
Perceived COVID-19 Threat and Reactions to Noncompliant Health-Protective Behaviors: The Mediating Role of Desired Cultural Tightness and the Moderating Role of Age


Abstract
:1. Introduction
2. Threat, Tightness, and Implications
3. The Present Research
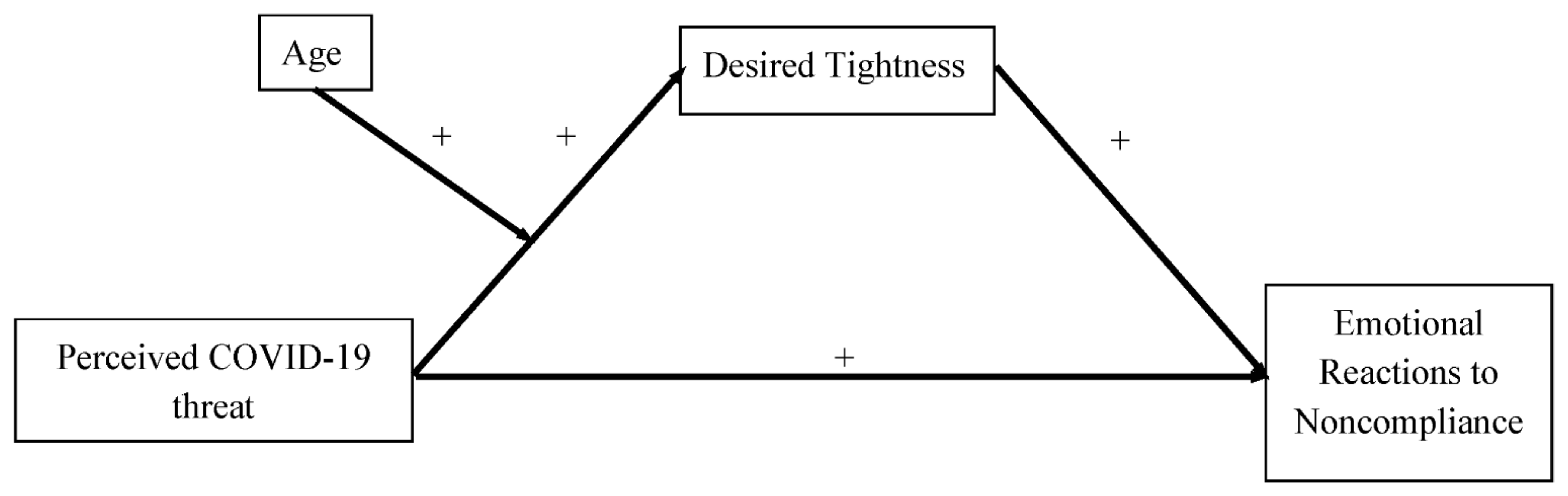
- H1
- The perceived COVID-19 threat should intensify desired tightness;
- H2
- The above relationship should be moderated by age;
- H3
- The desired tightness should intensify emotional negative reactions to the others’ non-compliance with health-protective behaviors.
4. Materials and Methods
4.1. Ethics
4.2. Participants and Procedures
4.3. Measures
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19). Available online: https://www.who.int/health-topics/coronavirus (accessed on 19 December 2021).
- Kandel, N.; Chungong, S.; Omaar, A.; Xing, J. Health security capacities in the context of COVID-19 outbreak: An analysis of International Health Regulations annual report data from 182 countries. Lancet 2020, 395, 1047–1053. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 19 December 2021).
