
Association between Objectively Measured Sedentary Behaviour and Sleep Quality in Japanese Adults: A Population-Based Cross-Sectional Study

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measurements of Sedentary Time and Physical Activity
2.3. Pittsburgh Sleep Quality Index (PSQI)
2.4. Visceral Fat Measurement
2.5. Other Variables
2.6. Statistical Analysis
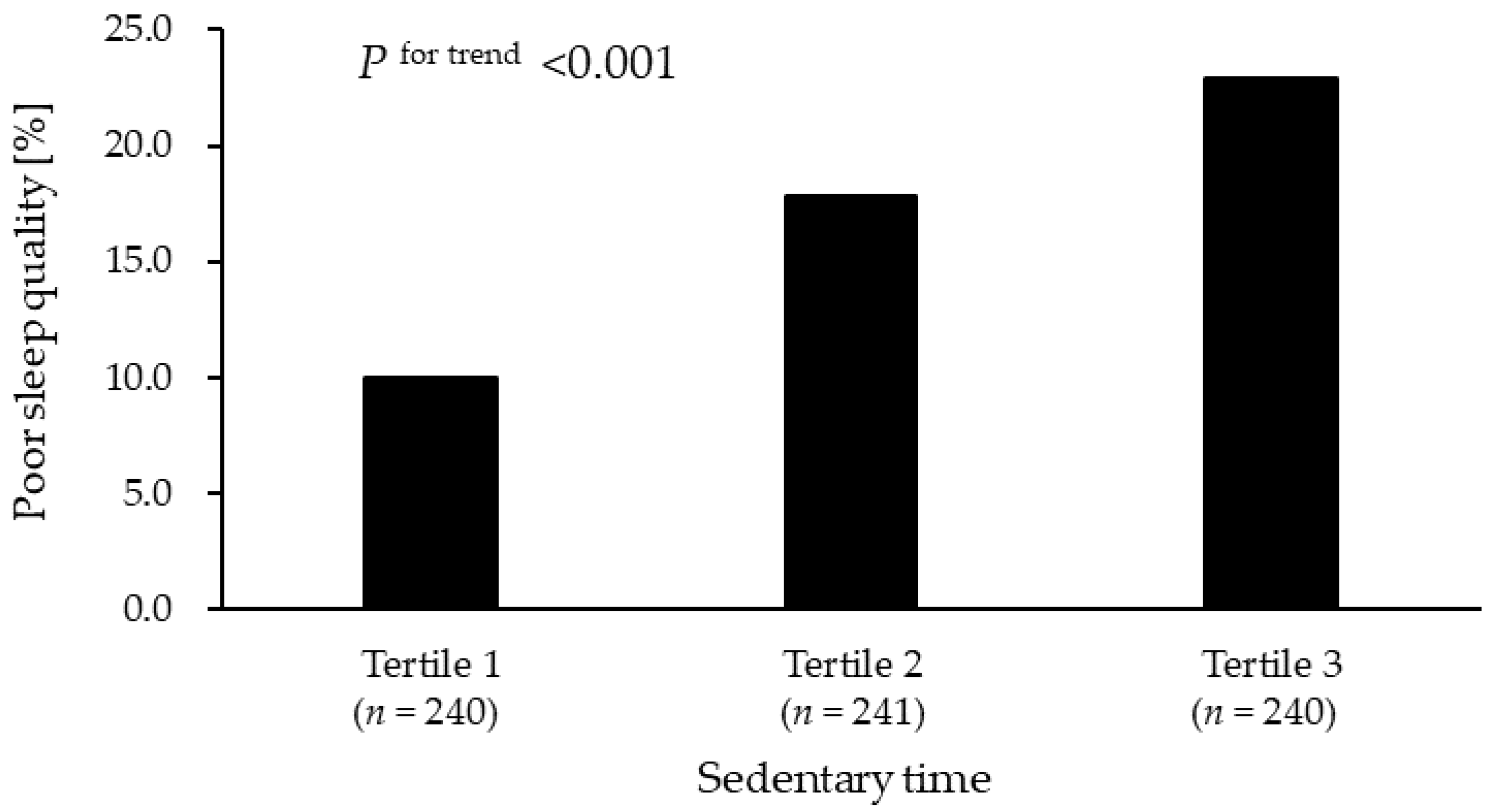
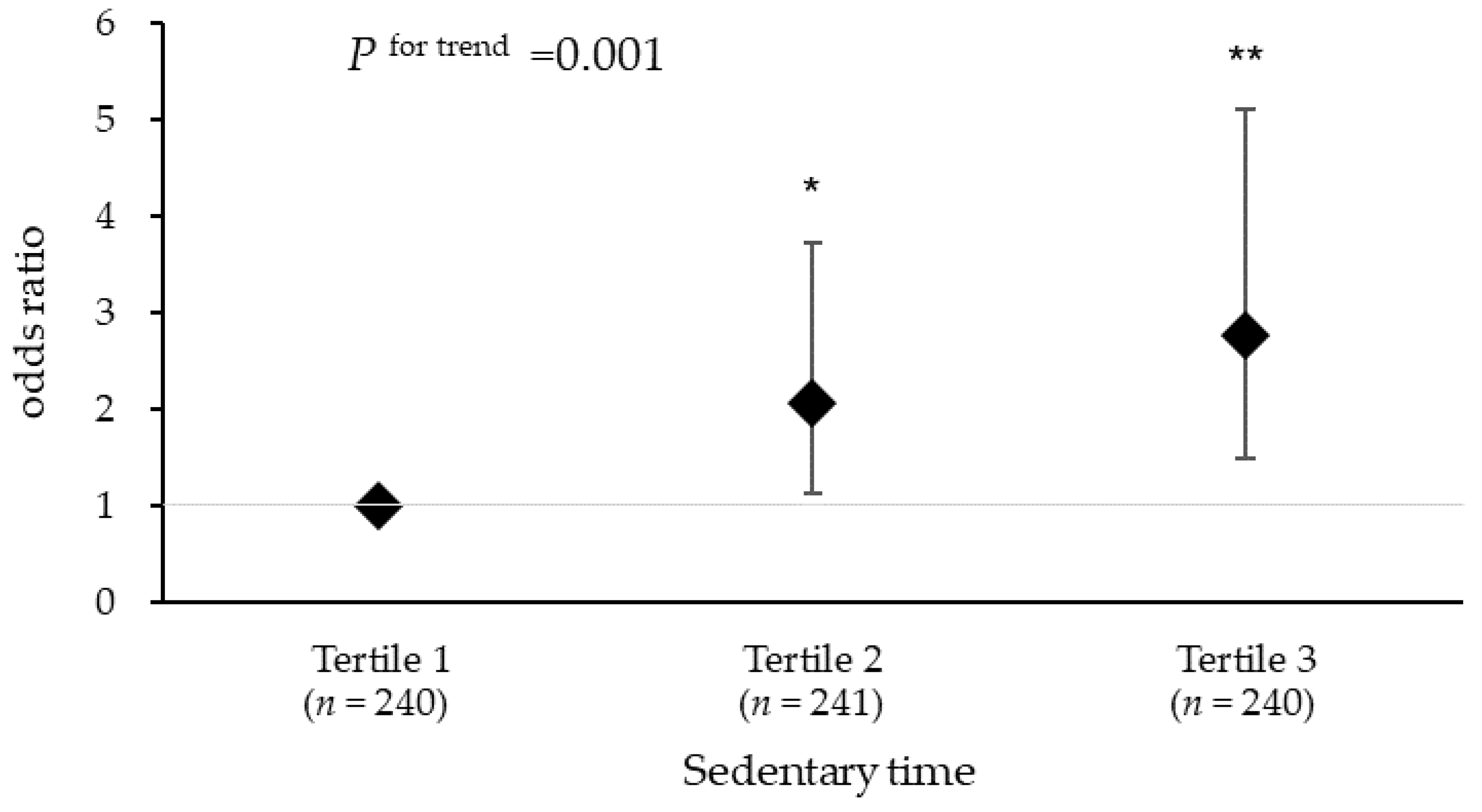
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koyanagi, A.; Stickley, A. The Association between Sleep Problems and Psychotic Symptoms in the General Population: A Global Perspective. Sleep 2015, 38, 1875–1885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leger, D.; Poursain, B.; Neubauer, D.; Uchiyama, M. An international survey of sleeping problems in the general population. Curr. Med. Res. Opin. 2008, 24, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Stranges, S.; Tigbe, W.; Gómez-Olivé, F.X.; Thorogood, M.; Kandala, N.B. Sleep Problems: An Emerging Global Epidemic? Findings From the INDEPTH WHO-SAGE Study Among More Than 40,000 Older Adults From 8 Countries across Africa and Asia. Sleep 2012, 35, 1173–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buysse, D.J. Sleep Health: Can We Define It? Does It Matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kido, K.; Hatakeyama, S.; Imai, A.; Yamamoto, H.; Tobisawa, Y.; Yoneyama, T.; Yoneyama, T.; Hashimoto, Y.; Koie, T.; Nakaji, S.; et al. Sleep Disturbance Has a Higher Impact on General and Mental Quality of Life Reduction than Nocturia: Results from the Community Health Survey in Japan. Eur. Urol. Focus. 2019, 5, 1120–1126. [Google Scholar] [CrossRef] [Green Version]
- Physical Activity Guidelines Advisory Committee, U.S. Department of Health and Human Services. Physical Activity Guidelines Advisory Committee Scientific Report; Physical Activity Guidelines Advisory Committee, U.S. Department of Health and Human Services: Washington, DC, USA, 2018.
- World Health Organization. WHO Guidelines for Physical Activity and Sedentary Behaviour; WHO: Geneva, Switzerland, 2020.
- Yang, Y.; Shin, J.C.; Li, D.; An, R. Sedentary Behavior and Sleep Problems: A Systematic Review and Meta-Analysis. Int. J. Behav. Med. 2017, 24, 481–492. [Google Scholar] [CrossRef]
