
Asbestos and Other Hazardous Fibrous Minerals: Potential Exposure Pathways and Associated Health Risks

 , , , , ,
, , , , ,
Abstract
:1. Introduction
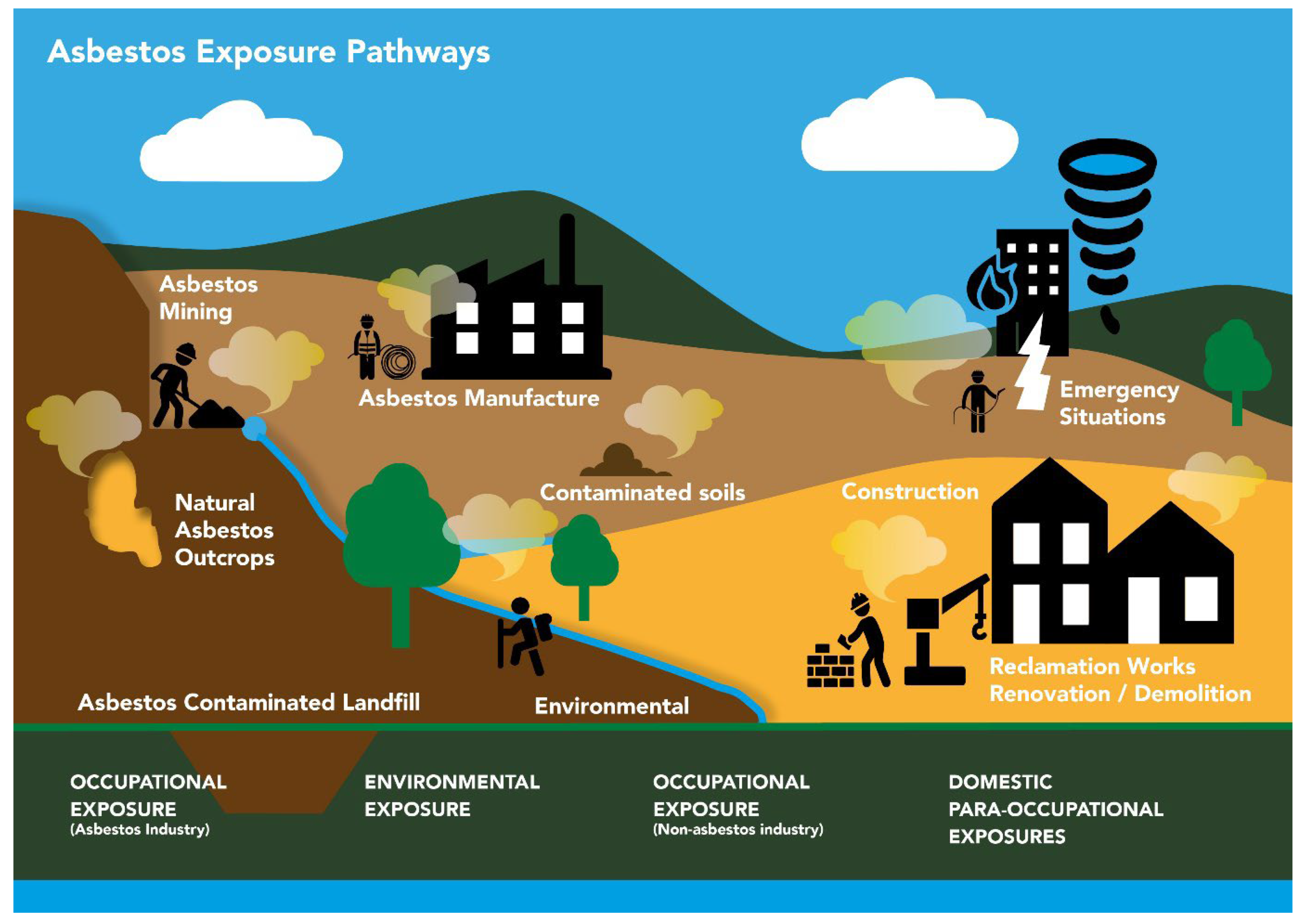
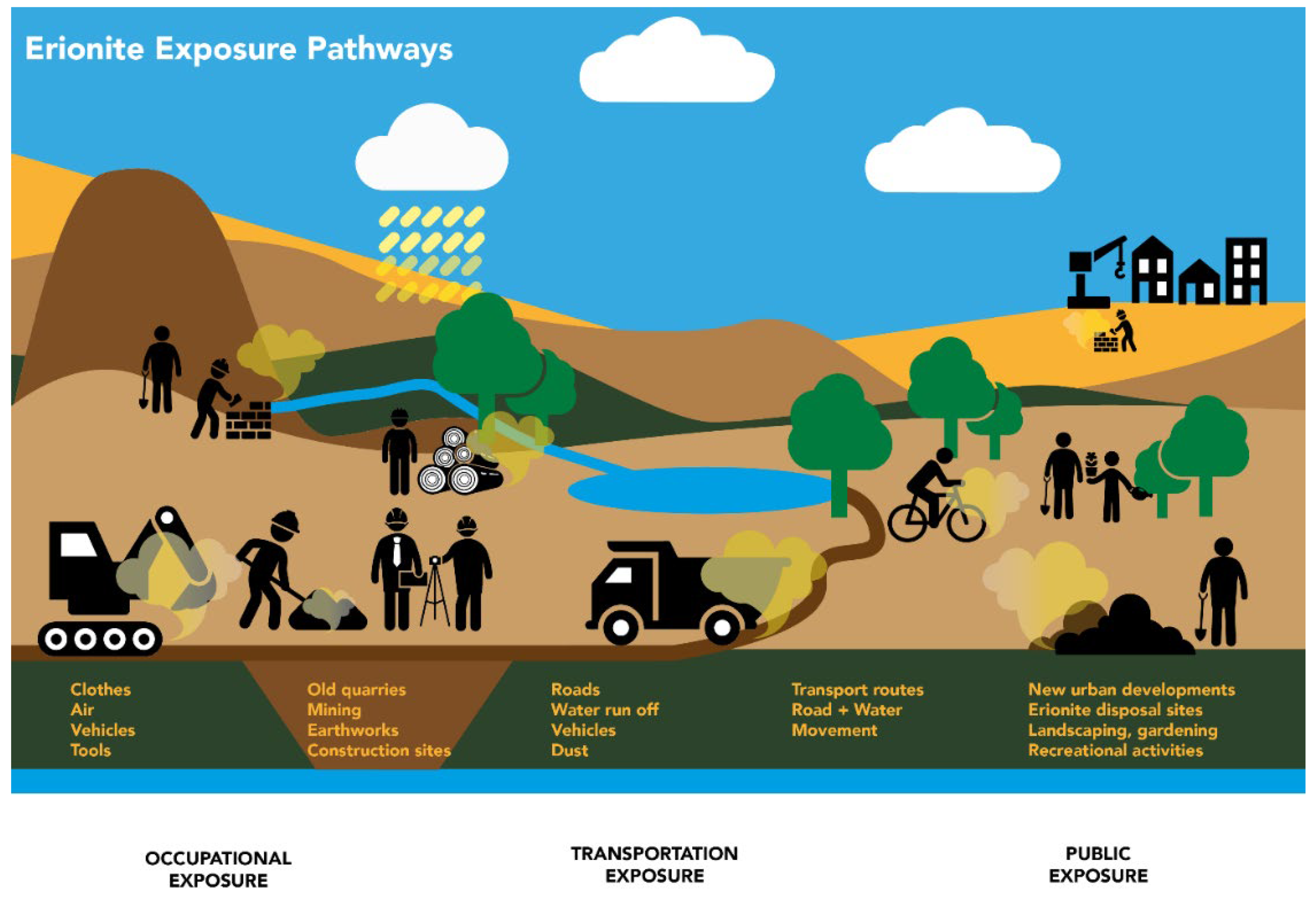
2. Exposure Pathways
2.1. Asbestos
Exposure Pathways
2.2. Other Elongated Mineral Particles (EMPs)
3. Crystallochemistry and Mineralogy of Zeolites
4. Malignant Mesothelioma (MM)
Future Exposure in Urban Areas
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Lin, R.-T.; Soeberg, M.J.; Chien, L.-C.; Fisher, S.; Takala, J.; Lemen, R.; Driscoll, T.; Takahashi, K. Bibliometric analysis of gaps in research on asbestos-related diseases: Declining emphasis on public health over 26 years. BMJ Open 2018, 8, e022806. [Google Scholar] [CrossRef] [PubMed]
- Odgerel, C.O.; Takahashi, K.; Sorahan, T.; Driscoll, T.; Fitzmaurice, C.; Yoko-o, M.; Sawanyawisuth, K.; Furuya, S.; Tanaka, F.; Horie, S.; et al. Estimation of the global burden of mesothelioma deaths from incomplete national mortality data. Occup. Environ. Med. 2017, 74, 851–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jablonski, R.P.; Kim, S.J.; Cheresh, P.; Kamp, D.W. Insights into mineral fibre-induced lung epithelial cell toxicity and pulmonary fibrosis. EMU Notes Mineral. 2017, 18, 447–500. [Google Scholar] [CrossRef]
- National Institute of Safety and Occupational Health (NIOSH). Current Intelligence Bulletin 62: Asbestos Fibres and Other Elongate Mineral Particles: State of the Science and Roadmap for Research. Centres for DISEASE Control and Prevention; DHHS (NIOSH) Publication: Washington, DC, USA, 2011; No. 2011-159.
- Filetti, V.; Vitale, E.; Broggi, G.; Hagnäs, M.P.; Candido, S.; Spina, A.; Lombardo, C. Update of in vitro, in vivo and ex vivo fluoro-edenite effects on malignant mesothelioma: A systematic review. Biomed. Rep. 2020, 13, 60. [Google Scholar] [CrossRef]