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-10 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallagher, M.W.; Zvolensky, M.J.; Long, L.J.; Rogers, A.H.; Garey, L. The impact of COVID-19 experiences and associated stress on anxiety, depression, and functional impairment in American adults. Cognit. Ther. Res. 2020, 44, 1043–1051. [Google Scholar] [CrossRef] [PubMed]
- Syropoulos, S.; Markowitz, E.M. Prosocial responses to COVID-19: Examining the role of gratitude, fairness and legacy motives. Pers. Individ. Differ. 2020, 171, 110488. [Google Scholar] [CrossRef]
- Jackson, J.C.; Van Egmond, M.; Choi, V.K.; Ember, C.R.; Halberstadt, J.; Balanovic, J.; Basker, I.N.; Boehnke, K.; Buki, N.; Fischer, R.; et al. Ecological and cultural factors underlying the global distribution of prejudice. PLoS ONE 2019, 14, e0221953. [Google Scholar] [CrossRef]
- Gelfand, M.J.; Raver, J.L.; Nishii, L.; Leslie, L.M.; Lun, J.; Lim, B.C.; Duan, L.; Almaliach, A.; Ang, S.; Arnadottir, J.; et al. Differences between tight and loose cultures: A 33-nation study. Science 2011, 332, 1100–1104. [Google Scholar] [CrossRef] [Green Version]
- Harrington, J.R.; Gelfand, M.J. Tightness-looseness across the 50 united states. Proc. Natl. Acad. Sci. USA 2014, 111, 7990–7995. [Google Scholar] [CrossRef] [Green Version]
- Gelfand, M.J. Rule Makers, Rule Breakers: Tight and Loose Cultures and the Secret Signals That Direct Our Lives; Scribner Book Company: New York, NY, USA, 2018. [Google Scholar]
- Mula, S.; Di Santo, D.; Gelfand, M.J.; Cabras, C.; Pierro, A. The Mediational Role of Desire for Cultural Tightness on Concern with COVID-19 and Perceived Self-Control. Front. Psychol. 2021, 12, 713952. [Google Scholar] [CrossRef]
- Mula, S.; Di Santo, D.; Resta, E.; Bakhtiari, F.; Baldner, C.; Molinario, E.; Pierro, A.; Gelfand, M.J.; Denison, E.; Agostini, M.; et al. Concern with COVID-19 pandemic threat and attitudes towards immigrants: The mediating effect of the desire for tightness. Curr. Res. Ecol. Soc. Psychol. 2022, 3, 100028. [Google Scholar] [CrossRef]
- Pepitone, A. The normative basis of aggression: Anger and punitiveness. Rech. De Psychol. Soc. 1981, 3, 3–17. [Google Scholar]
- Clark, C.; Davila, A.; Regis, M.; Kraus, S. Predictors of COVID-19 voluntary compliance behaviors: An international investigation. Glob. Transit. 2020, 2, 76–82. [Google Scholar] [CrossRef]
- Van Rooij, B.; de Bruijn, A.L.; Reinders Folmer, C.; Kooistra, E.B.; Kuiper, M.E.; Brownlee, M.; Olthuis, E.; Fine, A. Compliance with COVID-19 mitigation measures in the United States. Amst. Law Sch. Res. Pap. 2020, 1–40. [Google Scholar] [CrossRef]
- Norman, P.; Wilding, S.; Conner, M. Reasoned action approach and compliance with recommended behaviours to prevent the transmission of the SARS-CoV-2 virus in the UK. Br. J. Health Psychol. 2020, 25, 1006–1019. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.; Kroska, E.B. Face Covered and Six Feet Apart: Behavioral Awareness Predicts Greater Adherence to Public Health Guidelines during the COVID-19 Pandemic. Int. J. Environ. Res. 2021, 18, 8247. [Google Scholar] [CrossRef]
- Williams, S.N.; Armitage, C.J.; Tampe, T.; Dienes, K.A. Public perceptions of non-adherence to pandemic protection measures by self and others: A study of COVID-19 in the United Kingdom. PLoS ONE 2021, 16, e0258781. [Google Scholar] [CrossRef]
- Schunk, D.; Wagner, V. What Determines the Willingness to Sanction Violations of Newly Introduced Social Norms: Personality Traits or Economic Preferences? Evidence from the COVID-19 Crisis. J. Behav. Exp. Econ. 2021, 93, 101716. [Google Scholar] [CrossRef]
