
The Effectiveness and Cost of an Intervention to Increase the Provision of Preventive Care in Community Mental Health Services: Protocol for a Cluster-Randomized Controlled Trial


 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
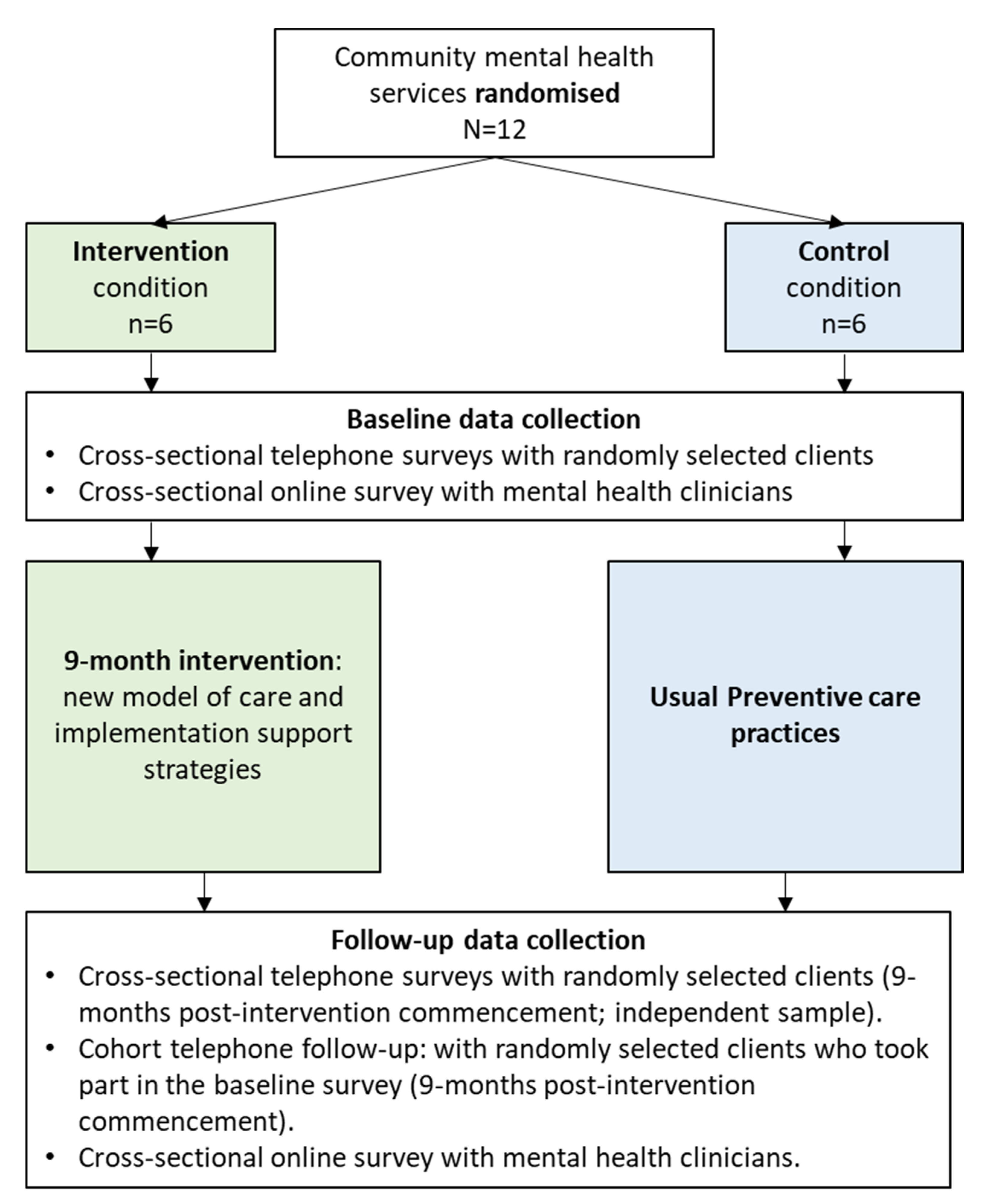
2.1. Study Design and Setting
2.2. Randomisation and Blinding
2.3. Participant Eligibility and Recruitment
2.3.1. Community Mental Health Services
2.3.2. Clients
Cross-Sectional Surveys
Cohort Client Follow-Up (Nested Study)
2.3.3. Mental Health Clinicians
2.4. Intervention
