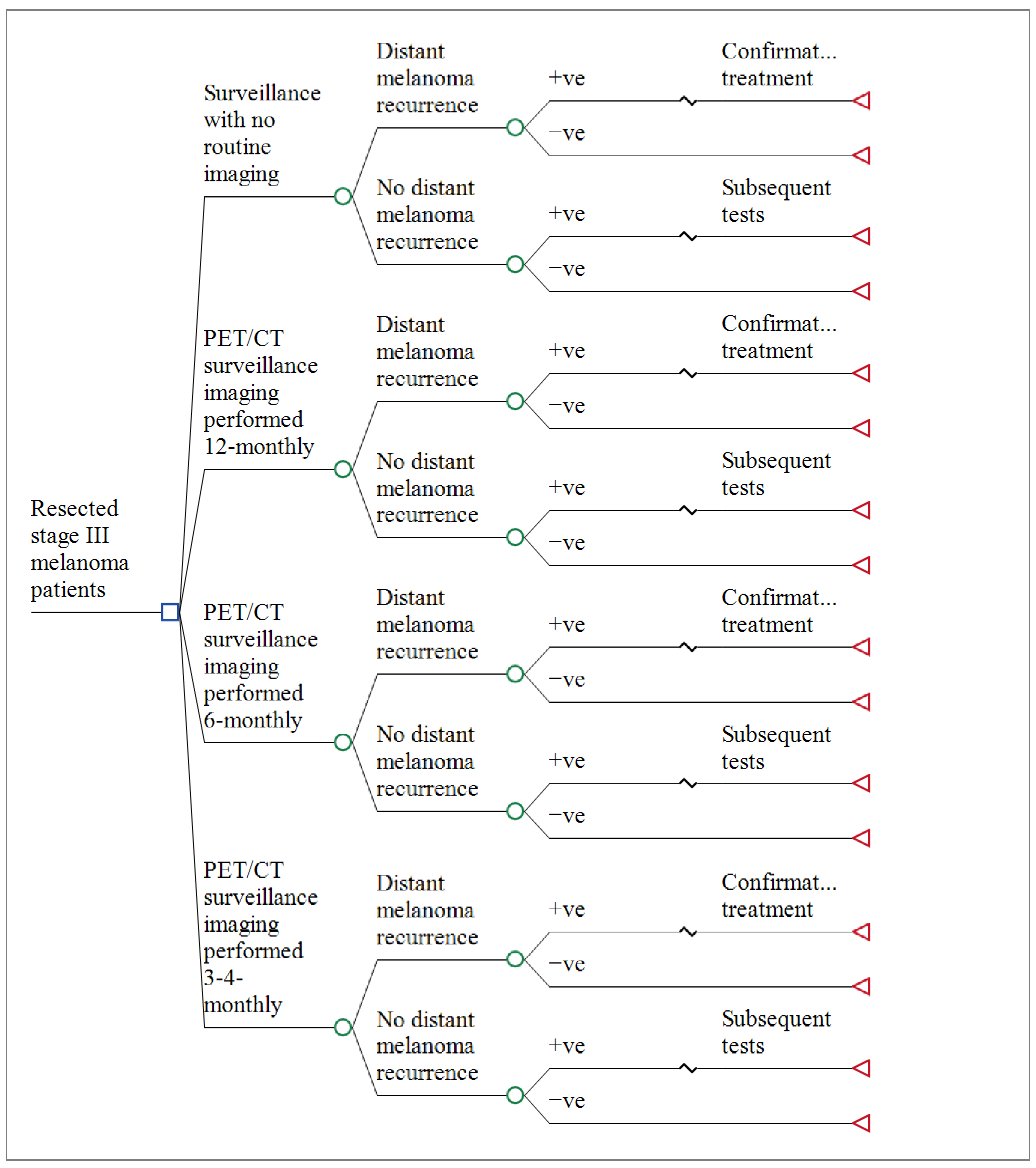
2.2. Decision Model Structure
2.3. Model Assumptions
- Surveillance imaging was primarily used to identify distant recurrence; therefore, loco-regional recurrences were excluded.