- International Agency for Research on Cancer (IARC). Arsenic, metals, fibres and dusts. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC Press: Lyon, France, 2012; Volume 100C. [Google Scholar]
- Bernstein, D.M.; Rogers, R.A.; Sepulveda, R.; Kunzendorf, P.; Bellmann, B.; Ernst, H.; Creutzenberg, O.; Phillips, J.I. Evaluation of the fate and pathological response in the lung and pleura of brake dust alone and in combination with added chrysotile compared to crocidolite asbestos following short-term inhalation exposure. Toxicol. Appl. Pharmacol. 2015, 283, 20–34. [Google Scholar] [CrossRef]
- Linton, A.; Vardy, J.; Clarke, S.; van Zandwijk, N. The ticking timebomb of asbestos: Its insidious role in the development of malignant mesothelioma. Crit. Rev. Oncol. Hematol. 2014, 84, 200–212. [Google Scholar] [CrossRef]
- Belluso, E.; Cavallo, A.; Halterman, D. Crystal Habit of Mineral Fibres. In Mineral Fibres: Crystal Chemistry, Chemical-Physical Properties, Biological Interaction and Toxicity; Gualtieri, A.F., Ed.; Mineralogical Society: London, UK, 2017; Volume 18, pp. 65–109. [Google Scholar] [CrossRef]
- Chatfield, E.J. Measurement of elongate mineral particles: What we should measure and how do we do it? Toxicol. Appl. Pharmacol. 2018, 361, 36–46. [Google Scholar] [CrossRef]
- Veblen, D.R.; Wylie, A.G. Mineralogy of amphiboles and 1:1 layer silicates. In Reviews in Mineralogy and Geochemistry; Guthrie, G.D., Mossman, B.T., Eds.; Mineralogical Society of America: Chantilly, VA, USA, 1993; Volume 28, pp. 61–137. [Google Scholar] [CrossRef]
- U.S. Geological Survey. Mineral Commodity Summaries, January 2021. 2021. Available online: https://pubs.usgs.gov/periodicals/mcs2021/mcs2021-asbestos.pdf (accessed on 10 September 2021).
