
Bullied Because of Their Teeth: Evidence from a Longitudinal Study on the Impact of Oral Health on Bullying Victimization among Australian Indigenous Children



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
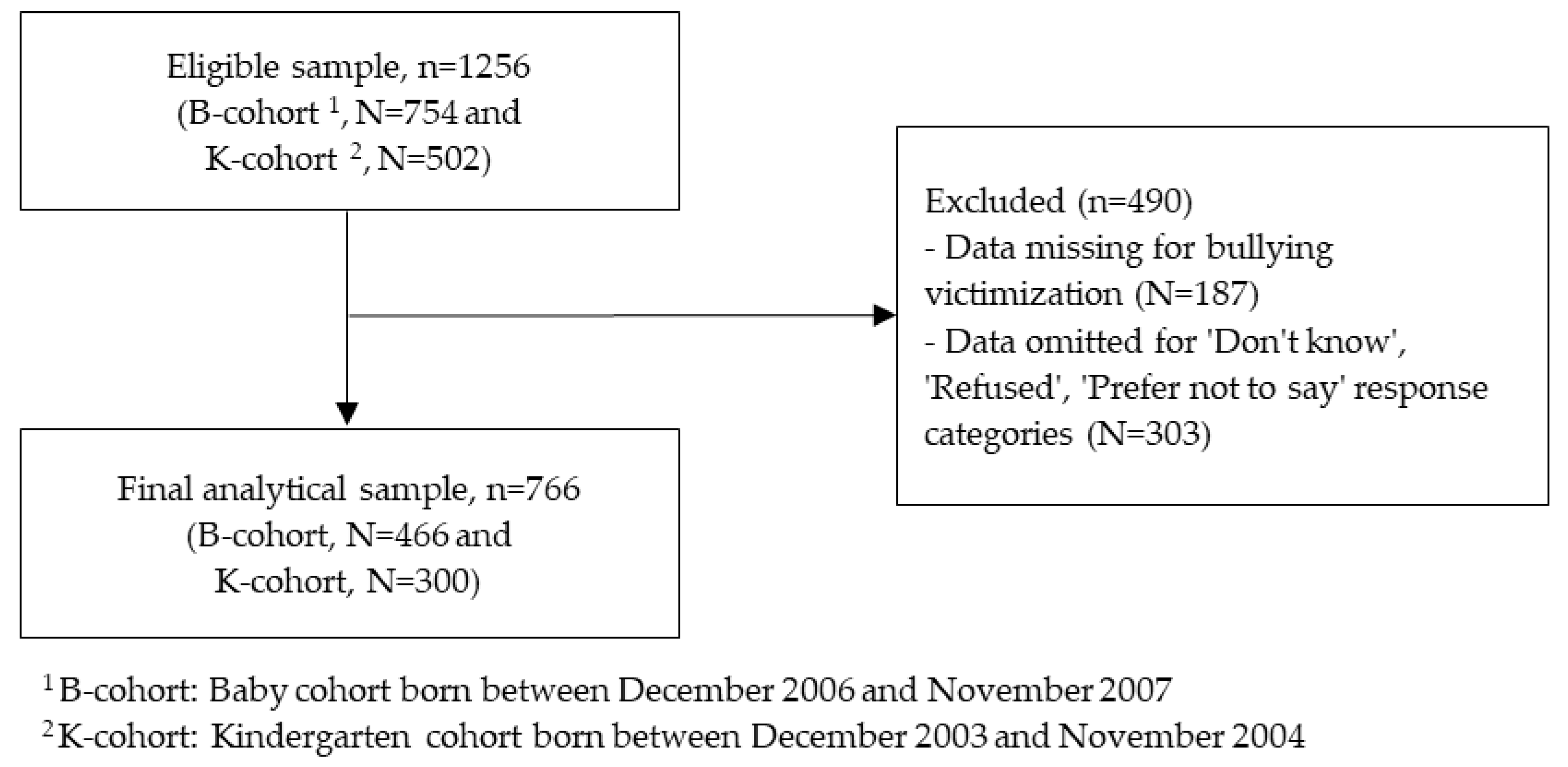
2.2. Participants
2.3. Measures
2.4. Data Analyses
3. Results
3.1. Sample Characteristics
3.2. Prevalence of Bullying and Dental Problems
3.3. Bivariate Relationships between Explanatory Variables and Bullying Victimization
3.4. Logistic Models for the Odds of Bullying Victimization
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hunt, J.; Smith, D. Strengthening Indigenous Community Governance: A Step towards Advancing Reconciliation in Australia. 2018. Available online: https://openresearch-repository.anu.edu.au/handle/1885/148930 (accessed on 3 September 2021).
- Commonwealth of Australia. National Strategic Framework for Aboriginal and Torres Strait Islander Peoples’ Mental Health and Social and Emotional Wellbeing; Department of the Prime Minister and Cabinet, Australian Government: Canberra, Australia, 2017.
- Gee, G.; Dudgeon, P.; Schultz, C.; Hart, A.; Kelly, K. Aboriginal and Torres Strait Islander social and emotional wellbeing. Work. Together Aborig. Torres Strait Isl. Ment. Health Wellbeing Princ. Pract. 2014, 2, 55–68. [Google Scholar]
- Dudgeon, P.B.S.; Bray, A.; Calma, T.; McPhee, R.; Ring, I. Connection between Family, Kinship and Social and Emotional Wellbeing; Australian Institute of Health and Welfare: Canberra, Australia, 2021.
- Miller, H.M.; Young, C.; Nixon, J.; Talbot-McDonnell, M.; Cutmore, M.; Tong, A.; Craig, J.C.; Woolfenden, S. Parents’ and carers’ views on factors contributing to the health and wellbeing of urban Aboriginal children. Aust. New Zealand J. Public Health 2020, 44, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Jamieson, L.; MacRae, A.; Gray, A. Review of Indigenous oral Health. 2011. Available online: https://ro.ecu.edu.au/ecuworks2011/757/ (accessed on 3 September 2021).