- A first distant recurrence only occurs once. Therefore, the model simulates the costs and benefits up to the first (initial) distant recurrence.
- Based on Australian guidelines [7], patients with positive imaging test results underwent confirmatory investigations, including fine-needle aspiration biopsy (FNAB) and whole-body PET/CT (if CT only was previously undertaken).
- All patients with distant melanoma detected underwent treatment.
- The costs for unresectable stage III or stage IV melanoma treatment included diagnostic imaging, doctors’ visits, genetic testing, and pharmacotherapies where relevant, as well as costs for management of Grade 3 and 4 adverse events from treatment modalities (e.g., colitis) [29].
- Radiation-attributable malignancies from PET/CT imaging were not included because these generally take >5 years to develop.
- Costs of palliative and end of life care were excluded because patients were censored after the development of distant disease.
2.4. Model Inputs
2.5. Base Case Analysis
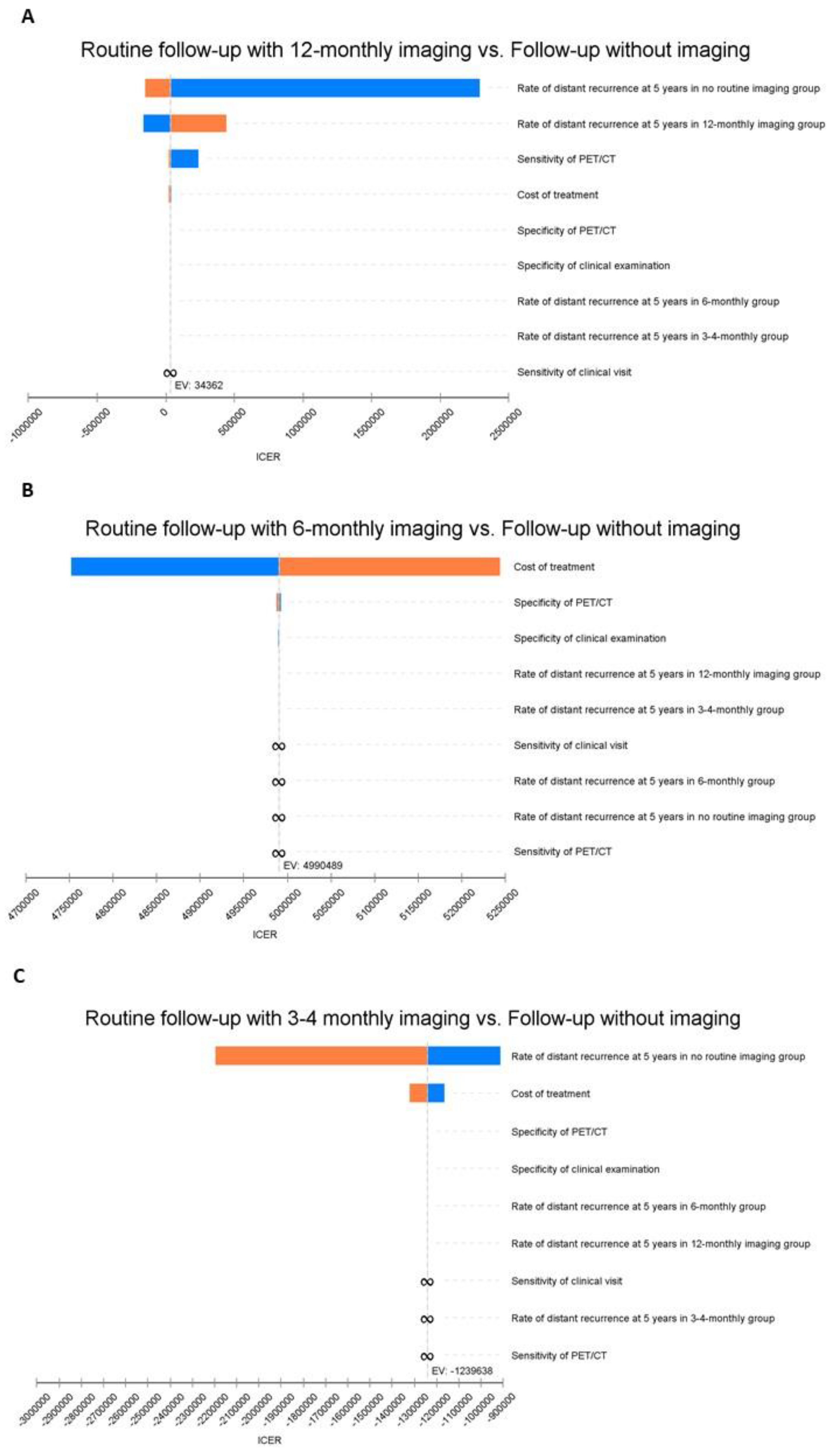
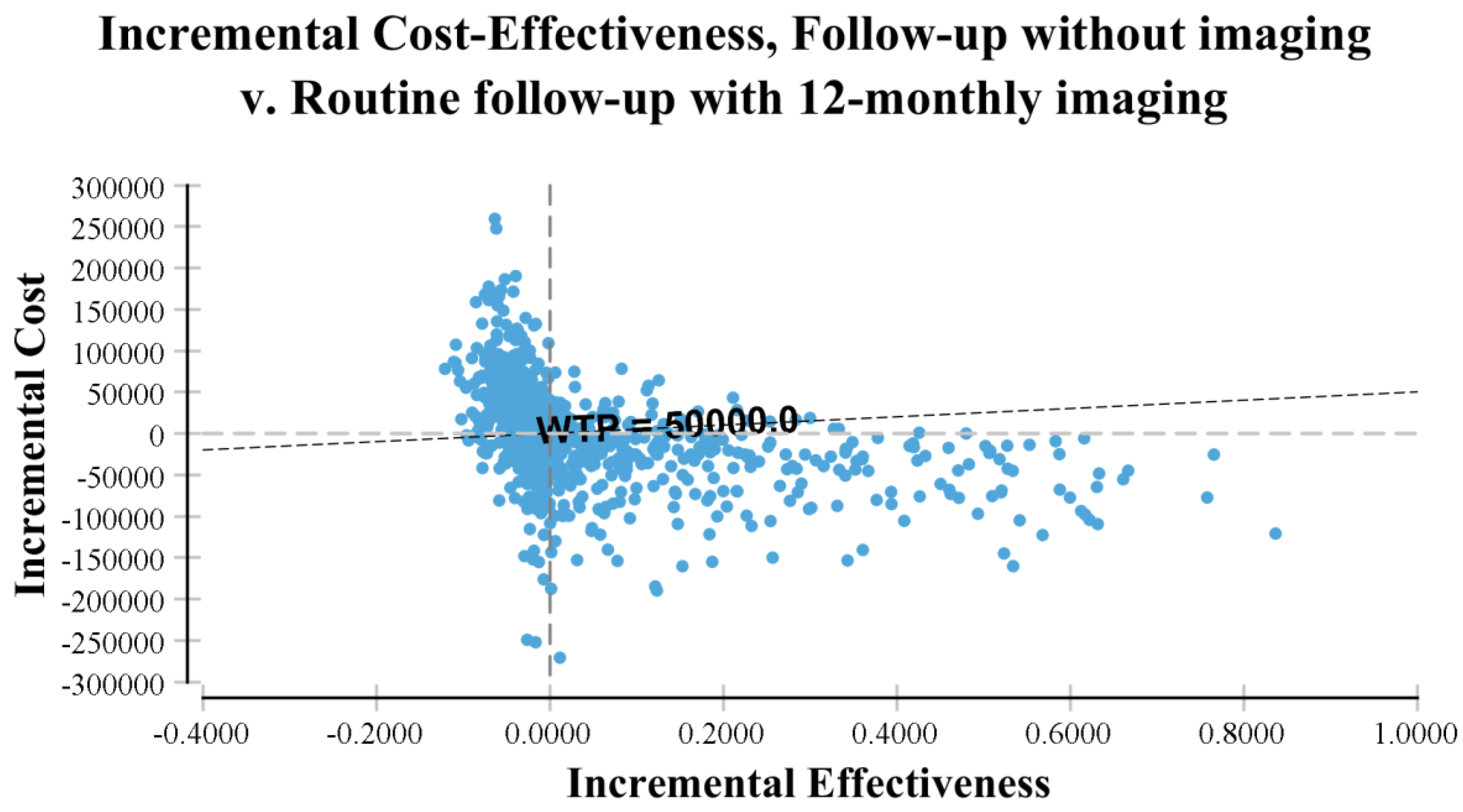
2.6. Sensitivity Analyses
3. Results
Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Nakamura, Y.; Kitano, S.; Takahashi, A.; Tsutsumida, A.; Namikawa, K.; Tanese, K.; Abe, T.; Funakoshi, T.; Yamamoto, N.; Amagai, M.; et al. Nivolumab for advanced melanoma: Pretreatment prognostic factors and early outcome markers during therapy. Oncotarget 2016, 7, 77404–77415. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Grob, J.-J.; Nathan, P.; Ribas, A.; Robert, C.; Schadendorf, D.; Lane, S.R.; Mak, C.; Legenne, P.; Flaherty, K.T.; et al. Factors predictive of response, disease progression, and overall survival after dabrafenib and trametinib combination treatment: A pooled analysis of individual patient data from randomised trials. Lancet Oncol. 2016, 17, 1743–1754. [Google Scholar] [CrossRef]
- Joseph, R.; Elassaiss-Schaap, J.; Kefford, R.; Hwu, W.-J.; Wolchok, J.D.; Joshua, A.; Ribas, A.; Hodi, F.S.; Hamid, O.; Robert, C.; et al. Baseline Tumor Size Is an Independent Prognostic Factor for Overall Survival in Patients with Melanoma Treated with Pembrolizumab. Clin. Cancer Res. 2018, 24, 4960–4967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poklepovic, A.S.; Carvajal, R.D. Prognostic Value of Low Tumor Burden in Patients With Melanoma. Oncology 2018, 32, e90–e96. [Google Scholar]