2.4.1. Co-Development Process
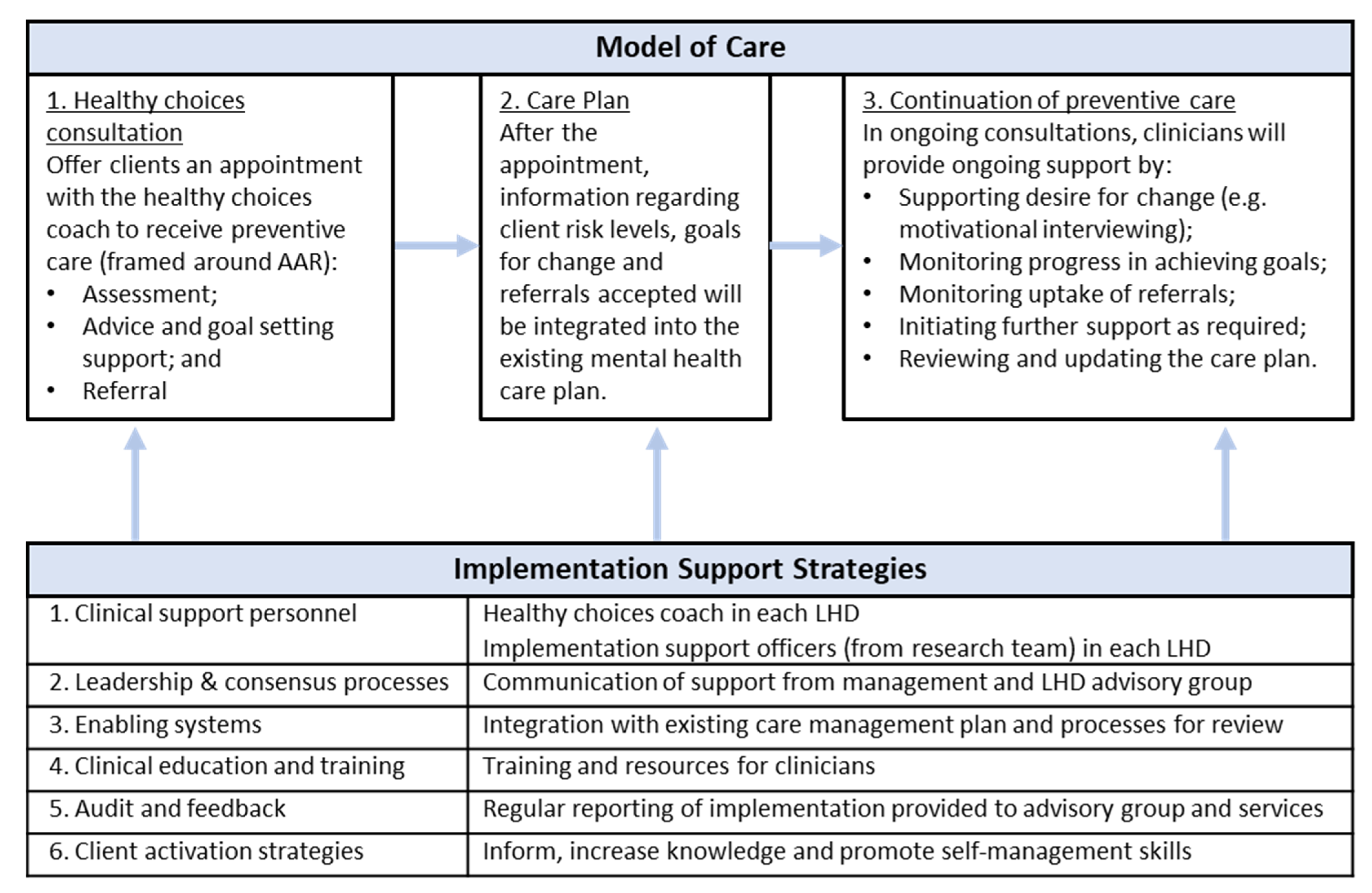
2.4.2. Model of Preventive Care
- ‘Healthy choices’ consultation
- Brief advice and goal setting: Information will be provided regarding how the client’s risk factors compare to Australian guidelines. Tailored motivational interviewing strategies will be used to foster client desire to change their risks and build agency. Clients will be encouraged to identify at least one health improvement goal in line with their risk status and/or desired areas for improvement.