- Hopcraft, M.; Chow, W. Dental caries experience in aboriginal and Torres Strait islanders in the northern peninsula area, Queensland. Aust. Dent. J. 2007, 52, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Endean, C.; Roberts-Thomson, K.; Wooley, S. A n angu oral health: The status of the Indigenous population of the Anangu Pitjantjatjara lands. Aust. J. Rural. Health 2004, 12, 99–103. [Google Scholar] [CrossRef]
- Schuch, H.S.; Haag, D.G.; Kapellas, K.; Arantes, R.; Peres, M.A.; Thomson, W.; Jamieson, L.M. The magnitude of Indigenous and non-Indigenous oral health inequalities in Brazil, New Zealand and Australia. Community Dent. Oral Epidemiol. 2017, 45, 434–441. [Google Scholar] [CrossRef]
- Australian Indigenous HealthInfoNet. Overview of Aboriginal and Torres Strait Islander Health Status 2020. 2021. Available online: https://ro.ecu.edu.au/ecuworkspost2013/10640/ (accessed on 3 September 2021).
- Australian Institute of Health and Welfare (AIHW). Australia’s Children; AIHW: Canberra, Australia, 2020.
- Davies, M.J.; Spencer, A.J.; Westwater, A.; Simmons, B. Dental caries among Australian Aboriginal, non-Aboriginal Australian-born, and overseas-born children. Bull. World Health Organ. 1997, 75, 197–203. [Google Scholar]
- Skamagas, M.; Breen, T.; LeRoith, D. Update on diabetes mellitus: Prevention, treatment, and association with oral diseases. Oral Dis. 2008, 14, 105–114. [Google Scholar] [CrossRef]
- Humphrey, L.L.; Fu, R.; Buckley, D.I.; Freeman, M.; Helfand, M. Periodontal disease and coronary heart disease incidence: A systematic review and meta-analysis. J. Gen. Intern. Med. 2008, 23, 2079. [Google Scholar] [CrossRef] [Green Version]
- Jamieson, L.M.; Paradies, Y.C.; Gunthorpe, W.; Cairney, S.J.; Sayers, S.M. Oral health and social and emotional well-being in a birth cohort of Aboriginal Australian young adults. BMC Public Health 2011, 11, 656. [Google Scholar] [CrossRef] [Green Version]
- Gatto, R.C.J.; Garbin, A.J.Í.; Corrente, J.E.; Garbin, C.A.S. The relationship between oral health-related quality of life, the need for orthodontic treatment and bullying, among Brazilian teenagers. Dent. Press J. Orthod. 2019, 24, 73–80. [Google Scholar] [CrossRef]
- Barasuol, J.C.; Soares, J.P.; Castro, R.G.; Giacomin, A.; Gonçalves, B.M.; Klein, D.; Torres, F.M.; Borgatto, A.F.; Ramos-Jorge, M.L.; Bolan, M.; et al. Untreated Dental Caries Is Associated with Reports of Verbal Bullying in Children 8–10 Years Old. Caries Res. 2017, 51, 482–488. [Google Scholar] [CrossRef] [PubMed]
- King, T. Bad Breath and School Bullying. Available online: http://www.thedentalnetwork.com.hk/bad-breath (accessed on 31 August 2021).
- Scheffel, D.L.S.; Jeremias, F.; Fragelli, C.M.B.; Dos Santos-Pinto, L.A.M.; Hebling, J.; de Oliveira, O.B., Jr. Esthetic dental anomalies as motive for bullying in schoolchildren. Eur. J. Dent. 2014, 8, 124–128. [Google Scholar] [CrossRef]
- Bright, M.A.; Alford, S.M.; Hinojosa, M.S.; Knapp, C.; Fernandez-Baca, D.E. Adverse childhood experiences and dental health in children and adolescents. Community Dent. Oral Epidemiol. 2015, 43, 193–199. [Google Scholar] [CrossRef]
- All4health. Bullying: Nothing to Smile About. Available online: https://all4oralhealth.wordpress.com/2016/02/11/bullying-nothing-to-smile/ (accessed on 31 August 2021).