- Creasy, S.A.; Crane, T.E.; Garcia, D.O.; Thomson, C.A.; Kohler, L.N.; Wertheim, B.C.; Baker, L.D.; Coday, M.; Hale, L.; Womack, C.R.; et al. Higher Amounts of Sedentary Time are Associated with Short Sleep Duration and Poor Sleep Quality in Postmenopausal Women. Sleep 2019, 42, zsz093. [Google Scholar] [CrossRef]
- Park, H.; Suh, B. Association Between Sleep Quality and Physical Activity According to Gender and Shift Work. J. Sleep Res. 2020, 29, e12924. [Google Scholar] [CrossRef]
- Sloan, R.A.; Kim, Y.; Sawada, S.S.; Asakawa, A.; Blair, S.N.; Finkelstein, E.A. Is Less Sedentary Behavior, More Physical Activity, or Higher Fitness Associated with Sleep Quality? A Cross-Sectional Study in Singapore. Int. J. Environ. Res. Public Health. 2020, 17, 1337. [Google Scholar] [CrossRef] [Green Version]
- Bauman, A.; Ainsworth, B.E.; Sallis, J.F.; Hagströmer, M.; Craig, C.L.; Bull, F.C.; Pratt, M.; Venugopal, K.; Chau, J.; Sjöström, M. IPS Group. The Descriptive Epidemiology of Sitting. Am. J. Prev. Med. 2011, 41, 228–235. [Google Scholar] [CrossRef]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, G.D.; Fiorelli, E.M.; Furlan, L.; Montano, N.; Tobaldini, E. Obesity and Sleep Disturbances: The “Chicken or the Egg” Question. Eur. J. Intern. Med. 2021, 92, 11–16. [Google Scholar] [CrossRef] [PubMed]
- Nishizawa, H.; Shimomura, I. Population Approaches Targeting Metabolic Syndrome Focusing on Japanese Trials. Nutrients 2019, 11, 1430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shinohara, E.; Kihara, S.; Yamashita, S.; Yamane, M.; Nishida, M.; Arai, T.; Kotani, K.; Nakamura, T.; Takemura, K.; Matsuzawa, Y. Visceral Fat Accumulation as an Important Risk Factor for Obstructive Sleep Apnoea Syndrome in Obese Subjects. J. Intern. Med. 1997, 241, 11–18. [Google Scholar] [CrossRef] [Green Version]
- Nakaji, S.; Ihara, K.; Sawada, K.; Parodi, S.; Umeda, T.; Takahashi, I.; Murashita, K.; Kurauchi, S.; Tokuda, I. Social Innovation for Life Expectancy Extension Utilizing a Platform-centered System Used in the Iwaki Health Promotion Project: A Protocol Paper. SAGE Open Med 2021, 9, 205031212110026. [Google Scholar] [CrossRef]