- Referral: Clients will be offered referrals to services that provide behaviour change support, based on their risk status [42,43,44,45,46] and/or their identified health improvement goals. This could include referral to services, such as state-level telephone services (e.g., the NSW Quitline [47] and NSW Get Healthy Information and Coaching service [48]) and local providers (e.g., GP, dietician, support groups, and walking groups).
- ii.
- Chronic disease risk information embedded in the care plan
- iii.
- Continuation of preventive care by mental health clinicians
2.4.3. Implementation Support Strategies
- Clinical support personnel: The HCC embedded within each service to support care delivery and provide education to staff. Implementation support officers (members of the research team; one allocated to each LHD) will support HCCs in this role.
- Leadership and consensus processes: Leaders in each LHD (e.g., service managers) will communicate their strong support for the project. Within each LHD, an advisory group will be established to oversee project direction and implementation.
- Enabling systems: Content from the healthy choices consultation will be integrated into the existing mental health care plan, which will be reviewed regularly in clinical review meetings.
- Clinician education and training: Training sessions and resources will be provided to cases managers regarding strategies for supporting client behaviour change, the importance of addressing chronic disease risks and the logistics of model implementation. Training of the HCC in their role.
- Audit and feedback: An update of progress will be prepared by the HCC and discussed in advisory and working groups to review progress and consider recommended actions.
- Client activation strategies: Resources to build behaviour change agency and self-management skills, and to inform clients about the new model of care (e.g., posters in waiting rooms, client diaries, and educational brochures).
2.5. Control
2.6. Measures
2.6.1. Primary Trial Outcomes
2.6.2. Secondary Trial Outcomes
Client Receipt of Preventive Care
Client Behaviour Change
- Whether they smoked any tobacco products (yes, daily; yes, at least once a week; yes, less than once a week; not at all, quit less than 6 months ago; not at all, quit 6 months or more ago; not at all, never smoked; do not know) and how many cigarettes they smoked per day;
- How many serves of fruit (open ended) and vegetables (open ended) they typically consumed per day;
- How often they consumed alcohol in the last month (never, I do not drink, e.g., never have; none in the last month, e.g., nil last month, drinks occasionally; once a month; 2-to-4 times a month; 2-to-3 times a week; 4 or more times a week; do not know). Those who report consuming alcohol in the previous month will be asked to report how many standard drinks they consumed on a typical drinking day (open ended) and how often they consumed five or more standard drinks on one occasion (never; less than monthly; monthly; weekly; almost daily; daily; do not know) (items adapted from the Alcohol Use Disorders Identification Test (AUDIT-C) for Alcohol Use [50]);
- How many minutes they engaged in walking, moderate physical activity, vigorous physical activity, and strength activities in a typical week (items adapted from the International Physical Activity Questionnaire [51]);
- Their current weight (kg) and height (cm).
2.6.3. Client Sociodemographic Characteristics
2.6.4. Mental Health Clinician Provision of Preventive Care
2.6.5. Implementation Process Outcomes
2.6.6. Cost Data
2.7. Sample Size and Power
2.8. Analysis
2.9. Economic Analysis
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Australia’s Health 2020. Available online: https://www.aihw.gov.au/reports-data/australias-health (accessed on 23 July 2020).
