
Exploring Support Provided by Community Managed Organisations to Address Health Risk Behaviours Associated with Chronic Disease among People with Mental Health Conditions: A Qualitative Study with Organisational Leaders

 , ,
, , {kind=link}
Abstract
:1. Introduction
- (1)
- The type of support provided to address five key health risk behaviours (smoking, poor nutrition, alcohol consumption, inadequate physical activity, and poor sleep) among CMO consumers with a mental health condition, and
- (2)
- The perceived organisational and staff level barriers and facilitators to providing support to address health risk behaviours.
2. Materials and Methods
2.1. Design and Setting
Setting Context
2.2. Participants and Recruitment
2.2.1. Community Managed Organisations
2.2.2. Organisational Leaders
2.3. Measures
2.4. Data Collection
2.5. Data Analysis
3. Results
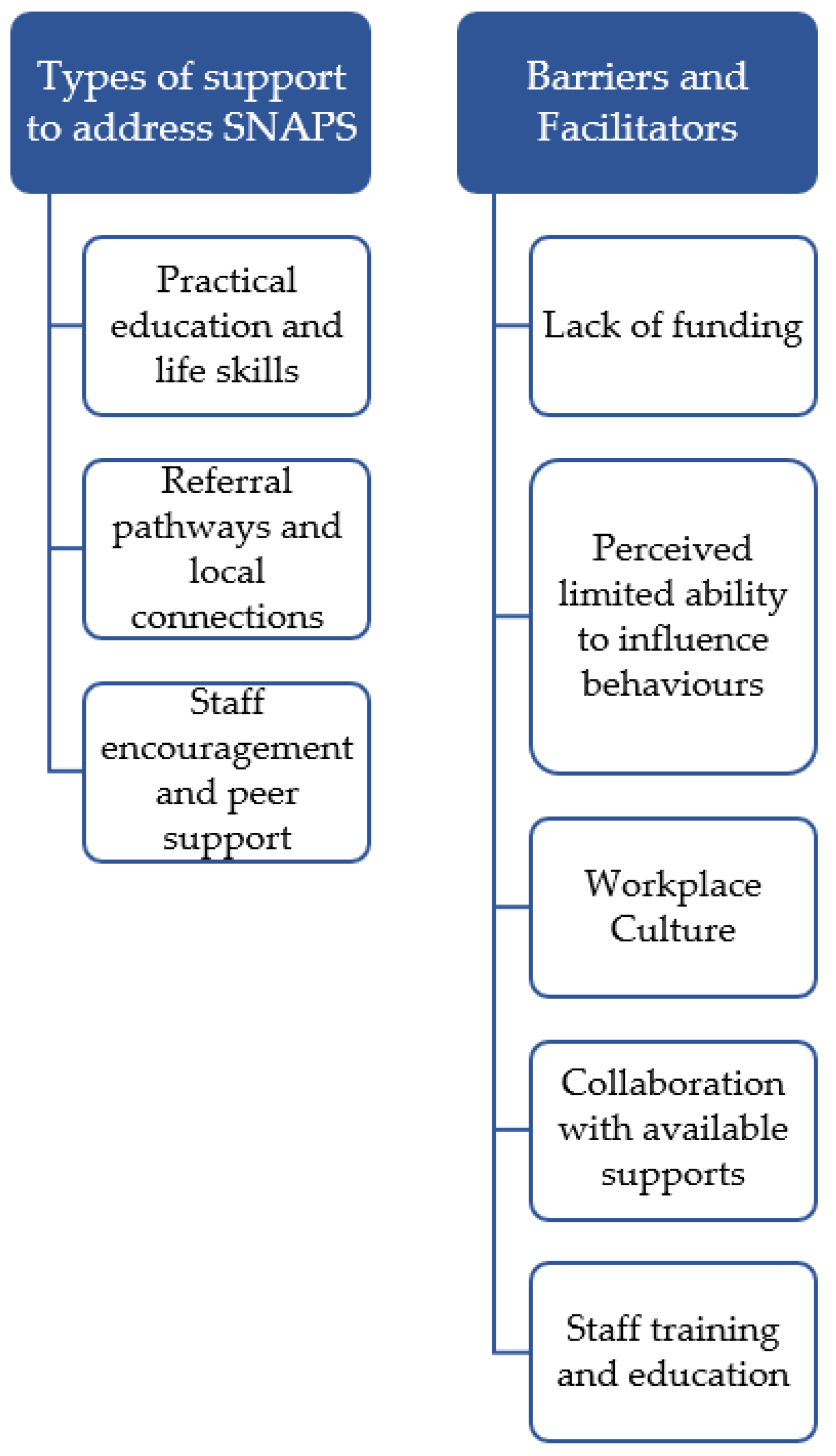
3.1. Types of Support Provided by CMOs to Address SNAPS Behaviours for Consumers with a Mental Health Condition
3.1.1. Practical Education and Life Skills
We’ve got our website, digital health website and it’ll have a section dedicated to smokers. It just asks whereby these people to just reflect on their smoking, whether they smoke or not, and whether they’d like information or support to quit.CMO leader 2
We support them to get things like nicotine patches and [gum].CMO leader 5
We have services develop resources, like cookbooks. Cooking for one, cookbooks, so, how to make the most of a supermarket shop and budget and make a large number of meals out of one shop, with pictures. All of the steps. All the ingredients.CMO leader 2
There is also a program called [name of nutrition program]...that takes people through the cycle of growing or understanding about the nutritional balance and priorities and then looking at the cycle of that from growing things to preparing and eating things together as a group.CMO leader 3
The [physical health checklist activity] the [form name] and the website all [explore] alcohol, and we do ask the question directly…if people would like to reduce it. If they’ve got concerns about the amount of alcohol…The website links people to information, being able to reduce.CMO leader 2
We have an hour and a half session on lifestyle practices which is around reducing alcohol consumption, understanding even what healthy alcohol consumption is. Yes, we educate people because it comes as a huge shock to most of them to recognise what two standard drinks are.CMO leader 7
It’s a 12-week intensive program for people with mental illness to—it’s focused on the cardio-metabolic syndrome, trying to get people fitter, lose weight…We provide gym memberships to people that join that.CMO leader 1
We do have a strong focus on [physical activity] when we hold events as an organisation, like we have regular picnic days, we have—and have had an annual volleyball.CMO leader 2
One of the quarterly health promotion topics. People talk about things like having an evening routine, for example, and ways to help you drift off to sleep. Maybe it might be mindfulness or meditation or different apps. It’s strategies to overcome those.CMO leader 2
3.1.2. Referral Pathways and Local Connections
We would probably issue them with the 13 QUIT Line number and refer them to their GP for appropriate treatment.CMO leader 11
[Name of nutrition program] that’s running at the moment, [addresses] nutrition and there’s a dietician involved there. A nutritionist and a dietician, which help and support the consumers.CMO leader 1