- Cunningham, S.J. The psychology of facial appearance. Dent. Update 1999, 26, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Seehra, J.; Fleming, P.S.; Newton, T.; DiBiase, A.T. Bullying in orthodontic patients and its relationship to malocclusion, self-esteem and oral health-related quality of life. J. Orthod. 2011, 38, 247–256. [Google Scholar] [CrossRef] [PubMed]
- Al-Bitar, Z.B.; Al-Omari, I.K.; Sonbol, H.N.; Al-Ahmad, H.T.; Cunningham, S.J. Bullying among Jordanian schoolchildren, its effects on school performance, and the contribution of general physical and dentofacial features. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Al-Omari, I.K.; Al-Bitar, Z.B.; Sonbol, H.N.; Al-Ahmad, H.T.; Cunningham, S.J.; Al-Omiri, M. Impact of bullying due to dentofacial features on oral health–related quality of life. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 734–739. [Google Scholar] [CrossRef]
- Coffin, J.; Larson, A.; Cross, D. Bullying in an Aboriginal Context. Aust. J. Indig. Educ. 2010, 39, 77–87. [Google Scholar] [CrossRef]
- Allison, S.; Roeger, L.; Reinfeld-Kirkman, N. Does school bullying affect adult health? Population survey of health-related quality of life and past victimization. Aust. N. Z. J. Psychiatry 2009, 43, 1163–1170. [Google Scholar] [CrossRef]
- O’Moore, M.; Kirkham, C. Self-esteem and its relationship to bullying behaviour. Aggress. Behav. Off. J. Int. Soc. Res. Aggress. 2001, 27, 269–283. [Google Scholar] [CrossRef]
- Gini, G.; Pozzoli, T. Association between bullying and psychosomatic problems: A meta-analysis. Pediatrics 2009, 123, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Fox, C.L.; Boulton, M.J. The social skills problems of victims of bullying: Self, peer and teacher perceptions. Br. J. Educ. Psychol. 2005, 75, 313–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berguno, G.; Leroux, P.; McAinsh, K.; Shaikh, S. Children’s Experience of Loneliness at School and Its Relation to Bullying and the Quality of Teacher Interventions. Qual. Rep. 2004, 9, 483–499. [Google Scholar] [CrossRef]
- Moore, S.E.; Norman, R.E.; Suetani, S.; Thomas, H.J.; Sly, P.D.; Scott, J.G. Consequences of bullying victimization in childhood and adolescence: A systematic review and meta-analysis. World J. Psychiatry 2017, 7, 60. [Google Scholar] [CrossRef] [PubMed]
- Forero, R.; McLellan, L.; Rissel, C.; Bauman, A. Bullying behaviour and psychosocial health among school students in New South Wales, Australia: Cross sectional survey. BMJ 1999, 319, 344–348. [Google Scholar] [CrossRef] [Green Version]
- Kochenderfer, B.J.; Ladd, G.W. Peer victimization: Cause or consequence of school maladjustment? Child Dev. 1996, 67, 1305–1317. [Google Scholar] [CrossRef]
- Bauman, S.; Yoon, J. This issue: Theories of bullying and cyberbullying. Theory Into Pract. 2014, 53, 253–256. [Google Scholar] [CrossRef]
- Thomson, S.; Hillman, K.; Schmid, M.; Rodrigues, S.; Fullarton, J. Highlights from PIRLS 2016: Australia’s Perspective; Australian Council for Educational Research Ltd.: Victoria, Australia, 2017; Available online: https://research.acer.edu.au/cgi/viewcontent.cgi?article=1001&context=pirls (accessed on 2 September 2021).
- Smokowski, P.R.; Cotter, K.L.; Robertson, C.; Guo, S. Demographic, psychological, and school environment correlates of bullying victimization and school hassles in rural youth. J. Criminol. 2013, 2013, 137583. [Google Scholar] [CrossRef] [Green Version]
- Babarro, I.; Andiarena, A.; Fano, E.; Lertxundi, N.; Vrijheid, M.; Julvez, J.; Barreto, F.B.; Fossati, S.; Ibarluzea, J. Risk and protective factors for bullying at 11 years of age in a Spanish birth cohort study. Int. J. Environ. Res. Public Health 2020, 17, 4428. [Google Scholar] [CrossRef]
- Ngo, A.T.; Nguyen, L.H.; Dang, A.K.; Hoang, M.T.; Nguyen, T.H.T.; Vu, G.T.; Do, H.T.; Tran, B.X.; Latkin, C.A.; Ho, R.C. Bullying experience in urban adolescents: Prevalence and correlations with health-related quality of life and psychological issues. PLoS ONE 2021, 16, e0252459. [Google Scholar] [CrossRef]
- Lohoar, S.; Butera, N.; Kennedy, E. Strengths of Australian Aboriginal Cultural Practices in Family Life and Child Rearing. 2014. Available online: https://aifs.gov.au/cfca/publications/strengths-australian-aboriginal-cultural-practices-family-life-and-child-r (accessed on 3 September 2021).
- Australian Institute of Family Studies (AIFS). The Longitudinal Study of Australian Children Annual Statistical Report 2016; AIFS: Melbourne, Australia, 2017.
- Thomson, S.; Wernert, N.; O’Grady, E.; Rodrigues, S. TIMSS 2015: Reporting Australia’s Results. 2017. Available online: https://research.acer.edu.au/cgi/viewcontent.cgi?article=1002&context=timss_2015 (accessed on 3 September 2021).
- Kiyak, H.A. Does orthodontic treatment affect patients’ quality of life? J. Dent. Educ. 2008, 72, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Irving, M.; Gwynne, K.; Angell, B.; Tennant, M.; Blinkhorn, A. Client perspectives on an Aboriginal community led oral health service in rural Australia. Aust. J. Rural. Health 2017, 25, 163–168. [Google Scholar] [CrossRef]
- Mejia, G.C.; Parker, E.J.; Jamieson, L.M. An introduction to oral health inequalities among Indigenous and non-Indigenous populations. Int. Dent. J. 2010, 60, 212–215. [Google Scholar] [PubMed]
- Roberts-Thomson, K.F.; Spencer, A.J.; Jamieson, L.M. Oral health of Aboriginal and Torres Strait Islander Australians. Med. J. Aust. 2008, 188, 592–593. [Google Scholar] [CrossRef]
- Tsey, K.; Whiteside, M.; Daly, S.; Deemal, A.; Gibson, T.; Cadet-James, Y.; Wilson, A.; Santhanam, R.; Haswell-Elkins, M.R. Adapting the ‘Family Wellbeing’empowerment program to the needs of remote Indigenous school children. Aust. N. Z. J. Public Health 2005, 29, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Gwynn, J.; Skinner, J.; Dimitropoulos, Y.; Masoe, A.; Rambaldini, B.; Christie, V.; Sohn, W.; Gwynne, K. Community based programs to improve the oral health of Australian Indigenous adolescents: A systematic review and recommendations to guide future strategies. BMC Health Serv. Res. 2020, 20, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. Bull. World Health Organ. 2007, 85, 867–872. [Google Scholar] [CrossRef]
- Thurber, K.A.; Banks, E.; Banwell, C. Cohort Profile: Footprints in Time, the Australian Longitudinal Study of Indigenous Children. Int. J. Epidemiol. 2015, 44, 789–800. [Google Scholar] [CrossRef] [Green Version]
- Westrupp, E.M.; D’Esposito, F.; Freemantle, J.; Mensah, F.K.; Nicholson, J.M. Health outcomes for Australian Aboriginal and Torres Strait Islander children born preterm, low birthweight or small for gestational age: A nationwide cohort study. PLoS ONE 2019, 14, e0212130. [Google Scholar] [CrossRef]
- Australian Government Department of Social Services. Footprints in Time: The Longitudinal Study of Indigenous Children, Release 11 (Waves 1–11). 2021. Available online: https://ada.edu.au/footprints-in-time-the-longitudinal-study-of-indigenous-children-release-11-waves-1-11/ (accessed on 3 September 2021).