- Jung, S.; Lee, S.; Lee, S.; Bae, S.; Imaoka, M.; Harada, K.; Shimada, H. Relationship between Physical Activity Levels and Depressive Symptoms in Community-Dwelling Older Japanese Adults. Geriatr. Gerontol. Int. 2018, 18, 421–427. [Google Scholar] [CrossRef]
- Harada, K.; Lee, S.; Lee, S.; Bae, S.; Anan, Y.; Harada, K.; Shimada, H. Distance from Public Transportation and Physical Activity in Japanese Older Adults: The Moderating Role of Driving Status. Health Psychol. 2018, 37, 355–363. [Google Scholar] [CrossRef]
- Jung, S.; Lee, S.; Bae, S.; Lee, S.; Makino, K.; Shinkai, Y.; Shimada, H. Effectiveness of the KENKOJISEICHI Local Revitalization System on Cognitive Function Change in Older Adults with Mild Cognitive Impairment: Study Protocol for a Randomized Controlled Trial. Trials 2018, 19, 276. [Google Scholar] [CrossRef] [Green Version]
- Doi, Y.; Minowa, M.; Uchiyama, M.; Okawa, M.; Kim, K.; Shibui, K.; Kamei, Y. Psychometric Assessment of Subjective Sleep Quality Using the Japanese Version of the Pittsburgh Sleep Quality Index (PSQI-J) in Psychiatric Disordered and Control Subjects. Psychiatry Res. 2000, 97, 165–172. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Ozato, N.; Katashima, M.; Sawada, K.; Katsuragi, Y.; Ihara, K.; Nakaji, S. A Novel Method to Visualize the Dietary Macronutrient Composition of Smaller Visceral Fat Accumulation. Front. Nutr. 2020, 6, 194. [Google Scholar] [CrossRef]
- Ryo, M.; Maeda, K.; Onda, T.; Katashima, M.; Okumiya, A.; Nishida, M.; Yamaguchi, T.; Funahashi, T.; Matsuzawa, Y.; Nakamura, T.; et al. A New Simple Method for the Measurement of Visceral Fat Accumulation by Bioelectrical Impedance. Diabetes Care 2005, 28, 451–453. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Comparison of Relative Validity of Food Group Intakes Estimated by Comprehensive and Brief-type Self-administered Diet History Questionnaires Against 16 d Dietary Records in Japanese Adults. Public Health Nutr. 2011, 14, 1200–1211. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Honda, S.; Murakami, K.; Sasaki, S.; Okubo, H.; Hirota, N.; Notsu, A.; Fukui, M.; Date, C. Both Comprehensive and Brief Self-Administered Diet History Questionnaires Satisfactorily Rank Nutrient Intakes in Japanese Adults. J. Epidemiol. 