- Frank, A.L.; Joshi, T.K. The global spread of asbestos. Ann. Glob. Health 2014, 80, 257–262. [Google Scholar] [CrossRef]
- Carlin, D.J.; Larson, T.C.; Pfau, J.C.; Gavett, S.H.; Shukla, A.; Miller, A.; Hines, R. Current research opportunities to address environmental asbestos exposures. Environ. Health Perspect. 2015, 123, 194–197. [Google Scholar] [CrossRef] [Green Version]
- Visonà, S.D.; Capella, S.; Bodini, S.; Borrelli, P.; Villani, S.; Crespi, E.; Frontini, A.; Colosio, C.; Belluso, E. Inorganic fibre lung burden in subjects with occupational and/or anthropogenic environmental asbestos exposure in Broni (Pavia, Northern Italy): An SEM-EDS study on autoptic samples. Int. J. Environ. Res. Public Health 2021, 18, 2053. [Google Scholar] [CrossRef]
- Barrett, J.C. Cellular and molecular mechanisms of asbestos carcinogenicity: Implications for biopersistence. Environ. Health Perspect. 1994, 102 (Suppl. S5), 19–23. [Google Scholar] [CrossRef] [Green Version]
- Carbone, M.; Yang, H. Molecular pathways: Targeting mechanisms of asbestos and erionite carcinogenesis in mesothelioma. Clin. Cancer Res. 2012, 18, 598–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaudino, G.; Xue, J.; Yang, H. How asbestos and other fibres cause mesothelioma. Transl. Lung Cancer Res. 2020, 9 (Suppl. S1), S39–S46. [Google Scholar] [CrossRef] [PubMed]
- Cheresh, P.; Kim, S.; Jablonski, R.P.; Watanabe, S.; Lu, Z.; Chi, M.; Helmin, K.A.; Gius, D.; Budinger, G.R.S.; Kamp, D.W. SIRT3 Overexpression ameliorates asbestos-induced pulmonary fibrosis, mt-DNA damage and lung fibrogenic monocyte recruitment. Int. J. Mol. Sci. 2021, 22, 6856. [Google Scholar] [CrossRef] [PubMed]
- Poole, A.; Brown, R.C.; Turver, C.J.; Skidmore, J.W.; Griffiths, D.M. In vitro genotoxic activities of fibrous erionite. Br. J. Cancer 1983, 47, 697–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gualtieri, A.F.; Gandolfi, N.B.; Pollastri, S.; Burghammer, M.; Tibaldi, E.; Belpoggi, F.; Pollok, K.; Langenhorst, F.; Vigliaturo, R.; Dražić, G. New insights into the toxicity of mineral fibres: A combined in situ synchrotron μ-XRD and HR-TEM study of chrysotile, crocidolite, and erionite fibres found in the tissues of Sprague-Dawley rats. Toxicol. Lett. 2017, 274, 20–30. [Google Scholar] [CrossRef]
- Wagner, J.C.; Skidmore, J.W.; Hill, R.J.; Griffiths, D.M. Erionite exposure and mesotheliomas in rats. Br. J. Cancer 1985, 51, 727–730. [Google Scholar] [CrossRef] [Green Version]
- Van Gosen, B.S.; Blitz, T.A.; Plumlee, G.S.; Meeker, G.P.; Pierson, P.M. Geologic occurrences of erionite in the United States: An emerging national public health concern for respiratory disease. Environ. Geochem. Health 2013, 35, 419–430. [Google Scholar] [CrossRef]
- Giacobbe, C.; Wright, J.; Dejoie, C.; Tafforeau, P.; Berruyer, C.; Vigliaturo, R.; Gieré, R.; Gualtieri, A.F. Depicting the crystal structure of fibrous ferrierite from British Columbia using a combined synchrotron techniques approach. J. Appl. Crystallogr. 2019, 52, 1397–1408. [Google Scholar] [CrossRef]
- Gualtieri, A.F.; Gandolfi, N.B.; Passaglia, E.; Pollastri, S.; Mattioli, M.; Giordani, M.; Ottaviani, M.F.; Cangiotti, M.; Bloise, A.; Barca, D.; et al. Is fibrous ferrierite a potential health hazard? Characterization and comparison with fibrous erionite. Am. Mineral. 2018, 103, 1044–1055. [Google Scholar] [CrossRef]
- National Research Council (NRC); Committee on Nonoccupational Health Risks of Asbestiform Fibres; Board on Toxicology and Environmental Health Hazards. Asbestiform Fibres: Nonoccupational Health Risks; National Academy Press: Washington, DC, USA, 1984. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/books/NBK216748/pdf/Bookshelf_NBK216748.pdf (accessed on 20 September 2021).