- Thurber, K.; Walker, J.; Dunbar, T.; Guthrie, J.; Calear, A.; Batterham, P.; Richardson, A.; Strazdins, L.; Walter, M.; Doery, K. Measuring Child Mental Health, Psychological Distress, and Social and Emotional Wellbeing in the Longitudinal Study of Indigenous Children. 2019. Available online: https://openresearch-repository.anu.edu.au/bitstream/1885/173695/1/Technical%20Report_Validation%20of%20child%20measures%20in%20LSIC__Final.pdf (accessed on 3 September 2021).
- Hewitt, B. The Longitudinal Study of Indigenous Children: Implications of the Study Design for Analysis and Results; Institute for Social Science Research: St Lucia, Australia, 2012. [Google Scholar]
- Zhuchkova, S.; Rotmistrov, A. How to choose an approach to handling missing categorical data:(un) expected findings from a simulated statistical experiment. Qual. Quant. 2021, 56, 1–22. [Google Scholar] [CrossRef]
- Carlson, B.; Frazer, R. Cyberbullying and Indigenous Australians: A Review of the Literature; Macquarie University: Sydney, Australia, 2018. [Google Scholar]
- Fogarty, W.; Lovell, M.; Langenberg, J.; Heron, M.-J. Deficit Discourse and Strengths-Based Approaches: Changing the Narrative of Aboriginal and Torres Strait Islander Health and Wellbeing; The Lowitja Institute: Melbourne, Australia, 2018. [Google Scholar]
- Thurber, K.A.; Thandrayen, J.; Banks, E.; Doery, K.; Sedgwick, M.; Lovett, R. Strengths-based approaches for quantitative data analysis: A case study using the Australian Longitudinal Study of Indigenous Children. SSM-Popul. Health 2020, 12, 100637. [Google Scholar] [CrossRef]
- Hamilton, M.; Redmond, G. Conceptualisation of Social and Emotional Wellbeing for Children and Young People, and Policy Implications; A Research Report for Australian Research Alliance for Children and Youth and the Australian Institute of Health and Welfare; Australian Research Alliance for Children and Youth: Canberra, Australia, 2010. [Google Scholar]
- Wang, H.; Wang, Y.; Wang, G.; Wilson, A.; Jin, T.; Zhu, L.; Yu, R.; Wang, S.; Yin, W.; Song, H. Structural family factors and bullying at school: A large scale investigation based on a Chinese adolescent sample. BMC Public Health 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Källestål, C.; Dahlgren, L.; Stenlund, H. Oral health behaviour and self-esteem in Swedish children. Soc. Sci. Med. 2000, 51, 1841–1849. [Google Scholar] [CrossRef]
- Low, W.; Tan, S.; Schwartz, S. The effect of severe caries on the quality of life in young children. Pediatr. Dent. 1999, 21, 325–326. [Google Scholar] [PubMed]
- Australian Institute of Health and Welfare (AIHW). Health Performance Framework 2020 Summary Report; Australian Institute of Health and Welfare (AIHW): Canberra, Australia, 2020.
- Davy, C.; Harfield, S.; McArthur, A.; Munn, Z.; Brown, A. Access to primary health care services for Indigenous peoples: A framework synthesis. Int. J. Equity Health 2016, 15, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butten, K.; Johnson, N.W.; Hall, K.K.; Toombs, M.; King, N.; O’Grady, K.-A.F. Impact of oral health on Australian urban Aboriginal and Torres Strait Islander families: A qualitative study. Int. J. Equity Health 2019, 18, 34. [Google Scholar] [CrossRef] [PubMed]
- Priest, N.; Kavanagh, A.; Bécares, L.; King, T. Cumulative effects of bullying and racial discrimination on adolescent health in Australia. J. Health Soc. Behav. 2019, 60, 344–361. [Google Scholar] [CrossRef] [PubMed]
- Priest, N.; Thompson, L.; Mackean, T.; Baker, A.; Waters, E. ‘Yarning up with Koori kids’—hearing the voices of Australian urban Indigenous children about their health and well-being. Ethn. Health 2017, 22, 631–647. [Google Scholar] [CrossRef]
- Australian Health Ministers’ Advisory Council. Aboriginal and Torres Strait Islander Health Performance Framework 2017 Report; AHMAC: Canberra, Australia, 2017.
- Kruger, E.; Perera, I.; Tennant, M. Primary oral health service provision in Aboriginal Medical Services-based dental clinics in Western Australia. Aust. J. Prim. Health 2010, 16, 291–295. [Google Scholar] [CrossRef]
- Ware, V. Improving the Accessibility of Health Services in Urban and Regional Setting for Indigenous People; Australian Institute of Health and Welfare: Canberra, Australia, 2013; Volume 27.
- Limber, S.P.; Olweus, D.; Luxenberg, H. Bullying in U.S. Schools: 2012 Status Report. 2013. Available online: https://www.violencepreventionworks.org/public/document/obppbullyingtrends_2014_final.pdf (accessed on 3 September 2021).
