
Rehabilitation of Difficult-to-Wean, Tracheostomized Patients Admitted to Specialized Unit: Retrospective Analyses over 10-Years

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Methods
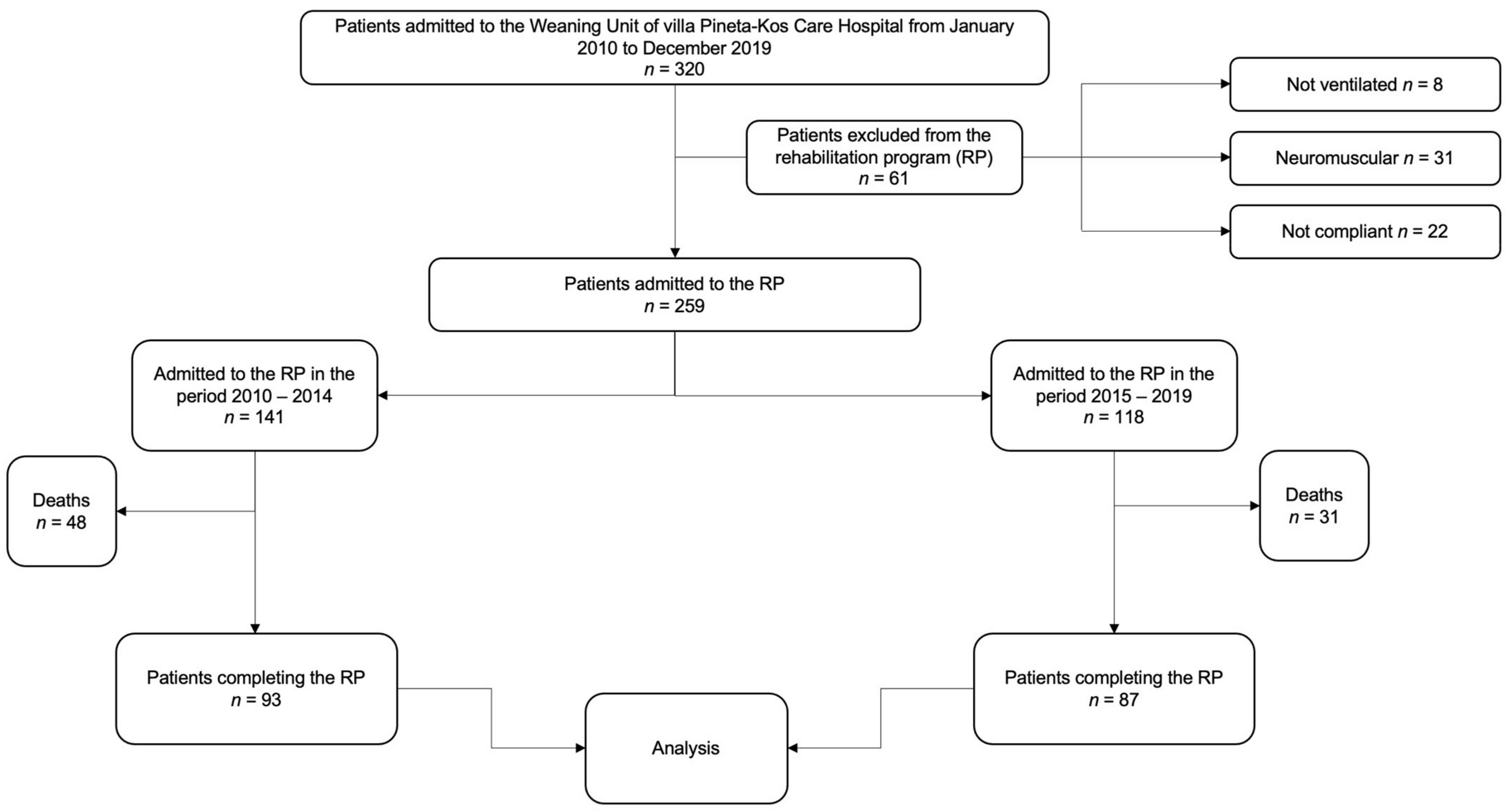
2.1. Study Design and Data Sources
2.2. Comprehensive Rehabilitation Program
2.3. Decannulation Protocol
- Patient was alert, oriented, and responsive to commands;
- Patient was able to manage oral secretions without risk of aspiration;
- Patient was no longer dependent on a ventilator for assisted breathing;
- The need for tracheal suctioning was less than once per day;
- Patient had the tracheostomy tube downsized to a size 4 Shiley or similar tracheostomy tube, and no breathing difficulty in the presence of this tube was reported;
- Successful 12 h occlusion test of the downsized tracheostomy tube was performed.