If it leaned to eating disorder territory, we would look at…connecting with a specialist.CMO leader 6
If we notice someone’s not cooking or not eating as well as they could, we will look at things like [name of food delivery service] as an option.CMO leader 12
If we thought somebody had a serious alcohol problem, we would most likely, with their consent, refer them to an alcohol and drug counsellor or an alcohol and drug specific service.CMO leader 1
We would have to refer them on to another organisation to get support with that. It would just be the case manager finding out who’s local and who can support and linking them up.CMO leader 9
The staff at all the different [name of group exercise centres] have been great. So that’s one we’ve really tapped into. Then where there’s not a [name of group exercise centre], we might go to a [name of gym] or whatever. They’ve been really open and really helpful. A lot of the times, they’ll give us a free personal trainer to work with the clients and staff. They’ve really—I must say, really embraced it.CMO leader 4
It could be related to tiredness, which could be a medication—so it might be saying, maybe talk to your doctor about the timing of medications.CMO leader 2
3.1.3. Staff Encouragement and Peer Support
Our support workers actually will attend gyms and classes with people, because we realise that it’s not only about that, sometimes people lack confidence, especially if they’re overweight, or they don’t have great self-esteem. So, people will accompany people to gyms and to classes.CMO leader 1
We support people to engage to the best of their ability in regular exercise just throughout their routine.CMO leader 5
More recently… every staff member is expected to be interested in and trying to encourage a change in smoking behaviour.CMO leader 3
If the consumer says [in the course of] the work with a staff member, I’m not sleeping, it’s a problem, the staff member will work with…and encourage the person to see their GP, do some basic environmental changes that are fairly widely accepted as common knowledge like coffee, don’t watch television in bed, darkened room, go to bed at the same time and all that sort of stuff.CMO leader 3
We had a peer health coaching program [in relation to smoking]...where we would have consumers providing health coaching over the telephone to other consumers.CMO leader 3
That relatability and a member of [name of organisation] works really hard on accessibility and being relatable for young people... I think that the peer workforce really takes that to a whole other level of hey, we’re doing this together. I understand where you’ve been and I’m here to do this with you.CMO leader 6
3.2. What Allows CMOs to Address SNAPS Behaviours for Consumers with a Mental Health Condition (Barriers and Facilitators)
But we’ve got other drop-in support people who, outside of the hours that we provide services to, well, they go out in the community, they go to the pub, they go to the bottle shop and buy beer and whatever they want, their choice of drink and they bring it back to [unclear] and we don’t have a lot of input into that.CMO leader 5
Our mandate really is to provide the very best experience we can in those five days for people… So, I think as an organisation, we provide the education and the one-on-one time with the counsellor but then it’s the follow up of course which is so important with smoking and drinking cessation that we don’t do.CMO leader 7