- Bartlem, K.M.; Bowman, J.A.; Bailey, J.M.; Freund, M.; Wye, P.M.; Lecathelinais, C.; McElwaine, K.M.; Campbell, E.M.; Gillham, K.E.; Wiggers, J.H. Chronic disease health risk behaviours amongst people with a mental illness. Aust. N. Z. J. Psychiatry 2015, 49, 731–741. [Google Scholar] [CrossRef] [PubMed]
- Liu, N.H.; Daumit, G.L.; Dua, T.; Aquila, R.; Charlson, F.; Cuijpers, P.; Druss, B.; Dudek, K.; Freeman, M.; Fujii, C.; et al. Excess mortality in persons with severe mental disorders: A multilevel intervention framework and priorities for clinical practice, policy and research agendas. World Psychiatry 2017, 16, 30–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, D.; Hancock, K.J.; Kisely, S. The gap in life expectancy from preventable physical illness in psychiatric patients in Western Australia: Retrospective analysis of population based registers. BMJ 2013, 346, f2539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. Mental Health Action Plan; World Health Organisation: Geneva, Switzerland, 2013. [Google Scholar]
- National Mental Health Commission. Equally Well Consensus Statement: Improving the Physical Health and Wellbeing of People Living with Mental Illness in Australia; Sydney NMHC: Washington, DC, USA, 2016. [Google Scholar]
- The Royal Australian College of General Practitioners. Guidelines for Preventive Activities in General Practice, 9th ed.; RACGP: East Melbourne, VIC, Australia, 2018. [Google Scholar]
- NSW Department of Health. Physical Health Care within Mental Health Services; NSW Governement: Canberra, Australia, 2017. [Google Scholar]
- Alexander, S.C.; Cox, M.E.; Turner, C.L.B.; Lyna, P.; Ostbye, T.; Tulsky, J.A.; Dolor, R.J.; Pollak, K.I. Do the Five A’s Work When Physicians Counsel About Weight Loss? Fam. Med. 2011, 43, 179–184. [Google Scholar] [PubMed]
- Pronk, N.P.; Peek, C.J.; Goldstein, M.G. Addressing multiple behavioral risk factors in primary care. A synthesis of current knowledge and stakeholder dialogue sessions. Am. J. Prev. Med. 2004, 27 (Suppl. 2), 4–17. [Google Scholar] [CrossRef]
- Royal Australian College of General Practitioners. Smoking, Nutrition, Alcohol, Physical Activity (SNAP): A Population Health Guide to Behavioural Risk Factors in General Practice; RACGP: Melbourne, VIC, Australia, 2015. [Google Scholar]
- Rueda-Clausen, C.F.; Benterud, E.; Bond, T.; Olszowka, R.; Vallis, M.T.; Sharma, A.M. Effect of implementing the 5As of obesity management framework on provider-patient interactions in primary care. Clin. Obes. 2014, 4, 39–44. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Mental Health Services–In Brief 2019; Australian Institute of Health and Welfare: Canberra, Australia, 2019.