2.4. Data Collection and Outcome Assessment
2.5. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Clinical Outcomes
3.3. Prediction of Rehabilitation Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fan, E.; Cheek, F.; Chlan, L.; Gosselink, R.; Hart, N.; Herridge, M.S.; Hopkins, R.O.; Hough, C.L.; Kress, J.P.; Latronico, N.; et al. An official American Thoracic Society Clinical Practice guideline: The diagnosis of intensive care unit-acquired weakness in adults. Am. J. Respir. Crit. Care Med. 2014, 190, 1437–1446. [Google Scholar] [CrossRef]
- Patthum, A.; Peters, M.; Lockwood, C. Effectiveness and safety of Neurally Adjusted Ventilatory Assist (NAVA) mechanical ventilation compared to standard conventional mechanical ventilation in optimizing patient-ventilator synchrony in critically ill patients: A systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2015, 13, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, A.F.; Ceriana, P.; Ambrosino, N.; Malovini, A.; Nava, S. Physiotherapy and Weaning from Prolonged Mechanical Ventilation. Respir. Care 2019, 64, 17–25. [Google Scholar] [CrossRef]
- Fisser, C.; Spoletini, G.; Soe, A.K.; Livesey, A.; Schreiber, A.; Swingwood, E.; Bos, L.D.; Dreher, M.; Schultz, M.J.; Heunks, L.; et al. European Respiratory Society International Congress 2018: Highlights from Assembly 2 on respiratory intensive care. ERJ Open Res. 2019, 5, 00198–2018. [Google Scholar] [CrossRef] [Green Version]
- Daniel Martin, A.; Smith, B.K.; Gabrielli, A. Mechanical ventilation, diaphragm weakness and weaning: A rehabilitation perspective. Respir. Physiol. Neurobiol. 2013, 189, 377–383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bornitz, F.; Ewert, R.; Knaak, C.; Magnet, F.S.; Windisch, W.; Herth, F. Weaning from Invasive Ventilation in Specialist Centers Following Primary Weaning Failure. Dtsch. Arztebl. Int. 2020, 117, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Rose, L.; Adhikari, N.K.; Leasa, D.; Fergusson, D.A.; McKim, D. Cough augmentation techniques for extubation or weaning critically ill patients from mechanical ventilation. Cochrane Database Syst. Rev. 2017, 1, CD011833. [Google Scholar] [CrossRef]
- MacIntyre, N.R. Early Mobilization of Patients on Mechanical Ventilation: Worth the Effort and Expense? Respir. Care 2019, 64, 112–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuke, R.; Hifumi, T.; Kondo, Y.; Hatakeyama, J.; Takei, T.; Yamakawa, K.; Inoue, S.; Nishida, O. Early rehabilitation to prevent postintensive care syndrome in patients with critical illness: A systematic review and meta-analysis. BMJ Open 2018, 8, e019998. [Google Scholar] [CrossRef] [Green Version]
- Schönhofer, B.; Euteneuer, S.; Nava, S.; Suchi, S.; Köhler, D. Survival of mechanically ventilated patients admitted to a specialised weaning centre. Intensive Care Med. 2002, 28, 908–916. [Google Scholar] [CrossRef]