3.2.1. Lack of Funding
I’m always going to say funding because funding should never stop you doing these incredibly important things, but it is sometimes the requirement in order to have a really [sustained] approach... I think I’d like to see funders, perhaps in terms of the funding we do get, be a little bit more open to us employing different types of people... It’d be great if I could turn say three or four of those positions into…personal trainer or nutritionist…but the problem is the way they fund this, we have to report a certain amount of activity and only certain types of activity is allowed to be counted.CMO leader 3
But the biggest challenge for me is when you’ve got someone that needs help, and particularly when you’ve got someone that’s willing to engage in help. That’s a really critical window, and what I’ve noticed is if you’ve got a very vulnerable person at a stage where they’re able to accept help, and you can’t get them that help, that’s a massive failing. But it’s a reality of the system that we can’t [all live in], particularly from a regional lens, who get less resources, less funding….So there’s all these extra, additional barriers, reductions in funding—not enough funding to begin with period, uncertain funding….CMO leader 8
3.2.2. Perceived Limited Ability to Influence Behaviours
I think it’s pretty underrepresented in the health promotion ads. Like you regularly see stuff about smoking and alcohol, drink driving, and all those sorts of things, but the promotion of healthy sleep is probably pretty a bland topic in health promotion and probably wouldn’t get a lot of funding.CMO leader 11
These guys are very stuck in their ways with smoking. It is super challenging.CMO leader 4
So it doesn’t matter how much you put a smoking plan in or even with a restrictive practice, if the consumer has enough independence where they’re allowed in the community without the need for any additional one-on-one support, then all they need to do is withdraw money, sit on a bench and smoke a couple of cigarettes and that’s it.CMO leader 11
3.2.3. Workplace Policies and Culture
My experience is when you get staff to be part of that, take ownership of that, be accountable for that and make positive changes themselves, the cascading effect is better and greater when you’re dealing with people in the community that you’re serving.CMO leader 8
We have a smoking policy for staff and we also have a smoking policy for the people that we support. That also covers illicit substances and alcohol as well. So that pretty much provides the main guide for staff as to what to do and what’s permitted, what’s not permitted, what the scope is.CMO leader 10
3.2.4. Collaboration with Available Supports
Regularly inviting people to come from local health districts and other providers in the community, to share information, education, and health promotions. We do things like the health promotions talk about things like—particularly around Christmas and holiday periods, a lot of the services focus on safe drinking and limiting drinking.CMO leader 2
We might get the [psychiatric medication] nurse out, and that way we can make sure that new staff members get that relevant information, but also, it never hurts to refresh—for anyone to have a refresh on those types of issues. I think that’s then that little bit of collaboration with the local health district as well, where they don’t—they know that we work quite closely with them, so they’re happy to share that information with us.CMO leader 4
