
Oral Health-Related Quality of Life in Children and Adolescents with a Traumatic Injury of Permanent Teeth and the Impact on Their Families: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
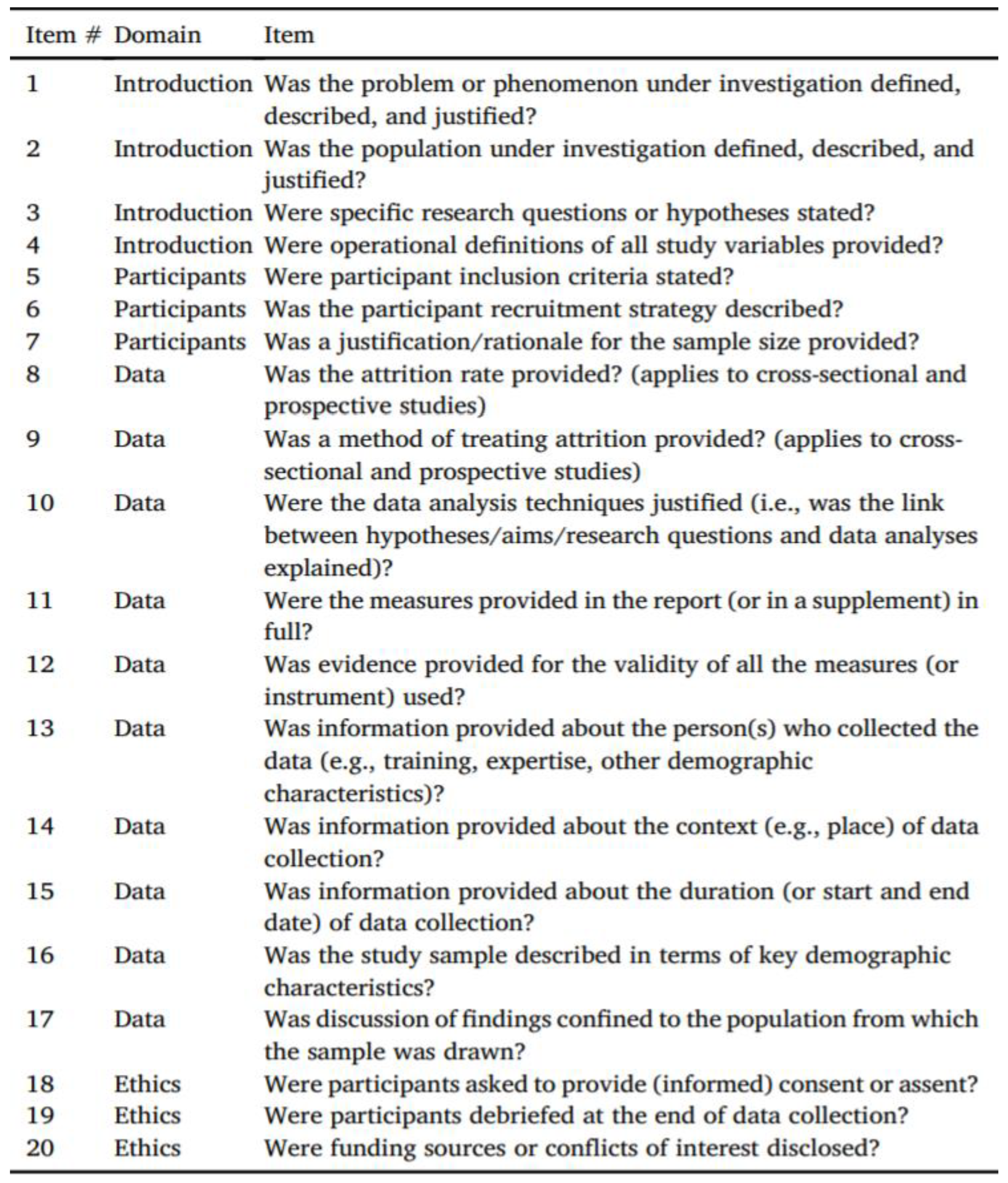
2.3. Study Quality Assessment
3. Results
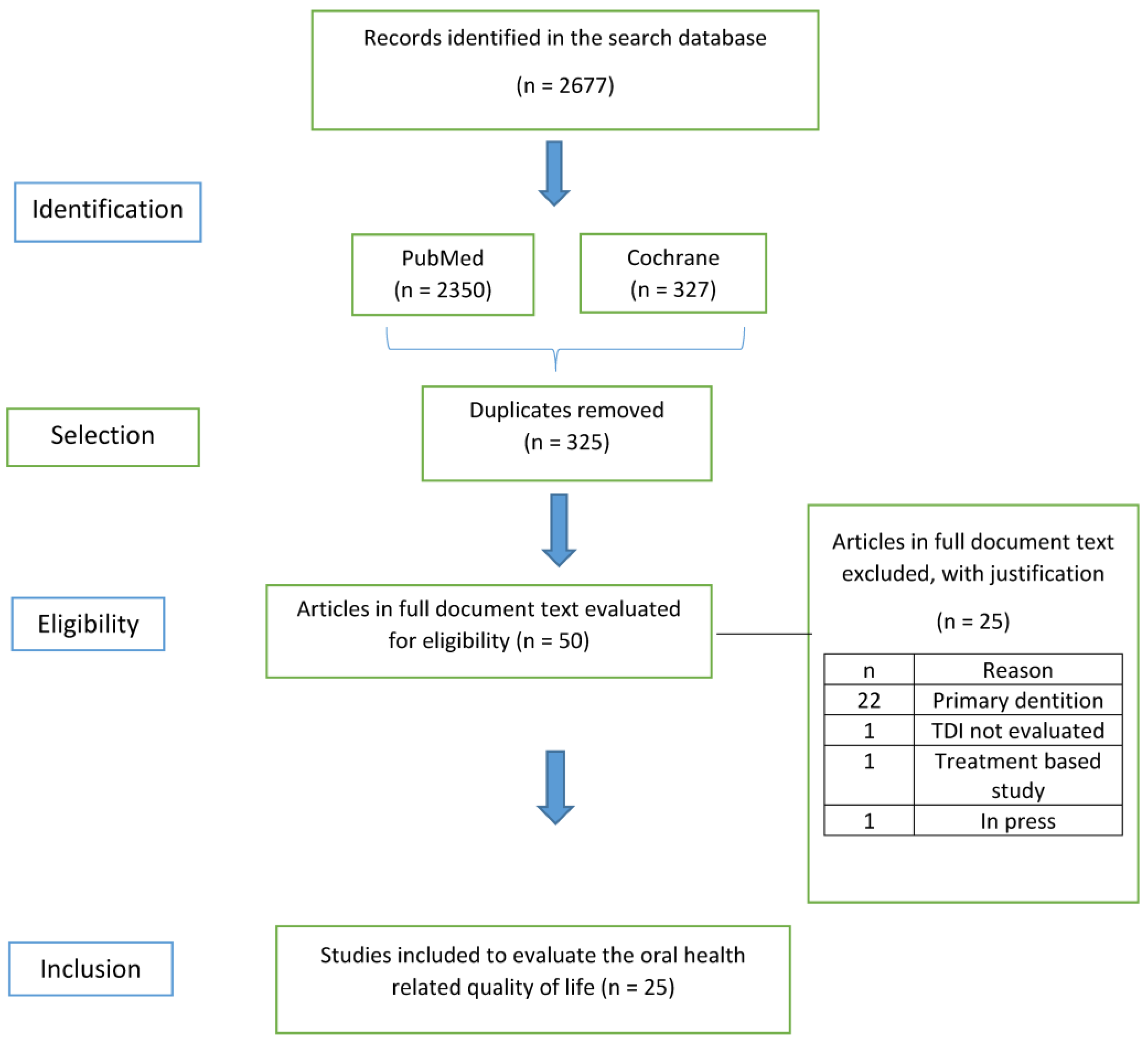
3.1. Selection of Studies
3.2. Characteristics of Studies
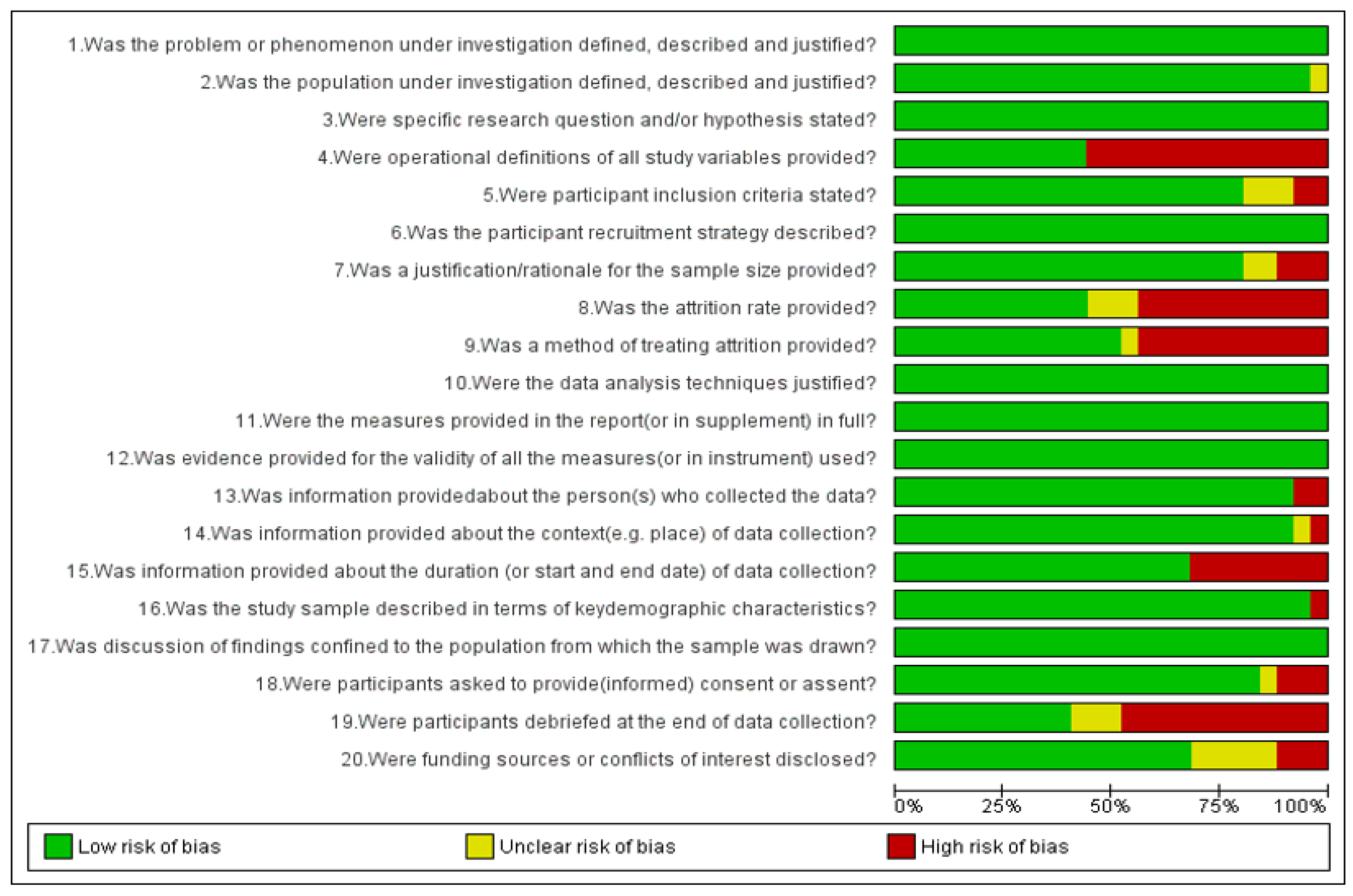
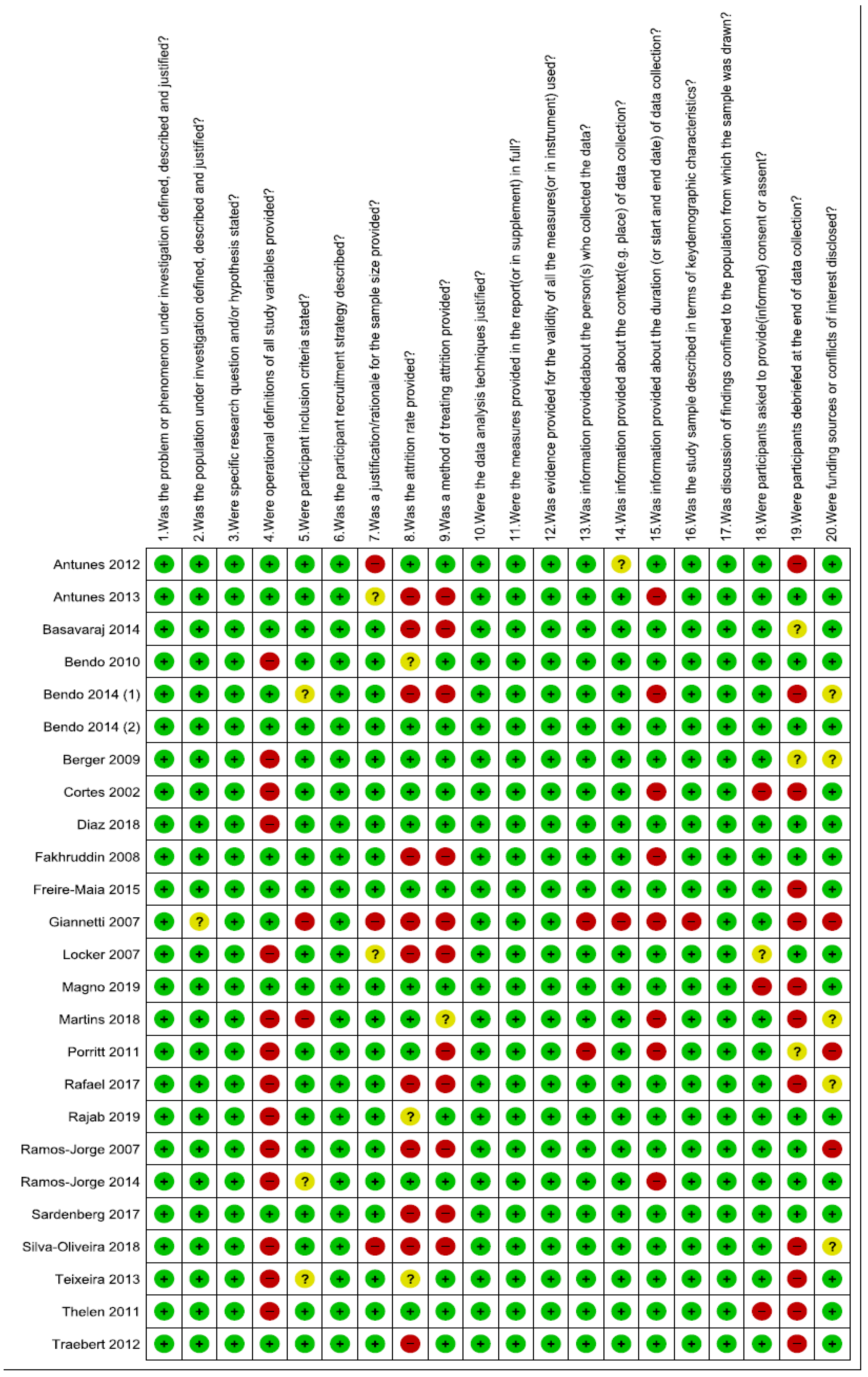
3.3. Analysis of Quality of the Studies
3.4. Synthesis of Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CFED | crown fracture involving enamel and dentin |
| COHQoL | Child Oral Health Quality of Life |
| CPQ | Child Perceptions Questionnaire |
| Child-OIDP | Child-Oral Impact on Daily Performances |
| FIS | Family Impact Scale in three articles |
| ISF | Impact Short Form |
| OIDP | Oral Impact on Daily Performances |
| OHIP | Oral Health Impact Profile |
| OHRQoL | Oral Health-Related Quality of Life |
| P-CPQ | Parental–Caregivers Perceptions Questionnaire |
| Q-SSP | Quality assessment checklist for survey studies in psychology |
| TDI | Traumatic Dental Inury |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Title | Reason for Exclusion |
|---|---|---|
| Flores et al. [63] | How Does Orofacial Trauma in Children Affect the Developing Dentition? Long-term Treatment and Associated Complications | The OHRQoL was not checked. It is a treatment-based study. |
| Gomes et al. [64] | Oral Problems and Self-Confidence in Preschool Children | This study was conducted in primary dentition. |
| Cengiz et al. [65] | Impact of seizure-related injuries on quality of life | TDI has not been evaluated. |
| Sakaryali et al. [66] | Evaluation of the Impact of Early Childhood Caries, Traumatic Dental Injury, and Malocclusion on Oral Health–Related Quality of Life for Turkish Preschool Children and Families | The study was conducted in primary dentition. |
| Soares et al. [10] | The impact of crown fracture in the permanent dentition on children’s quality of life | This article is not published in any journal and is in press. |
| Gonçalves et al. [67] | Impact of dental trauma and esthetic impairment on the quality of life of preschool children. | The study was conducted in primary dentition. |
| Braimah et al. [68] | Self-esteem following maxillofacial and orthopedic injuries: preliminary observations in sub-Saharan Africans | This study did not include permanent dentition. |
| Ramos-Jorge et al. [69] | Parents’ recognition of dental trauma in their children | This study was conducted in primary dentition. |
| Ramos-Jorge et al. [70] | Effect of dark discolouration and enamel/dentine fracture on the oral health-related quality of life of pre-schoolers | This study was conducted in primary dentition. |
| Granville-Garcia et al. [71] | Parental influence on children’s answers to an oral-health-related quality of life questionnaire | This study was conducted in primary dentition. |
| Vieira-Andrade et al. [72] | Impact of traumatic dental injury on the quality of life of young children: a case–control study | This study was conducted in primary dentition. |
| Aldrigui et al. [73] | Impact of traumatic dental injuries and malocclusions on quality of life of young children | This study was conducted in primary dentition. |
| Firmino et al. [74] | Impact of oral health problems on the quality of life of preschool children: a case-control study | This study was conducted in primary dentition. |
| Barbosa Neves et al. [75] | Perception of parents and self-reports of children regarding the impact of traumatic dental injury on quality of life | This study was conducted in primary dentition. |
| Siqueira et al. [76] | Impact of Traumatic Dental Injury on the Quality of Life of Brazilian Preschool Children | This study was conducted in primary dentition. |
| Viegas et al. [77] | Influence of traumatic dental injury on quality of life of Brazilian preschool children and their families | This study was conducted in primary dentition. |
| Gomes et al. [78] | Impact of oral health conditions on the quality of life of preschool children and their families: a cross-sectional study | This study was conducted in primary dentition. |
| Abanto et al. [79] | Impact of traumatic dental injuries and malocclusions on quality of life of preschool children: a population-based study | This study was conducted in primary dentition. |
| Abanto et al. [80] | The impact of dental caries and trauma in children on family quality of life | This study was conducted in primary dentition. |
| Abanto et al. [81] | Impact of dental caries and trauma on quality of life among 5- to 6-year-old children: perceptions of parents and children | This study was conducted in primary dentition. |
| Feldens et al. [82] | Enamel fracture in the primary dentition has no impact on children’s quality of life: implications for clinicians and researchers | This study was conducted in primary dentition. |
| Scarpelli et al. [83] | Oral health-related quality of life among Brazilian preschool children | This study was conducted in primary dentition. |
| Viegas et al. [84] | Impact of Traumatic Dental Injury on Quality of Life Among Brazilian Preschool Children and Their Families | This study was conducted in primary dentition. |
| Kramer et al. [85] | Exploring the impact of oral diseases and disorders on quality of life of preschool children | This study was conducted in primary dentition. |
| Borges et al. [86] | Relationship between overweight/obesity in the first year of age and traumatic dental injuries in early childhood: Findings from a birth cohort study | This study was conducted in primary dentition. |
References
- Goursand, D.; Paiva, S.M.; Zarzar, P.M.; Pordeus, I.A.; Grochowski, R.; Allison, P.J. Measuring parental-caregiver perceptions of child oral health-related quality of life: Psychometric properties of the Brazilian version of the P-CPQ. Braz. Dent. J. 2009, 20, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Pahel, B.T.; Rozier, R.G.; Slade, G.D. Parental perceptions of children’s oral health: The Early Childhood Oral Health Impact Scale (ECOHIS. Health Qual. Life Outcomes 2007, 5, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheiham, A.; Steele, J.G.; Marcenes, W.; Tsakos, G.; Finch, S.; Walls, A.W.G. Prevalence of impacts of dental and oral disorders and their effects on eating among older people; a national survey in Great Britain. Community Dent. Oral Epidemiol. 2001, 29, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Sgan-Cohen, H.D.; Megnagi, G.; Jacobi, Y. Dental trauma and its association with anatomic, behavioral, and social variables among fifth and sixth grade schoolchildren in Jerusalem. Community Dent. Oral Epidemiol. 2005, 33, 174–180. [Google Scholar] [CrossRef]
- Cardoso, M.; De Carvalho Rocha, M.J. Traumatized Primary Teeth in Children Assisted at the Federal University of Santa Catarina, Brazil. Dent. Traumatol. 2002, 18, 129–133. [Google Scholar] [CrossRef]
- Şaroğlu, I.; Sönmez, H. The prevalence of traumatic injuries treated in the pedodontic clinic of Ankara University, Turkey, during 18 months. Dent. Traumatol. 2002, 18, 299–303. [Google Scholar] [CrossRef]
- Eiser, C.; Morse, R. The measurement of quality of life in children: Past and future perspectives. J. Dev. Behav. Pediatr. JDBP 2001, 22, 248–256. [Google Scholar] [CrossRef]
- Allison, P.J.; Locker, D.; Feine, J.S. Quality of life: A dynamic construct. Soc. Sci. Med. 1982, 45, 221–230. [Google Scholar] [CrossRef]
- Ramos-Jorge, J.; Paiva, S.M.; Tataounoff, J.; Pordeus, I.A.; Marques, L.S.; Ramos-Jorge, M.L. Impact of treated/untreated traumatic dental injuries on quality of life among Brazilian schoolchildren. Dent. Traumatol. 2014, 30, 27–31. [Google Scholar] [CrossRef]
- Soares, J.P.; Barasuol, J.C.; Torres, F.M.; Giacomin, A.; Gonçalves, B.M.; Klein, D.; Borgatto, A.F.; Ramos-Jorge, M.L.; Cardoso, M.; Bolan, M. The impact of crown fracture in the permanent dentition on children’s quality of life. Dent. Traumatol. 2018, 34, 158–163. [Google Scholar] [CrossRef]