- Deschner, B.; Wayne, J.D. Follow-up of the melanoma patient. J. Surg. Oncol. 2019, 119, 262–268. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Cancer (UK). Melanoma: Assessment and Management; National Institute for Health and Care Excellence (NICE): London, UK, 2015. [Google Scholar]
- Cancer Council Australia. Clinical Practice Guidelines for the Diagnosis and Management of Melanoma; Cancer Council Australia: Sydney, Australia, 2018. [Google Scholar]
- National Cancer Council Network. Clinical Practice Guidelines in Oncology. Melanoma; National Comprehensive Cancer Network: Philadelphia, PA, USA, 2014. [Google Scholar]
- Marciano, N.J.; Merlin, T.L.; Bessen, T.; Street, J.M. To what extent are current guidelines for cutaneous melanoma follow up based on scientific evidence? Int. J. Clin. Pract. 2014, 68, 761–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pflugfelder, A.; Kochs, C.; Blum, A.; Capellaro, M.; Czeschik, C.; Dettenborn, T.; Dill, D.; Dippel, E.; Eigentler, T.; Feyer, P.; et al. Malignant Melanoma S3-Guideline “Diagnosis, Therapy and Follow-up of Melanoma”. J. Dtsch. Dermatol. Ges. 2013, 11, 1–116. [Google Scholar] [CrossRef]
- Coit, D.G.; Thompson, J.A.; Algazi, A.; Andtbacka, R.; Bichakjian, C.K.; Carson, I.W.E.; Daniels, G.A.; DiMaio, D.; Ernstoff, M.; Fields, R.C.; et al. Melanoma, Version 2. 2016, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2016, 14, 450–473. [Google Scholar]
- Bastiaannet, E.; Groot, C.A.U.-D.; Brouwers, A.H.; van der Jagt, E.J.; Hoekstra, O.S.; Oyen, W.; Verzijlbergen, F.; van Ooijen, B.; Thompson, J.F.; Hoekstra, H.J. Cost-effectiveness of Adding FDG-PET or CT to the Diagnostic Work-up of Patients with Stage III Melanoma. Ann. Surg. 2012, 255, 771–776. [Google Scholar] [CrossRef]
- Krug, B.; Crott, R.; Roch, I.; Lonneux, M.; Beguin, C.; Baurain, J.-F.; Pirson, A.-S.; Borght, T.V. Cost-effectiveness analysis of FDG PET-CT in the management of pulmonary metastases from malignant melanoma. Acta Oncol. 2010, 49, 192–200. [Google Scholar] [CrossRef]
- Hong, N.J.L.; Petrella, T.; Chan, K. Cost-effectiveness analysis of staging strategies in patients with regionally metastatic melanoma. J. Surg. Oncol. 2015, 111, 423–430. [Google Scholar] [CrossRef] [PubMed]