- Nikolich-Zugich, J.; Knox, K.S.; Rios, C.T.; Natt, B.; Bhattacharya, D.; Fain, M.J. SARS-CoV-2 and COVID-19 in older adults: What we may expect regarding pathogenesis, immune responses, and outcomes. GeroScience 2020, 42, 505–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Pearman, A.; Hughes, M.L.; Smith, E.L.; Neupert, S.D. Age differences in risk and resilience factors in COVID-19–related stress. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, 38–44. [Google Scholar] [CrossRef]
- Jin, S.; Balliet, D.; Romano, A.; Spadaro, G.; Van Lissa, C.J.; Agostini, M.; Bélanger, J.J.; Gützkow, B.; Kreienkamp, J.; Abakoumkin, G.; et al. Intergenerational conflicts of interest and prosocial behavior during the COVID-19 pandemic. Personal. Individ. Differ. 2021, 171, 110535. [Google Scholar] [CrossRef]
- Bruine de Bruin, W. Age differences in COVID-19 risk perceptions and mental health: Evidence from a national US survey conducted in March 2020. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e24–e29. [Google Scholar] [CrossRef] [PubMed]
- Pelto, P. The difference between “tight” and “loose” societies. Transaction 1968, 5, 37–40. [Google Scholar] [CrossRef]
- Gelfand, M.J.; Nishii, L.H.; Raver, J.L. On the nature and importance of cultural tightness-looseness. J. Appl. Psychol. 2006, 91, 1225–1244. [Google Scholar] [CrossRef] [Green Version]
- Gelfand, M.J.; Jackson, J.C.; Pan, X.; Nau, D.; Pieper, D.; Denison, E.; Dagher, M.; Van Lange, P.A.; Chiu, C.Y.; Wang, M. The relationship between cultural tightness–looseness and COVID-19 cases and deaths: A global analysis. Lancet Planet. Health 2021, 5, e135–e144. [Google Scholar] [CrossRef]
- Nisa, C.F.; Bélanger, J.J.; Faller, D.G.; Buttrick, N.R.; Mierau, J.O.; Austin, M.M.; Schumpe, B.M.; Sasin, E.M.; Agostini, M.; Gützkow, B.; et al. Lives versus Livelihoods? Perceived economic risk has a stronger association with support for COVID-19 preventive measures than perceived health risk. Sci. Rep. 2021, 11, 9669. [Google Scholar] [CrossRef] [PubMed]
- Qin, X.; Yam, K.C.; Chen, C.; Li, W.; Dong, X. Talking about COVID-19 is positively associated with team cultural tightness: Implications for team deviance and creativity. J. Appl. Psychol. 2021, 106, 530–541. [Google Scholar] [CrossRef]
- Kemmelmeier, M.; Jami, W.A. Mask wearing as cultural behavior: An investigation across 45 US states during the COVID-19 pandemic. Front. Psychol. 2021, 12, 648692. [Google Scholar] [CrossRef]
- Petretto, D.R.; Pili, R. Ageing and COVID-19: What is the role for elderly people? Geriatrics 2020, 5, 25. [Google Scholar] [CrossRef]
- Our World In Data. Cumulative COVID-19 Tests, Confirmed Cases and Deaths per Million People, Italy. Available online: https://ourworldindata.org/grapher/covid-tests-cases-deaths-per-million?time=2020-03-07..latest&country=~ITA (accessed on 19 December 2021).
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Github.com. COVID-19/Dati-Regioni. Available online: https://github.com/pcm-dpc/COVID-19/blob/master/dati-regioni/dpc-covid19-ita-regioni-latest.csv (accessed on 19 December 2021).
- Conway, L.G., III; Woodard, S.R.; Zubrod, A. Social Psychological Measurements of COVID-19: Coronavirus Perceived Threat, Government Response, Impacts, and Experiences Questionnaires. PsyarXiv 2020. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 3rd ed.; Sage: Thousand Oaks, CA, USA, 2022. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation and Conditional Process Analysis. Available online: www.guilford.com/ebooks (accessed on 20 November 2021).