3.2.5. Staff Training and Education
To be able to deliver really targeted support, train the staff, development of resources that will be useful to people accessing the service, and relevant to them and their needs.CMO leader 2
So by training our staff and getting our staff to go through it, we’re sort of unlocking the lived experience that’s already there around some of these issues. When we’re able to do that, which is not everywhere, does enhance what we deliver because people are then able to say well, I did this.CMO leader 3
We do a lot of internal training…any time any local training comes up that we can put staff through.CMO leader 9
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Siddiqi, N.; Koyanagi, A.; Siskind, D.; Rosenbaum, S.; Galletly, C.; Allan, S.; Caneo, C.; Carney, R.; Carvalho, A.F. The Lancet Psychiatry Commission: A blueprint for protecting physical health in people with mental illness. Lancet Psychiatry 2019, 6, 675–712. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Meeting Report on Excess Mortality in Persons with Severe Mental Disorders; World Health Organisation: Geneva, Switzerland, 2015. [Google Scholar]
- Ministerial Advisory Committee on Mental Health. Improving the Physical Health of People with Severe Mental Illness: No Mental Health without Physical Health; Department of Health & Human Services: Melbourne, VIC, Australia, 2012. [Google Scholar]
- Mental Health Coordinating Council. The NSW Community Managed Mental Health Sector Mapping Report 2010; Mental Health Coordinating Council: Lilyfield, NSW, Australia, 2010. [Google Scholar]
- Boyle, F.M.; Donald, M.; Dean, J.H.; Conrad, S.; Mutch, A.J. Mental health promotion and non-profit health organisations. Health Soc. Care Community 2007, 15, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Gibson, L.; Clinton-McHarg, T.; Wilczynska, M.; Latter, J.; Bartlem, K.; Henderson, C.; Wiggers, J.; Wilson, A.; Searles, A.; Bowman, J. Preventive care practices to address health behaviours among people living with mental health conditions: A survey of Community Managed Organisations. Prev. Med. Rep. 2021, 23, 101495. [Google Scholar] [CrossRef]
- Bartlem, K.; Fehily, C.; Wynne, O.; Gibson, L.; Lodge, S.; Clinton-McHarg, T.; Dray, J.; Bowman, J.; Wolfenden, L.; Wiggers, J. Implementing Initiatives to Improve Physical Health for People in Community-Based Mental Health Programs: An Evidence Check Rapid Review Brokered by the Sax Institute for the NSW Ministry of Health; The Sax Institute: Glebe NSW, Australia, 2020; Available online: https://www.saxinstitute.org.au/publications/evidence-check-library/initiatives-to-improve-physical-health-for-people-in-community-based-mental-health-programs/ (accessed on 27 April 2022).
- Mucheru, D.; Ashby, S.; Hanlon, M.-C.; McEvoy, M.; MacDonald-Wicks, L. Factors to consider during the implementation of nutrition and physical activity trials for people with psychotic illness into an Australian community setting. BMC Health Serv. Res. 2020, 20, 743. [Google Scholar] [CrossRef] [PubMed]
- Lyons, M. Third Sector: The Contribution of Nonprofit and Cooperative Enterprise in Australia; Allen & Unwin: St Leonards, NSW, Australia, 2001. [Google Scholar]
- Mental Health Coordinating Council. About the Sector. Available online: https://www.mhcc.org.au/about-mhcc/about-the-sector/ (accessed on 15 May 2021).