- Marcenes, W.; Beiruti, N.; Tayfour, D.; Issa, S. Epidemiology of traumatic injuries to the permanent incisors of 9-12-year-old schoolchildren in Damascus, Syria. Endod Dent. Traumatol. 1999, 15, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Granville-Garcia, A.F.; de Menezes, V.A.; de Lira, P.I.C. Dental trauma and associated factors in Brazilian preschoolers. Dent. Traumatol. 2006, 22, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Årtun, J.; Behbehani, F.; Al-Jame, B.; Kerosuo, H. Incisor trauma in an adolescent Arab population: Prevalence, severity, and occlusal risk factors. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Traebert, J.; Bittencourt, D.D.; Peres, K.G.; Peres, M.A.; de Lacerda, J.T.; Marcenes, W. Aetiology and rates of treatment of traumatic dental injuries among 12-year-old school children in a town in southern Brazil. Dent. Traumatol. 2006, 22, 173–178. [Google Scholar] [CrossRef]
- Bendo, C.B.; Paiva, S.M.; Torres, C.S.; Oliveira, A.C.; Goursand, D.; Pordeus, I.A. Association between treated/untreated traumatic dental injuries and impact on quality of life of Brazilian schoolchildren. Health Qual. Life Outcomes 2010, 8, 114. [Google Scholar] [CrossRef] [Green Version]
- Noori, A.J.; Al-Obaidi, W.A. Traumatic dental injuries among primary school children in Sulaimani city, Iraq. Dent. Traumatol. 2009, 25, 442–446. [Google Scholar] [CrossRef]
- Fakhruddin, K.S.; Lawrence, H.P.; Kenny, D.J.; Locker, D. Etiology and environment of dental injuries in 12- to 14-year-old Ontario schoolchildren. Dent. Traumatol. 2008, 24, 305–308. [Google Scholar] [CrossRef]
- Zaleckiene, V.; Peciuliene, V.; Brukiene, V.; Drukteinis, S. Traumatic dental injuries: Etiology, prevalence and possible outcomes. Stomatologija 2014, 16, 7–14. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Protogerou, C.; Hagger, M.S. A checklist to assess the quality of survey studies in psychology. Methods Psychol. 2020, 3, 100031. [Google Scholar] [CrossRef]
- Díaz, S.; Vélez, M.P.; Martínez, L.M.; Ramos, K.; Boneckër, M.; Martins Paiva, S.; Abanto, J. Parental perceptions of impact of oral disorders on Colombian schoolchildren’s oral healthrelated quality of life. Acta. Odontol. Latinoam. 2018, 31, 82–90. [Google Scholar] [PubMed]
- Martins, M.T.; Sardenberg, F.; Bendo, C.B.; Vale, M.P.; Paiva, S.M.; Pordeus, I.A. Dental caries are more likely to impact on children’s quality of life than malocclusion or traumatic dental injuries. Eur. J. Paediatr. Dent. 2018, 19, 194–198. [Google Scholar] [PubMed]
- Freire-Maia, F.B.; Auad, S.M.; Abreu, M.H.N.G.D.; Sardenberg, F.; Martins, M.T.; Paiva, S.M.; Pordeus, I.A.; Vale, M.P. Oral Health-Related Quality of Life and Traumatic Dental Injuries in Young Permanent Incisors in Brazilian Schoolchildren: A Multilevel Approach. PLoS ONE 2015, 10, e0135369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardenberg, F.; Cavalcante-Leão, B.L.; Todero, S.R.B.; Ferreira, F.M.; Rebellato, N.L.B.; Fraiz, F.C. A population-based study on the impact of orofacial dysfunction on oral health-related quality of life among Brazilian schoolchildren. Acta Odontol. Scand. 2017, 75, 173–178. [Google Scholar] [CrossRef]
- Silva-Oliveira, F.; Goursand, D.; Ferreira, R.C.; Paiva, P.C.P.; Paiva, H.N.; Ferreira, E.F.; Zarzar, P.M. Traumatic dental injuries in Brazilian children and oral health-related quality of life. Dent. Traumatol. 2018, 34, 28–35. [Google Scholar] [CrossRef]
- Rajab, L.D.; Abu Al Huda, D. Impact of treated and untreated traumatic dental injuries on oral health-related quality of life among 12-year-old schoolchildren in Amman. Dent. Traumatol. 2019, 35, 153–162. [Google Scholar] [CrossRef]
- Damé-Teixeira, N.; Alves, L.S.; Ardenghi, T.M.; Susin, C.; Maltz, M. Traumatic dental injury with treatment needs negatively affects the quality of life of Brazilian schoolchildren. Int. J. Paediatr. Dent. 2013, 23, 266–273. [Google Scholar] [CrossRef]
- Basavaraj, P.; Sunil, M.K.; Nagarajappa, R.; Ashish, S.; Ramesh, G. Correlation between oral health and Child-OIDP index in 12- and 15-year-old children from Modinagar, India. Asia Pac. J. Public Health 2014, 26, 390–400. [Google Scholar] [CrossRef]
- Bendo, C.B.; Paiva, S.M.; Abreu, M.H.; Figueiredo, L.D.; Vale, M.P. Impact of traumatic dental injuries among adolescents on family’s quality of life: A population-based study. Int. J. Paediatr. Dent. 2014, 24, 387–396. [Google Scholar] [CrossRef]
- Bomfim, R.A.; Herrera, D.R.; De-Carli, A.D. Oral health-related quality of life and risk factors associated with traumatic dental injuries in Brazilian children: A multilevel approach. Dent. Traumatol. 2017, 33, 358–368. [Google Scholar] [CrossRef]
- Bendo, C.B.; Paiva, S.M.; Varni, J.W.; Vale, M.P. Oral health-related quality of life and traumatic dental injuries in Brazilian adolescents. Community Dent. Oral Epidemiol. 2014, 42, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Antunes, L.S.; Debossan, P.F.; Bohrer, L.S.; Abreu, F.V.; Quintanilha, L.E.L.P.; Antunes, L.A.A. Impact of traumatic dental injury on the quality-of-life of children and adolescents: A case-control study. Acta Odontol. Scand. 2013, 71, 1123–1128. [Google Scholar] [CrossRef] [PubMed]
- Fakhruddin, K.S.; Lawrence, H.P.; Kenny, D.J.; Locker, D. Impact of treated and untreated dental injuries on the quality of life of Ontario school children. Dent. Traumatol. 2008, 24, 309–313. [Google Scholar] [CrossRef] [PubMed]
- Thelen, D.S.; Trovik, T.A.; Bårdsen, A. Impact of traumatic dental injuries with unmet treatment need on daily life among Albanian adolescents: A case-control study. Dent. Traumatol. 2011, 27, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Ilma de Souza Cortes, M.; Marcenes, W.; Sheiham, A. Impact of traumatic injuries to the permanent teeth on the oral health-related quality of life in 12-14-year-old children. Community Dent. Oral Epidemiol. 2002, 30, 193–198. [Google Scholar] [CrossRef]
- Ramos-Jorge, M.L.; Bosco, V.L.; Peres, M.A.; Nunes, A.C.G.P. The impact of treatment of dental trauma on the quality of life of adolescents ? A case-control study in southern Brazil. Dent. Traumatol. 2007, 23, 114–119. [Google Scholar] [CrossRef]
- Antunes, L.A.A.; Luiz, R.R.; Leão, A.T.T.; Maia, L.C. Initial assessment of responsiveness of the P-CPQ (Brazilian Version) to describe the changes in quality of life after treatment for traumatic dental injury. Dent. Traumatol. 2012, 28, 256–262. [Google Scholar] [CrossRef]
- Magno, M.B.; Jural, L.A.; Nogueira, A.D.V.; Lenzi, M.M.; Pithon, M.M.; Maia, L.C. Impact of crown fracture treatment on oral health-related quality of life of children, adolescents, and their families: A prospective clinical study. Int. J. Paediatr. Dent. 2019, 29, 86–93. [Google Scholar] [CrossRef] [Green Version]
- Giannetti, L.; Murri, A.; Vecci, F.; Gatto, R. Dental avulsion: Therapeutic protocols and oral health-related quality of life. Eur. J. Paediatr. Dent. 2007, 2, 69–75. [Google Scholar]
- Berger, T.D.; Kenny, D.J.; Casas, M.J.; Barrett, E.J.; Lawrence, H.P. Effects of severe dentoalveolar trauma on the quality-of-life of children and parents. Dent. Traumatol. 2009, 25, 462–469. [Google Scholar] [CrossRef]
- Porritt, J.M.; Rodd, H.D.; Ruth Baker, S. Quality of life impacts following childhood dento-alveolar trauma. Dent. Traumatol. 2011, 27, 2–9. [Google Scholar] [CrossRef] [PubMed]
- Locker, D. Disparities in oral health-related quality of life in a population of Canadian children. Community Dent. Oral Epidemiol. 2007, 35, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Traebert, J.; de Lacerda, J.T.; Foster Page, L.A.; Thomson, W.M.; Bortoluzzi, M.C. Impact of traumatic dental injuries on the quality of life of schoolchildren. Dent. Traumatol. 2012, 28, 423–428. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General; U.S. Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health: Rockville, MD, USA, 2000. Available online: https://www.nidcr.nih.gov/sites/default/files/2017-10/hck1ocv.%40www.surgeon.fullrpt.pdf (accessed on 2 March 2022).