- Pilcher, D.V.; Bailey, M.J.; Treacher, D.F.; Hamid, S.; Williams, A.J.; Davidson, A.C. Outcomes, cost and long term survival of patients referred to a regional weaning centre. Thorax 2005, 60, 187–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vitacca, M.; Paneroni, M.; Peroni, R.; Barbano, L.; Dodaj, V.; Piaggi, G.; Vanoglio, F.; Luisa, A.; Giordano, A.; Ceriana, P. Effects of a multidisciplinary care program on disability, autonomy, and nursing needs in subjects recovering from acute respiratory failure in a chronic ventilator facility. Respir. Care 2014, 59, 1863–1871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chiang, L.L.; Wang, L.Y.; Wu, C.P.; Wu, H.D.; Wu, Y.T. Effects of physical training on functional status in patients with prolonged mechanical ventilation. Phys. Ther. 2006, 86, 1271–1281. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Su, C.L.; Wu, Y.T.; Wang, L.Y.; Wu, C.P.; Wu, H.D.; Chiang, L.L. Physical training is beneficial to functional status and survival in patients with prolonged mechanical ventilation. J. Formos. Med. Assoc. 2011, 110, 572–579. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.H.; Lin, H.L.; Hsiao, H.F.; Chou, L.T.; Kao, K.C.; Huang, C.C.; Tsai, Y.H. Effects of exercise training on pulmonary mechanics and functional status in patients with prolonged mechanical ventilation. Respir. Care 2012, 57, 727–734. [Google Scholar] [CrossRef] [Green Version]
- Polverino, E.; Nava, S.; Ferrer, M.; Ceriana, P.; Clini, E.; Spada, E.; Zanotti, E.; Trianni, L.; Barbano, L.; Fracchia, C.; et al. Patients’ characterization, hospital course and clinical outcomes in five Italian respiratory intensive care units. Intensive Care Med. 2010, 36, 137–142. [Google Scholar] [CrossRef]
- Carlucci, A.; Delmastro, M.; Rubini, F.; Fracchia, C.; Nava, S. Changes in the practice of non-invasive ventilation in treating COPD patients over 8 years. Intensive Care Med. 2003, 29, 419–425. [Google Scholar] [CrossRef]
- Burns, K.E.A.; Stevenson, J.; Laird, M.; Adhikari, N.K.J.; Li, Y.; Lu, C.; He, X.; Wang, W.; Liang, Z.; Chen, L.; et al. Non-invasive ventilation versus invasive weaning in critically ill adults: A systematic review and meta-analysis. Thorax 2021. [Google Scholar] [CrossRef]
- Barchfeld, T.; Schönhofer, B. Schwierige Entwöhnung vom Respirator: Beatmung und weitere Strategien. Difficult weaning. Pneumologie 2006, 60, 616–628. [Google Scholar] [CrossRef] [Green Version]
- Parrilla, F.J.; Morán, I.; Roche-Campo, F.; Mancebo, J. Ventilatory strategies in obstructive lung disease. Semin. Respir. Crit. Care Med. 2014, 35, 431–440. [Google Scholar] [CrossRef]
- Ghiani, A.; Paderewska, J.; Sainis, A.; Crispin, A.; Walcher, S.; Neurohr, C. Variables predicting weaning outcome in prolonged mechanically ventilated tracheotomized patients: A retrospective study. J. Intensive Care 2020, 8, 19. [Google Scholar] [CrossRef] [Green Version]