- Malecki, C.K.; Demaray, M.K. The role of social support in the lives of bullies, victims, and bully-victims. In Bullying in American Schools; Routledge: London, UK, 2004; pp. 233–248. [Google Scholar]
- Davidson, L.M.; Demaray, M.K. Social support as a moderator between victimization and internalizing–externalizing distress from bullying. Sch. Psychol. Rev. 2007, 36, 383–405. [Google Scholar] [CrossRef]
- Bodkin-Andrews, G.; Paradies, Y.; Parada, R.; Denson, N.; Priest, N.; Bansel, P. Theory and research on bullying and racism from an Aboriginal Australian perspective. In Proceedings of the AARE 2012, Australian Association for Research in Education 2012 Conference, Sydney, Australia, 2–6 December 2012; pp. 1–14. [Google Scholar]
- Conners-Burrow, N.A.; Johnson, D.L.; Whiteside-Mansell, L.; McKelvey, L.; Gargus, R.A. Adults matter: Protecting children from the negative impacts of bullying. Psychol. Sch. 2009, 46, 593–604. [Google Scholar] [CrossRef]
- Kelly, K.; Dudgeon, P.; Gee, G.; Glaskin, B. Living on the Edge: Social and Emotional Wellbeing and Risk and Protective Factors for Serious Psychological Distress among Aboriginal and Torres Strait Islander People; Cooperative Research Centre: Mount Stromlo, Australia, 2009. [Google Scholar]
- Day, A.; Francisco, A. Social and emotional wellbeing in Indigenous Australians: Identifying promising interventions. Aust. N. Z. J. Public Health 2013, 37, 350–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haswell, M.R.; Blignault, I.; Fitzpatrick, S.; Jackson Pulver, L. The Social And emotional Wellbeing of Indigenous Youth: Reviewing and Extending the Evidence and Examining Its Implications for Policy and Practice; Muri Marri, University of New South Wales: Sydney, Australia, 2013. [Google Scholar]
- Jamieson, L.; Do, L.G.; Bailie, R.S.; Sayers, S.; Turrell, G. Associations between area-level disadvantage and DMFT among a birth cohort of Indigenous Australians. Aust. Dent. J. 2013, 58, 75–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, I.; Robson, B.; Connolly, M.; Al-Yaman, F.; Bjertness, E.; King, A.; Tynan, M.; Madden, R.; Bang, A.; Coimbra Jr, C.E. Indigenous and tribal peoples’ health (The Lancet–Lowitja Institute Global Collaboration): A population study. Lancet 2016, 388, 131–157. [Google Scholar] [CrossRef]
- Priest, N.; King, T.; Bécares, L.; Kavanagh, A.M. Bullying victimization and racial discrimination among Australian children. Am. J. Public Health 2016, 106, 1882–1884. [Google Scholar] [CrossRef]
- Bazán-Serrano, M.; Carruitero, M.J. Assessment of general bullying and bullying due to appearance of teeth in a sample of 11-16 year-old Peruvian schoolchildren. J. Oral Res. 2017, 6, 287–290. [Google Scholar] [CrossRef] [Green Version]
- Baldo Moraes, R.; Knorst, J.K.; Brondani, B.; Baldo Marques, B.; de Sousa Reis, M.; Henriqson, D.; Ardenghi, T.M. Relationship between gingival bleeding and associated factors with reports of verbal bullying in adolescents. J. Periodontol. 2021, 92, 225–233. [Google Scholar] [CrossRef]
- D’Esposito, S.E.; Blake, J.; Riccio, C.A. Adolescents’ vulnerability to peer victimization: Interpersonal and intrapersonal predictors. Prof. Sch. Couns. 2011, 14, 2156759X1101400502. [Google Scholar] [CrossRef]
- Price, M.; Chin, M.A.; Higa-McMillan, C.; Kim, S.; Frueh, B.C. Prevalence and internalizing problems of ethnoracially diverse victims of traditional and cyber bullying. Sch. Ment. Health 2013, 5, 183–191. [Google Scholar] [CrossRef]
- Farmer, T.W.; Irvin, M.J.; Motoca, L.M.; Leung, M.-C.; Hutchins, B.C.; Brooks, D.S.; Hall, C.M. Externalizing and internalizing behavior problems, peer affiliations, and bullying involvement across the transition to middle school. J. Emot. Behav. Disord. 2015, 23, 3–16. [Google Scholar] [CrossRef]
- Wiens, B.A.; Haden, S.C.; Dean, K.L.; Sivinski, J. The impact of peer aggression and victimization on substance use in rural adolescents. J. Sch. Violence 2010, 9, 271–288. [Google Scholar] [CrossRef]
- Australian Government Department of Social Services. Australian Government Department of Social Services Footprints in Time: The Longitudinal Study of Indigenous Children—Data User Guide; Australian Government Department of Social Services: Canberra, Australia, 2018.
- Han, Z.; Zhang, G.; Zhang, H. School bullying in urban China: Prevalence and correlation with school climate. Int. J. Environ. Res. Public Health 2017, 14, 1116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Walters, E.E. Epidemiology of DSM-III-R major depression and minor depression among adolescents and young adults in the national comorbidity survey. Depress. Anxiety 1998, 7, 3–14. [Google Scholar] [CrossRef]
- Sareen, J.; Cox, B.J.; Afifi, T.O.; Clara, I.; Yu, B.N. Perceived need for mental health treatment in a nationally representative Canadian sample. Can. J. Psychiatry 2005, 50, 643–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | Longitudinal Study of Indigenous Children (LSIC) Interview Question Wording or Description | Data Source | Coding for Analysis |
|---|---|---|---|
| Outcome variables | |||
| Bullying victimization | Has the study child been bullied (or treated unfairly) at school (in the previous 12 months)? | Both—parent and child questionnaire | 1 = Yes, 0 = No |
| Remoteness | Australian Statistical Geography Standard (ASGC) Remoteness area 2016 | Both—parent and child questionnaire | 1 = Major cities, 0 = Rural/Remote |
| Main explanatory variables | |||
| Dental problems | Has the study child ever had any of the following problems with (his/her) teeth or gums?