- Sischo, L.; Broder, H.L. Oral health-related quality of life: What, why, how, and future implications. J. Dent. Res. 2011, 90, 1264–1270. [Google Scholar] [CrossRef] [Green Version]
- Kavaliauskienė, A.; Šidlauskas, A.; Zaborskis, A. Modification and psychometric evaluation of the child perceptions questionnaire (CPQ11-14) in assessing oral health related quality of life among Lithuanian children. BMC Oral Health 2019, 19, 1. [Google Scholar] [CrossRef]
- Gherunpong, S.; Tsakos, G.; Sheiham, A. Developing and evaluating an oral health-related quality of life index for children; the CHILD-OIDP. Community Dent. Health 2004, 21, 161–169. [Google Scholar]
- Bernabé, E.; Oliveira, C.M.; Sheiham, A.; Tsakos, G. Comparison of the generic and condition-specific forms of the Oral Impacts on Daily Performances (OIDP) Index. J. Public Health Dent. 2009, 69, 176–181. [Google Scholar] [CrossRef]
- Soriano, E.P.; Caldas, A.D., Jr.; Carvalho, M.V.; Amorim Filho, H.D. Prevalence and risk factors related to traumatic dental injuries in Brazilian schoolchildren. Dent. Traumatol. 2007, 23, 232–240. [Google Scholar] [CrossRef]
- Glendor, U. Epidemiology of traumatic dental injuries—A 12 year review of the literature. Dent. Traumatol. 2008, 24, 603–611. [Google Scholar] [CrossRef]
- De Carvalho Rocha, M.J.; Cardoso, M. Traumatized permanent teeth in Brazilian children assisted at the Federal University of Santa Catarina, Brazil. Dent. Traumatol. 2001, 17, 245–249. [Google Scholar] [CrossRef]
- Leme, M.S.; de Souza Barbosa, T.; Gavião, M.B. Relationship among oral habits, orofacial function and oral health-related quality of life in children. Braz. Oral Res. 2013, 27, 272–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Sayans, M.; Fernandez-Gonzalez, B.; Somoza-Martin, M.; Gándara-Rey, J.M.; García-García, A. Peri-Implant Bone Resorption around Implants Placed in Alveolar Bone Subjected to Distraction Osteogenesis. J. Oral Maxillofac. Surg. 2008, 66, 787–790. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, T.S.; Tureli, M.C.M.; Gavião, M.B.D. Validity and reliability of the Child Perceptions Questionnaires applied in Brazilian children. BMC Oral Health 2009, 9, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shaw, W.C. The influence of children’s dentofacial appearance on their social attractiveness as judged by peers and lay adults. Am. J. Orthod. 1981, 79, 399–415. [Google Scholar] [CrossRef]
- Marcenes, W.; Murray, S. Social deprivation and traumatic dental injuries among 14-year-old schoolchildren in Newham, London. Dent. Traumatol. 2001, 17, 17–21. [Google Scholar] [CrossRef]
- Cortes, M.I.S.; Marcenes, W.; Sheiham, A. Prevalence and correlates of traumatic injuries to the permanent teeth of school-children aged 9-14 years in Belo Horizonte, Brazil. Dent. Traumatol. 2001, 17, 22–26. [Google Scholar] [CrossRef]
- Damé-Teixeira, N.; Alves, L.S.; Susin, C.; Maltz, M. Traumatic dental injury among 12-year-old South Brazilian schoolchildren: Prevalence, severity, and risk indicators. Dent. Traumatol. 2013, 29, 52–58. [Google Scholar] [CrossRef]
- Bendo, C.B.; Paiva, S.M.; Oliveira, A.C.; Goursand, D.; Torres, C.S.; Pordeus, I.A. Prevalence and associated factors of traumatic dental injuries in Brazilian schoolchildren. J. Public Health Dent. 2010, 70, 313–318. [Google Scholar] [CrossRef]
- Marques, L.S.; Ramos-Jorge, M.L.; Paiva, S.M.; Pordeus, I.A. Malocclusion: Esthetic impact and quality of life among Brazilian schoolchildren. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 424–427. [Google Scholar] [CrossRef]
- Jokovic, A.; Locker, D.; Guyatt, G. What do children’s global ratings of oral health and well-being measure? Community Dent. Oral Epidemiol. 2005, 33, 205–211. [Google Scholar] [CrossRef]
- Ahrari, F.; Heravi, F.; Rashed, R.; Zarrabi, M.J.; Setayesh, Y. Which Factors Affect Dental Esthetics and Smile Attractiveness in Orthodontically Treated Patients? J. Dent. Tehran Iran 2015, 12, 491. [Google Scholar]
- Flores, M.T.; Onetto, J.E. How does orofacial trauma in children affect the developing dentition? Long-term treatment and associated complications. Dent. Traumatol. 2019, 35, 312–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomes, M.C.; Perazzo, M.F.; Neves, É.T.; Martins, C.C.; Paiva, S.M.; Granville-Garcia, A.F. Oral problems and self-confidence in preschool children. Braz. Dent. J. 2017, 28, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, O.; Atalar, A.Ç.; Tekin, B.; Bebek, N.; Baykan, B.; Gürses, C. Impact of seizure-related injuries on quality of life. Neurol. Sci. 2019, 40, 577–583. [Google Scholar] [CrossRef]
- Sakaryali, D.; Bani, M.; Cinar, C.; Alacam, A. Evaluation of the impact of early childhood caries, traumatic dental injury, and malocclusion on oral health-Related quality of life for Turkish preschool children and families. Niger. J. Clin. Pract. 2019, 22, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, B.M.; Dias, L.F.; Da Silva Pereira, C.; Filho, M.X.P.; Konrath, A.C.; Da Silva Bolan, M.; Cardoso, M. Impact of dental trauma and esthetic impairment on the quality of life of preschool children. Rev. Paul. Pediatr. 2017, 35, 448–455. [Google Scholar] [CrossRef] [Green Version]
- Braimah, R.O.; Ukpong, D.I.; Ndukwe, K.C.; Akinyoola, L. Self-esteem following maxillofacial and orthopedic injuries: Preliminary observations in sub-Saharan Africans. Oral Maxillofac. Surg. 2019, 23, 71–76. [Google Scholar] [CrossRef]
- Ramos-Jorge, M.L.; Ramos-Jorge, J.; Mota-Veloso, I.; Oliva, K.J.; Zarzar, P.M.; Marques, L.S. Parents’ recognition of dental trauma in their children. Dent. Traumatol. 2013, 29, 266–271. [Google Scholar] [CrossRef]
- Ramos-Jorge, J.; Sá-Pinto, A.C.; Almeida Pordeus, I.; Martins Paiva, S.; Castro Martins, C.; Ramos-Jorge, M.L. Effect of dark discolouration and enamel/dentine fracture on the oral health-related quality of life of pre-schoolers. Eur. Arch. Paediatr. Dent. 2017, 18, 83–89. [Google Scholar] [CrossRef]
- Granville-Garcia, A.F.; Gomes, M.C.; Dantas, L.R.; Dantas, L.R.; da Silva, B.R.C.; Perazzo, M.D.F.; Siqueira, M.B.L.D. Parental influence on children’s answers to an oral-health-related quality of life questionnaire. Braz. Oral Res. 2016, 30, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Vieira-Andrade, R.G.; Siqueira, M.B.L.; Gomes, G.B.; D’Avila, S.; Pordeus, I.A.; Paiva, S.M.; Granville-Garcia, A.F. Impact of traumatic dental injury on the quality of life of young children: A case-control study. Int. Dent. J. 2015, 65, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Aldrigui, J.M.; Abanto, J.; Carvalho, T.S.; Mendes, F.M.; Wanderley, M.T.; Bönecker, M.; Raggio, D.P. Impact of traumatic dental injuries and malocclusions on quality of life of young children. Health Qual. Life Outcomes 2011, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Firmino, R.T.; Gomes, M.C.; Clementino, M.A.; Martins, C.C.; Paiva, S.M.; Granville-Garcia, A.F. Impact of oral health problems on the quality of life of preschool children: A case–control study. Int. J. Paediatr. Dent. 2016, 26, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Barbosa Neves, É.T.; Perazzo, M.F.; Gomes, M.C.; Martins, C.C.; Paiva, S.M.; Granville-Garcia, A.F. Perception of parents and self-reports of children regarding the impact of traumatic dental injury on quality of life. Dent. Traumatol. 2017, 33, 444–450. [Google Scholar] [CrossRef]
- Siqueira, M.B.; Firmino, R.T.; Clementino, M.A.; Martins, C.C.; Granville-Garcia, A.F.; Paiva, S.M. Impact of traumatic dental injury on the quality of life of Brazilian preschool children. Int. J. Environ. Res. Public Health 2013, 10, 6422–6441. [Google Scholar] [CrossRef] [Green Version]
- Viegas, C.M.; Paiva, S.M.; Carvalho, A.C.; Scarpelli, A.C.; Ferreira, F.M.; Pordeus, I.A. Influence of traumatic dental injury on quality of life of Brazilian preschool children and their families. Dent. Traumatol. 2014, 30, 338–347. [Google Scholar] [CrossRef]
- Gomes, M.C.; Pinto-Sarmento, T.C.D.A.; Costa, E.M.M.D.B.; Martins, C.C.; Granville-Garcia, A.F.; Paiva, S.M. Impact of oral health conditions on the quality of life of preschool children and their families: A cross-sectional study. Health Qual. Life Outcomes 2014, 12, 55. [Google Scholar] [CrossRef] [Green Version]
- Abanto, J.; Tello, G.; Bonini, G.C.; Oliveira, L.B.; Murakami, C.; Bönecker, M. Impact of traumatic dental injuries and malocclusions on quality of life of preschool children: A population-based study. Int. J. Paediatr. Dent. 2015, 25, 18–28. [Google Scholar] [CrossRef]
- Abanto, J.; Paiva, S.M.; Raggio, D.P.; Celiberti, P.; Aldrigui, J.M.; Bönecker, M. The impact of dental caries and trauma in children on family quality of life. Community Dent. Oral Epidemiol. 2012, 40, 323–331. [Google Scholar] [CrossRef]
- Abanto, J.; Tsakos, G.; Paiva, S.M.; Carvalho, T.S.; Raggio, D.P.; Bönecker, M. Impact of dental caries and trauma on quality of life among 5- to 6-year-old children: Perceptions of parents and children. Community Dent. Oral Epidemiol. 2014, 42, 385–394. [Google Scholar] [CrossRef]
- Feldens, C.A.; Day, P.; Borges, T.S.; Feldens, E.G.; Kramer, P.F. Enamel fracture in the primary dentition has no impact on children’s quality of life: Implications for clinicians and researchers. Dent. Traumatol. 2016, 32, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Scarpelli, A.C.; Paiva, S.M.; Viegas, C.M.; Carvalho, A.C.; Ferreira, F.M.; Pordeus, I.A. Oral health-related quality of life among Brazilian preschool children. Community Dent. Oral Epidemiol. 2013, 41, 336–344. [Google Scholar] [CrossRef] [PubMed]
- Viegas, C.M.; Scarpelli, A.C.; Carvalho, A.C.; De Morais Ferreira, F.; Pordeus, I.A.; Paiva, S.M. Impact of traumatic dental injury on quality of life among brazilian preschool children and their families. Pediatr. Dent. 2012, 34, 300–306. [Google Scholar] [PubMed]
- Kramer, P.F.; Feldens, C.A.; Helena Ferreira, S.; Bervian, J.; Rodrigues, P.H.; Peres, M.A. Exploring the impact of oral diseases and disorders on quality of life of preschool children. Community Dent. Oral Epidemiol. 2013, 41, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Borges, T.S.; Chaffee, B.W.; Kramer, P.F.; Feldens, E.G.; Vítolo, M.R.; Feldens, C.A. Relationship between overweight/obesity in the first year of age and traumatic dental injuries in early childhood: Findings from a birth cohort study. Dent. Traumatol. 2017, 33, 465–471. [Google Scholar] [CrossRef]




| Search Strategy |
|---|
| #1 (Quality of life[MeSH Terms] OR Quality of life[Title/Abstract] OR QoL[Title/Abstract] OR OHRQoL[Title/Abstract] OR Early Childhood Oral Health Impact Scale[Title/Abstract] OR ECOHIS[Title/Abstract] OR Child Perceptions Questionnaire[Title/Abstract] OR CPQ 8–10[Title/Abstract] OR CPQ 11–14[Title/Abstract] OR Child-OIDP[Title/Abstract] OR SOHO[Title/Abstract] OR COHIP[Title/Abstract] OR PCPQ[Title/Abstract] OR Scale of Oral Health Outcomes[Title/Abstract] OR Psychology[Title/Abstract] OR Self esteem[Title/Abstract] |
| #2 (tooth injuries[MeSH Terms] OR tooth injuries[Title/Abstract] OR dental injuries[Title/Abstract] OR dental trauma[Title/Abstract] OR dentoalveolar trauma[Title/Abstract] OR tooth avulsion[Title/Abstract] OR Tooth Dislocation[Title/Abstract] OR Tooth Luxation[Title/Abstract] OR tooth intrusion[Title/Abstract] OR dental intrusion[Title/Abstract] OR tooth extrusion[Title/Abstract] OR tooth subluxation[Title/Abstract] OR Tooth Fractures[Title/Abstract] OR permanent teeth |
| Final search done:#1 and #2 |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
|
|
|
|
|
|
|
| Author/Year | Population Investigated | Age Group | Instrument | TDI Index | Association of TDI and OHRQoL | Conclusions | Funding |
|---|---|---|---|---|---|---|---|
| Diaz et al. (2018) [21] | Colombia | 6–14 years | P-CPQ of COHRQoL | Andreasen | No | Children who studied at public schools were more likely to experience a negative impact on the emotional wellbeing and social wellbeing domains. There was no association between traumatic dental injuries and the perception of the impact of OHRQoL, but this may be due to the low prevalence of TDI in the sample. | None. |