- Clini, E.M.; Crisafulli, E.; Antoni, F.D.; Beneventi, C.; Trianni, L.; Costi, S.; Fabbri, L.M.; Nava, S. Functional recovery following physical training in tracheotomized and chronically ventilated patients. Respir. Care 2011, 56, 306–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fässberg, M.M.; Cheung, G.; Canetto, S.S.; Erlangsen, A.; Lapierre, S.; Lindner, R.; Draper, B.; Gallo, J.J.; Wong, C.; Wu, J.; et al. A systematic review of physical illness, functional disability, and suicidal behaviour among older adults. Aging Ment. Health 2016, 20, 166–194. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.T.; Lang, J.K.; Haines, K.J.; Skinner, E.H.; Haines, T.P. Physical Rehabilitation in the ICU: A Systematic Review and Meta-Analysis. Crit. Care Med. 2022, 50, 375–388. [Google Scholar] [CrossRef]
- Boles, J.M.; Bion, J.; Connors, A.; Herridge, M.; Marsh, B.; Melot, C.; Pearl, R.; Silverman, H.; Stanchina, M.; Viellard-Baron, A.; et al. Weaning from mechanical ventilation. Eur. Respir. J. 2007, 29, 1033–1056. [Google Scholar] [CrossRef]
- Ghauri, S.K.; Javaeed, A.; Mustafa, K.J.; Khan, A.S. Predictors of prolonged mechanical ventilation in patients admitted to intensive care units: A systematic review. Int. J. Health Sci. 2019, 13, 31–38. [Google Scholar]
- Fortin, M.; Hudon, C.; Dubois, M.F.; Almirall, J.; Lapointe, L.; Soubhi, H. Comparative assessment of three different indices of multimorbidity for studies on health-related quality of life. Health Qual. Life Outcomes 2005, 3, 74. [Google Scholar] [CrossRef] [Green Version]
- Jones, J.R.A.; Berney, S.; Berry, M.J.; Files, D.C.; Griffith, D.M.; McDonald, L.A.; Morris, P.E.; Moss, M.; Nordon-Craft, A.; Walsh, T.; et al. Response to physical rehabilitation and recovery trajectories following critical illness: Individual participant data meta-analysis protocol. BMJ Open 2020, 10, e035613. [Google Scholar] [CrossRef]
- Martin, U.J.; Hincapie, L.; Nimchuk, M.; Gaughan, J.; Criner, G.J. Impact of whole-body rehabilitation in patients receiving chronic mechanical ventilation. Crit. Care Med. 2005, 33, 2259–2265. [Google Scholar] [CrossRef]
- Montagnani, G.; Vagheggini, G.; Panait Vlad, E.; Berrighi, D.; Pantani, L.; Ambrosino, N. Use of the functional independence measure in people for whom weaning from mechanical ventilation is difficult. Phys. Ther. 2011, 91, 1109–1115. [Google Scholar] [CrossRef] [Green Version]
- Carson, S.S.; Bach, P.B. Predicting mortality in patients suffering from prolonged critical illness: An assessment of four severity-of-illness measures. Chest 2001, 120, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Corner, E.J.; Wood, H.; Englebretsen, C.; Thomas, A.; Grant, R.L.; Nikoletou, D.; Soni, N. The Chelsea critical care physical assessment tool (CPAx): Validation of an innovative new tool to measure physical morbidity in the general adult critical care population; an observational proof-of-concept pilot study. Physiotherapy 2013, 99, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Winck, J.C.; Gilet, H.; Kalin, P.; Murcia, J.; Plano, F.; Regnault, A.; Dreher, M.; Vitacca, M.; Ambrosino, N. Validation of the Multi-INdependence Dimensions (MIND) questionnaire for prolonged mechanically ventilated subjects. BMC Pulm. Med. 2019, 19, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucena, J.F.; Alegre, F.; Martinez-Urbistondo, D.; Landecho, M.F.; Huerta, A.; García-Mouriz, A.; García, N.; Quiroga, J. Performance of SAPS II and SAPS 3 in intermediate care. PLoS ONE 2013, 8, e77229. [Google Scholar] [CrossRef]