- Wright, W.W.; Rom, W.N.; Moatamed, F. Characterisation of zeolite fibre sizes using scanning electron microscopy. Arch. Environ. Occup. Health 1983, 38, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Ilgren, E.B.; Kazemian, H.; Hoskins, J.A. Kandovan the next ‘Capadoccia’? A potential public health issue for erionite related mesothelioma risk. Epidemiol. Biostatics Public Health 2015. [Google Scholar] [CrossRef]
- Ballirano, P.; Andreozzi, G.B.; Dogan, M.; Dogan, A.U. Crystal structure and iron topochemistry of erionite-K from Rome, Oregon, U.S.A. Am. Mineral. 2009, 94, 1262–1270. [Google Scholar] [CrossRef]
- Coffin, D.L.; Cook, P.M.; Creason, J.P. Relative mesothelioma induction in rats by mineral fibres: Comparison with residual pulmonary mineral fibre number and epidemiology. Inhal. Toxicol. 1992, 4, 273–300. [Google Scholar] [CrossRef]
- Marantos, I.; Christidis, G.E.; Ulmanu, M. Zeolite formation and deposits. In Handbook of Natural Zeolites; Inglezakis, V.J., Zorpas, A.A., Eds.; Bentham Science Publishers: Sharjah, United Arab Emirates, 2012; pp. 28–51. [Google Scholar] [CrossRef] [Green Version]
- Christie, A.B.; Brathwaite, R.L.; Thompson, B.N. Mineral Commodity Report 23—Zeolites. N. Z. Min. 2002, 31, 16–24. [Google Scholar]
- Diale, P.P.; Muzenda, E.; Zimba, J. A study of South African natural zeolites properties and applications. In Proceedings of the World Congress on Engineering and Computer Science 2011, Vol II, WCECS 2011, San Francisco, CA, USA, 19–21 October 2011. [Google Scholar]
- Batiashvili, T.V.; Gvakharia, G.V. Erionite found for the first time in Georgia. Dokl. Russ. Acad. Sci. Earth Sci. Sect. 1968, 179, 122–124. [Google Scholar]
- Lehtinen, M. Lake Lappajärvi, a Meteorite Impact Site in Western Finland. Geological Survey of Finland Bulletin; Geologinen tutkimuslaitos: Espoo, Finland, 1976; Volume 282, pp. 1–92. [Google Scholar]
- Tschernick, R.W. Zeolites of the World; Geoscience Press Inc: Phoenix, AZ, USA, 1992. [Google Scholar]
- Carbone, M.; Baris, Y.I.; Bertino, P.; Brass, B.; Comertay, S.; Dogan, A.U.; Gaudino, G.; Jube, S.; Kanodia, S.; Partridge, C.R.; et al. Erionite exposure in North Dakota and Turkish villages with mesothelioma. Proc. Natl. Acad. Sci. USA 2011, 108, 13618–13623. [Google Scholar] [CrossRef] [Green Version]
- Galli, E.; Quartieri, S.; Vezzalini, G.; Alberti, A. Gottardiite, a new high-silica zeolite from Antarctica: The natural counterpart of synthetic NU-87. Eur. J. Minerol. 1996, 8, 687–693. [Google Scholar] [CrossRef] [Green Version]
- Surdam, R.C.; Eugster, H.P. Mineral reactions in the sedimentary deposits of the Lake Magadi region, Kenya. Geol. Soc. Am. Bull. 1976, 87, 1739–1752. [Google Scholar] [CrossRef]
- Noh, J.H.; Kim, S.J. Zeolites from tertiary tuffaceous rocks in Yeongil area, Korea. Stud. Surf. Sci. Catal. 1986, 28, 59–66. [Google Scholar]
- Passaglia, E.; Artioli, G.; Gualtieri, A. Crystal chemistry of the zeolites erionite and offretite. Am. Mineral. 1998, 83, 577–589. [Google Scholar] [CrossRef]
- Suprychev, V.A.; Prokhorov, I.G. Erionite from keratophyre volkanites of the Karadag Reserve in the Crimea. Mineral. Sb. 1986, 40, 85–88. [Google Scholar]
- Kirov, G.; Samajova, E.; Nedialkov, R.; Stanimirova, T.S. Alteration processes and products of acid pyroclastic rocks in Bulgaria and Slovakia. Clay Miner. 2011, 46, 279–294. [Google Scholar] [CrossRef]
- Saracci, R. Erionite and cancer in a Mexican village. Occup. Environ. Med. 2015, 72, 163–164. [Google Scholar] [CrossRef] [PubMed]
- Giordani, M.; Mattioli, M.; Ballirano, P.; Pacella, A.; Cenni, M.; Boscardin, M.; Valentini, L. Geological occurrence, mineralogical characterisation, and risk assessment of potentially carcinogenic erionite in Italy. Toxicol. Environ. Health Part B Crit. Rev. 2017, 20, 81–103. [Google Scholar] [CrossRef] [PubMed]
- Mattioli, M.; Giordani, M.; Arcangeli, P.; Valentini, L.; Boscardin, M.; Pacella, A.; Ballirano, P. Prismatic to asbestiform offretite from Northern Italy: Occurrence, morphology and crystal-chemistry of a new potentially hazardous zeolite. Minerals 2018, 8, 69. [Google Scholar] [CrossRef] [Green Version]
- Sahmel, J.; Barlow, C.A.; Simmons, B.; Gaffney, S.H.; Avens, H.J.; Madl, A.K.; Henshaw, J.; Lee, R.J.; Van Orden, D.; Sanchez, M.; et al. Evaluation of Take-Home Exposure and Risk Associated with the Handling of Clothing Contaminated with Chrysotile Asbestos. Risk Anal. 2014, 34, 1448–1468. [Google Scholar] [CrossRef]
- Kazan-Allen, L. Chronology of National Asbestos Bans. 2019. Available online: http://www.ibasecretariat.org/chron_ban_list.php (accessed on 9 September 2021).