| Antunes et al. (2012) [37] | Brazil | 8–14 years | P-CPQ Brazilian version | Andreasen | Yes | The tooth most affected was the right maxillary central incisor (41.2%). The type of tissue most injured was dental tissue (54.8%). The most prevalent type of TDI was fracture of enamel and dentin (48.9%). It could be observed that the highest levels of impact and its reduction after treatment were in the group of trauma affecting both dental and support tissue. However, noticeable change over time could be identified (positive reduction) for all types of TDI, which denotes 100% of the population benefitting from trauma treatment. | DAB/SAS/MS (Department of Primary Care/Secretary of Health Care/Ministry of Health), DECIT/SCTIE/MS (Department of Science and Technology/Secretary of Science, Technology and Strategic Resources/Ministry of Health)—CNPq (The National Council for Scientific and Technological Development) and FAPERJ. |
| Magno et al. (2019) [38] | Brazil | 8–14 years | CPQ8–10, CPQ11–14, P-CPQ, FIS | Andreasen | Yes | In general, children (aged 8–10 years) and adolescents (aged 10–14 years) presented with a reduction of the negative impact of OHRQoL following restorative treatment of CFED; however, the completion of the same treatment did not affect the OHRQoL of their families. | Coordenacao de Aperfeicoamnto de Pessoal de. |
| Berger et al. (2009) [40] | Canada | 8–20 years | CPQ8–10, CPQ11–14, PPQ and FIS | Yes | Children and adolescents who sustain a dental injury severe enough to warrant splinting of the maxillary anterior teeth suffer an immediate decrease in their QoL. Results indicated that at one year, children are affected mostly in the emotional or social well-being domains, yet their parents exclusively reported one-year effects that were based on oral symptoms and functional limitations. Results from the emotional well-being component of the COHQoL questionnaire indicate that dental trauma continues to cause emotional distress and financial difficulties for the injured child and their parent one year later. | Dentistry Clinical Research Fund: Rhani Ghar Grotto Endowment. | |
| Martins et al. (2018) [22] | Brazil | 8–10 years | CPQ8–10 | Andreasen | Yes | Children who presented with dental caries associated with TDI, as well as dental caries associated with malocclusion, were more likely to experience a high negative impact on their OHRQoL than those without any oral condition. Children with the three oral conditions were 2.01-fold more likely to experience a high negative impact on their OHRQoL (total score) than those without any oral health problems. | Not stated. |
| Sardenberg et al. (2017) [24] | Brazil | 8–10 years | CPQ8–10 | Andreasen | Yes | The mean CPQ8–10 score was 1.38-fold (95% CI: 1.17–1.63; p < 0.001) higher among the girls than boys, and children from families with a higher income had lower CPQ8–10 scores (RR: 0.67, 95% CI: 0.51–0.88; p < 0.004) than those from families with a lower income. Children who sought dental care due to pain or factors other than prevention, those with orofacial dysfunction, and those with a history of TDI also experienced a greater impact on OHRQoL. | Conselho Nacional de Desenvolvimento Científico e Tecnológico and Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. |
| Freire-Maia et al. (2015) [23] | Brazil | 8–10 years | CPQ8–10 Brazilian version | Andreasen | Yes | Girls had a 1.46-fold greater chance of presenting a high negative impact on OHRQoL and younger children had more chance of a high negative impact. Children with severe dental trauma (55.9%) reported more negative impact on OHRQoL than children with dental caries (44.4%) and/or accentuated anterior maxillary overjet (41.1%). | National Council for Scientific and Technological Development (CNPq), the Ministry of Science and Technology, and the State of Minas Gerais Research Foundation (FAPEMIG), Brazilian Coordination of Higher Education (CAPES), Brazil. |
| Silva-Oliveira et al. (2018) [25] | Brazil | 12 years | CPQ11–14—ISF:16 short form | Andreasen | Yes | The central incisors were the most affected teeth. TDI was associated with an overjet equal to or greater than 3 mm. There was also an association of the negative impact on oral health-related quality of life, among patients who presented with TDI, in the social well-being and emotional well-being subscales. No association between TDI and socioeconomic factors was observed. | Not stated. |
| Rajab et al. (2019) [26] | Jordan | 12 years | CPQ11–14 Arabic version | Andreasen | Yes | When each of the 16 items of the CPQ11–14 was considered, higher impacts were reported by children who had untreated TDI. The mean scores of the 16 items of the CPQ11–14 were higher in the group of untreated TDI than those in both the group treated TDI and the group with absence of trauma. The results of the present study confirm the negative impact of untreated TDI on QoL of schoolchildren. | Not stated. |
| Bendo et al. (2010) [15] | Brazil | 11–14 years | CPQ11–14 Brazilian version | Andreasen | Yes | Children with untreated TDI were 1.2-fold (95% CI = 0.9–1.6) more likely to feel “upset” and 1.2-fold (95% CI = 0.9–1.7) more likely to have “avoided smiling/ laughing” than children without TDI. In the comparison of children with treated fractures and those without TDI, there was no association to the overall CPQ11–14—ISF: 16 score (Fisher = 0.610). Dental pain and difficulty chewing were more prevalent among children with treated teeth than those with no TDI, but this difference did not achieve statistical significance (p > 0.05). | National Council for Scientific and Technological Development (CNPq), Ministry of Science and Technology, and the State of Minas Gerais Research Foundation (FAPEMIG), Brazil. |
| Bendo et al. (2014) (1) [31] | Brazil | 11–14 years | CPQ11–14 Brazilian version | Andreasen | Yes | Age was not associated with impact on adolescents’ OHRQoL. However, adolescents diagnosed with fractures involving dentin and/or pulp, untreated dental caries, and malocclusion had a greater chance of presenting high negative impact on OHRQoL. The results demonstrated that adolescents diagnosed with fractures involving dentin and/or pulp had a 2.40-fold greater chance of presenting high negative impact on QHRQoL than those without evidence of TDI. | Coordination for the Improvement of Higher-Level Education Personnel (CAPES), the National Council for Scientific and Technological Development (CNPq), and the State of Minas Gerais Research Foundation (FAPEMIG), Brazil. |
| Porrit et al. (2011) [41] | UK | 7–17 years | CPQ11–14 – ISF:16 short form | Andreasen | Yes | The results revealed that girls were more likely to report a higher level of impact on their OHRQoL and HRQoL than boys following traumatic injury to their permanent incisors. | Not stated. |
| Traebert et al. (2012) [43] | Brazil | 11–14 years | CPQ11–14 – ISF:16 short form | O’Brien | Yes | Enamel fractures were the most common form of TDI, while adhesive restoration was the most common form of treatment needed for TDI. This study showed a statistically significant and independent association between TDI and OHRQoL among Brazilian 11–14-year-old schoolchildren. | Grant from FAPESC – Fundacao de Apoio a. |
| Dame-Texeira et al. (2013) [27] | Brazil | 12 years | CPQ11–14- ISF:16 short form | O’Brien | No | Individuals presenting TDI with treatment needs experienced a higher average CPQ11–14 score than individuals with no TDI or with TDI without treatment needs. The main finding was that schoolchildren affected by TDI and needing clinical intervention had significantly higher adjusted mean CPQ11–14 scores for function impairment than those with no TDI or affected by TDI with no treatment needs, indicating a significant but limited effect on quality of life. Where no overall association was observed between TDI and OHRQoL, a domain-specific analysis revealed significant association between TDI and function impairment. Schoolchildren presenting with TDI with clinical treatment needs (e.g., restorations, crowns, root canal therapy) had a 1.2-fold higher adjusted mean CPQ11–14 score than the reference group (no TDI/no treatment needs). | None. |
| Antunes et al. (2013) [32] | Brazil | 10–15 y | CPQ11–14 – ISF:16 short form | WHO 1997 | Yes | Children and adolescents with traumatic dental injury were more likely to have a greater impact on their life than those with no injuries. Traumatic dental injury actually affects the quality-of-life of children and adolescents and, consequently, it is not enough to treat only its signs and physical symptoms. In fact, oral symptoms but also functional limitations and emotional and social well-being should be considered. | Not stated. |
| Locker et al. (2007) [42] | Canada | 11/12 years 13/14 years | CPQ11–14—10 short form | Dental Trauma Index | Yes | Over one third, 37.5%, showed evidence of injury to the anterior dentition (DTI codes of 1–5), with 15.3% having one or more teeth with severe injury (DTI codes of 2–5). Children from low-income households had higher scores on a short form of the CPQ11–14 than children from high-income households, indicating poorer oral health-related quality of life. | Grant from the Ontario Ministry of Health. |
| Fakhruddin et al. (2008) [33] | Canada | 12–14 years | CPQ11–14—10 short form | Dental Trauma Index | Yes | Children with untreated dental injuries were approximately three times more likely to report difficulty chewing than those without injury. Subjects with untreated dental trauma were approximately three times more likely to avoid smiling or laughing and four times more likely to report not wanting to talk to other children compared with uninjured controls. The impact of dental trauma to upper incisors on social well-being was greater than on functional and psychological well-being in this sample of 12–14-year-old schoolchildren. Those with untreated dental injuries experienced a higher risk of negative social impact on their daily living than those without injury. | Grant from the Ontario Ministry of Health. |
| Bendo et al. (2014) (2) [29] | Brazil | 11–14 years | FIS Brazilian version | Andreasen | Yes | TDI severity was directly associated with an impact on the family’s QoL, especially regarding parental/family activities. Parents/caregivers of adolescents with fractures involving the dentine or dentine/pulp reported more negative impact on parental/family activities than those with less severe TDI, such as enamel fracture. | Coordination for the Improvement of Higher-Level Education Personnel (CAPES), Ministry of Education, and the State of Minas Gerais Research Foundation (FAPEMIG), Brazil. |
| Gianenetti et al. (2007) [39] | Italy | Under 18 years | OHIP-14 | Andreasen | Yes | It was a single tooth avulsed in 63.3% of the population, 49.5% was central incisor. Adverse impacts on OHRQoL were reported much more frequently among patients who got into failure of replantation compared with patients who got into successful replantation. The findings show that if patients got into tooth avulsion, then their quality of life is adversely affected. | Not stated. |
| Bomfim et al. (2017) [30] | Brazil | 12 years | National Research in Oral Health (SBBrasil2010) | Yes | Regarding occlusal characteristics, crowding in at least one segment was associated with trauma in the maxillary teeth and in mandibular teeth. Crowding in two segments increased the chances of fracture. The spacing/diastema between the arches was a risk factor for enamel fractures, fractures in mandibular teeth, and for any fracture analyzed. The presence of a diastema and mandibular overjet was not associated with any type of TDI. Maxillary overjet (greater than 3 mm) was associated with all fractures in maxillary teeth. Anterior open bite was a protective factor for enamel fractures in maxillary teeth and any analyzed TDI. | Not stated. | |