- James, L.; Brown, M.P.; Arance, A.M.; Axel, H.; Paola, Q.; Del Vecchio, M.; Ascierto, P.A.; Ivana, K.; Jacob, S.; Bart, N.; et al. An open-label, multicentre safety study of vemurafenib in patients with BRAF(V600)-mutant metastatic melanoma: Final analysis and a validated prognostic scoring system. Eur. J. Cancer 2019, 107, 175–185. [Google Scholar]
- Wolchok, J.D.; Hoos, A.; O’Day, S.; Weber, J.S.; Hamid, O.; Lebbé, C.; Maio, M.; Binder, M.; Bohnsack, O.; Nichol, G.; et al. Guidelines for the evaluation of immune therapy activity in solid tumors: Immune-related response criteria. Clin. Cancer Res. 2009, 15, 7412–7420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larkin, J.; Minor, D.; D’Angelo, S.; Neyns, B.; Smylie, M.; Miller, W.H., Jr.; Gutzmer, R.; Linette, G.; Chmielowski, B.; Lao, C.D.; et al. Overall Survival in Patients With Advanced Melanoma Who Received Nivolumab Versus Investigator’s Choice Chemotherapy in CheckMate 037: A Randomized, Controlled, Open-Label Phase III Trial. J. Clin. Oncol. 2018, 36, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Severens, J.L.; Mandrik, O. Disutility associated with cancer screening programs: A systematic review. PLoS ONE 2019, 14, e0220148. [Google Scholar] [CrossRef]
- Lin, E.C. Radiation Risk From Medical Imaging. Mayo Clin. Proc. 2010, 85, 1142–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijhuis, A.A.G.; Dieng, M.; Mecon, N.K.; Lord, S.J.; Dalton, J.; Menzies, A.M.; Turner, R.M.; Allen, J.; Saw, R.P.M.; Nieweg, O.E.; et al. False-Positive Results and Incidental Findings with Annual CT or PET/CT Surveillance in Asymptomatic Patients with Resected Stage III Melanoma. Ann. Surg. Oncol. 2019, 26, 1860–1868. [Google Scholar] [CrossRef]
- Ding, A.; Eisenberg, J.D.; Pandharipande, P.V. The Economic Burden of Incidentally Detected Findings. Radiol. Clin. N. Am. 2011, 49, 257–265. [Google Scholar] [CrossRef] [Green Version]
- Jones, W.O.; Harman, C.R.; Ng, A.K.; Shaw, J.H. Incidence of Malignant Melanoma in Auckland, New Zealand: Highest Rates in the World. World J. Surg. 1999, 23, 732–735. [Google Scholar] [CrossRef]
- Naeser, Y.; Helgadottir, H.; Brandberg, Y.; Hansson, J.; Bagge, R.O.; Elander, N.O.; Ingvar, C.; Isaksson, K.; Flygare, P.; Nilsson, C.; et al. TRIM study protocol-a prospective randomized multicenter Trial to assess the Role of Imaging during follow-up after radical surgery of stage IIB-C and III cutaneous malignant Melanoma. BMC Cancer 2020, 20, 1–10. [Google Scholar] [CrossRef]