- Rake, C.; Gilham, C.; Hatch, J.; Darnton, A.; Hodgson, J.; Peto, J. Occupational, domestic and environmental mesothelioma risks in the British population: A case-control study. Br. J. Cancer 2009, 100, 1175–1183. [Google Scholar] [CrossRef] [Green Version]
- Scarselli, A.; Marinaccio, A.; Corfiati, M.; Di Marzio, D.; Iavicoli, S. Occupational asbestos exposure after the ban: A job exposure matrix developed in Italy. Eur. J. Public Health 2020, 30, 936–941. [Google Scholar] [CrossRef]
- Bard, D.; Burdett, G. Exposure of UK Industrial Plumbers to Asbestos, Part II: Awareness and Responses of Plumbers to Working with Asbestos During a Survey in Parallel with Personal Sampling. Ann. Occup. Hyg. 2007, 51, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.; Cherrie, J.W.; Rao, B.; Asolekar, S.R. Assessment of the future mesothelioma disease burden from past exposure to asbestos in ship recycling yards in India. Int. J. Hyg. Environ. Health 2020, 225, 113478. [Google Scholar] [CrossRef] [PubMed]
- Lemen, R.A.; Landrigan, P.J. Sailors and the Risk of Asbestos-Related Cancer. Int. J. Environ. Res. Public Health 2021, 18, 8417. [Google Scholar] [CrossRef] [PubMed]
- Wallis, S.L.; Emmett, E.A.; Hardy, R.; Casper, B.B.; Blanchon, D.J.; Testa, J.R.; Menges, C.W.; Gonneau, C.; Jerolmack, D.J.; Seiphoori, A.; et al. Challenging global waste management—bioremediation to detoxify asbestos. Front. Environ. Sci. 2020, 8, 20. [Google Scholar] [CrossRef] [Green Version]
- Landrigan, P.J. The third wave of asbestos disease: Exposure to asbestos in place—Public health control. Introduction. Ann. N. Y. Acad. Sci. 1991, 643. [Google Scholar] [CrossRef] [PubMed]
- Olsen, N.J.; Franklin, P.J.; Reid, A.; De Klerk, N.H.; Threlfall, T.J.; Shilkin, K.; Musk, B. Increasing incidence of malignant mesothelioma after exposure to asbestos during home maintenance and renovation. Med. J. Aust. 2011, 195, 271–274. [Google Scholar] [CrossRef]
- WorkSafe. Approved Code of Practice: Management and Removal of Asbestos. 2016. Available online: https://www.worksafe.govt.nz/topic-and-industry/asbestos/management-and-removal-of-asbestos/ (accessed on 9 September 2021).
- National Occupational Health and Safety Commission (NOHSC). Code of Practice for the Management and Control of Asbestos in Workplaces. 2005. Available online: https://www.safetyusb.online/documents/Asbestos/SAFEWORKAUSTRALIA-COP-MgtControlofAsbestosInTheWorkplace_NOHSC2018-2005_PDF.pdf (accessed on 9 September 2021).
- Lee, R.J.; Van Orden, D.R. Airborne asbestos in buildings. Regul. Toxicol. Pharmacol. 2008, 50, 218–225. [Google Scholar] [CrossRef]
- Lee, E.S.; Kim, Y.K. Asbestos Exposure Level and the Carcinogenic Risk Due to Corrugated Asbestos-Cement Slate Roofs in Korea. Int. J. Environ. Res. Public Health 2021, 18, 6925. [Google Scholar] [CrossRef]
- Campopiano, A.; Casciardi, S.; Fioravanti, F.; Ramires, D. Airborne asbestos levels in school buildings in Italy. J. Occup. Environ. Hyg. 2004, 1, 256–261. [Google Scholar] [CrossRef]
- Pastuszka, J.S. Emission of airborne fibers from mechanically impacted asbestos-cement sheets and concentration of fibrous aerosol in the home environment in Upper Silesia, Poland. J. Hazard. Mater. 2009, 162, 1171–1177. [Google Scholar] [CrossRef]
- Bourgault, M.H.; Gagne, M.; Valcke, M. Lung cancer and mesothelioma risk assessment for a population environmentally exposed to asbestos. Int. J. Hyg. Environ. Health 2014, 217, 340–346. [Google Scholar] [CrossRef]
- Marsh, G.M.; Riordan, A.S.; Keeton, K.A.; Benson, S.M. Non-occupational exposure to asbestos and risk of pleural mesothelioma: Review and meta-analysis. Occup. Environ. Med. 2017, 74, 838–846. [Google Scholar] [CrossRef] [PubMed]
- Ballirano, P.; Cametti, G. Crystal chemical and structural modifications of erionite fibres leached with simulated lung fluids. Am. Mineral. 2015, 100, 1003–1012. [Google Scholar] [CrossRef]
- Bertino, P.; Marconi, A.; Palumbo, L.; Bruni, M.; Barbone, D.; Germano, S.; Dogan, A.U.; Tassis, G.F.; Porta, C.; Mutti, L.; et al. Erionite and asbestos differently cause transformation of human mesothelial cells. Int. J. Cancer 2007, 121, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Ilgren, E.B.; Pooley, F.D.; Larragoitiac, J.C.; Talamantes, M.; Navarretee, G.L.; Krauss, E.; Brena, A.F. First confirmed erionite related mesothelioma in North America. Indoor Built Environ. 2008, 17, 567–568. [Google Scholar] [CrossRef]
- Dogan, A.U.; Baris, Y.I.; Dogan, M.; Emri, S.; Steele, I.; Elmishad, A.G.; Carbone, M. Genetic predisposition to fibre carcinogenesis causes a mesothelioma epidemic in Turkey. Cancer Res. 2006, 66, 5063–5068. [Google Scholar] [CrossRef] [Green Version]
- Metintas, M.; Hillerdal, G.; Metintas, S.; Dumortier, P. Endemic malignant mesothelioma: Exposure to erionite is more important than genetic factors. Arch. Environ. Occup. Health 2010, 65, 86–93. [Google Scholar] [CrossRef]
- Beaucham, C.; King, B.; Feldmann, K.; Harper, M.; Dozier, A. Assessing occupational erionite and respirable crystalline silica exposure among outdoor workers in Wyoming, South Dakota, and Montana. J. Occup. Environ. Hyg. 2018, 15, 455–465. [Google Scholar] [CrossRef]
