
Factors Associated with Symptom Burden in Adults with Chronic Kidney Disease Undergoing Hemodialysis: A Prospective Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
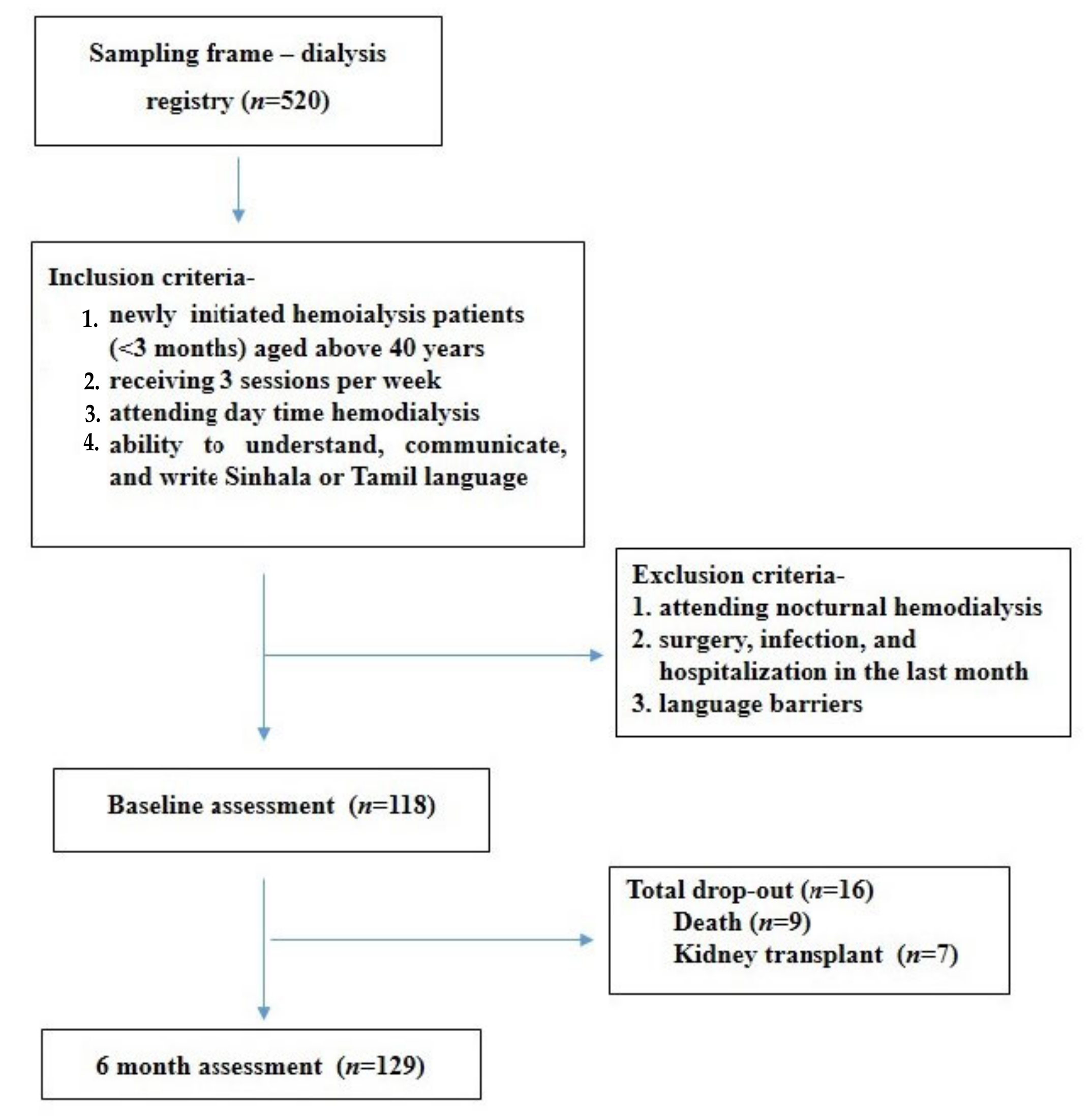
2.1. Study Design, Participants and Setting
2.2. Sample Size
2.3. Measures
2.3.1. Symptom Burden
2.3.2. Socio-Demographic Characteristics
2.3.3. Anthropometric Measurements and Clinical Characteristics
2.3.4. Stress
2.3.5. Illness Perception
2.3.6. Social Support
2.4. Ethical Considerations
2.5. Statistics
3. Results
3.1. Patient Characteristics
3.2. Prevalence, and Burden of Symptoms
3.3. Factors Associated with Symptom Burden among Patients on Hemodialysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- BANK AD. Growing Old before Becoming Rich: Challenges of an Aging Population in Sri Lanka: Asian Development Bank. 2019. Available online: https://0-scholar-google-com.brum.beds.ac.uk/scholar?hl=en&as_sdt=0%2C5&q=BANK.+AD.+Growing+old+before+becoming+rich%3A+Challenges+of+an+aging+population+in+Sri+Lanka%3A+Asian+Development+Bank%3B+2019.&btnG= (accessed on 1 April 2022).