- Schroeder, S.A. What to do with a patient who smokes. JAMA J. Am. Med Assoc. 2005, 294, 482–487. [Google Scholar] [CrossRef]
- Gordon, J.S.; Andrews, J.A.; Crews, K.M.; Payne, T.J.; Severson, H.H. The 5A’s vs 3A’s plus proactive quitline referral in private practice dental offices: Preliminary results. Tob. Control 2007, 16, 285–288. [Google Scholar] [CrossRef] [Green Version]
- Gordon, J.S.; Andrews, J.A.; Crews, K.M.; Payne, T.J.; Severson, H.H.; Lichtenstein, E. Do faxed quitline referrals add value to dental office-based tobacco-use cessation interventions? J. Am. Dent. Assoc. 2010, 141, 1000–1007. [Google Scholar] [CrossRef] [Green Version]
- Fiore, M.C.; Jaén, C.R.; Baker, T.B.; Bailey, W.C.; Bennett, G.; Benowitz, N.L.; Chrisiansen, B.A.; Connell, M.; Curry, S.J.; Dorfman, S.F.; et al. Treating Tobacco Use and Dependence: 2008 Update; US Department of Health and Human Services: Rockville, MD, USA, 2008. [Google Scholar]
- Glasgow, R.E.; Emont, S.; Miller, D.C. Assessing delivery of the five ‘As’ for patient-centered counseling. Health Promot. Int. 2006, 21, 245–255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Happell, B.; Scott, D.; Platania-Phung, C.; Nankivell, J. Should we or shouldn’t we? Mental health nurses’ views on physical health care of mental health consumers. Int. J. Ment. Health Nurs. 2012, 21, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Bailey, J.M.; Bartlem, K.M.; Wiggers, J.H.; Wye, P.M.; Stockings, E.A.L.; Hodder, R.K.; Metse, A.P.; Regan, T.W.; Clancy, R.; Dray, J.A.; et al. Systematic review and meta-analysis of the provision of preventive care for modifiable chronic disease risk behaviours by mental health services. Prev. Med. Rep. 2019, 16, 100969. [Google Scholar] [CrossRef] [PubMed]
- Happell, B.; Scott, D.; Platania-Phung, C. Perceptions of barriers to physical health care for people with serious mental illness: A review of the international literature. Issues Ment. Health Nurs. 2012, 33, 752–761. [Google Scholar] [CrossRef] [PubMed]
- Fehily, C.; Hodder, R.; Bartlem, K.; Wiggers, J.; Wolfenden, L.; Dray, J.; Bailey, J.; Wilczynska, M.; Stockings, E.; Clinton-McHarg, T.; et al. The effectiveness of interventions to increase preventive care provision for chronic disease risk behaviours in mental health settings: A systematic review and meta-analysis. Prev. Med. Rep. 2020, 19, 101108. [Google Scholar] [CrossRef] [PubMed]
- Effective Practice and Organisation of Care (EPOC). EPOC Taxonomy. 2015. Available online: Epoc.cochrane.org/epoc-taxonomy (accessed on 3 January 2022).
- Druss, B.G.; von Esenwein, S.A.; Compton, M.T.; Rask, K.J.; Zhao, L.; Parker, R.M. The Primary Care Access Referral, and Evaluation (PCARE) Study: A Randomized Trial of Medical Care Management for Community Mental Health Settings. Am. J. Psychiatry 2010, 167, 151–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Happell, B.; Ewart, S.B.; Platania-Phung, C.; Bocking, J.; Griffiths, K.; Scholz, B.; Stanton, R. Embedding a physical health nurse consultant within mental health services: Consumers’ perspectives. Int. J. Ment. Health Nurs. 2016, 25, 377–384. [Google Scholar] [CrossRef]
- Happell, B.; Platania-Phung, C.; Stanton, R.; Millar, F. Exploring the views of nurses on the cardiometabolic health nurse in mental health services in australia. Issues Ment. Health Nurs. 2015, 36, 135–144. [Google Scholar] [CrossRef]
- Fehily, C.M.; Bartlem, K.M.; Wiggers, J.H.; Wye, P.M.; Clancy, R.V.; Castle, D.J.; Wilson, A.; Rissel, C.E.; Wutzke, S.; Hodder, R.K.; et al. Effectiveness of embedding a specialist preventive care clinician in a community mental health service in increasing preventive care provision: A randomised controlled trial. Aust. N. Z. J. Psychiatry 2020, 54, 620–632. [Google Scholar] [CrossRef]