- Wagner, J.C. Health hazards of substitutes. In Asbestos, Health & Safety, Proceedings of the World Symposium on Asbestos, Montreal, QC, Canada, 25–27 May 1982; Canadian Asbestos Information Centre: Ottawa, ON, Canada, 1982. [Google Scholar]
- Baumann, F.; Maurizot, P.; Mangeas, M.; Ambrosi, J.P.; Douwes, J.; Robineau, B. Pleural mesothelioma in New Caledonia: Associations with environmental risk factors. Environ. Health Perspect. 2011, 119, 695–700. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, C.; Buck, B.; Miller, A.; Lockey, J.; Weis, C.; Weissman, D.; Jonesi, A.; Ryan, P. Exposure to naturally occurring mineral fibres due to off-road vehicle use: A review. Int. J. Hyg. Environ. Health 2017, 220, 1230–1241. [Google Scholar] [CrossRef]
- Matassa, R.; Familiari, G.; Relucenti, M.; Battaglione, E.; Downing, C.; Pacella, A.; Cametti, G.; Ballirano, P. A deep look into erionite fibres: An electron microscopy investigation of their self-assembly. Sci. Rep. 2015, 5, 16757. [Google Scholar] [CrossRef] [Green Version]
- Brook, M.S.; Black, P.M.; Salmond, J.; Dirks, K.N.; Berry, T.-A.; Steinhorn, G. Erionite in Auckland bedrock and malignant mesothelioma: An emerging public and occupational health hazard? N. Z. Med. J. 2020, 133, 73–78. [Google Scholar] [PubMed]
- Gottardi, G.; Galli, E. General Information on Zeolites. In Natural Zeolites; Springer: Berlin/Heidelberg, Germany, 1985; pp. 1–34. [Google Scholar] [CrossRef]
- Klein, C. Rocks, minerals and a dusty world. In Health Effects of Mineral Dusts; Guthrie, G.D., Mossman, B.T., Eds.; Mineralogical Society of America: Berlin, Germany; Boston, MA, USA, 1993; Volume 28, pp. 7–59. [Google Scholar]
- Regis, A.J. Occurrences of ferrierite in altered pyroclastics in central Nevada. Geol. Soc. Am. Abstr. Programs 1970, 2, 661. [Google Scholar]
- Wise, W.S.; Tschernick, R.W. Chemical composition of ferrierite. Am. Mineral. 1976, 61, 60–66. [Google Scholar]
- Vaughan, P.A. The crystal structure of the zeolite ferrierite. Acta Crystallogr. 1966, 21, 983–990. [Google Scholar] [CrossRef]
- Meier, W.M. Zeolite structures. In S.C.I. Monograph, Molecular Sieves; Society of the Chemical Industry: London, UK, 1968; pp. 10–27. [Google Scholar]
- Smith, B.K. Variations in the framework structure of the zeolite ferrierite. Am. Mineral. 1986, 71, 989–998. [Google Scholar]
- Galli, E.; Passaglia, E.; Pongiluppi, D.; Rinaldi, R. Mazzite, a new mineral, the natural counterpart of the synthetic zeolite. Contrib. Mineral. Petrol. 1974, 45, 99–105. [Google Scholar] [CrossRef]
- Deer, A.; Howie, R.; Wise, W.S.; Zussman, J. Rock Forming Minerals. Rock Forming Minerals. Volume 4B. Framework Silicates: Silica Minerals. In Feldspathoids and the Zeolites; The Geological Society: London, UK, 2004. [Google Scholar]
- Galli, E. The crystal structure of roggianite, a zeolite-like silicate. In Proceedings of the 5th International Conference of Zeolites, Naples, Italy, 2–6 June 1980; pp. 205–213. [Google Scholar]
- Passaglia, E.; Vezzalini, G. Roggianite: Revised chemical formula and zeolitic properties. Mineral. Mag. 1988, 52, 201–206. [Google Scholar] [CrossRef]
- Amin, W.; Linkov, F.; Landsittel, D.P.; Silverstein, J.C.; Bshara, W.; Gaudioso, C.; Feldman, M.D.; Pass, H.I.; Melamed, J.; Friedberg, J.S.; et al. Factors influencing malignant mesothelioma survival: A retrospective review of the National Mesothelioma Virtual Bank cohort. F1000 Res. 2018, 7, 1184. [Google Scholar] [CrossRef]
- Carbone, M.; Ly, B.H.; Dodson, R.F.; Pagano, I.; Morris, P.T.; Dogan, U.A.; Gazdar, A.F.; Pass, H.; Yang, H. Malignant mesothelioma: Facts, myths and hypotheses. J. Cell. Physiol. 2011, 227, 44–58. [Google Scholar] [CrossRef] [Green Version]
- Povtak, T. Canada Closing Its Chrysotile Institute, Signaling End of Country’s Asbestos Industry. 2012. Available online: https://www.asbestos.com/news/2012/04/30/canada-chrysotile-institute-asbestos/ (accessed on 20 September 2021).
- Ruff, K. How Canada changed from exporting asbestos to banning asbestos: The challenges that had to be overcome. Int. J. Environ. Res. Public Health 2017, 14, 1135. [Google Scholar] [CrossRef] [Green Version]
- Bianchi, C.; Bianchi, T.; Tommasi, M. Mesothelioma of the pleura in the Province of Trieste. Med. Lav. 2007, 98, 374–380. [Google Scholar] [PubMed]
- Kjellstrom, T. Increased mesothelioma incidence in New Zealand: The asbestos-cancer epidemic has started. N. Z. Med. J. 2000, 113, 485–490. [Google Scholar]
- Australian Institute of Health & Welfare (AIHW). Mesothelioma in Australia 2018. Safe Work Australia, Australian Government. 2019. Available online: https://www.aihw.gov.au/getmedia/7df8ff10-d0b7-4d42-881b-76647a9263ef/aihw-can-130-infocus_1.pdf.aspx?inline=true (accessed on 8 September 2021).
- World Health Organization (WHO). Chemical Safety and Health—Asbestos. 2020. Available online: https://www.who.int/teams/environment-climate-change-and-health/chemical-safety-and-health/health-impacts/chemicals/asbestos (accessed on 20 October 2020).