{kind=link}
| Total | 2010–2014 | 2015–2019 | p-Value | |
|---|---|---|---|---|
| Admitted to rehabilitation, n (%) | 259 (100) | 141 (54) | 118 (46) | |
| Death, n (%) | 79 (31) | 48 (34) | 31 (26) | 0.18 |
| Included in analysis, n (%) | 180 (69) | 93 (66) | 87 (74) | 0.22 |
| Part 1. Baseline variables * | ||||
| Age, years (SD) | 73 (10.1) | 73.1 (9.9) | 72.9 (10.2) | 0.88 |
| Male sex (%) | 102 (56.7) | 45 (48.4) | 57 (65.5) | 0.02 |
| Baseline CIRS, score (SD) | 19 (3.9) | 18.2 (4.2) | 20.0 (3.4) | 0.002 |
| Baseline SAPS II, score (SD) | 21.5 (14.1) | 19.7 (11.4) | 23.4 (16.4) | 0.08 |
| Time in an acute care hospital, days (SD) | 36.4 (26.7) | 36.6 (25.0) | 36.1 (28.6) | 0.9 |
| Time from tracheostomy, days (SD) | 22.1 (22.3) | 22.4 (20.8) | 21.7 (23.9) | 0.84 |
| Diagnosis of admission: | ||||
| COPD, n (%) | 75 (42) | 41 (44) | 34 (39) | 0.54 |
| Heart surgery, n (%) | 32 (18) | 20 (22) | 12 (14) | 0.24 |
| Abdominal surgery, n (%) | 22 (12) | 16 (17) | 6 (7) | 0.04 |
| Polytrauma, n (%) | 20 (11) | 7 (8) | 13 (15) | 0.15 |
| Metabolic syndrome, n (%) | 9 (5) | 2 (2) | 7 (8) | 0.09 |
| Thoracic surgery, n (%) | 6 (3) | 2 (2) | 4 (5) | 0.43 |
| Acute brain damage, n (%) (hemorrhage/ischemia) | 9 (2) | 3 (2) | 6 (3) | 0.19 |
| OSAS, n (%) | 4 (2) | 1 (1) | 3 (3) | 0.35 |
| Pulmonary fibrosis, n (%) | 2 (1) | 1 (1) | 1 (1) | 0.9 |
| WNV encephalitis, n (%) | 1 (0.6) | 0 (0) | 1 (1) | 0.48 |
| Part 2. Clinical outcomes * | ||||
| Successful weaning, n (%) | 119 (66.1) | 55 (59.1) | 73.6/26.4 | 0.06 |
| Decannulation, n (%) | 82 (45.6) | 47 (50.5) | 40.2/59.8 | 0.17 |
| Ability to walk, n (%) | 106 (58.9) | 51 (54.8) | 63.2/36.8 | 0.26 |
| BALD change | ||||
| ≤0, n (%) | 48 (26.7) | 18 (19.4) | 30 (34.5) | 0.03 |
| +1, n (%) | 42 (23.3) | 21 (22.6) | 21 (24.1) | 0.86 |
| +2, n (%) | 34 (18.9) | 19 (20.4) | 15 (17.3) | 0.7 |
| +3, n (%) | 20 (11.1) | 15 (16.1) | 5 (5.7) | 0.03 |
| +4, n (%) | 9 (5) | 4 (4.3) | 5 (5.7) | 0.74 |
| +5, n (%) | 10 (5.6) | 6 (6.5) | 4 (4.6) | 0.75 |
| +6, n (%) | 17 (9.4) | 10 (10.8) | 7 (8.1) | 0.8 |
| Discharged, n (%) | 53 (29.4) | 27 (29) | 26 (29.9) | 0.9 |
| Transfer to a residential care facility, n (%) | 97 (53.9) | 47 (50.5) | 50 (57.5) | 0.37 |
| Transfer to acute care hospital, n (%) | 30 (16.7) | 19 (20.4) | 11 (12.6) | 0.23 |
| AGE | SEX | CIRS | SAPS II % | Days at Acute Hospital | Timing of Tracheostomy | ||
|---|---|---|---|---|---|---|---|
| Weaning | R2McF | 0.01 | 0.00165 | 0.0153 | 0.00721 | 0.00111 | 5.86 × 10−4 |
| p-value | 0.05 | 0.48 | 0.03 | 0.14 | 0.57 | 0.68 | |
| Association | No (borderline significant) | No | Yes | No | No | No | |
| Decannulation | R2McF | 0.0154 | 8.01 × 10−5 | 0.0497 | 0.0207 | 0.00369 | 0.00176 |
| p-value | 0.05 | 0.89 | <0.001 | 0.28 | 0.352 | 0.517 | |