| Ramos-Jorge et al. (2014) [9] | Brazil | 11–14 years | Child-OIDP | O’Brien | Yes | Schoolchildren with untreated TDI experienced a greater negative impact on quality of life in comparison with those without TDI. This impact was significant regarding eating and smiling. No significant differences were found on the Child-OIDP between schoolchildren with treated TDI and those without TDI. The association between untreated TDI and impact on quality of life in the present study was stronger for ‘eating and enjoying food’ and ‘smiling and showing teeth’. | Brazilian fostering agencies the Coordination of Higher Education (CAPES), Ministry of Education, and the State of Minas Gerais Research Foundation (FAPEMIG). |
| Thelen et al. (2011) [34] | Albania | 16–19 years | OIDP | O’Brien | Yes | The overall impact prevalence of OIDP among cases was significantly higher (88.4%) than for the controls (58.9%). The most prevalent impact was ‘smiling and showing teeth without embarrassment’ which was reported by cases 78.9% and their controls 31.6%. The second-most prevalent impact was ‘enjoying contact with people’. TDI with unmet treatment needs in this sample of adolescents are associated with reduced OHRQoL. Compared to adolescents with no history of TDI, those affected by TDI with unmet treatment needs are at greater risk of suffering impacts on OHRQoL in the form of OIDP. | Department of Clinical Dentistry and the Centre for International Health, University of Bergen. |
| Basavaraj et al. (2014) [28] | India | 12 and 15 years | Child-OIDP | WHO | Yes | Impacts on eating were the most prevalent (45.3%). The prevalence of impacts on cleaning teeth (42.3%) and smiling (40.1%) were also relatively high. There is a strong association between clinical dental indicators and oral impacts in children. | None. |
| Cortes et al. (2002) [35] | Brazil | 12–14 years | OIDP | O’Brien | Yes | The prevalence of oral impacts, measured by the OIDP index, was higher for children with untreated fractured teeth than for children with non-fractured teeth. For both groups of children, the most prevalent OIDP impact was ‘smiling, laughing, and showing teeth without embarrassment’, with the proportion being higher for cases (55.9%) than for controls (13.2%). | Grant from Conselho Nacional de Pesquisa (CNPq). |
| Ramos-Jorge et al. (2007) [36] | Brazil | 12–14 years | OIDP | O’Brien | Yes | The impact prevalence was greater in the case group for nearly all the appraised activities. In the previous six months, 40% of the teenagers with a history of treatment for enamel dentin fractures had at least one negatively affected daily activity, and 16.9% of the teenagers without a history of trauma were found to have some oral impact on their daily lives. The most affected activities in decreasing order were showing teeth when smiling, eating, speaking, maintaining a stable emotional state, and cleaning the mouth. Sleeping, doing school tasks, practicing sports, and going out with friends were all mentioned as activities that no adolescent reported as having an impact. Adolescents with aesthetically-treated enamel dentin fractures were more likely than those who had never experienced dental trauma to present oral impact on daily activities. Treatment for coronary fractures does not completely eradicate the impact of trauma on the adolescents daily lives, but it does help to mitigate it. | Not stated. |
| Author/Year | Value of Each Domain | Results | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Diaz et al. (2018) [21] | P-CPQ | Mean | SD | Range | Significant association (p < 0.05) between oral symptoms and mother’s education and family income; emotional wellbeing domain and dental caries experience; social wellbeing domain and children’s education, number of siblings; total PCPQ and members in family and dental caries. Children from public schools and children who had dental caries experience (RR = 1.28; p = 0.04 and RR = 1.37; p = 0.018, respectively) had a negative impact on total PCPQ scores. Public school-going children were more likely to experience negative impact on the emotional wellbeing and social wellbeing domains (p < 0.05). Children whose mothers had an educational level < 10 years and children who had dental caries experience showed positive and negative impact on the oral symptoms domain, respectively (RR = 0.75, p = 0.02 and RR = 1.22, p = 0.04, respectively). | |||||||
| OS | 3.88 | 3.5 | 0–20 | |||||||||
| FL | 3.43 | 4.17 | 0–24 | |||||||||
| EWB | 2.09 | 3.90 | 0–30 | |||||||||
| SWB | 3.09 | 6.15 | 0–48 | |||||||||
| Total score | 12.49 | 14.04 | 0–90 | |||||||||
| Antunes et al. (2012) [37] | B-P-CPQ | A1 | A2 | The group of trauma affecting both dental and support tissue had the highest levels of impact (A1) and the greatest reduction in impact following therapy (A2). Positive reduction after receiving the treatment over time was observed for all types of TDI, indicating that 100% of the population benefitted from trauma treatment. Post-treatment oral symptoms did positively affect the OHRQoL. However, out of all the domain scores, oral symptoms had the lowest impact on OHRQoL. The FL domain had the highest impact on OHRQoL. The functional limitations drastically improved the OHRQoL. The EWB and SWB positively improved the OHRQoL after treatment. Overall post-treatment of TDI significantly improved the OHRQoL. Out of all four domains tested, EWB and FL improved and resulted in the highest impact on OHRQoL. | ||||||||
| p-value < 0.01 | Mean (SD) | Median | Mean (SD) | Median | ||||||||
| OS(0–24) | 3.36 (3.11) | 3.00 | 0.05 (0.31) | 0.00 | ||||||||
| FL(0–32) | 9.83 (6.50) | 9.50 | 1.38 (2.78) | 0.00 | ||||||||
| EWB(0–28) | 9.12 (6.60) | 10.00 | 0.17 (0.70) | 0.00 | ||||||||
| SWB(0–40) | 7.74 (6.41) | 7.00 | 1.07 (1.63) | 0.00 | ||||||||
| Total(0–124) | 30.05 (17.39) | 27.50 | 2.67 (4.02) | 2.00 | ||||||||
| Magno et al. (2019) [38] | CPQ(8–10) | BT | AT | p-value | OS domain: CPQ(8–10): There was significant improvement in oral symptoms after treatment. CPQ(11–14): This observation was not statistically significant. This implied that for children between 11–14 years, oral symptoms perception did not affect the OHRQoL. Overall assessment: This indicated that overall parents perception on OHRQoL in the oral symptom domain improved after the child received the treatment. FL domain: The FL domain score for all three questionnaires did not show significant difference in domain score (p > 0.05). This result signifies that functional limitations before and post treatment, both in children and parent perception, did not statistically or significantly impact the OHRQoL. EWB domain: For CPQ(8–10), there was no impact on emotional well-being. CPQ(11–14) scores implied that EWB improved post treatment and had positive impact on OHRQoL in children between the age group of 11–14 years. p-CPQ scores indicated no significant difference. SWB domain: The CPQ(8–10), CPQ(11–14), and P-CPQ scores indicated that there was no statistical significant difference in score in all three groups. This indicated that SWB did not statistically impact the OHRQoL. The cumulative scores of all domains indicated that there was significant improvement in OHRQoL for CPQ(8–10), CPQ(9–14), and P-CPQ after receiving the treatment of TDI. Familiar Impact Scale (FIS) scores: TDI among children involving enamel and dentine fracture did not impact family perspective. | |||||||
| OS | 5.3 (3.4) | 2.7 (2.9) | 0.0003 b | |||||||||
| FL | 2.6 (3.5) | 1.7 (2.0) | 0.4498 b | |||||||||
| EWB | 1.1 (2.8) | 0.3 (0.7) | 0.4990 b | |||||||||
| SWB | 2.8 (3.5) | 1.5 (1.1) | 0.0843 b | |||||||||
| TOTAL | 10.8 (10.0) | 6.5 (4.5) | 0.0065 b | |||||||||
| CPQ(11–14) | ||||||||||||
| OS | 3.2 (2.6) | 2.4 (1.8) | 0.37 a | |||||||||
| FL | 2.0 (1.6) | 1.2 (1.6) | 0.2049 b | |||||||||
| EWB | 1.1 (1.6) | 0.0 (0.0) | 0.0431 b | |||||||||
| SWB | 2.5 (3.5) | 1.3 (1.7) | 0.1083 b | |||||||||
| TOTAL | 8.8 (5.4) | 5.4 (2.7) | 0.0486 a | |||||||||
| P-CPQ | ||||||||||||
| OS | 4.5 (3.2) | 3.6 (2.9) | 0.0455 b | |||||||||
| FL | 5.4 (4.4) | 3.9 (3.5) | 0.1213 b | |||||||||
| EWB | 5.4 (6.5) | 3.5 (6.6) | 0.0534 b | |||||||||
| SWB | 5.4 (4.9) | 4.7 (6.5) | 0.1482 b | |||||||||
| TOTAL | 20.7 (14.1) | 15.7 (16.6) | 0.0259 b | |||||||||
| FIS | ||||||||||||
| PE | 5.1 (4.6) | 5.7 (5.3) | 0.8456 | |||||||||
| FC | 1.7 (2.2) | 1.3 (2.3) | 0.2805 | |||||||||
| FA | 1.2 (1.8) | 1.0 (1.8) | 0.1823 | |||||||||
| TOTAL | 7.9 (7.4) | 8.0 (7.9) | 0.5850 | |||||||||
| Berger et al. (2009) [40] | n | CPQ(8–10) | PPQ(8–10) | FIS | 6 months: After receiving the treatment, the post6-month follow up of the COHRQoL score was improved in all domains. However, the parental COHRQoL scores were dependent upon the initial COHRQoL scores at p = 0.03 (ANCOVA), but the patient scores were not dependent upon the initial score at p = 0.12 (ANCOVA). The PPQ was statistically significant when compared with baseline values. 12 months: The parental 12-month results indicated that scores were dependent upon the initial scores (p = 0.001, ANCOVA). The child 12-month results (CPQ8–10, CPQ11–14) were also dependent upon the baseline COHRQoL scores (p = 0.005, ANCOVA). At 12 months, both age groups of children/adolescents reported lasting effects in each of the four CPQ domains, but their parents only saw lasting effects in two domains (oral symptoms and functional limitations), and they did not offer a single response in the emotional and social well-being domains for both age groups. One year after the injury, the parents of 11–14 year-old patients noticed a significant ongoing effect on their personal QoL. The high initial parental PPQ scores suggest that TDI has a significant impact on the parents’ QoL. FIS: There was no significant differences between the FIS scores for the 8–10 years and 11–14 years age group across all time periods. The initial high parental FIS scores suggest that TDI has a significant impact on the parents’ QoL. Parents of the older children perceived their child’s pain as being greater than the pain reported by the patient, and younger children perceived the initial injury as more painful than the older group. | |||||||
| Initial | 11 | 31.2 (13.3) | 34.8 (18.6) | 13.1 (6.4) | ||||||||
| 6 months | 10 | 20.6 (14.8) | 20.6 (21.8) | 9.7 (8.2) | ||||||||
| 12 months | 8 | 17.5 (12.3) | 15.9 (12.0) | 7.6 (6.1) | ||||||||
| n | CPQ11–14 | PPQ11–14 | FIS | |||||||||
| Initial | 12 | 29.3 (10.9) | 38.8 (22.6) | 9.8 (6.9) | ||||||||
| 6 months | 11 | 19.8 (12.2) | 28.0 (17.7) | 7.6 (5.6) | ||||||||
| 12 months | 9 | 16.7 (9.3) | 27.4 (18.3) | 7.2 (6.0) | ||||||||
| Martins et al. (2018) [22] | Variables Mean (SD) p-value < 0.001 | OS | FL | EWB | SWB | TOTAL | OS domain: TDI showed no statistical significant difference with the group that had no oral condition. However, dental caries associated with TDI had a high negative impact on OHRQoL. FL domain: The dental caries children scores were statistically significant with children with TDI at p = 0.001. EWB domain: In this domain, TDI had no significant impact on OHRQoL. SWB: In this domain, TDI had no significant impact on OHRQoL. Children who presented with dental caries associated with TDI were more likely to experience a high negative impact on their OHRQoL, as shown by the total score, than those without any oral condition. The presence of dental caries and its association with TDI were significantly associated with all CPQ(8–10) subscales at p < 0.05. | |||||
| No conditions | 3.84 (3.07) | 1.87 (2.72) | 3.15 (4.08) | 2.89 (4.63) | 11.61 (11.88) | |||||||
| Dental caries | 5.31(3.52) | 3.02 (3.59) | 4.82 (4.55) | 4.36 (5.42) | 17.50 (14.31) | |||||||
| Malocclusion | 4.14 (3.40) | 2.37(3.02) | 4.83(4.83) | 4.18 (6.03) | 15.49 (14.54) | |||||||
| TDI | 3.91(3.16) | 1.53(2.13) | 3.39 (4.14) | 3.06 (4.20) | 12.03 (11.52) | |||||||