| Parent questionnaire | 1 = Yes, 0 = No |
| Sociodemographic covariates | |||
| Age | Age of study child (in years) | Both—parent and child questionnaire | 1 = ≥13 to 15, 0 = 10 to ≤12 |
| Gender | Gender of the study child | Both—parent and child questionnaire | 1 = Boys, 0 = Girls |
| School grade | In what year/grade is the study child currently enrolled? | Both—parent and child questionnaire | 1 = Yes, 0 = No |
| School type | What kind of school does study child go to? | Parent questionnaire | 2 = Government, 1 = Catholic, 0 = Private |
| Parents’ educational qualification | What was the highest qualification that you have completed? | Parent questionnaire | 2 = Diploma and above, 1 = Certificate III or IV, 0 = Year 12 and below |
| Parents’ employment status | Do you have a job? | Parent questionnaire | 1 = Employed, 0 = Unemployed |
| Parents’ satisfaction with life | How much do you agree or disagree with the following statement? In general, I am happy with how things are for me in my life right now. Note that ‘overall satisfaction with life’ is a direct indicator of SEWB across different populations—children, young people and adults [59] | Parent questionnaire | 2 = Unhappy, 1 = Neither, 0 = Happy |
| Community safety | Do you (parent and child asked separately) think where you live/in your community that is safe during the day and at night? | Both—parent and child questionnaire | 1 = Safe, 0 = Unsafe |
| Child oral hygiene practice | How often are study child’s teeth cleaned? | Both—parent and child questionnaire | 1 = Rarely/never, 0 = Once a day or more |
| Family functioning | Do your family get along well with each other? Note that ‘family functioning’ is multi-component factor (includes cohesion, safety at home and perceived parental support), and good family functioning found to be protective against school bullying [60]. | Both—parent and child questionnaire | 1 = Very good/Good, 0 = Fair/Poor |
| Family experiences racial discrimination | How often does your family experience racism, discrimination, or prejudice? | Both—parent and child questionnaire | 1 = Frequently, 0 = Occasionally/Never |
| Family income | How much money do you usually get from all of your sources of income in total, (including your partner), after deductions are taken out, such as tax, quarantined payments, etc.? | Parent questionnaire | 2 = High ($2000 or more per fortnight), 1 = Medium ($800–$1999 per fortnight), 0 = Low ($0–$799 per fortnight) |
| SEIFA IRSAD quintiles | The SEIFA (Socio-Economic Indexes for Areas) IRSAD (Index of Relative Socio-economic Advantage and Disadvantage) is used to estimate area-level SES. A lowest IRSAD score (Quintile 1, 0–20%) signifies greater disadvantage, as well as a lack of advantages in general and highest IRSAD score (Quintile 5, 80–100%), indicates greater advantages as well as a lack of disadvantage at the area level. | Parent questionnaire | 4 = Q5 (Most advantaged), 3 = Q4, 2 = Q3, 1 = Q2, 0 = Q1 (Most disadvantaged) |
| Total | Major Cities | Rural/Remote | |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| Total | 766 (100.0) | 250 (32.6) | 516 (67.4) |
| Age (Mean = 12.25, SD = 1.49) | |||
| 10 to ≤12 | 466 (60.8) | 152 (32.6) | 314 (67.4) |
| >12 to 15 | 300 (39.2) | 98 (32.7) | 202 (67.3) |
| Gender | |||
| Boys | 381 (49.7) | 122 (32.0) | 259 (68.0) |
| Girls | 385 (50.3) | 128 (33.3) | 257 (66.7) |
| School Grade | |||
| Grade 4 | 15 (2.0) | 4 (26.7) | 11 (73.3) |
| Grade 5 | 232 (30.3) | 74 (31.9) | 158 (68.1) |
| Grade 6 | 201 (26.2) | 71 (35.3) | 130 (64.7) |
| Grade 7 | 34 (4.4) | 6 (17.7) | 28 (82.3) |
| Grade 8 | 184 (24.0) | 60 (32.6) | 124 (67.4) |
| Grade 9 | 100 (13.1) | 35 (35.0) | 65 (65.0) |
| School type | |||
| Private | 52 (6.8) | 25 (48.1) | 27 (51.9) |
| Catholic | 76 (9.9) | 33 (43.4) | 43 (56.6) |
| Government | 638 (83.3) | 192 (30.1) | 446 (69.9) |
| Parents’ educational qualification | |||
| Year 12 or below | 381 (49.7) | 108 (28.4) | 273 (71.7) |
| Certificate III or IV | 240 (31.3) | 73 (30.4) | 167 (69.6) |
| Diploma or above | 145 (18.9) | 69 (47.6) | 76 (52.4) |
| Parents’ employment status | |||
| Unemployed | 315 (41.1) | 88 (27.9) | 227 (72.1) |
| Employed | 451 (58.9) | 162 (35.9) | 289 (64.1) |
| Parents’ satisfaction with life | |||