- DESA UN. World Population Prospects 2019. United Nations. Department of Economic and Social Affairs. World Population Prospects. 2019. Available online: https://0-scholar-google-com.brum.beds.ac.uk/scholar?hl=en&as_sdt=0%2C5&q=U.+World+Population+Prospects+2019.+United+Nations.+Department+of+Economic+and+Social+Affairs.+World+Popula-tion+Prospects%2C+2019.+Available+online&btnG= (accessed on 20 December 2021).
- Senanayake, S.; Mahesh, P.K.B.; Gunawardena, N.; Graves, N.; Kularatna, S. Validity and internal consistency of EQ-5D-3L quality of life tool among pre-dialysis patients with chronic kidney disease in Sri Lanka, a lower mid-dle-income country. PLoS ONE 2019, 14, e0211604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemmelgarn, B.R.; Zhang, J.; Manns, B.J.; Tonelli, M.; Larsen, E.; Ghali, W.A.; Southern, D.A.; McLaughlin, K.; Mortis, G.; Culleton, B.F. Progression of kidney dysfunction in the community-dwelling elderly. Kidney Int. 2006, 69, 2155–2161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigo, C.; Samarakoon, L.; Rajapakse, S.; Lanerolle, R.; Sheriff, R. Kidney disease in the elderly: A Sri Lankan perspec-tive. Saudi J. Kidney Dis. Transplant. 2013, 24, 1285–1290. [Google Scholar] [CrossRef] [PubMed]
- Gooneratne, I.K.; Ranaweera, A.K.; Liyanarachchi, N.P.; Gunawardane, N.; Lanerolle, R.D. Epidemiology of chronic kidney disease in a Sri Lankan population. Int. J. Diabetes Dev. Ctries. 2008, 28, 60–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernando, W.B.N.T.; Nanayakkara, N.; Gunarathne, L.; Chandrajith, R. Serum and urine fluoride levels in populations of high environmental fluoride exposure with endemic CKDu: A case–control study from Sri Lanka. Environ. Geochem. Health 2020, 42, 1497–1504. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.; Misra, S.S.; Sahu, R.; Saxena, P.; Mathur, H.; Agarwal, H. Environmental Contamination and Its Association with Chronic Kidney Disease of Unknown Etiology in North Central Region of Sri Lanka 37; Centre for Science and Environment: New Delhi, India, 2012. [Google Scholar]
- Perera, W.P.R.T.; Dayananda, M.D.N.R.; Liyanage, J.A. Exploring the root cause for chronic kidney disease of unknown etiology (CKDU) via analysis of metal ion and counterion contaminants in drinking water: A study in Sri Lanka. J. Chem. 2020, 2020, 8670974. [Google Scholar] [CrossRef]
- Ruwanpathirana, T.; Senanayake, S.; Gunawardana, N.; Munasinghe, A.; Ginige, S.; Gamage, D.; Amarasekara, J.; Lokuketagoda, B.; Chulasiri, P.; Amunugama, S.; et al. Prevalence and risk factors for impaired kidney function in the district of Anuradhapura, Sri Lanka: A cross-sectional population-representative survey in those at risk of chronic kidney disease of unknown aetiology. BMC Public Health 2019, 19, 763. [Google Scholar] [CrossRef]