| Freire-Maia et al. (2015) [23] | Domain | OR | 95% | p | Effect of Gender on OHRQL: Girls had a 1.46-fold greater chance of presenting with a negative impact on OHRQoL. Effect of trauma status on OHRQoL: Children with severe dental trauma reported a more negative impact on OHRQoL than children with dental caries and malocclusion involving increased anterior overjet. Effect of individual domain score of TDI on OHRQOL: Severe trauma was significantly associated with a negative impact on overall quality of life (55.9%). Trauma did not significantly affect the OS and FL domain, but SWB and EWB egatively affected the OHRQOL in the bivariate analyses. | |||||||
| OS | 2.67 | 1.31–5.46 | 0.005 | |||||||||
| SWB | 2.93 | 1.46–5.90 | 0.002 | |||||||||
| EWB | 2.61 | 1.31–5.20 | 0.005 | |||||||||
| Sardenberg et al. (2017) [24] | CPQ8–10 Subscales | Number of items | Mean (S.D.) | Possible range | Observed range | Effect of gender on OHRQoL: OHRQoL was significantly associated (p < 0.05) with sex. The CPQ(8–10) score was 1.38 times (95% CI: 1.17–1.63; p < 0.001) higher among girls than boys. This signified that there was a more negative impact on OHRQoL among girls when compared to boys. Socioeconomic status and education level of parents: Negative impact on children’s OHRQoL was significantly associated with a lower parent’s/ guardian’s schooling and lower family income. Effect of TDI and orofacial dysfunction on OHRQoL: A significant negative impact on OHRQoL associated with a history of TDI (RR: 1.39; 95% CI: 1.15–1.69) and orofacial dysfunction (RR: 1.62; 95% CI: 1.30–2.02) was seen. Effect of access to dental care: The children who reported difficulty in having access to dental care and only sought dental care due to pain or factors other than prevention (RR: 1.41; 95% CI: 1.18–1.68) were more likely to experience a negative impact on OHRQoL. | ||||||
| OS | 5 | 5.15 (3.64) | 0–20 | 0–19 | ||||||||
| FL | 5 | 2.84 (3.52) | 0–20 | 0–18 | ||||||||
| EWB | 5 | 3.51 (4.47) | 0–20 | 0–20 | ||||||||
| SWB | 10 | 2.45 (4.50) | 0–40 | 0–28 | ||||||||
| Overall | 25 | 13.95 (13.12) | 0–100 | 0–76 | ||||||||
| Silva-Oliveira et al. (2018) [25] | Subscale | Mean | Independent variable | TDI present n (%) | p-value | Effect of gender on OHRQoL: There was no association between TDI and gender. Impact of TDI alone on OHRQoL: There were statistically significant values indicating that TDI was associated with a high impact on OHRQoL (OR = 1.61 (95% CI: 1.08–2.39)) in children. Effect of mother’s education on OHRQoL: Mother’s educational level was not related to TDI and did not affect the OHRQoL in children. Effect of socioeconomic status on TDI: Monthly household income was not related to TDI and did not affect the OHRQoL in children. Effect of type of school on OHRQoL: The type of school was not related to TDI and did not affect the OHRQoL in children. TDI was significantly associated with the results of social and emotional well-being subscales. Overall, TDI exerted a negative impact on the OHRQoL of the adolescents analyzed. | ||||||
| OS | 2.65 | Low impact High impact | 65 (27.0) 108 (31.1) | 0.277 | ||||||||
| FL | 1.70 | Low impact High impact | 74 (26.8) 99 (31.7) | 0.191 | ||||||||
| EWB | 1.66 | Low impact High impact | 77 (24.6) 96 (34.9) | 0.006 | ||||||||
| SWB | 1.27 | Low impact High impact | 47 (20.2) 126 (35.5) | <0.001 | ||||||||
| TOTAL | 12.54 | Low impact High impact | 69 (24.2) 107 (35.3) | 0.003 | ||||||||
| Rajab et al. (2019) [26] | Domain | Mean (S.D.) | Range Observed | Socioeconomic status: The results of simple logistic regression showed that social class had no significant impact on overall QoL. Effect of gender: Gender had no significant impact on overall QoL. There was a significant impact of untreated TDI on overall OHRQoL. The impact of oral health of the study sample on QoL was much greater on OS and EWB than FL and SWB. Children with untreated TDI in this study risked a higher negative impact on their daily living than those without TDI. Children with untreated TDI had significant poorer overall OHRQoL than those with treated injured teeth and those without trauma. The results of the present study confirmed the negative impact of untreated TDI on QoL of schoolchildren. | ||||||||
| OS | 4.45 (3.25) | 0.00–16.00 | ||||||||||
| FL | 2.91 (3.13) | 0.00–16.00 | ||||||||||
| EWB | 3.54 (3.73) | 0.00–16.00 | ||||||||||
| SWB | 2.37 (3.09) | 0.00–15.00 | ||||||||||
| TOTAL | 13.27 (11.41) | 0.00–55.00 | ||||||||||
| Bendo et al. (2010) [15] | Domain | Untreated TDI | Absence of TDI | Unadjusted PR (95% CI) | p-value †- Chi square test ‡-Fisher’s test | There were no statistically significant differences between children with untreated TDI and those without TDI in terms of the overall CPQ(11–14) scores. There was no association between the overall CPQ11–14—ISF:16 score (Fisher = 0.610) in children with treated fractures and those without TDI. | ||||||
| OS | ||||||||||||
| Pain CPQ11–14 = 0 CPQ11–14 ≥1 | 81 (37.0) 138 (63.0) | 541 (40.5) 796 (59.5) | 1 1.1 (0.8–1.5) | 0.330 | ||||||||
| Mouth sores CPQ11–14 = 0 CPQ11–14 ≥1 | 85 (38.8) 134 (61.2) | 475 (35.5) 862 (64.5) | 1 0.8 (0.6–1.1) | 0.348 † | ||||||||
| FL | ||||||||||||
| Difficulty chewing CPQ11–14 = 0 CPQ11–14 ≥1 | 128 (58.4) 91 (41.6) | 772 (57.7) 565 (42.3) | 1 0.9 (0.7–1.3) | 0.844 † | ||||||||
| Difficulty eating/drinking hot/cold foods CPQ11–14 = 0 CPQ11–14 ≥1 | 84 (38.4) 135 (61.6) | 455 (34.0) 882 (66.0) | 1 0.8 (0.6–1.1) | 0.212 † | ||||||||
| EWB | ||||||||||||
| Felt irritable/frustrated CPQ11–14 = 0 CPQ11–14 ≥1 | 138 (63.0) 81 (37.0) | 827 (61.9) 510 (38.1) | 1 0.9 (0.7–1.2) | 0.743 † | ||||||||
| Upset CPQ11–14 = 0 CPQ11–14 ≥1 | 118 (53.9) 101 (46.1) | 795 (59.5) 542 (40.5) | 1 1.2 (0.9–1.6) | 0.120 † | ||||||||
| Concerned with what others think CPQ11–14 = 0 CPQ11–14 ≥1 | 107 (48.9) 112 (51.1) | 548 (41.0) 789 (59.0) | 1 0.7 (0.5–0.9) | 0.029 † | ||||||||
| SWB | ||||||||||||
| Avoided smiling/laughing CPQ11–14 = 0 CPQ11–14 ≥1 | 141 (64.4) 78 (35.6) | 939 (70.2) 398 (29.8) | 1 1.2 (0.9–1.7) | 0.082 † | ||||||||
| Teased/called names CPQ11–14 = 0 CPQ11–14 ≥1 | 151 (68.9) 68 (31.1) | 913 (68.3) 424 (31.7) | 1 0.9 (0.7–1.3) | 0.845 † | ||||||||
| Other children asked questions CPQ11–14 = 0 CPQ11–14 ≥1 | 125 (57.1) 94 (42.9) | 832 (62.2) 505 (37.8) | 1 1.2 (0.9–1.6) | 0.146 † | ||||||||
| Overall CPQ11–14 = 0 CPQ11–14 ≥1 | 5 (2.3) 214 (97.7) | 19 (1.4) 1318 (98.6) | 0.6 (0.2–1.6) | 0.368 ‡ | ||||||||
| Domain | Treated TDI | Unadjusted PR (95% CI) | p-value | |||||||||
| OS | ||||||||||||
| Pain CPQ11–14 = 0 CPQ11–14 ≥1 | 20 (31.2) 44 (68.8) | 1 1.4 (0.8–2.5) | 0.142 † | |||||||||
| Mouth sores CPQ11–14 = 0 CPQ11–14 ≥1 | 23 (35.9) 41 (64.1) | 1 0.9 (0.5–1.6) | 0.947 † | |||||||||
| FL | ||||||||||||
| Difficulty chewing CPQ11–14 = 0 CPQ11–14 ≥1 | 32 (50.0) 32 (50.0) | 1 1.3 (0.8–2.2) | 0.221 † | |||||||||
| Difficulty eating/drinking hot/cold foods CPQ11–14 = 0 CPQ11–14 ≥1 | 25 (39.1) 39 (60.9) | 1 0.8 (0.4–1.3) | 0.407 † | |||||||||
| EWB | ||||||||||||
| Felt irritable/frustrated CPQ11–14 = 0 CPQ11–14 ≥1 | 43 (67.2) 21 (32.8) | 1 0.7 (0.4–1.3) | 0.390 † | |||||||||
| Upset CPQ11–14 = 0 CPQ11–14 ≥1 | 41 (64.1) 23 (35.9) | 1 0.8 (0.4–1.3) | 0.464 † | |||||||||
| Concerned with what others think CPQ11–14 = 0 CPQ11–14 ≥1 | 28 (43.8) 36 (56.2) | 1 0.8 (0.5–1.4) | 0.661 † | |||||||||
| SWB | ||||||||||||
| Avoided smiling/laughing CPQ11–14 = 0 CPQ11–14 ≥1 | 45 (70.3) 19 (29.7) | 1 0.9 (0.5–1.7) | 0.989 † | |||||||||
| Teased/called names CPQ11–14 = 0 CPQ11–14 ≥1 | 48 (75.0) 16 (25.0) | 1 0.7 (0.4–1.2) | 0.258 † | |||||||||
| Other children asked questions CPQ11–14 = 0 CPQ11–14 ≥1 | 31 (48.4) 33 (51.6) | 1 1.5 (1.1–2.8) | 0.027 † | |||||||||
| Overall CPQ11–14 = 0 CPQ11–14 ≥1 | 1 (1.6) 63 (98.4) | 1 0.9 (0.1–6.8) | 0.610 ‡ | |||||||||
| Bendo et al. (2014) (1) [31] | Variables | Case | Control | Unadjusted OR (95% CI) | p-value | Effect of gender on OHRQoL: Gender did not affect the OHRQoL. Effect of age on OHRQoL: Age was not associated with impact on adolescents’ OHRQoL. Effect of type of school: Type of school had no impact on TDI. Effect of type of dental trauma on OHRQoL: There was strong association between more severe TDI (fractures involving dentin and/or pulp) and poorer OHRQoL among adolescents. However, mild TDI (enamel fractures only) and restored fractures were not associated with negative impact on OHRQoL. Overall effect of TDI using the CPQ tool on OHRQoL: The overall CPQ(11–14) showed that TDI appeared to affect an adolescent’s OHRQoL. There is a strong association between the severity of TDI and OHRQoL. | ||||||
| Traumatic dental injuries | ||||||||||||
| Without injuries | 340 (84.0) | 694 (85.7) | 1.00 | |||||||||
| Restored fracture | 20 (4.9) | 25 (3.1) | 1.63 (0.89–2.98) | 0.110 | ||||||||
| Enamel fracture only | 23 (5.7) | 73 (9.0) | 0.64 (0.40–1.05) | 0.075 | ||||||||
| Fracture involving dentin/pulp | 22 (5.4) | 18 (2.2) | 2.50 (1.32–4.71) | 0.005 | ||||||||
| Porrit et al. (2011) [41] | Domain | N | Baseline mean (SD) | Follow-up mean (SD) | Wilcoxon test Z± | Sig change | Effect of gender on OHRQoL: Gender was found to be a significant predictor of children’s OHRQoL. The results revealed that girls were more likely to report impacts on their OHRQoL (F (1) = 6.58, p < 0.05) than boys. Effect of age on OHRQoL: There were no significant interaction effects between gender and age or age when sustained injury or deprivation. 6-month follow-up: At the 6-month follow up, school functioning and functional limitations remained the areas of children’s OHRQoL that had the most impacts. A total of 62.9% of children reported improvement in their OHRQoL, whereas 30% of children had a negative impact, and 7.1% had no impact on OHRQoL at the 6-month follow up. Children with high levels of OHRQoL at baseline were more likely to report high levels of OHRQoL at follow up. Effect of individual domain on OHRQoL: With respect to OHRQoL, children were most likely to report difficulties related to OS, FL, and EWB domains. Social impacts remained the least affected area, within the child’s OHRQoL, at the 6-month follow up. | |||||
| Overall | 70 | |||||||||||
| OS | 70 | 4.2 (3.0) | 3.0 (2.5) | Z = −3.13 ** | ↑ | |||||||
| FL | 70 | 4.3 (3.6) | 3.2 (3.1) | Z = −3.18 ** | ↑ | |||||||
| Emotional impacts | 70 | 3.8 (3.9) | 2.9 (3.2) | Z = −2.22 * | ↑ | |||||||
| Social impacts | 70 | 3.2 (3.4) | 2.9 (2.8) | Z = −1.03 | ↔ | |||||||
| Traebert et al. (2012) [43] | Mean CPQ11–14 (SD) | OS: Significant association was observed between TDI and OS domain at p-value 0.036. FL: Significant association was observed between TDI and FL domain at p-value 0.013. EWB: Significant association was observed between TDI and EWB domain at p-value 0.030. Overall score: There were significant associations between the prevalence of one or more adverse impacts occurring often/very often through the overall CPQ11–14 scale and TDI (p = 0.007). A prevalence ratio of 1.79 (95% CI 1.16–2.76) of one or more adverse impacts occurring often/very often in schoolchildren with TDI was found, compared to those without TDI. TDI has a strong association with appearing to affect school children’s OHRQoL. | ||||||||||
| Overall | OS | FL | EW | SW | 95% CI | |||||||
| Schoolchildren with TDI | 14.6 (8.6) | 4.7 (2.3) | 3.4 (3.0) | 3.7 (3.1) | 2.8 (2.7) | 62.1 (50.4–73.8) ** | ||||||
| Schoolchildren without TDI | 9.6 (7.5) | 3.8 (2.4) | 2.3 (2.4) | 1.8 (2.5) | 1.7 (2.1) | 44.0 (38.7–49.3) | ||||||
| p-value | 0.019 * | 0.026 * | 0.016 * | 0.031 * | 0.869 * | 0.019 ** | ||||||
| All children | 12.4 (9.2) | 4.1 (2.6) | 2.8 (2.9) | 3.4 (3.5) | 2.1 (2.5) | 46.5 (41.6–51.4) | ||||||
| Dame-Texeira et al. (2013) [27] | Domain | No TDI/No treatment | Treated | Treatment need | Total | Effect of gender on OHRQoL: There was significant association. Effect of socioeconomic status on OHRQoL: There was significant association. Effect of individual domain on OHRQoL: OS: The OS domain was not associated with TDI. This indicated that TDI did not affect the OHRQoL. FL: The FL domain was significantly associated with TDI with treatment needs, whereas no association was observed with treated TDI. EWB: The EWB domain was not associated with TDI. This indicated that TDI did not affect the OHRQoL. SWB: The SWB domain was not associated with TDI. This indicated that TDI did not affect the OHRQoL. Overall score: Individuals presenting TDI with treatment needs experienced a higher average CPQ11–14 score than individuals with no TDI or with TDI without treatment needs (RR = 1.2; 95% CI = 1.0–1.4). The overall CPQ11–14 score was not associated with TDI. This indicated that TDI did not affect the OHRQoL. | ||||||