| Unhappy | 63 (8.2) | 24 (38.1) | 39 (61.9) |
| Neither | 78 (10.2) | 28 (35.9) | 50 (64.1) |
| Happy | 625 (81.6) | 198 (31.7) | 427 (68.3) |
| Community safety | |||
| Safe | 704 (91.9) | 230 (32.7) | 474 (67.3) |
| Unsafe | 62 (8.1) | 20 (32.3) | 42 (67.7) |
| Child oral hygiene practice | |||
| Once a day or more | 637 (83.2) | 213 (33.4) | 424 (66.6) |
| Rarely or never | 129 (16.8) | 37 (28.7) | 92 (71.3) |
| Family functioning | |||
| Fair/Poor | 20 (2.6) | 6 (30.0) | 14 (70.0) |
| Very good/Good | 746 (97.4) | 244 (32.7) | 502 (67.3) |
| Family experiences racial discrimination | |||
| No | 392 (51.2) | 97 (24.7) | 295 (75.3) |
| Yes | 374 (48.8) | 153 (40.9) | 221 (59.1) |
| Family income | |||
| Low ($0–$799 per fortnight) | 75 (9.8) | 22 (29.3) | 53 (70.7) |
| Medium ($800–$1999 per fortnight) | 348 (45.4) | 97 (27.9) | 251 (72.1) |
| High ($2000 or more per fortnight) | 343 (44.8) | 131 (38.2) | 212 (61.8) |
| SEIFA IRSAD quintiles | |||
| Q1- Most disadvantaged | 371 (48.4) | 91 (24.5) | 280 (75.5) |
| Q2 | 182 (23.8) | 51 (28.0) | 131 (72.0) |
| Q3 | 114 (14.9) | 51 (44.7) | 63 (55.3) |
| Q4 | 65 (8.5) | 34 (52.3) | 31 (47.7) |
| Q5—Most advantaged | 34 (4.4) | 23 (67.7) | 11 (32.3) |
| Bullying Victimization—Parent Data | ||||
|---|---|---|---|---|
| Major Cities (n = 80) | Rural/Remote (n = 177) | |||
| n (%) | p-Value | n (%) | p-Value | |
| Dental problems | 0.016 * | 0.050 * | ||
| No | 42 (52.5) | 105 (59.3) | ||
| Yes | 38 (47.5) | 72 (40.7) | ||
| Age | 0.859 | 0.415 | ||
| 10 to ≤12 | 48 (60.0) | 112 (63.3) | ||
| >12 to 15 | 32 (40.0) | 65 (36.7) | ||
| Gender | 0.422 | 0.689 | ||
| Boys | 42 (52.5) | 91 (51.4) | ||
| Girls | 38 (47.5) | 86 (48.6) | ||
| School Grade | 0.931 | 0.629 | ||
| Grade 4 | 1 (1.2) | 2 (1.1) | ||
| Grade 5 | 22 (27.5) | 57 (32.2) | ||
| Grade 6 | 25 (31.3) | 49 (27.7) | ||
| Grade 7 | 1 (1.2) | 7 (4.0) | ||
| Grade 8 | 19 (23.8) | 40 (22.6) | ||
| Grade 9 | 12 (15.0) | 22 (12.4) | ||
| School type | 0.735 | 0.812 | ||
| Private | 9 (11.3) | 10 (5.7) | ||
| Catholic | 12 (15.0) | 13 (7.3) | ||
| Government | 59 (73.7) | 154 (87.0) | ||
| Parents’ educational qualification | 0.872 | 0.061 | ||
| Year 12 or below | 33 (30.6) | 81 (29.7) | ||
| Certificate III or IV | 25 (34.3) | 67 (40.1) | ||
| Diploma or above | 22 (31.9) | 29 (38.2) | ||
| Parents’ employment status | 0.601 | 0.871 | ||
| Unemployed | 30 (37.5) | 77 (43.5) | ||
| Employed | 50 (62.5) | 100 (56.5) | ||
| Parents’ happiness with life | 0.014 * | 0.619 | ||
| Unhappy | 14 (17.5) | 12 (6.8) | ||
| Neither | 9 (11.3) | 20 (11.3) | ||
| Happy | 57 (71.2) | 145 (81.9) | ||
| Community safety | 0.022 * | 0.010 * | ||
| Safe | 69 (86.3) | 155 (87.6) | ||
| Unsafe | 11 (13.7) | 22 (12.4) | ||
| Oral hygiene practice | 0.061 | 0.384 | ||
| Once a day or more | 64 (80.0) | 144 (79.7) | ||
| Rarely or never | 16 (20.0) | 33 (20.3) | ||
| Family functioning | 0.415 | 0.068 | ||
| Fair/Poor | 1 (1.3) | 8 (4.5) | ||
| Very good/Good | 79 (98.7) | 169 (95.5) | ||
| Family experiences racism | <0.001 *** | <0.001 *** | ||
| No | 17 (21.3) | 77 (43.5) | ||
| Yes | 63 (78.8) | 100 (56.5) | ||
| Family income | 0.096 | 0.324 | ||
| Low ($0–$799 per fortnight) | 11 (13.7) | 23 (13.0) | ||
| Medium ($800–$1999 per fortnight) | 33 (41.3) | 85 (48.0) | ||
| High ($2000 or more per fortnight) | 36 (45.0) | 69 (39.0) | ||
| SEIFA IRSAD quintiles | 0.744 | 0.569 | ||
| Q1—Most disadvantaged | 26 (32.5) | 88 (49.7) | ||
| Q2 | 20 (25.0) | 51 (28.8) | ||
| Q3 | 15 (18.7) | 24 (13.6) | ||
| Q4 | 11 (13.8) | 11 (6.2) | ||
| Q5—Most advantaged | 8 (10.0) | 3 (1.7) | ||
| Bullying Victimization—Child Data | ||||
|---|---|---|---|---|
| Major Cities (n = 113) | Rural/Remote (n = 227) | |||
| n (%) | p-Value | n (%) | p-Value | |
| Dental problems | 0.027 * | 0.054 | ||
| No | 63 (55.7) | 137 (60.4) | ||
| Yes | 50 (44.3) | 90 (39.6) | ||
| Age | <0.001 *** | <0.001 *** | ||
| 10 to £12 | 90 (79.7) | 161 (70.9) | ||
| ≥13 to 15 | 23 (20.3) | 66 (29.1) | ||
| Gender | 0.217 | 0.602 | ||
| Boys | 60 (53.1) | 111 (48.9) | ||
| Girls | 53 (46.9) | 116 (51.1) | ||
| School Grade | 0.080 | 0.110 | ||
| Grade 4 | 0 (0.0) | 4 (1.8) | ||
| Grade 5 | 45 (39.8) | 80 (35.2) | ||
| Grade 6 | 44 (38.9) | 65 (28.6) | ||
| Grade 7 | 2 (1.8) | 14 (6.2) | ||