2012, 22, 151–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Qi, Q.; Strizich, G.; Merchant, G.; Sotres-Alvarez, D.; Buelna, C.; Castaneda, S.F.; Gallo, L.C.; Cai, J.; Gellman, M.D.; Isasi, C.R.; et al. Objectively Measured Sedentary Time and Cardiometabolic Biomarkers in US Hispanic/Latino Adults: The Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Circulation 2015, 132, 1560–1569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, K.M.; Howard, V.J.; Hutto, B.; Colabianchi, N.; Vena, J.E.; Safford, M.M.; Blair, S.N.; Hooker, S.P. Patterns of Sedentary Behavior and Mortality in U.S. Middle-Aged and Older Adults: A National Cohort Study. Ann. Intern. Med. 2017, 167, 465–475. [Google Scholar] [CrossRef] [PubMed]
- Gilchrist, S.C.; Howard, V.J.; Akinyemiju, T.; Judd, S.E.; Cushman, M.; Hooker, S.P.; Diaz, K.M. Association of Sedentary Behavior With Cancer Mortality in Middle-aged and Older US Adults. JAMA Oncol 2020, 6, 1210–1217. [Google Scholar] [CrossRef]
- Ando, S.; Koyama, T.; Kuriyama, N.; Ozaki, E.; Uehara, R. The Association of Daily Physical Activity Behaviors with Visceral Fat. Obes. Res. Clin. Pract. 2020, 14, 531–535. [Google Scholar] [CrossRef]
- Sweatt, S.K.; Gower, B.A.; Chieh, A.Y.; Liu, Y.; Li, L. Sleep Quality is Differentially Related to Adiposity in Adults. Psychoneuroendocrinology. 2018, 98, 46–51. [Google Scholar] [CrossRef]
- Kubitz, K.A.; Landers, D.M.; Petruzzello, S.J.; Han, M. The Effects of Acute and Chronic Exercise on Sleep. Sports Med. 1996, 21, 277–291. [Google Scholar] [CrossRef]
- Driver, H.S.; Taylor, S.R. Exercise and Sleep. Sleep Med. Rev. 2000, 4, 387–402. [Google Scholar] [CrossRef] [PubMed]
- Sasai, T.; Inoue, Y.; Komada, Y.; Nomura, T.; Matsuura, M.; Matsushima, E. Effects of Insomnia and Sleep Medication on Health-related Quality of Life. Sleep Med. 2010, 11, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Algul, A.; Ates, M.A.; Semiz, U.B.; Basoglu, C.; Ebrinc, S.; Gecici, O.; Gulsun, M.; Kardesoglu, E.; Cetin, M. Evaluation of General Psychopathology, Subjective Sleep Quality, and Health-related Quality of Life in Patients with Obesity. Int. J. Psychiatry Med. 2009, 39, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Koren, D.; Dumin, M.; Gozal, D. Role of Sleep Quality in the Metabolic Syndrome. Diabetes Metab. Syndr. Obes. 2016, 9, 281–310. [Google Scholar] [CrossRef] [Green Version]