| Mean (95% CI) | Mean (95% CI) | p-value | Mean (95% CI) | p-value | ||||||||
| OS | 4.15 (3.74–4.56) | 4.48 (3.58–5.37) | 0.198 | 4.44 (3.65–5.23) | 0.183 | 4.18 (3.77–4.59) | ||||||
| FL | 2.96(2.64–3.29) | 3.39 (2.03–4.76) | 0.385 | 3.63 (3.11–4.16) | 0.132 | 3.02 (2.70–3.35) | ||||||
| EWB | 2.90 (2.48–3.31) | 2.79 (1.89–3.69) | 0.714 | 2.81 (1.94–3.69) | 0.771 | 2.89 (2.49–3.28) | ||||||
| SWB | 2.33 (1.98–2.69) | 2.03 (1.43–2.64) | 0.427 | 2.84 (2.11–3.56) | 0.210 | 2.36 (2.03–2.68) | ||||||
| Overall CPQ11–14 | 12.35 (10.98–13.72) | 12.70 (10.58–14.83) | 0.652 | 13.74 (11.70–15.78) | 0.476 | 12.46 (11.21–13.72) | ||||||
| Antunes et al. (2013) [32] | CPQ11–14 Domain | Case Group Mean ± SD | Control group Mean ± SD | p-value | Effect of individual domain on OHRQoL: OS: There was a statistically significant difference between the case and control group. This indicated that children with TDI had a negative impact on OHRQoL. FL: Children with TDI had a negative impact on OHRQoL. EWB: Children with TDI had a negative impact on OHRQoL. SWB: Children with TDI had a negative impact on OHRQoL. Overall score: Children with TDI had a negative impact on OHRQoL. Children and adolescents with a traumatic dental injury were more likely to have a greater impact on their life than those with no injuries. | |||||||
| OS | 3.82 ± 2.60 | 1.30 ± 2.02 | <0.01 | |||||||||
| FL | 5.29 ± 4.03 | 1.33 ± 1.94 | <0.01 | |||||||||
| EWB | 5.00 ± 6.34 | 0.24 ± 1.22 | <0.01 | |||||||||
| SWB | 3.47 ± 4.36 | 0.21 ± 0.59 | <0.01 | |||||||||
| TOTAL | 17.59 ± 14.01 | 3.09 ± 4.42 | <0.01 | |||||||||
| Locker et al. (2007) [42] | Clinical indicator | Mean CPQ11–14 score | p-value | Associations were significant for all variables except school grade and mother’s educational attainment. Both variables denoting the socioeconomic status of the household in which the child participants lived (annual household income, receipt of government income support) indicated that children from lower-income households had the highest CPQ11–14 short form scores. In the higher income group, there were no differences in CPQ11–14 scores for children with or without severe injury to the anterior dentition. However, the differences were significant for children in the lower-income group. Children from low-income households had higher scores on a short form of the CPQ11–14 than children from high-income households, indicating poorer oral health-related quality of life. | ||||||||
| Incisors with DTI codes 1–5 | ||||||||||||
| None | 12.7 | NS | ||||||||||
| One | 13.4 | |||||||||||
| Two or more | 13.7 | |||||||||||
| Incisors with DTI codes 2–5 | ||||||||||||
| None | 12.7 | <0.001 | ||||||||||
| One | 13.6 | |||||||||||
| Two or more | 16.4 | |||||||||||
| Fakhruddin et al. (2008) [33] | Dimensions and items | Case (n = 92) | Control (n = 92) | Unadjusted odds ratio ** (95% CI) | Adjusted odds ratio ** (95% CI) | |||||||
| Untreated dental injury n (%) | No dental injury n (%) | |||||||||||
| OS | ||||||||||||
| Pain CPQ11–14 = 0 CPQ11–14 = 1 | 54 (58.7) 38 (41.3) | 59 (64.1) 33 (35.9) | 1.31 (0.68–2.52) | 1.54 (0.71–3.36) | ||||||||
| FL | ||||||||||||
| Sleep disturbances CPQ11–14 = 0 CPQ11–14 = 1 | 86 (93.5) 6 (6.5) | 84 (91.3) 8 (8.7) | 0.75 (0.26–2.16) | 1.29 (0.39–4.16) | ||||||||
| Chewing difficulty CPQ11–14 = 0 CPQ11–14 = 1 | 59 (64.1) 33 (35.9) | 70 (76.1) 22 (23.9) | 2.00 (0.97–4.12) | 2.86 (1.13–7.26) * | ||||||||
| EWB | ||||||||||||
| Shy or embarrassed CPQ11–14 = 0 CPQ11–14 = 1 | 72 (78.3) 20 (21.7) | 76 (82.6) 16 (17.4) | 1.27 (0.64–2.49) | 1.71 (0.78–3.75) | ||||||||
| Concerned with what others think CPQ11–14 = 0 CPQ11–14 = 1 | 63 (68.5) 29 (31.5) | 76 (82.6) 16 (17.4) | 2.00 (1.03–3.89) * | 2.07 (0.96–4.47) | ||||||||
| SWB | ||||||||||||
| Low concentration in school CPQ11–14 = 0 CPQ11–14 = 1 | 79 (85.9) 13 (14.1) | 82 (90.1) 9 (9.9) | 1.50 (0.61–3.67) | 1.80 (0.67–4.87) | ||||||||
| Avoid smiling/laughing CPQ11–14 = 0 CPQ11–14 = 1 | 72 (78.3) 20 (21.7) | 83 (90.2) 9 (9.8) | 2.38 (1.04–5.43) * | 3.09 (1.12–8.50) * | ||||||||
| Did not want to talk to other children CPQ11–14 = 0 CPQ11–14 = 1 | 79 (85.9) 13 (14.1) | 88 (95.7) 4 (4.3) | 3.25 (1.06–9.97) * | 3.84 (1.12–13.18) * | ||||||||
| Did not want to spend time with other children CPQ11–14 = 0 CPQ11–14 = 1 | 85 (92.4) 7 (7.6) | 90 (97.8) 1 2 (2.2) | 3.50 (0.73–16.84) | 5.12 (0.85–30.76) | ||||||||
| Teased by other children CPQ11–14 = 0 CPQ11–14 = 1 | 79 (85.9) 13 (14.1) | 85 (92.4) 7 (7.6) | 1.86 (0.74–4.65) | 2.19 (0.78–6.18) | ||||||||
| Overall CPQ11–14 CPQ11–14 = 0 CPQ11–14 = 1 | 33 (35.9) 59 (64.1) | 44 (47.8) 48 (52.2) | 1.58 (0.89–2.81) | 1.80 (0.93–3.48) | ||||||||
| Dimensions and items | Case (n = 43) | Control (n = 43) | Unadjusted odds ratio ** (95% CI) | Adjusted odds ratio ** (95% CI) | ||||||||
| Restored injury n (%) | No dental injury n (%) | |||||||||||
| OS | ||||||||||||
| Pain CPQ11–14 = 0 CPQ11–14 = 1 | 24 (55.8) 19 (44.2) | 24 (55.8) 19 (44.2) | 1.00 (0.42–2.40) | 1.17 (0.40–3.43) | ||||||||
| FL | ||||||||||||
| Sleep disturbances CPQ11–14 = 0 CPQ11–14 = 1 | 41 (95.3) 2 (4.7) | 37 (86.0) 6 (14.0) | 0.33 (0.07–1.65) | 0.16 (0.02–1.32) | ||||||||
| Chewing difficulty CPQ11–14 = 0 CPQ11–14 = 1 | 27 (62.8) 16 (37.2) | 35 (81.4) 8 (18.6) | 2.60 (0.93–7.29) | 4.16 (1.08–16.12) * | ||||||||
| EWB | ||||||||||||
| Shy or embarrassed CPQ11–14 = 0 CPQ11–14 = 1 | 31 (72.1) 12 (27.9) | 35 (81.4) 8 (18.6) | 2.33 (0.60–9.02) | 2.14 (0.37–12.31) | ||||||||
| Concerned with what others think CPQ11–14 = 0 CPQ11–14 = 1 | 32 (74.4) 11 (25.6) | 34 (79.1) 9 (20.9) | 1.40 (0.44–4.41) | 2.01 (0.39–10.29) | ||||||||
| SWB | ||||||||||||
| Low concentration in school CPQ11–14 = 0 CPQ11–14 = 1 | 39 (90.7) 4 (9.3) | 40 (95.2) 2 (4.8) | 2.00 (0.37–10.91) | 1.81 (0.23–14.15) | ||||||||
| Avoid smiling/laughing CPQ11–14 = 0 CPQ11–14 = 1 | 36 (83.7) 7 (16.3) | 39 (90.7) 4 (9.3) | 2.00 (0.50–7.99) | 1.67 (0.26–10.82) | ||||||||
| Did not want to talk to other children CPQ11–14 = 0 CPQ11–14 = 1 | 38 (88.4) 5 (11.6) | 41 (95.3) 2 (4.7) | 2.50 (0.49–12.89) | 1.16 (0.13–10.75) | ||||||||
| Did not want to spend time with other children CPQ11–14 = 0 CPQ11–14 = 1 | 38 (88.4) 5 (11.6) | 41 (95.3) 2 (4.7) | 2.50 (0.49–12.89) | 0.74 (0.09–5.49) ` | ||||||||
| Teased by other children CPQ11–14 = 0 CPQ11–14 = 1 | 38 (88.4) 5 (11.6) | 39 (90.7) 4 (9.3) | 1.33 (0.29–5.96) | 2.54 (0.29–22.33) | ||||||||
| Overall CPQ11–14 CPQ11–14 = 0 CPQ11–14 = 1 | 16 (37.2) 27 (62.8) | 18 (41.9) 25 (58.1) | 1.20 (0.52–2.78) | 1.43 (0.52–3.88) | ||||||||
| Bendo et al. (2014) (2) [29] | Variables | Overall B-FIS Robust RR (95% CI) | Parental/ family activity Robust RR (95% CI) | Parental emotions Robust RR (95% CI) | Family conflict Robust RR (95% CI) | Financial burden Robust RR (95% CI) | Effect of individual domain: Parental/ family activity: Parents/caregivers of adolescents who had suffered a fracture involving the dentine or dentine/pulp had higher scores on the parental/family activity subscale than those whose adolescents were diagnosed with an absence of TDI or enamel fracture alone. Greater social vulnerability had a negative impact on families’ QoL regarding parental/family activity. The severity of the TDI was significantly associated with negative impacts on the parental activity. Parental emotions: Greater social vulnerability had a negative impact on families’ QoL regarding parental emotions. The severity of the TDI was significantly associated with negative impacts on the parental emotion subscale. Family conflict: Greater social vulnerability had a negative impact on families’ QoL regarding the family conflict subscales. The severity of the TDI was significantly associated with negative impacts on the family conflict subscales. Financial burden: There was absence of impact on the financial burden subscale, which reflects the fact that TDI is not considered a disease by most parents. Overall score: Parents/caregivers of adolescents who had suffered a fracture involving the dentine or dentine/pulp had higher scores on overall B-FIS than those whose adolescents were diagnosed with an absence of TDI or enamel fracture alone. Greater social vulnerability had a negative impact on families’ QoL regarding the overall B-FIS. Adolescents with a fracture of dentine or dentine/pulp had a 44%-higher chance of increasing their overall B-FIS score by one point (RR = 1.44; 95%zx CI; 1.10–1.88) than those without TDI. A fracture involving dentin or dentin/pulp was associated with a greater likelihood of a negative impact on family’s QoL. | |||||
| TDI absent | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | |||||||
| Enamel fracture alone | 0.96 (0.77–1.18) | 1.04 (0.82–1.32) | 0.87 (0.67–1.12) | 0.98 (0.73–1.30) | 0.78 (0.52–1.16) | |||||||
| Fracture involving dentine or dentine/pulp | 1.44 (1.10–1.88) ** | 1.45 (1.09–1.94) * | 1.45 (1.03–2.04) * | 1.46 (1.01–2.11) * | 1.26 (0.79–2.00) | |||||||
| Gianenetti et al. (2007) [39] | Age % under 18 years old | 72.27 (73) | Adverse impacts on OHRQoL were reported much more frequently among patients who got into failure of replantation compared with patients who got into successful replantation. If patients got into tooth avulsion, then their quality of life was adversely affected. | |||||||||
| Sex % Male % Female | 63.4 (64) 36.6 (37) | |||||||||||
| Tooth Avulsed % central incisors % lateral incisors % more than one element | 49.5 (50) 13.8 (14) 36.7 (37) | |||||||||||
| Time since last dental visit % visited in last month | 39.6 (40) | |||||||||||
| Bomfim et al. (2017) [30] | Trauma | n | % | CI 95% | ||||||||
| Maxillary | 1344 | 18.56 | 17.68 | 19.47 | Effect of family income on OHRQoL: Income level had no association with TDI. This indicated that family income did not impact the OHRQoL. Effect of parent’s education on OHRQoL: Parents education was not associated with TDI outcome. This indicated that parental education did not impact the OHRQoL. Effect of trauma on OHRQoL: Enamel fractures were risk factors for feelings of shame among children (OR 1.27 and 95%CI: 1:05–1:53) and were significantly associated with embarrassment of smiling, whereas dentine/enamel fractures were risk factors for dissatisfaction with their teeth or for feeling embarrassed of smiling and messing up with the study. This type of TDI was also associated with the unadjusted coefficient used to report difficulty with eating. This indicated that dentin fracture or fractures involving pulp impacted the OHRQoL negatively. Mandibular tooth fractures did not affect the quality of life of 12-year-old Brazilian children. The greater the severity of the TDI, the greater its impact on OHRQoL. TDI causes aesthetic, emotional, and functional problems in patients that might be irreversible in some cases. | |||||||
| Mandibular | 391 | 5.4 | 4.9 | 5.9 | ||||||||
| Enamel | 1378 | 19.03 | 18.1 | 20 | ||||||||
| Dentine | 271 | 3.7 | 3.32 | 4.2 | ||||||||
| Pulp exposition | 22 | 0.3 | 0.2 | 0.4 | ||||||||
| Avulsion | 12 | 0.17 | 0.1 | 0.3 | ||||||||
| Ramos-Jorge et al. (2014) [9] | Variables | Without TDI n (%) | Untreated TDI n (%) | Treated TDI n (%) | p | Effect of mother’s education on OHRQoL: There was a statistically significant difference for mother’s schooling in comparison of schoolchildren without TDI and those with treated TDI. Effect of individual items on OIDP: Children with untreated TDI experienced a greater negative impact on QoL in comparison with those without TDI in eating and enjoying food and smiling and showing teeth. No impact on OIDP was seen in all children in the treated TDI group for cleaning mouth, speaking, sleeping, and relaxing. No impact on OIDP was seen in all children in the no TDI group, untreated TDI, or in treated TDI group in maintaining usual emotional state and carrying out school-related tasks. Enjoying contact with people: Impact on OIDP was seen in 0.2% of children in the without TDI group and no impact on OIDP was seen in all children in the untreated TDI group and treated TDI group. Overall: Children with untreated TDI experienced a greater negative impact on QoL in comparison with those without TDI. | ||||||