- Robinson, B.M. Malignant pleural mesothelioma: An epidemiological perspective. Ann. Cardiothorac. Surg. 2012, 1, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Santana, V.S.; Salvi, L.; Cavalcante, F.; Campos, F.; Algranti, E. Underreporting of mesothelioma, asbestosis and pleural plaques in Brazil. Occup. Med. 2021, 71, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Z.; Ruan, J.; Zheng, Y.; Xiang, D.; Li, N.; Hu, J.; Shen, J.; Deng, Y.; Yao, J.; Zhao, P.; et al. Assessment of Global Trends in the Diagnosis of Mesothelioma From 1990 to 2017. JAMA Netw. Open 2021, 4, e2120360. [Google Scholar] [CrossRef]
- Delgermaa, V.; Takahashi, K.; Park, E.-K.; Le, G.V.; Hara, T.; Sorathan, T. Global mesothelioma deaths reported to the World Health Organization between 1994 and 2008. Bull. World Health Organ. 2011, 89, 716–724. [Google Scholar] [CrossRef]
- Franz, F. Study Revisits Health Risk of Chrysotile: Why Is This Still a Debate in 2013? 2013. Available online: https://www.asbestos.com/news/2013/02/01/health-risk-of-chrysotile/ (accessed on 10 September 2021).
- Health & Safety Executive (HSE). Mesothelioma Statistics for Great Britain, 2019. 2019. Available online: https://www.hse.gov.uk/Statistics/causdis/mesothelioma/mesothelioma.pdf. (accessed on 10 September 2021).
- Selby, K. Mesothelioma in Canada. 2021. Available online: https://www.asbestos.com/mesothelioma/canada/ (accessed on 9 September 2021).
- Bray, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Zanetti, R.; Ferlay, J. (Eds.) Cancer Incidence in Five Continents, Vol. XI; IARC Scientific Publication No. 166; International Agency for Research on Cancer: Lyon, France, 2021; Available online: https://publications.iarc.fr/597 (accessed on 17 September 2021).
- Zhao, J.; Zuo, T.; Zheng, R.; Zhang, S.; Zeng, H.; Xia, C.; Yang, Z.; Chen, W. Epidemiology and trend analysis on malignant mesothelioma in China. Chin. J. Cancer 2017, 29, 361–368. [Google Scholar] [CrossRef] [Green Version]
- Schonfeld, S.J.; McCormack, V.; Rutherford, M.J.; Schüz, J. Regional variations in German mesothelioma mortality rates: 2000–2010. Cancer Causes Control 2014, 25, 615–624. [Google Scholar] [CrossRef]
- Robert Koch Institut. Cancer in Germany 2015/2016. 2020. Available online: https://www.krebsdaten.de/Krebs/EN/Content/Publications/Cancer_in_Germany/cancer_chapters_2015_2016/cancer_germany_2015_2016.pdf?__blob=publicationFile (accessed on 18 March 2022).
- Vigliaturo, R.; Ventura, G.D.; Choi, J.K.; Marengo, A.; Lucci, F.; O’Shea, M.J.; Perez-Rodriguez, I.; Giere, R. Mineralogical characterization and dissolution experiments in Gamble’s solution of tremolitic amphibole from Passo di Caldenno (Sondrio, Italy). Minerals 2018, 8, 557. [Google Scholar] [CrossRef] [Green Version]
- Vigliaturo, R.; Choi, J.K.; Pérez-Rodriguez, I.; Gieré, R. Dimensional distribution control of elongate mineral particles for their use in biological assays. MethodsX 2020, 7, 100937. [Google Scholar] [CrossRef]
- Vigliaturo, R.; Elkassas, S.M.; Ventura, G.D.; Redhammer, G.J.; Ruiz-Zepeda, F.; O’Shea, M.J.; Drazic, G.; Giere, R. Multi-scale characterization of glaucophane from Chiavolino (Biella, Italy): Implications for international regulations on elongate mineral particles. Eur. J. Mineral. 2021, 33, 77–112. [Google Scholar] [CrossRef] [PubMed]
- Stanton, M.F.; Layard, M.; Tegeris, A.; Miller, E.; May, M.; Morgan, E.; Smith, A. Relation of particle dimension to carcinogenicity in amphibole asbestoses and other fibrous minerals. J. Natl. Cancer Inst. 1981, 67, 965–975. [Google Scholar] [PubMed]
- Nolan, R.P.; Langer, A.M. Limitations of the Stanton hypothesis. Rev. Mineral. 1993, 28, 309–326. [Google Scholar]
- Baris, Y.I.; Sahin, A.A.; Ozesmi, M.; Kerse, I.; Ozen, E.; Kolacan, B.; Altinörs, M.; Göktepeli, A. An outbreak of pleural mesothelioma and chronic fibrosing pleurisy in the village of Karain/Urgüp in Anatolia. Thorax 1978, 33, 181–192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baris, Y.I.; Saracci, R.; Simonato, L.; Skidmore, J.W.; Artvinli, M. Malignant mesothelioma and radiological chest abnormalities in two villages in Central Turkey. An epidemiological and environmental investigation. Lancet 1981, 1, 984–987. [Google Scholar] [CrossRef]
- Niklinski, J.; Niklinska, W.; Chyczewska, E.; Laudanski, J.; Naumnik, W.; Chyczewski, L.; Pluygers, E. The epidemiology of asbestos-related diseases. Lung Cancer 2004, 45 (Suppl. S1), S7–S15. [Google Scholar] [CrossRef] [PubMed]
- Roushdy-Hammady, I.; Siegel, J.; Emri, S.; Testa, J.R.; Carbone, M. Genetic-susceptibility factor and malignant mesothelioma in the Cappadocian region of Turkey. Lancet 2001, 357, 444–445. [Google Scholar] [CrossRef]
- Testa, J.R.; Cheung, M.; Pei, J.; Below, J.E.; Tan, Y.; Sementino, E.; Cox, N.J.; Dogan, A.U.; Pass, H.I.; Trusa, S.; et al. Germline BAP1 mutations predispose to malignant mesothelioma. Nat. Genet. 2011, 43, 1022–1025. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Kadariya, Y.; Cheung, M.; Pei, J.; Talarchek, J.; Sementino, E.; Tan, Y.; Menges, C.W.; Cai, K.Q.; Litwin, S.; et al. Germline mutation of Bap1 accelerates development of asbestos-induced malignant mesothelioma. Cancer Res. 2014, 74, 4388–4397. [Google Scholar] [CrossRef] [Green Version]