- Després, J.P. Body Fat Distribution and Risk of Cardiovascular Disease. Circulation 2012, 126, 1301–1313. [Google Scholar] [CrossRef] [Green Version]
- Matsushita, Y.; Nakagawa, T.; Yamamoto, S.; Takahashi, Y.; Yokoyama, T.; Noda, M.; Mizoue, T. Associations of Visceral and Subcutaneous Fat Areas With the Prevalence of Metabolic Risk Factor Clustering in 6292 Japanese Individuals: The Hitachi Health Study. Diabetes Care 2010, 33, 2117–2119. [Google Scholar] [CrossRef] [Green Version]
- Shah, R.V.; Murthy, V.L.; Abbasi, S.A.; Blankstein, R.; Kwong, R.Y.; Goldfine, A.B.; Jerosch-Herold, M.; Lima, J.A.; Ding, J.; Allison, M.A. Visceral Adiposity and the Risk of Metabolic Syndrome Across Body Mass Index: The MESA Study. JACC Cardiovasc. Imaging 2014, 7, 1221–1235. [Google Scholar] [CrossRef] [Green Version]
- Dekker, S.A.; Noordam, R.; Biermasz, N.R.; De Roos, A.; Lamb, H.J.; Rosendaal, F.R.; Rensen, P.C.N.; Van Heemst, D.; De Mutsert, R. Habitual Sleep Measures are Associated with Overall Body Fat, and not Specifically with Visceral Fat, in Men and Women. Obesity 2018, 26, 1651–1658. [Google Scholar] [CrossRef] [Green Version]
- Cillekens, B.; Lang, M.; Van Mechelen, W.; Verhagen, E.; Huysmans, M.A.; Holtermann, A.; Van der Beek, A.J.; Coenen, P. How Does Occupational Physical Activity Influence Health? An Umbrella Review of 23 Health Outcomes Across 158 Observational Studies. Br. J. Sports Med. 2020, 54, 1474–1481. [Google Scholar] [CrossRef]
- Edwards, M.K.; Loprinzi, P.D. Experimentally Increasing Sedentary Behavior Results in Decreased Sleep Quality Among Young Adults. Ment. Health Phys. Act. 2017, 12, 132–140. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PSQI < 6 (n = 599) | PSQI ≥ 6 (n = 122) | p-Value | |
|---|---|---|---|
| Age, years | 58 (44–66) | 52 (39–65) | 0.031 |
| Sex, % women | 59.9 | 69.7 | 0.052 |
| Smoking Status, % | |||
| Never | 62.9 | 68.0 | 0.105 |
| Former | 23.9 | 15.6 | |
| Current | 13.2 | 16.4 | |
| Alcohol intake, % | |||
| None | 43.1 | 51.6 | 0.239 |
| Low (<20 g/day) | 34.6 | 29.5 | |
| High (≥20 g/day) | 22.4 | 18.9 | |