- Connor, K.L.; Breslau, J.; Finnerty, M.T.; Leckman-Westin, E.; Pritam, R.; Yu, H. Integrating physical health: What were the costs to behavioral health care clinics? Gen. Hosp. Psychiatry 2018, 51, 41–45. [Google Scholar] [CrossRef] [PubMed]
- Murphy, K.A.; Daumit, G.L.; Bandara, S.N.; Stone, E.M.; Kennedy-Hendricks, A.; Stuart, E.A.; Pollack, C.E.; McGinty, E.E. Association Between the Maryland Medicaid Behavioral Health Home Program and Cancer Screening in People with Serious Mental Illness. Psychiatr. Serv. 2020, 71, 608–611. [Google Scholar] [CrossRef]
- Flanagan, S.M.; Hancock, B. Reaching the hard to reach—Lessons learned from the VCS (voluntary and community Sector). A qualitative study. BMC Health Serv. Res. 2010, 10, 92. [Google Scholar] [CrossRef] [Green Version]
- Hancock, N.; Cowles, C. How NSW Mental Health Community Managed Organisations Assist People Living with Mental Health Conditions to Address their Physical Health Needs: A Scoping Study and Review of the Literature; NSW Mental Health Coordinating Council: Lilyfield, NSW, Australia, 2014. [Google Scholar]
- Marlowe, P.; Paynter, J. Investigating change in non-government mental health service organisations’ ‘smoke-free’ attitudes and practice in New Zealand. J. Smok. Cessat. 2015, 10, 124–134. [Google Scholar] [CrossRef]
- Mental Health Coordinating Council & The Cancer Council NSW. Report on the Smoking Survey of MHCC Member Organisations: Current Attitudes, Policies and Practices in Addressing the Issue of Tobacco Smoking; Mental Health Coordinating Council: Lilyfield, NSW, Australia, 2008. [Google Scholar]
- Brown, J.D. Availability of Integrated Primary Care Services in Community Mental Health Care Settings. Psychiatr. Serv. 2019, 70, 499–502. [Google Scholar] [CrossRef]
- Shim, R.S.; Lally, C.; Farley, R.; Ingoglia, C.; Druss, B.G. Medical Care Services in Community Mental Health Centers: A National Survey of Psychiatrists. J. Behav Health Serv. Res. 2015, 42, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Scharf, D.M.; Schmidt Hackbarth, N.; Eberhart, N.K.; Horvitz-Lennon, M.; Beckman, R.; Han, B.; Pincus, H.A.; Burnam, M.A. General Medical Outcomes from the Primary and Behavioral Health Care Integration Grant Program. Psychiatr. Serv. 2016, 67, 1226–1232. [Google Scholar] [CrossRef] [PubMed]
- Ashton, M.; Lawn, S.; Hosking, J.R. Mental health workers’ views on addressing tobacco use. Aust. N. Z. J. Psychiatry 2010, 44, 846–851. [Google Scholar] [CrossRef] [PubMed]
- Hull, P.; Salmon, A.M.; O’Brien, J.; Chapman, K.; Williams, K. Can social and community service organisations embrace tobacco control for their disadvantaged clients? Health Promot. J. Aust. 2012, 23, 188–193. [Google Scholar] [CrossRef]
- Bryant, J.; Bonevski, B.; Paul, C.; O’Brien, J.; Oakes, W. Developing cessation interventions for the social and community service setting: A qualitative study of barriers to quitting among disadvantaged Australian smokers. BMC Public Health 2011, 11, 493. [Google Scholar] [CrossRef] [Green Version]
- McGinty, E.E.; Kennedy-Hendricks, A.; Linden, S.; Choksy, S.; Stone, E.; Daumit, G.L. An innovative model to coordinate healthcare and social services for people with serious mental illness: A mixed-methods case study of Maryland’s Medicaid health home program. Gen. Hosp. Psychiatry 2018, 51, 54–62. [Google Scholar] [CrossRef]
- Gibson, L.; Bartlem, K.; Clinton-McHarg, T.; Wilczynska, M.; Rasmussen, A.; Bailey, J.; Ryall, J.; Orr, M.; Ford, J.; Bowman, J. The Provision of Preventive Care for Chronic Disease Risk Behaviours to People with a Mental Health Condition: A Survey of Staff from One Australian Community Managed Organisation. J. Psychosoc. Rehabil. Ment. Health 2021, 8, 191–198. [Google Scholar] [CrossRef]
- Creswell, J.W.; Poth, C.N. Five qualitative approaches to inquiry. In Qualitative Inquiry and Research Design: Choosing Among Five Approaches, 4th ed.; Creswell, J.Q., Poth, C.N., Eds.; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Turner, D.W. Qualitative Interview Design: A Practical Guide for Novice Investigators. Qual. Rep. 2010, 15, 754–760. [Google Scholar] [CrossRef]
- NSW Ministry of Health. Housing and Accommodation Support Initiative (HASI). Available online: https://www.health.nsw.gov.au/mentalhealth/services/adults/Pages/hasi.aspx (accessed on 10 August 2021).