- Valenti, V.E.; Silva, A.P. The effect of negationism on public health. J. Hum. Growth Dev. 2021, 31, 189–191. [Google Scholar] [CrossRef]
- Roos, P.; Gelfand, M.J.; Nau, D.; Lun, J. Societal threat and cultural variation in the strength of social norms: An evolutionary basis. Organ. Behav. Hum. Decis. Process. 2015, 129, 14–23. [Google Scholar] [CrossRef] [Green Version]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Age Range | Number of Participants out of the Total Sample | Percentage on the Total Sample |
|---|---|---|
| 18–29 | 388 | 62.2% |
| 30–44 | 108 | 17.3% |
| 45–59 | 102 | 16.3% |
| 60+. | 26 | 4.2% |
| M | SD | Min | Max | Skewness | Kurtosis | |
|---|---|---|---|---|---|---|
| Emotional Reactions to Non-compliance | 3.44 | 0.747 | 1.00 | 5.00 | −0.525 | 0.762 |
| Do not wear protective devices against COVID-19 (e.g., mask). | 3.49 | 0.827 | 1 | 5 | −0.549 | 0.674 |
| Little or no engagement in social distancing. | 3.41 | 0.796 | 1 | 5 | −0.316 | 0.543 |
| Do not respect hygiene rules against the spread of COVID-19. | 3.29 | 0.827 | 1 | 5 | −0.255 | 0.369 |
| Do not respect the lockdown when is mandatory. | 3.49 | 0.968 | 1 | 5 | −0.485 | -0.021 |
| Ignoring the restrictions against the spread of COVID-19. | 3.57 | 0.912 | 1 | 5 | −0.582 | 0.489 |
| Perceived COVID-19 threat | 4.99 | 1.361 | 1.00 | 7.00 | −0.429 | −0.511 |
| Thinking about the coronavirus (COVID-19) makes me feel threatened. | 4.60 | 1.802 | 1 | 7 | −0.389 | −0.852 |
| I am afraid of the coronavirus (COVID-19). | 4.59 | 1.799 | 1 | 7 | −0.346 | −0.890 |
| I am not worried about the coronavirus (COVID-19). (R) | 4.78 | 1.875 | 1 | 7 | −0.406 | −0.981 |
| I am worried that I or people I love will become sick from the coronavirus (COVID-19). | 5.56 | 1.468 | 1 | 7 | −0.863 | −0.042 |
| How concerned are you about the current coronavirus threat? | 5.45 | 1.535 | 1 | 7 | −0.964 | 0.423 |
| Desired Tightness | 6.28 | 1.585 | 1.00 | 9.00 | −0.494 | 0.128 |
| To what extent do you think that your place (municipality) of residence should have the following characteristics right now? | ||||||
| 1 = Have flexible social norms; 9 = Have rigid social norms. | 6.07 | 2.038 | 1 | 9 | −0.515 | −0.232 |
| 1 = Treat people who do not conform to norms kindly; 9 = Treat people who do not conform to norms harshly. | 6.29 | 2.045 | 1 | 9 | −0.693 | −0.050 |
| 1 = Have fewer rules; 9 = Have more rules. | 6.21 | 1.801 | 1 | 9 | −0.349 | −0.144 |