| CES-D score | 5 (2–10) | 12 (6–20) | <0.001 |
| BMI, kg/m2 | 22.5 (20.3–24.7) | 22.8 (20.6–25.3) | 0.789 |
| VFA, cm2 | 75 (48–108) | 79 (50–111) | 0.774 |
| Accelerometer wear time, h/day | 15.5 (14.2–16.6) | 15.6 (14.4–17.2) | 0.341 |
| Sedentary time, h/day 1 | 10.9 (9.87–11.8) | 11.4 (10.6–12.2) | <0.001 |
| MVPA, h/day | 0.38 (0.26–0.53) | 0.39 (0.27–0.53) | 0.616 |
| PSQI global score | 3 (2–4) | 7 (6–8) | <0.001 |
| PSQI Global Score | Sleep Quality | Sleep Latency | Sleep Duration | Habitual Sleep Efficiency | Sleep Disturbance | Use of Sleeping Medication | Daytime Dysfunction | |
|---|---|---|---|---|---|---|---|---|
| Sedentary time | 0.10 * | 0.06 | 0.11 * | −0.01 | 0.03 | 0.04 | 0.06 | 0.13 ** |
| Tertiles of Sedentary Time | ||||
|---|---|---|---|---|
| Tertile 1 (n = 240) | Tertile 2 (n = 241) | Tertile 3 (n = 240) | p-Value for Trend | |
| Model 1 | 1.00 (reference) | 1.87 (1.09, 3.20) | 2.44 (1.44, 4.14) | <0.001 |
| Model 2 | 1.00 (reference) | 2.07 (1.15, 3.75) | 2.98 (1.62, 5.48) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kinoshita, K.; Ozato, N.; Yamaguchi, T.; Sudo, M.; Yamashiro, Y.; Mori, K.; Katsuragi, Y.; Yasukawa, T.; Murashita, K.; Nakaji, S.; et al. Association between Objectively Measured Sedentary Behaviour and Sleep Quality in Japanese Adults: A Population-Based Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 3145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19053145
Kinoshita K, Ozato N, Yamaguchi T, Sudo M, Yamashiro Y, Mori K, Katsuragi Y, Yasukawa T, Murashita K, Nakaji S, et al. Association between Objectively Measured Sedentary Behaviour and Sleep Quality in Japanese Adults: A Population-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(5):3145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19053145
Chicago/Turabian StyleKinoshita, Keita, Naoki Ozato, Tohru Yamaguchi, Motoki Sudo, Yukari Yamashiro, Kenta Mori, Yoshihisa Katsuragi, Takuji Yasukawa, Koichi Murashita, Shigeyuki Nakaji, and et al. 2022. "Association between Objectively Measured Sedentary Behaviour and Sleep Quality in Japanese Adults: A Population-Based Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 5: 3145. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19053145