| Grade 8 | 15 (13.3) | 46 (20.3) | ||
| Grade 9 | 7 (6.2) | 18 (7.9) | ||
| School type | 0.812 | 0.233 | ||
| Private | 10 (8.8) | 8 (3.5) | ||
| Catholic | 16 (14.2) | 17 (7.5) | ||
| Government | 87 (77.0) | 202 (89.0) | ||
| Parents’ educational qualification | 0.762 | 0.010 | ||
| Year 12 or below | 46 (40.7) | 104 (45.8) | ||
| Certificate III or IV | 34 (30.1)) | 88 (38.8) | ||
| Diploma or above | 33 (29.2) | 35 (15.4) | ||
| Parents’ employment status | 0.261 | 0.980 | ||
| Unemployed | 44 (38.9) | 100 (44.1) | ||
| Employed | 69 (61.1) | 127 (55.9) | ||
| Parents’ happiness with life | 0.029 * | 0.203 | ||
| Unhappy | 15 (13.3) | 12 (5.3) | ||
| Neither | 17 (15.0) | 24 (10.6) | ||
| Happy | 81 (71.7) | 191 (84.1) | ||
| Community safety | 0.166 | 0.034 * | ||
| Safe | 101 (89.4) | 202 (89.0) | ||
| Unsafe | 12 (10.6) | 25 (11.0) | ||
| Child oral hygiene practice | 0.648 | 0.015 * | ||
| Once a day or more | 95 (84.1) | 176 (77.5) | ||
| Rarely or never | 18 (15.9) | 51 (22.5) | ||
| Family functioning | 0.057 | 0.646 | ||
| Fair/Poor | 5 (4.4) | 7 (3.1) | ||
| Very good/Good | 108 (95.6) | 220 (96.9) | ||
| Family experiences racism | 0.278 | 0.224 | ||
| No | 48 (42.5) | 123 (54.2) | ||
| Yes | 65 (57.5) | 104 (45.8) | ||
| Family income | 0.842 | 0.684 | ||
| Low ($0–$799 per fortnight) | 10 (8.9) | 26 (11.5) | ||
| Medium ($800–$1999 per fortnight) | 46 (40.7) | 111 (48.9) | ||
| High ($2000 or more per fortnight) | 57 (50.4) | 90 (39.6) | ||
| SEIFA IRSAD quintiles | 0.189 | 0.121 | ||
| Q1—Most disadvantaged | 41 (36.3) | 117 (51.5) | ||
| Q2 | 30 (26.5) | 63 (27.8) | ||
| Q3 | 19 (16.8) | 23 (10.1) | ||
| Q4 | 15 (13.3) | 16 (7.1) | ||
| Q5—Most advantaged | 8 (7.1) | 8 (3.5) | ||
| Parent Data | Child Data | |||
|---|---|---|---|---|
| Major Cities | Rural/Remote | Major Cities | Rural/Remote | |
| aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | aOR (95% CI) | |
| Dental problems (ref. No) | ||||
| Yes | 2.20 ** (1.20, 4.02) | 1.41 (0.93, 2.14) | 1.57 (0.87, 2.83) | 1.38 (0.94, 2.04) |
| Age (ref. 10 to ≤12 years) | ||||
| ≥13 to 15 | 1.40 (0.76, 2.56) | 0.82 (0.54, 1.24) | 0.19 *** (0.10, 0.36) | 0.42 *** (0.29, 0.62) |
| Parents’ educational qualification (ref. Year 12 or below) | ||||
| Certificate III or IV | 1.44 (0.72, 2.90) | 1.65 * (1.06, 2.57) | 1.09 (0.55, 2.16) | 2.04 ** (1.35, 3.09) |
| Diploma or above | 0.99 (0.48, 2.04) | 1.35 (0.74, 2.45) | 1.18 (0.58, 2.40) | 1.56 (0.90, 2.70) |
| Parents’ happiness with life (ref. Happy) | ||||
| Neither | 0.53 (0.15, 1.83) | 1.54 (0.58, 4.07) | 1.53 (0.41, 5.66) | 2.27 (0.89, 5.76) |
| Unhappy | 0.41 (0.15, 1.10) | 1.24 (0.58, 2.66) | 0.56 (0.21, 1.57) | 2.08 * (0.99, 4.39) |
| Community safety (ref. Safe) | ||||
| Unsafe | 2.67 (0.93, 7.59) | 2.65 ** (1.30, 5.40) | 2.26 (0.77, 6.62) | 2.44 * (1.22, 4.86) |
| Child oral hygiene practice (ref. Once a day or more) | ||||
| Rarely or never | 1.45 (0.63, 3.36) | 1.33 (0.78, 2.27) | 0.73 (0.31, 1.76) | 2.33 ** (1.41, 3.86) |
| Family experiences racial discrimination (ref. No) | ||||
| Yes | 3.27 *** (1.70, 6.29) | 2.39 *** (1.58, 3.63) | 0.69 (0.38, 1.26) | 1.14 (0.78, 1.66) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Islam, M.I.; Chadwick, V.; Esgin, T.; Martiniuk, A. Bullied Because of Their Teeth: Evidence from a Longitudinal Study on the Impact of Oral Health on Bullying Victimization among Australian Indigenous Children. Int. J. Environ. Res. Public Health 2022, 19, 4995. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19094995
Islam MI, Chadwick V, Esgin T, Martiniuk A. Bullied Because of Their Teeth: Evidence from a Longitudinal Study on the Impact of Oral Health on Bullying Victimization among Australian Indigenous Children. International Journal of Environmental Research and Public Health. 2022; 19(9):4995. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19094995
Chicago/Turabian StyleIslam, Md Irteja, Verity Chadwick, Tuguy Esgin, and Alexandra Martiniuk. 2022. "Bullied Because of Their Teeth: Evidence from a Longitudinal Study on the Impact of Oral Health on Bullying Victimization among Australian Indigenous Children" International Journal of Environmental Research and Public Health 19, no. 9: 4995. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19094995