- Kuntz, K.M. Can mathematical modeling remove the tarnish on old clinical trials? Am. J. Med. 2001, 111, 155–156. [Google Scholar] [CrossRef]
- Gershenwald, J.E.; Scolyer, R.A. Melanoma Staging: American Joint Committee on Cancer (AJCC) 8th Edition and Beyond. Ann. Surg. Oncol. 2018, 25, 2105–2110. [Google Scholar] [CrossRef]
- Dieng, M.; Khanna, N.; Nguyen, M.T.H.; Turner, R.; Lord, S.J.; Menzies, A.M.; Allen, J.; Saw, R.; Nieweg, E.O.; Thompson, J.; et al. Cost-effectiveness analysis of PET/CT surveillance imaging to detect systemic recurrence in resected stage III melanoma: Study protocol. BMJ Open 2020, 10, e037857. [Google Scholar] [CrossRef]
- Culyer, T. The Dictionary of Health Economics, 3rd ed; Edward Elgar Publishing: Cheltenham, UK, 2014. [Google Scholar]
- Pharmaceutical Benefits Advisory Committee (PBAC). Guidelines for Preparing a Submission to the Pharmaceutical Benefits Advisory Committee (PBAC Guidelines), Version 5.0; Pharmaceutical Benefits Advisory Committee: Canberra, Australia, 2016. [Google Scholar]
- Elliott, T.M.; Whiteman, D.C.; Olsen, C.; Gordon, L.G. Estimated Healthcare Costs of Melanoma in Australia Over 3 Years Post-Diagnosis. Appl. Health. Econ. Health. Policy 2017, 15, 805–816. [Google Scholar] [CrossRef]
- Australian Government. Pricing Framework for Australian Public Hospital Services 2019-20, in Authority IHP, 30th ed.; Australian Government: Canberra, Australia, 2018. [Google Scholar]
- Australian Bureau of Statistics (ABS). Consumer Price Index of Australia; ABS: Canberra, Australia, 2021. [Google Scholar]
- Turner, R.M.; Dieng, M.; Khanna, N.; Nguyen, M.; Zeng, J.; Nijhuis, A.A.G.; Nieweg, O.E.; Einstein, A.J.; Emmett, L.; Lord, S.J.; et al. Performance of Long-Term CT and PET/CT Surveillance for Detection of Distant Recurrence in Patients with Resected Stage IIIA–D Melanoma. Ann. Surg. Oncol. 2021, 28, 4561–4569. [Google Scholar] [CrossRef]
- Machet, L.; Nemeth-Normand, F.; Giraudeau, B.; Perrinaud, A.; Tiguemounine, J.; Ayoub, J.; Alison, D.; Vaillant, L.; Lorette, G. Is ultrasound lymph node examination superior to clinical examination in melanoma follow-up? A monocentre cohort study of 373 patients. Br. J. Dermatol. 2005, 152, 66–70. [Google Scholar]