- NSW Ministry of Health. Community Living Supports (CLS). Available online: https://www.health.nsw.gov.au/mentalhealth/services/adults/Pages/community-living-supports.aspx (accessed on 10 August 2021).
- National Disability Insurance Agency. NDIS. Available online: https://www.ndis.gov.au/ (accessed on 12 August 2021).
- Australian Government Department of Health. Fact Sheet: Primary Health Networks. Available online: https://www1.health.gov.au/internet/main/publishing.nsf/Content/Fact-Sheet-Primary-Health-Networks+ (accessed on 12 August 2021).
- Hancock, N.; Gye, B.; Digolis, C.; Smith-Merry, J.; Borilovic, J.; De Vries, J. Commonwealth Mental Health Programs Monitoring Project: Tracking Transitions of People from PIR, PHaMs and D2DL Into the NDIS. Final Report; The University of Sydney & Community Mental Health Australia: Sydney, Australia, 2019. [Google Scholar]
- WayAhead. WayAhead Directory. Available online: https://directory.wayahead.org.au/ (accessed on 1 November 2018).
- Hennink, M.M.; Kaiser, B.N.; Marconi, V.C. Code Saturation Versus Meaning Saturation: How Many Interviews Are Enough? Qual. Health Res. 2017, 27, 591–608. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Ennals, P.; Muchamore, I.; Langan, V.; Hall, C.; Wolstencroft, K. Active8: Promoting health beyond the absence of mental illness. Aust. J. Rural. Health 2020, 28, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Lo, B. Health Prompt Review: Evaluation Report; Neami National: Rosanna, VIC, Australia, 2014. [Google Scholar]
- Hanusaik, N.; Sabiston, C.M.; Kishchuk, N.; Maximova, K.; O’Loughlin, J. Association between organizational capacity and involvement in chronic disease prevention programming among Canadian public health organizations. Health Educ. Res. 2015, 30, 206–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, S.E.; Mitrou, F.; Lawrence, D.; Zubrick, S.R.; Wolstencroft, K.; Ennals, P.; Hall, C.; McNaught, E. The Effectiveness of a Consumer Centred Tobacco Management (CCTM) Approach in Enabling Mental Health Consumers to Reduce or Quit Smoking–A Pilot Study; Neami National: Preston, VIC, Australia, 2019. [Google Scholar]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage: Newbury Park, CA, USA, 1985. [Google Scholar]
- Braun, V.; Clarke, V. Reflecting on reflexive thematic analysis. Qual. Res. Sport Exerc. Health 2019, 11, 589–597. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dray, J.; Gibson, L.; Clinton-McHarg, T.; Byrnes, E.; Wynne, O.; Bartlem, K.; Wilczynska, M.; Latter, J.; Fehily, C.; Wolfenden, L.; et al. Exploring Support Provided by Community Managed Organisations to Address Health Risk Behaviours Associated with Chronic Disease among People with Mental Health Conditions: A Qualitative Study with Organisational Leaders. Int. J. Environ. Res. Public Health 2022, 19, 5533. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095533
Dray J, Gibson L, Clinton-McHarg T, Byrnes E, Wynne O, Bartlem K, Wilczynska M, Latter J, Fehily C, Wolfenden L, et al. Exploring Support Provided by Community Managed Organisations to Address Health Risk Behaviours Associated with Chronic Disease among People with Mental Health Conditions: A Qualitative Study with Organisational Leaders. International Journal of Environmental Research and Public Health. 2022; 19(9):5533. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095533
Chicago/Turabian StyleDray, Julia, Lauren Gibson, Tara Clinton-McHarg, Emma Byrnes, Olivia Wynne, Kate Bartlem, Magdalena Wilczynska, Joanna Latter, Caitlin Fehily, Luke Wolfenden, and et al. 2022. "Exploring Support Provided by Community Managed Organisations to Address Health Risk Behaviours Associated with Chronic Disease among People with Mental Health Conditions: A Qualitative Study with Organisational Leaders" International Journal of Environmental Research and Public Health 19, no. 9: 5533. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095533