- Fehily, C.; Ling, R.; Searles, A.; Bartlem, K.; Wiggers, J.; Hodder, R.; Wilson, A.; Colyvas, K.; Bowman, J. An economic evaluation of a specialist preventive care clinician in a community mental health service: A randomised controlled trial. BMC Health Serv. Res. 2020, 20, 405. [Google Scholar] [CrossRef]
- Fehily, C.M.C.; Bartlem, K.M.; Wiggers, J.H.; Hodder, R.K.; Gibson, L.K.; Hancox, N.; Bowman, B.A. Uptake of a preventive care consultation offered to clients of a community mental health service. Prev. Med. Rep. 2020, 18, 101076. [Google Scholar] [CrossRef] [PubMed]
- Flodgren, G.; Parmelli, E.; Doumit, G.; Gattellari, M.; O’Brien, M.A.; Grimshaw, J. Local opinion leaders: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2011, 6, CD000125. [Google Scholar] [CrossRef] [PubMed]
- Forsetlund, L.; Bjørndal, A.; Rashidian, A.; Jamtvedt, G.; O’Brien, M.A.; Wolf, F.; Davis, D.; Herrin, J. Continuing education meetings and workshops: Effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2009, 15, CD003030. [Google Scholar] [CrossRef] [PubMed]
- Ivers, N.; Jamtvedt, G.; Flottorp, S.; Young, J.M.; Odgaard-Jensen, J.; French, S.D.; O’Brien, M.A.; Johansen, M.; Grimshaw, J.; Oxman, A.D. Audit and feedback: Effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2012, 13, CD000259. [Google Scholar] [CrossRef] [PubMed]
- Fønhus, M.S.; Dalsbø, T.K.; Johansen, M.; Fretheim, A.; Skirbekk, H.; Flottorp, S.A. Patient-mediated interventions to improve professional practice. Cochrane Database Syst. Rev. 2018, 9, CD012472. [Google Scholar] [CrossRef] [PubMed]
- Bartlem, K.M.; Bowman, J.; Freund, M.; Wye, P.M.; Barker, D.; McElwaine, K.M.; Wolfenden, L.; Campbell, E.M.; McElduff, P.; Gillham, K.; et al. Effectiveness of an intervention in increasing the provision of preventive care by community mental health services: A non-randomized, multiple baseline implementation trial. Implement. Sci. IS 2016, 11, 46. [Google Scholar] [CrossRef] [Green Version]
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.M.; Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217–226. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Management of Physical Health Conditions in Adults with Severe Mental Disorders: WHO Guidelines; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- NSW Health. Physical Health Care for People Living with Mental Health Issues; NSW Health: Sydney, Australia, 2021. [Google Scholar]
- Bartlem, K.; Bowman, J.; Freund, M.; Wye, P.; Lecathelinais, C.; McElwaine, K.; Wolfenden, L.; Gillham, K.; Wiggers, J. Acceptability and Receipt of Preventive Care for Chronic-Disease Health Risk Behaviors Reported by Clients of Community Mental Health Services. Psychiatr. Serv. 2015, 66, 857–864. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Socio-Economic Indexes for Areas; 2018. Available online: https://www.abs.gov.au/websitedbs/censushome.nsf/home/seifa (accessed on 27 March 2018).
- Morton, K.; Beauchamp, M.; Prothero, A.; Joyce, L.; Saunders, L.; Spencer-Bowdage, S.; Dancy, B.; Pedlar, C. The effectiveness of motivational interviewing for health behaviour change in primary care settings: A systematic review. Health Psychol. Rev. 2015, 9, 205–223. [Google Scholar] [CrossRef]
- Department of Health. Australia’s Physical Activity and Sedentary Behaviour Guidelines for Adults (18–64 Years); Commonwealth of Australia: Canberra, Australia, 2014. [Google Scholar]
- Intergovernmental Committee on Drugs. National Tobacco Strategy 2012–2018; Commonwealth of Australia: Canberra, Australia, 2012. [Google Scholar]
- National Health and Medical Research Council. Eat for Health: Australian Dietary Guidelines; Commonwealth of Australia: Canberra, Australia, 2013. [Google Scholar]
- National Health and Medical Research Council. Australian Guidelines to Reduce Health Risks from Drinking Alcohol; Commonwealth of Australia: Canberra, Australia, 2020. [Google Scholar]
- Australian Institute of Health and Welfare. Australia’s Health 2020: In Brief. Available online: https://www.aihw.gov.au/ (accessed on 23 July 2020).