- Briggs, A.H.; Weinstein, M.C.; Fenwick, E.A.; Karnon, J.; Sculpher, M.J.; Paltiel, A.D. Model Parameter Estimation and Uncertainty: A Report of the ISPOR-SMDM Modeling Good Research Practices Task Force-6. Value Health. 2012, 15, 835–842. [Google Scholar] [CrossRef] [Green Version]
- Briggs, A.H.; Mooney, C.Z.; Wonderling, D. Constructing confidence intervals for cost-effectiveness ratios: An evaluation of parametric and non-parametric techniques using Monte Carlo simulation. Stat. Med. 1999, 18, 3245–3262. [Google Scholar] [CrossRef]
- Husereau, D.; Drummond, M.; Petrou, S.; Carswell, C.; Moher, D.; Greenberg, D.; Augustovski, F.; Briggs, A.H.; Mauskopf, J.; Loder, E.; et al. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)—Explanation and Elaboration: A Report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health 2013, 16, 231–250. [Google Scholar] [CrossRef] [Green Version]
- Leiter, U.; Marghoob, A.A.; Lasithiotakis, K.; Eigentler, T.K.; Meier, F.; Meisner, C.; Garbe, C. Costs of the detection of metastases and follow-up examinations in cutaneous melanoma. Melanoma Res. 2009, 19, 50–57. [Google Scholar] [CrossRef]
- Hengge, U.R.; Wallerand, A.; Stutzki, A.; Kockel, N. Cost-effectiveness of reduced follow-up in malignant melanoma. JDDG: J. Dtsch. Dermatol. Ges. 2007, 5, 898–907. [Google Scholar] [CrossRef] [PubMed]
- Podlipnik, S.; Moreno-Ramírez, D.; Carrera, C.; Barreiro, A.; Manubens, E.; Ferrandiz-Pulido, L.; Sánchez, M.; Vidal-Sicart, S.; Malvehy, J.; Puig, S. Cost-effectiveness analysis of imaging strategy for an intensive follow-up of patients with American Joint Committee on Cancer stage IIB, IIC and III malignant melanoma. Br. J. Dermatol. 2019, 180, 1190–1197. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Nivolumab plus ipilimumab or nivolumab alone versus ipilimumab alone in advanced melanoma (CheckMate 067): 4-year outcomes of a multicentre, randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1480–1492. [Google Scholar] [CrossRef]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.; Weber, J.S.; et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE-001. Ann. Oncol. 2019, 30, 582–588. [Google Scholar] [CrossRef] [PubMed]