| Eating and enjoying food Child-OIDP = 0 Child-OIDP ≥1 | 419 (95.4) 20 (4.6) | 148 (90.2) 16 (9.8) | 59 (90.8) 6 (9.2) | Without vs. Untreated = 0.016 Without vs. Treated = 0.128 | ||||||||
| Cleaning mouth Child-OIDP = 0 Child-OIDP ≥1 | 428 (97.5) 11 (2.5) | 162 (98.8) 2 (1.2) | 65 (100.0) | Without vs. Untreated = 0.530 Without vs. Treated = 0.3742 | ||||||||
| Speaking Child-OIDP = 0 Child-OIDP ≥1 | 434 (98.9) 5 (1.1) | 159 (97.0) 5 (3.0) | 65 (100.0) | Without vs. Untreated = 0.145 Without vs. Treated = 1.000 | ||||||||
| Sleeping and relaxing Child-OIDP = 0 Child-OIDP ≥1 | 435 (99.1) 4 (0.9) | 163 (99.4) 1 (0.6) | 65 (100.0) - | Without vs. Untreated = 1.000 Without vs. Treated = 1.000 | ||||||||
| Smiling and showing teeth Child-OIDP = 0 Child-OIDP ≥1 | 395 (90.0) 44 (10.0) | 130 (79.3) 34 (20.7) | 56 (86.2) 9 (13.8) | Without vs. Untreated < 0.001 Without vs. Treated = 0.348 | ||||||||
| Maintaining usual emotional state Child-OIDP = 0 Child-OIDP ≥1 | 439 (100.0) - | 164 (100.0) - | 65 (100.0) - | * | ||||||||
| Carrying out school-related tasks Child-OIDP = 0 Child-OIDP ≥1 | 439 (100.0) - | 164 (100.0) - | 65 (100.0) - | * | ||||||||
| Enjoying contact with people Child-OIDP = 0 Child-OIDP ≥1 | 438 (99.8) 1 (0.2) | 164 (100.0) - | 65 (100.0) - | Without vs. Untreated = 1.000 Without vs. Treated = 1.000 | ||||||||
| Overall OIDP Child-OIDP = 0 Child-OIDP ≥1 | 364 (82.9) 75 (17.1) | 115 (70.1) 49 (29.9) | 52 (80.0) 13 (20.0) | Without vs. Untreated < 0.001 Without vs. Treated = 0.563 | ||||||||
| Thelen et al. (2011) [34] | Variables | Cases n (%) | Controls n (%) | OR-unadjusted (CI = 95%) | OR-adjusted (CI = 95%) | Effect of individual items on OHRQoL: Eating and enjoying food: A total of 46.3% of cases and 34.2% of controls had an impact on OIDP. Cleaning mouth: A total of 28.4% of cases and 28.4% of controls had an impact on OIDP. Speaking: A total of 3.2% of cases and 8.9% of controls had an impact on OIDP. Sleeping and relaxing: A total of 18.9% of cases and 18.4% of controls had an impact on OIDP. Smiling and showing teeth: A total of 78.9% of cases and 31.6% of controls had an impact on OIDP. This item showed the most prevalent impact on OHRQoL. Statistical significant difference was observed between cases and controls. Maintaining usual emotional state: A total of 31.6% of cases and 20% of controls had an impact on OIDP. A significant difference was found between cases and controls at p-value <0.05. Carrying out school-related tasks: A total of 4.2% cases of and 11.6% of controls had an impact on OIDP. Enjoying contact with people: A total of 66.3% of cases and 23.2% of controls had an impact on OIDP. This item had the second-most prevalent impact, which was significantly more in cases than controls at p-value <0.001. Statistical significant difference was observed between cases and controls. Overall score: The overall impact prevalence of OIDP among cases was significantly higher (88.4%) than for the controls (58.9%) (p < 0.001). There was a significantly greater probability of perceiving an oral impact on daily life among cases than controls. TDI with unmet treatment need in this sample of adolescents was associated with reduced OHRQoL. Compared to adolescents with no history of TDI, those affected by TDI with unmet treatment need were at greater risk of suffering impacts on OHRQoL in the form of OIDP. | ||||||
| Eating and enjoying food OIDP = 0 OIDP ≥1 | 51 (53.7) 44 (46.3) | 125 (65.8) 65 (34.2) | 1 1.7 (1.01–2.78) p < 0.05 | 1 1.01 (0.6–2.1) | ||||||||
| Cleaning your mouth OIDP = 0 OIDP ≥1 | 68 (71.6) 27 (28.4) | 136 (71.6) 54 (28.4) | 1 0.3 (0.08–1.2) | 1 0.2 (0.06–1.1) | ||||||||
| Speaking OIDP = 0 OIDP ≥1 | 92 (96.8) 3 (3.2) | 173 (91.1) 17 (8.9) | 1 1.2 (0.5–1.7) | 1 0.9 (0.5–1.9) | ||||||||
| Sleeping and relaxing OIDP = 0 OIDP ≥1 | 77 (81.1) 18 (18.9) | 155 (81.6) 35 (18.4) | 1 1.1 (0.6–1.9) | 1 0.8 (0.4–1.6) | ||||||||
| Smiling and showing teeth OIDP = 0 OIDP ≥1 | 20 (21.1) 75 (78.9) | 130 (68.4) 60 (31.6) | 1 8.4 (4.2–16.5) p < 0.001 | 1 10.9 (4.5–26.6) p < 0.001 | ||||||||
| Maintaining usual emotional state OIDP = 0 OIDP ≥1 | 65 (68.4) 30 (31.6) | 152 (80.0) 38 (20.0) | 1 1.8 (1.1–3.2) p < 0.05 | 1 1.8 (0.9–3.6) | ||||||||
| Carrying out school related tasks OIDP = 0 OIDP ≥1 | 91 (95.8) 4 (4.2) | 168 (88.4) 22 (11.6) | 1 0.4 (0.1–1.1) | 1 0.5 (0.1–1.8) | ||||||||
| Enjoying contact with people OIDP = 0 OIDP ≥1 | 32 (33.7) 63 (66.3) | 146 (76.8) 44 (23.2) | 1 5.6 (3.2–9.8) p < 0.001 | 1 6.1 (3.1–12.1) p < 0.001 | ||||||||
| Overall OIDP OIDP = 0 OIDP ≥1 | 11 (11.6) 84 (88.4) | 78 (41.1) 112 (58.9) | 1 5 (2.4–10.2) p < 0.001 | 1 3.9 (1.6–9.1) p < 0.05 | ||||||||
| Cortes et al. (2002) [35] | Variable | Cases n (%) | Controls n (%) | OR-unadjusted (CI = 95%) | OR-adjusted (CI = 95%) | Effect of individual item on OHRQoL: Eating and enjoying food: Cases were 13.4 times (95% CI = 3.0–61.0) more likely to report an impact for ‘eating and enjoying food’ than children with no traumatic dental injury. Speaking and pronouncing clearly: This item had the least impact for both case and control groups. Cleaning your mouth: The impact for ‘cleaning teeth’ was statistically and significantly associated with the group of children with untreated fractured teeth. Children with fractured teeth were more likely to report an impact for this item than children without TDI. Smiling, laughing, and showing teeth without embarrassment: The most prevalent OIDP impact was seen in this item for both cases and controls. Children with fractured teeth were more likely to report an impact for this item than children without a TDI. The appearance of untreated fractured teeth was the main factor affecting this OIDP item. Maintaining emotional state without being irritable: The impact of this item on OIDP was statistically significant. Cases were 11.8 times more likely to report an impact for this item than controls. The appearance of untreated fractured teeth was the main factor affecting this OIDP item. Contact with people: There was a statistically significant association between ‘enjoying contact with people’ and the presence of fractured teeth. Cases were 10.0 times more likely to report an impact for the item ‘enjoying contact with people’ when compared to controls. Overall OIDP score: Children with fractured teeth were 20 times more likely to report any impact on their daily living than children with no traumatic dental injury. This shows that children with fractured teeth had significantly higher OIDP scores than those without TDI. | ||||||
| Eating and enjoying your food OIDP = 0 OIDP >0 | 55 (80.9) 13 (19.1) | 134 (98.5) 2 (1.5) | 1 13.0 (2.9–57.6) p < 0.01 | 1 13.4 (3.0–61.0) p < 0.01 | ||||||||
| Speaking and pronouncing clearly OIDP = 0 OIDP >0 | 64 (94.1) 4(5.9) | 135 (99.3) 1 (0.7) | 1 8.0 (0.9–71.6) | 1 8.0 (0.9–75.0) | ||||||||
| Cleaning your mouth OIDP = 0 OIDP >0 | 58 (85.3) 10 (7.14) | 129 (94.9) 7 (5.1) | 1 4.0 (1.2–13.1) p < 0.05 | 1 3.9 (1.2–13.0) p < 0.05 | ||||||||
| Smiling, laughing, and showing our teeth without embarrassment OIDP = 0 OIDP >0 | 30 (44.1) 38 (55.9) | 118 (86.8) 18 (13.2) | 1 8.6 (3.8–19.5) p < 0.001 | 1 15.7 (5.0–44.6) p < 0.001 | ||||||||
| Maintaining your emotional state without being irritatble OIDP = 0 OIDP >0 | 45 (66.2) 23 (33.8) | 129 (94.9) 7 (5.1) | 1 10.4 (3.6–30.3) p < 0.001 | 1 11.8 (3.9–35.5) p < 0.001 | ||||||||
| Contact with people OIDP = 0 OIDP >0 | 58 (85.3) 10 (14.7) | 134 (98.5) 2 (1.5) | 1 10.0 (2.2–45.6) p < 0.01 | 1 10.0 (2.1–47.2) p < 0.001 | ||||||||
| Overall OIDP OIDP = 0 OIDP >0 | 23 (33.8) 45 (66.2) | 116 (85.3) 20 (14.7) | 1 10.2 (4.6–22.8) p < 0.001 | 1 20.0 (7.0–57.7) p < 0.001 | ||||||||
| Basavaraj et al. (2014) [28] | OIDP | Impact score mean (SD) | OR (95% CI) | Effect of gender on oral impact: There was no association between oral impacts and gender. Effect of age on OIDP: There was a significant difference among the age groups, with younger age groups reporting more trauma. Effect of individual item on OIDP: Eating: Children with TDI demonstrated significant impacts on eating (OR = 11.0). Difficulty with eating due to oral problems was the most common impact (72.9%) and led to more severe oral impacts on children’s quality of life than impacts on other performances. Children with TDI demonstrated significant impacts on cleaning teeth (OR = 3.5), emotional status (OR = 10.0), smiling (OR = 15.2), and contact (OR = 13.1). Children with TDI were less likely to have an impact on relaxing (OR = 0.6). Overall impact: Significant association was observed for oral impacts on daily performance with TDI at p-value ≤ 0.05. Overall, 60% of children reported at least one impact on quality of life attributed to oral health in the last three months. | ||||||||
| Overall impacts(%) | 2.49 (3.92) | |||||||||||
| Eating | 1.60 (4.49) | 11.0 (10.7–9.11) p ≤ 0.05 | ||||||||||
| Speaking | 0.10 (0.71) | 7.0 (2.1–55.2) | ||||||||||
| Cleaning teeth | 0.87 (3.07) | 3.5 (2.4–16.2) p ≤ 0.05 | ||||||||||
| Relaxing | 0.39 (2.65) | 0.6 (0.1–0.9) | ||||||||||
| Emotion | 0.61 (2.92) | 10.0 (1.2–18.2) p ≤ 0.05 | ||||||||||
| Smiling | 1.31 (4.22) | 15.2 (11.1–24.2) p ≤ 0.05 | ||||||||||
| Study | 0.06 (0.59) | 0.8 (0.2–1.7) | ||||||||||
| Contact | 0.51 (2.13) | 13.1 (9.4–19.2) p ≤ 0.05 | ||||||||||
| Ramos-Jorge et al. (2007) [36] | Variables | Case group (n%) | Control group (n%) | p | Effect of mother’s education on OHRQoL: There were no statistical significant differences between the case and control group with relation to mother’s education. Adolescents with aesthetically-treated enamel dentin fractures had a greater chance of presenting an oral impact on daily activities than those never having suffered dental trauma (OR 3.26–95% (CI) = 1.4–7.7). The treatment of coronary fractures did not eliminate the impact of trauma on the daily life of the adolescents surveyed, although it possibly reduced such an impact. | |||||||
| Eating OIDP = 0 OIDP ≥1 | 34 (85.0) 6 (15.0) | 153 (95.6) 7 (4.4) | 0.015 C C- chi-square test | |||||||||
| Speaking OIDP = 0 OIDP ≥1 | 38 (95.0) 2 (5.0) | 158 (98.8) 2 (1.2) | 0.179 F F- Fisher’s exact test | |||||||||
| Showing teeth OIDP = 0 OIDP ≥1 | 26 (65.0) 14 (35.0) | 138 (86.3) 22 (13.8) | 0.002 C C- chi-square test | |||||||||
| Maintaining stable emotional state OIDP = 0 OIDP ≥1 | 39 (97.5) 1 (2.5) | 160 (100.0) 0 (0.0) | 0.215 F F- Fisher’s exact test | |||||||||
| Cleaning mouth OIDP = 0 OIDP ≥1 | 40 (100.0) 0 (0.0) | 159 (99.5) 1 (0.5) | 0.215 F | |||||||||
| Total OIDP OIDP = 0 OIDP ≥1 | 24 (60.0) 16 (40.0) | 133 (83.1) 27 (16.9) | 0.001 C | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Das, P.; Mishra, L.; Jena, D.; Govind, S.; Panda, S.; Lapinska, B. Oral Health-Related Quality of Life in Children and Adolescents with a Traumatic Injury of Permanent Teeth and the Impact on Their Families: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 3087. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19053087
Das P, Mishra L, Jena D, Govind S, Panda S, Lapinska B. Oral Health-Related Quality of Life in Children and Adolescents with a Traumatic Injury of Permanent Teeth and the Impact on Their Families: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(5):3087. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19053087
Chicago/Turabian StyleDas, Priyankaa, Lora Mishra, Debkant Jena, Shashirekha Govind, Saurav Panda, and Barbara Lapinska. 2022. "Oral Health-Related Quality of Life in Children and Adolescents with a Traumatic Injury of Permanent Teeth and the Impact on Their Families: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 5: 3087. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19053087