- NSW Quitline. Available online: https://www.cancer.nsw.gov.au/prevention-and-screening/preventing-cancer/quit-smoking/nsw-quitline (accessed on 1 January 2022).
- NSW Get Healthy Information and Coaching Service. Available online: https://www.gethealthynsw.com.au/ (accessed on 3 January 2022).
- Bartlem, K.M.; Bowman, J.A.; Freund, M.; Wye, P.M.; McElwaine, K.M.; Wolfenden, L.; Campbell, E.M.; Gillham, K.E.; Wiggers, J.H. Care Provision to Prevent Chronic Disease by Community Mental Health Clinicians. Am. J. Prev. Med. 2014, 47, 762–770. [Google Scholar] [CrossRef] [Green Version]
- Babor, T.F.; Higgins-Biddle, J.C.; Saunders, J.B.; Monteiro, M.G. The Alcohol Use Disorders Identification Test; World Health Organisation, Department of Mental Health and Substance Dependence: Geneva, Switzerland, 2001. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.L.F.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heather, N.; Smailes, D.; Cassidy, P. Development of a Readiness Ruler for use with alcohol brief interventions. Drug Alcohol Depend. 2008, 98, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Fehily, C.; Bartlem, K.; Wiggers, J.; Wye, P.; Clancy, R.; Castle, D.; Wutzke, S.; Rissel, C.; Wilson, A.; McCombie, P.; et al. Evaluating the effectiveness of a healthy lifestyle clinician in addressing the chronic disease risk behaviours of community mental health clients: Study protocol for a randomised controlled trial. Trials 2017, 18, 276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiner, B.J.; Lewis, C.C.; Stanick, C.; Powell, B.J.; Dorsey, C.N.; Clary, A.S.; Boynton, M.H.; Halko, H. Psychometric assessment of three newly developed implementation outcome measures. Implement. Sci. IS 2017, 12, 108. [Google Scholar] [CrossRef] [PubMed]
- Metse, A.P.; Wiggers, J.; Wye, P.; Wolfenden, L.; Freund, M.; Clancy, R.; Stockings, E.; Terry, M.; Allan, J.; Colyvas, K.; et al. Efficacy of a universal smoking cessation intervention initiated in inpatient psychiatry and continued post-discharge: A randomised controlled trial. Aust. N. Z. J. Psychiatry 2017, 51, 366–381. [Google Scholar] [CrossRef] [PubMed]
- Mechling, B.M.; Arms, T. Losing to Gain: The Effects of a Healthy Lifestyle Intervention on the Physical and Psychosocial Well-being of Clients in a Community-based Mental Health Setting. Community Ment. Health J. 2019, 55, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Stanton, S.; Rosenbaum, S.; Kalucy, M.; Reaburn, P.; Happell, B. A call to action: Exercise as treatment for patients with mental illness. Aust. J. Prim. Health 2015, 21, 120–125. [Google Scholar] [CrossRef] [Green Version]
- Ashdown-Franks, G.; Sabiston, C.M.; Stubbs, B. The evidence for physical activity in the management of major mental illnesses: A concise overview to inform busy clinicians’ practice and guide policy. Curr. Opin. Psychiatry 2019, 32, 375–380. [Google Scholar] [CrossRef]
- Taylor, G.M.J.; Lindson, N.; Farley, A.; Leinberger-Jabari, A.; Sawyer, K.; Te Water Naudé, R.; Theodoulou, A.; King, N.; Burke, C.; Aveyard, P. Smoking cessation for improving mental health. Cochrane Database Syst. Rev. 2021, 3, CD013522. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Component/ Strategy | Description (Providing a Basis for Co-Development) | Examples of Elements to Be Determined Through Co-Development |
|---|---|---|
| Model of Care | ||
| Healthy choices consultation | Clients are offered an appointment with the healthy choices clinician (HCC) to receive preventive care (framed around the AAR framework):
|
|
| Care plan | After the consultation, information regarding client risks, goals for change, and referrals offered and/or accepted are integrated into the existing mental health care plan. |
|
| Continuation of preventive care | In ongoing mental health consultations (commencing in the next scheduled appointment after the healthy choices consultation), clinicians provide ongoing support and follow-up by:
|
|
| Implementation Support Strategies | ||
| Clinical support personnel | The HCC embedded within each service is funded for 9 months by the trial, employed by the LHD as a member of the service. In addition to client care delivery, the HCC also provides support and training to clinicians. Implementation support officers (research team members; one allocated to each LHD) will regularly contact the HCC to support them in this role. |