| Association | No (borderline significant) | No | Yes | Yes | No | No | |
| Ability to walk | R2McF | 0.0297 | 0.00592 | 0.0757 | 0.00434 | 0.00308 | 0.00334 |
| p-value | 0.01 | 0.23 | < 0.001 | 0.3 | 0.39 | 0.38 | |
| Association | Yes | No | Yes | No | No | No | |
| Any BADL improvement | R2McF | 0.0305 | 0.00137 | 0.0896 | 0.0111 | 0.0021 | 1.36 × 10−4 |
| p-value | < 0.001 | 0.03 | < 0.001 | 0.008 | 0.25 | 0.77 | |
| Association | Yes | No | Yes | Yes | No | No | |
| Weaning | Decannulation | Ability to Walk | Any BADL Improvement | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diagnosis | OR | 95%CI | p-Value | OR | 95%CI | p-Value | OR | 95%CI | p-Value | OR | 95%CI | p-Value |
| COPD | 1.8 | 0.9–3.3 | 0.08 | 1.2 | 0.7–2.2 | 0.5 | 0.8 | 0.5–1.5 | 0.6 | 0.9 | 0.4–1.7 | 0.7 |
| Heart surgery | 1.3 | 0.6–3.2 | 0.5 | 1.1 | 0.5–2.3 | 0.9 | 0.6 | 0.3–1.4 | 0.3 | 0.8 | 0.3–1.8 | 0.5 |
| Abdominal surgery | 0.8 | 0.3–2.2 | 0.8 | 1.2 | 0.5–3 | 0.7 | 1 | 0.4–2.5 | 0.9 | 1.7 | 0.6–5.4 | 0.3 |
| Polytrauma | 0.9 | 0.4–2.5 | 0.9 | 1.9 | 0.7–5 | 0.2 | 1.3 | 0.5–3.5 | 0.7 | 1.1 | 0.4–3.2 | 0.9 |
| Metabolic syndrome | 4.4 | 0.7–50 | 0.2 | 0.9 | 0.2–3.7 | 0.9 | 1.4 | 0.3–5.9 | 0.6 | 1.3 | 0.3–6.4 | 0.8 |
| Thoracic surgery | 2.6 | 0.3–23 | 0.4 | 2.5 | 0.4–14 | 0.3 | 1.4 | 0.2–7.9 | 0.7 | 1.9 | 0.2–16 | 0.6 |
| Acute brain damage (ischemia/hemorrhage) | 1 | 0.3–4.3 | 0.9 | 0.3 | 0.1–1.6 | 0.1 | 0.2 | 0.03–0.9 | 0.02 | 0.1 | 0.03–0.7 | 0.01 |
| OSAS | 1.6 | 0.2–15 | 0.7 | 1.2 | 0.2–8.7 | 0.9 | 2.1 | 0.2–21 | 0.5 | 1 | 0.1–11 | 0.9 |
| Pulmonary fibrosis | 0.5 | 0.03–8.3. | 0.6 | 0.2 | 0.01–4.9 | 0.2 | 3.6 | 0.2–75 | 0.2 | 1.9 | 0.1–39 | 0.4 |
| WNV encephalitis | 1.6 | 0.1–39 | 0.5 | 0.4 | 0.01–9.8 | 0.4 | 2.1 | 0.08–53 | 0.9 | 1.1 | 0.04–28 | 0.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costi, S.; Brogneri, A.; Bagni, C.; Pennacchi, G.; Beneventi, C.; Tabbì, L.; Dell’Orso, D.; Fantini, R.; Tonelli, R.; Beghi, G.M.; et al. Rehabilitation of Difficult-to-Wean, Tracheostomized Patients Admitted to Specialized Unit: Retrospective Analyses over 10-Years. Int. J. Environ. Res. Public Health 2022, 19, 2982. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052982
Costi S, Brogneri A, Bagni C, Pennacchi G, Beneventi C, Tabbì L, Dell’Orso D, Fantini R, Tonelli R, Beghi GM, et al. Rehabilitation of Difficult-to-Wean, Tracheostomized Patients Admitted to Specialized Unit: Retrospective Analyses over 10-Years. International Journal of Environmental Research and Public Health. 2022; 19(5):2982. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052982
Chicago/Turabian StyleCosti, Stefania, Antonio Brogneri, Chiara Bagni, Giulia Pennacchi, Claudio Beneventi, Luca Tabbì, Daniela Dell’Orso, Riccardo Fantini, Roberto Tonelli, Gianfranco Maria Beghi, and et al. 2022. "Rehabilitation of Difficult-to-Wean, Tracheostomized Patients Admitted to Specialized Unit: Retrospective Analyses over 10-Years" International Journal of Environmental Research and Public Health 19, no. 5: 2982. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052982