- Sloane, F.A. Valuing Health Care: Costs, Benefits, and Effectiveness of Pharmaceuticals and Other Medical Technologies; Cambridge University Press: New York, NY, USA, 1995. [Google Scholar]
- Wall, B.F.; Haylock, R.; Jansen, J.T.M.; Hillier, M.C.; Hart, D.; Shrimpton, P.C. Radiation Risks from Medical X-ray Examinations As a Function of Age and Sex of the Patient; Health Protection Agency: London, UK, 2011. [Google Scholar]
- Thompson, C.A.; Charlson, M.E.; Schenkein, E.; Wells, M.T.; Furman, R.R.; Elstrom, R.; Ruan, J.; Martin, P.; Leonard, J.P. Surveillance CT scans are a source of anxiety and fear of recurrence in long-term lymphoma survivors. Ann. Oncol. 2010, 21, 2262–2266. [Google Scholar] [CrossRef]
- Grol, R.; Grimshaw, J. From best evidence to best practice: Effective implementation of change in patients’ care. Lancet 2003, 362, 1225–1230. [Google Scholar] [CrossRef]
- Ubel, P.A.; Jepson, C.; Baron, J.; Hershey, J.C.; Asch, D.A. The influence of cost-effectiveness information on physicians’ cancer screening recommendations. Soc. Sci. Med. 2003, 56, 1727–1736. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Imaging Schedule | ||||
|---|---|---|---|---|---|
| 3–4 Monthly | 6-Monthly | 12-Monthly | No-Imaging | Total | |
| Total: N (%) | 146 (18%) | 47 (6%) | 284 (35%) | 346 (42%) | 823 (100%) |
| Gender: N (%) | |||||
| Male | 91 (11%) | 33 (4%) | 181 (22%) | 230 (28%) | 535 (65%) |
| Age at Diagnosis: Mean (SD) | 59 (14.19) | 54 (13.68) | 52 (14.70) | 61 (16.71) | 57 (15.94) |
| Age at Diagnosis: Median (IQR) | 60 (49–69) | 55 (44–64) | 53 (42–62) | 62 (50–74) | 58 (46–69) |
| Site of Primary: N (%) | |||||
| Head and Neck | 22 (15%) | 9 (19%) | 43 (15%) | 69 (20%) | 143 (17%) |
| Trunk | 38 (26%) | 12 (26%) | 102 (36%) | 91 (26%) | 243 (30%) |
| Upper Limbs | 13 (9%) | 4 (9%) | 33 (12%) | 30 (9%) | 80 (10%) |
| Lower Limbs | 28 (19%) | 12 (25%) | 72 (25%) | 60 (17%) | 172 (21%) |
| Occult | 45 (31%) | 10 (21%) | 34 (12%) | 95 (27%) | 184 (22%) |
| Other | 1 (0.3%) | 1 (0.1%) | |||
| AJCC Stage: N (%) | |||||
| III | 45 (31%) | 10 (21%) | 35 (12%) | 101 (29%) | 191 (23%) |
| IIIA | 26 (18%) | 12 (26%) | 117 (41%) | 42 (12%) | 197 (24%) |
| IIIB | 39 (27%) | 12 (26%) | 91 (32%) | 74 (21%) | 216 (26%) |
| IIIC | 36 (25%) | 13 (28%) | 41 (14%) | 129 (37%) | 219 (27%) |
| Resource Use | |||||
| Diagnostic Imaging (surveillance) | |||||