|
| Leadership and consensus processes | Managers communicate support for the new model to all clinicians and reinforce its alignment with state policy and the LHD’s strategic directions. An advisory group for each LHD is established, with representation of the research team, directors, and service managers to oversee implementation, and to monitor and provide feedback throughout. |
|
| Enabling systems | The HCC records a summary of each ‘healthy choices’ consultation in the electronic medical record system. Content regarding risk behaviours, goals for change, and referrals offered and/or accepted is integrated into the existing care management plan that is part of routine mental health care delivery. The review of the plan is incorporated within the regular team clinical review meetings where the needs and progress of individual clients are discussed. The HCC attends clinical review meetings, contributing to discussions of how plans are incorporated in routine care and offering additional support or advice to clinicians as required. |
|
| Clinician education and training | Training sessions and resources are provided regarding the importance of addressing risk factors for both physical and mental health, risk guidelines and referral services. Clinicians are upskilled in strategies to support client behaviour change, including motivational interviewing, setting and reviewing, e.g., goals, and identifying and addressing barriers. Training is provided in the processes to implement the model of care, such as in scheduling and facilitating client attendance of the ‘healthy choices’ consultation and checking and updating the care plan. |
|
| Audit and feedback | A summary of preventive care delivery and implementation of the intervention is regularly prepared by the HCC and provided to the LHD advisory group to review progress and consider possible implementation modifications. Summary is also provided to managers and clinicians. |
|
| Client activation strategies | Resources are provided to clients to build behaviour change agency and promote self-management skills, such as educational brochures. Materials are also developed to inform clients about the model of preventive care. New clients receive information outlining the care they will receive as part of standard intake processes. |
|
| Risk Factor | Definition of Risk | References |
|---|---|---|
| Tobacco smoking | Any tobacco smoking | [43] |
| Inadequate fruit and vegetable intake | Consuming less than two servings of fruit or five servings of vegetables daily (as an indicator of poor nutrition) | [44] |
| Harmful alcohol consumption | Consuming more than two standard drinks on an average day or five or more on any one occasion | [45] |
| Physical inactivity | Engaging in less than 150 min of moderate-intensity physical activity or 75 min of vigorous-intensity physical activity, or an equivalent combination of each, weekly | [44] |
| Unhealthy weight | Waist circumference above 80 cm for women and 94 cm for men, or body mass index (method to be determined through co-development) | [46] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fehily, C.; McKeon, E.; Stettaford, T.; Campbell, E.; Lodge, S.; Dray, J.; Bartlem, K.; Reeves, P.; Oldmeadow, C.; Castle, D.; et al. The Effectiveness and Cost of an Intervention to Increase the Provision of Preventive Care in Community Mental Health Services: Protocol for a Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 3119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19053119
Fehily C, McKeon E, Stettaford T, Campbell E, Lodge S, Dray J, Bartlem K, Reeves P, Oldmeadow C, Castle D, et al. The Effectiveness and Cost of an Intervention to Increase the Provision of Preventive Care in Community Mental Health Services: Protocol for a Cluster-Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(5):3119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19053119
Chicago/Turabian StyleFehily, Caitlin, Emma McKeon, Tegan Stettaford, Elizabeth Campbell, Simone Lodge, Julia Dray, Kate Bartlem, Penny Reeves, Christopher Oldmeadow, David Castle, and et al. 2022. "The Effectiveness and Cost of an Intervention to Increase the Provision of Preventive Care in Community Mental Health Services: Protocol for a Cluster-Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 5: 3119. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19053119