- Emmett, E.A. Asbestos in high-risk communities: Public health implications. Int. J. Environ. Res. Public Health 2021, 18, 1579. [Google Scholar] [CrossRef]
- Carbone, M.; Emri, S.; Dogan, A.U.; Steele, I.; Tuncer, M.; Pass, H.I.; Baris, Y.I. A mesothelioma epidemic in Cappadocia: Scientific developments and unexpected social outcomes. Nat. Rev. Cancer 2007, 7, 147–154. [Google Scholar] [CrossRef] [PubMed]
- Paoletti, L.; Batisti, D.; Bruno, C.; Di Paola, M.; Gianfagna, A.; Mastrantonio, M.; Nesti, M.; Comba, P. Unusually high incidence of malignant pleural mesothelioma in a town in eastern Sicily: An epidemiological and environmental study. Arch. Environ. Occup. Health 2000, 55, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.L.; Day, H.W.; Wang, W.; Beckett, L.A.; Schenker, M.B. Residential proximity to naturally occurring asbestos and mesothelioma risk in California. Am. J. Respir. Crit. Care Med. 2005, 172, 1019–1025. [Google Scholar] [CrossRef] [Green Version]
- Maher, B. Epidemiology: Fear in the dust. Nature 2010, 468, 884–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jurinski, J.B.; Jurinski, N.B. A proposed control limit for exposure to airborne erionite fibres. Appl. Occup. Environ. Hyg. 1997, 12, 429–434. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Location | Erionite Form/Species | Evidence of MM? | Main Exposure Pathways Highlighted |
|---|---|---|---|
| Rome, Oregon, USA | Fibrous, Erionite-K, Erionite-Na, Fe-free [65] | Test organisms (rats) only | Low population density, no exposure described [66] |
| Zacatecas and Jalisco, Mexico | Not specified | Yes, human fatalities. Erionite confirmed in lung tissue of one MM case [67] | Adobe bricks and terraces [44]; agricultural tilling [67] |
| Karlik, Cappadocia, Turkey | Fibrous, Erionite-K [68] | Yes, human fatalities; low rate compared to neighbouring Karain [69] | General low concentration; environmental exposure suggested responsible for the relatively low incidence rate of MM in Karlik [69] |
| Karain, Cappadocia, Turkey | Fibrous, Erionite-K [68] | Yes, human fatalities at extremely high rate [69] | Living in houses built of materials containing erionite nodules [69] |
| East Gate, Nevada, USA | Not specified | Not specified | Not specified |
| Dunn County, North Dakota, USA | Not specified | No | Gravel used as building materials, e.g., non-paved roads [65] |
| Wyoming, South Dakota and Montana, USA | Fibrous, form not specified | No | Campground maintenance, universal terrain vehicle use, tree surgery, digging [70] |
| Northern Italy, Lessini Mountain area | Fibrous and asbestiform, Erionite-Ca predominantly with Na and K [45] | Elevated MM rates in the general region, but no detailed epidemiological study yet [45] | Mining, quarrying and construction materials [45] |
| Kandovan, Iran | Fibrous, form not specified | No | Construction and inhabitation of cave dwellings and agricultural use suspected [28] |
| New Caledonia | Not specified | Not specified | Not specified |
| New Zealand | Not specified | Test organisms (rats) | Not specified [71] |
| Country | No. MM Deaths per Year | Ave. Age at Diagnosis (Years) | Percentage of Population (% × 10−4) | No. of MM Cases Cases per Year Timeframe | |
|---|---|---|---|---|---|
| New Zealand | 100–170 ^ | 50–60 * | 23.4–39.8 (2008) | 1.8–33 | 1971–1996 |
| USA | 3000 | 65–74 | 7.6 (2011) | 3200 +,** | 2003–2008 |
| Australia | 757 | 70–79 | 31.0 (2016) | 135–631 | 1982–2017 * |
| UK | 2500 | 75–79 * | 37.4 (2017) | 1164–2526 | 1982–2015 * |
| Canada | 515 | 60 | 15.1 (2010) | 153–344 | 1984–2003 |
| China | 1659 | N/A # | 1.2 (2013) | 2041 | 2013 |
| Brazil | 142 | N/A | 0.7 (2010) | N/A | 2008–2014 |
| Germany | 1480 | 74–75 | 18.0 (2016) | 1340 | 2016 |
| Netherlands | 481–1000 | N/A # | 29.0–60.2 (2010) | 2587 | 2008–2012 |
| World | 47,000 | - | 6.7 (2011) | 3718–9993 ** | 1994–2008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berry, T.-A.; Belluso, E.; Vigliaturo, R.; Gieré, R.; Emmett, E.A.; Testa, J.R.; Steinhorn, G.; Wallis, S.L. Asbestos and Other Hazardous Fibrous Minerals: Potential Exposure Pathways and Associated Health Risks. Int. J. Environ. Res. Public Health 2022, 19, 4031. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19074031
Berry T-A, Belluso E, Vigliaturo R, Gieré R, Emmett EA, Testa JR, Steinhorn G, Wallis SL. Asbestos and Other Hazardous Fibrous Minerals: Potential Exposure Pathways and Associated Health Risks. International Journal of Environmental Research and Public Health. 2022; 19(7):4031. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19074031
Chicago/Turabian StyleBerry, Terri-Ann, Elena Belluso, Ruggero Vigliaturo, Reto Gieré, Edward A. Emmett, Joseph R. Testa, Gregor Steinhorn, and Shannon L. Wallis. 2022. "Asbestos and Other Hazardous Fibrous Minerals: Potential Exposure Pathways and Associated Health Risks" International Journal of Environmental Research and Public Health 19, no. 7: 4031. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19074031