| Count | 902 | 172 | 1214 | 2116 | |
| Mean (SD) | 6.3 (3.7) | 3.7 (2.3) | 4.3 (2.4) | ||
| Range | [2–19] | [1–11] | [1–13] | ||
| Extra investigations * | |||||
| Count | 690 | 222 | 960 | 1872 | |
| Mean (SD) | 4.8 (5.5) | 4.7 (4.6) | 3.4 (3.2) | ||
| Range | [0–28] | [0–22] | [0–16] | ||
| Strategy | Mean Cost Per Patient (AUD) | Incremental Cost (AUD) | Effectiveness * | Incremental Proportion of Distant Disease Appropriately Diagnosed and Treated * | ICER ** (AUD/Outcome) |
|---|---|---|---|---|---|
| No imaging | 51,149 | 0.8770 | - | - | |
| 12-monthly | 52,160 | 2748 | 0.9181 | 0.0411 | 34,362 |
| 6-monthly | 77,998 | 28,476 | 0.8824 | 0.0054 | Dominated |
| 3 to 4-monthly | 88,387 | 36,860 | 0.8845 | 0.0075 | Dominated *** |
| Strategy | Mean Total Cost Per Patient (AUD) | Incremental Cost (AUD) | Effectiveness (Diagnostic Error Avoided) | Incremental Effectiveness * |
|---|---|---|---|---|
| No imaging follow-up | 1513 | 0.8832 | ||
| 12-monthly imaging | 9084 | 7571 | 0.8503 | −0.0329 |
| 6-monthly imaging | 16,268 | 14,755 | 0.8386 | −0.0446 |
| 3 to 4-monthly imaging | 25,304 | 23,791 | 0.7999 | −0.0833 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dieng, M.; Turner, R.M.; Lord, S.J.; Einstein, A.J.; Menzies, A.M.; Saw, R.P.M.; Nieweg, O.E.; Thompson, J.F.; Morton, R.L. Cost-Effectiveness of PET/CT Surveillance Schedules to Detect Distant Recurrence of Resected Stage III Melanoma. Int. J. Environ. Res. Public Health 2022, 19, 2331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042331
Dieng M, Turner RM, Lord SJ, Einstein AJ, Menzies AM, Saw RPM, Nieweg OE, Thompson JF, Morton RL. Cost-Effectiveness of PET/CT Surveillance Schedules to Detect Distant Recurrence of Resected Stage III Melanoma. International Journal of Environmental Research and Public Health. 2022; 19(4):2331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042331
Chicago/Turabian StyleDieng, Mbathio, Robin M. Turner, Sarah J. Lord, Andrew J. Einstein, Alexander M. Menzies, Robyn P. M. Saw, Omgo E. Nieweg, John F. Thompson, and Rachael L. Morton. 2022. "Cost-Effectiveness of PET/CT Surveillance Schedules to Detect Distant Recurrence of Resected Stage III Melanoma" International Journal of Environmental Research and Public Health 19, no. 4: 2331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042331