| 1 = To be permissive; 9 = To be restrictive. | 5.96 | 1.789 | 1 | 9 | −0.239 | −0.143 |
| 1 = Be tolerant of those who violate the norms; 9 = Be intransigent with those who violate the norms. | 6.89 | 1.797 | 1 | 9 | −0.895 | 0.508 |
| 1 | 2 | 3 | 4 | |
|---|---|---|---|---|
| 1. Age | - | |||
| 2. Perceived COVID-19 threat | 0.01 | (0.86) | ||
| 3. Desired Tightness | 0.12 ** | 0.24 ** | (0.89) | |
| 4. Emotional Reactions to Non-compliance | 0.08 * | 0.35 ** | 0.20 ** | (0.91) |
| Desired Tightness | Emotional Reactions to Non-Compliance | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| b | se | p | 95%CI | b | se | p | 95%CI | |||
| LL | UL | LL | UL | |||||||
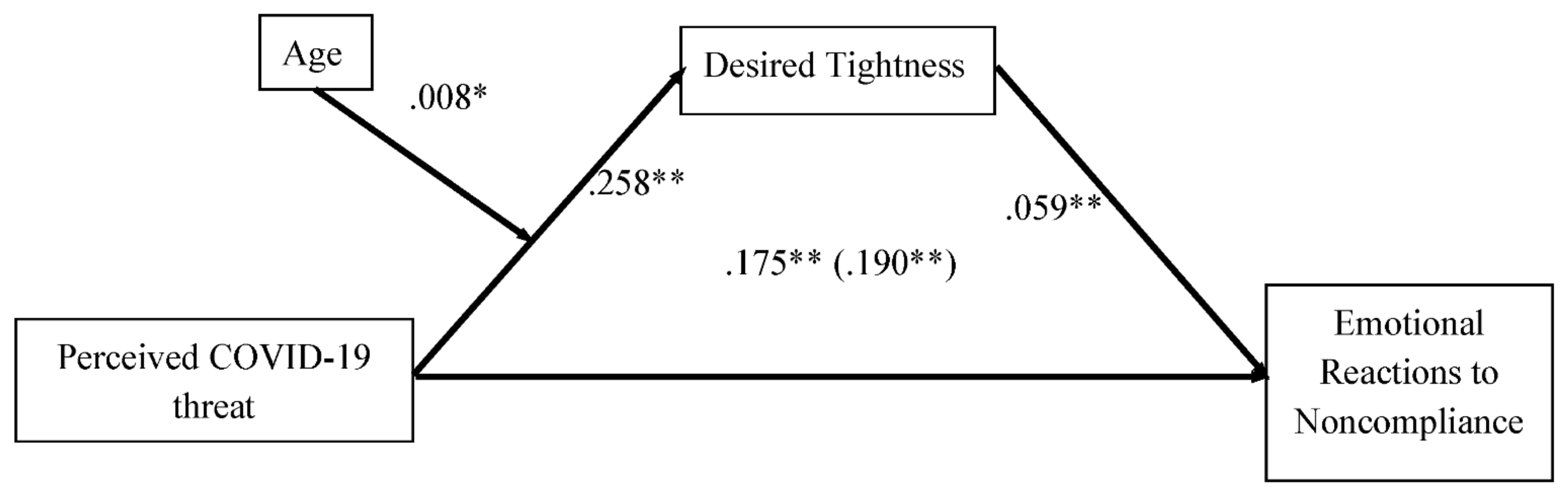
| Age | 0.014 | 0.004 | 0.002 | 0.005 | 0.023 | - | - | - | - | - |
| Gender | 0.301 | 0.138 | 0.029 | 0.029 | 0.573 | 0.025 | 0.063 | 0.691 | −0.099 | 0.149 |
| Education Level | −0.057 | 0.069 | 0.407 | −0.194 | 0.079 | 0.007 | 0.031 | 0.813 | −0.054 | 0.069 |
| Perceived COVID-19 Perceived threat | 0.258 | 0.047 | <0.001 | 0.165 | 0.350 | 0.175 | 0.022 | <0.001 | 0.132 | 0.218 |
| Perceived Threat x Age | 0.008 | 0.003 | 0.022 | 0.001 | 0.015 | - | - | - | - | - |
| Desired Tightness | - | - | - | - | - | 0.059 | 0.018 | 0.001 | 0.023 | 0.094 |
| F (5, 618) = 12.10, p < 0.001, R2 = 0.089 | F (4, 619) = 25.23, p < 0.001, R2 = 0.1402 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baldner, C.; Di Santo, D.; Viola, M.; Pierro, A. Perceived COVID-19 Threat and Reactions to Noncompliant Health-Protective Behaviors: The Mediating Role of Desired Cultural Tightness and the Moderating Role of Age. Int. J. Environ. Res. Public Health 2022, 19, 2364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042364
Baldner C, Di Santo D, Viola M, Pierro A. Perceived COVID-19 Threat and Reactions to Noncompliant Health-Protective Behaviors: The Mediating Role of Desired Cultural Tightness and the Moderating Role of Age. International Journal of Environmental Research and Public Health. 2022; 19(4):2364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042364
Chicago/Turabian StyleBaldner, Conrad, Daniela Di Santo, Marta Viola, and Antonio Pierro. 2022. "Perceived COVID-19 Threat and Reactions to Noncompliant Health-Protective Behaviors: The Mediating Role of Desired Cultural Tightness and the Moderating Role of Age" International Journal of Environmental Research and Public Health 19, no. 4: 2364. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042364