- Dyussenbayev, A. Age periods of human life. Adv. Soc. Sci. Res. J. 2017, 4, 258–263. [Google Scholar] [CrossRef] [Green Version]
- Yu, I.C.; Huang, J.Y.; Tsai, Y.F. Symptom cluster among hemodialysis patients in Taiwan. Appl. Nurs. Res. 2012, 25, 190–196. [Google Scholar] [CrossRef]
- Almutary, H.; Bonner, A.; Douglas, C. Symptom burden in chronic kidney disease: A review of recent literature. J. Ren. Care 2013, 39, 140–150. [Google Scholar] [CrossRef]
- Hui, D.S.; Wong, T.Y.; Ko, F.W.; Li, T.S.; Choy, D.K.; Wong, K.K.; Szeto, C.C.; Lui, S.F.; Li, P.K. Prevalence of sleep disturbances in Chinese patients with end-stage renal failure on continuous ambulatory peritoneal dialysis. Am. J. Kidney Dis. 2000, 36, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Merkus, M.P.; Jager, K.J.; Dekker, F.W.; de Haan, R.J.; Boeschoten, E.W.; Krediet, R. Physical symptoms and quality of life in patients on chronic dialysis: Results of the Netherlands Cooperative Study on Adequacy of Dialysis (NECOSAD). Nephrol. Dial. Transplant. 1999, 14, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Gapstur, R.L. Symptom burden: A concept analysis and implications for oncology nurses. Oncol. Nurs. Forum. 2007, 34, 673–680. [Google Scholar] [CrossRef] [Green Version]
- Lenz, E.R.; Pugh, L.C.; Milligan, R.A.; Gift, A.; Suppe, F. The middle-range theory of unpleasant symptoms: An update. Adv. Nurs. Sci. 1997, 19, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; Kim, B.; Park, K.S.; Choi, J.Y.; Seo, J.J.; Park, S.H.; Kim, C.D.; Kim, Y.L. Health-related quality of life with KDQOL-36 and its association with self-efficacy and treatment satisfaction in Korean dialysis patients. Qual. Life Res. 2013, 22, 753–758. [Google Scholar] [CrossRef] [Green Version]
- Almutary, H.; Bonner, A.; Douglas, C. Which patients with chronic kidney disease have the greatest symptom burden? A comparative study of advanced CKD stage and dialysis modality. J. Ren. Care 2016, 42, 73–82. [Google Scholar] [CrossRef]
- Gao, Y.; Zhou, Y. A survey of the status of symptom distress in maintenance hemodialysis patients. Mod. Prev. Med. 2014, 41, 2872–2874. (In Chinese) [Google Scholar]
- Abdel-Kader, K.; Unruh, M.L.; Weisbord, S.D. Symptom burden, depression, and quality of life in chronic and end-stage kidney disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 1057–1064. [Google Scholar] [CrossRef]
- Ludman, E.J.; Katon, W.; Russo, J.; Von Korff, M.; Simon, G.; Ciechanowski, P.; Lin, E.; Bush, T.; Walker, E.; Young, B. Depression and diabetes symptom burden. Gen. Hosp. Psychiatry 2004, 26, 430–436. [Google Scholar] [CrossRef]
- Dorian, P.; Jung, W.; Newman, D.; Paquette, M.; Wood, K.; Ayers, G.M.; Camm, J.; Akhtar, M.; Luderitz, B. The impairment of health-related quality of life in patients with intermittent atrial fibrillation: Implications for the assessment of investigational therapy. J. Am. Coll. Cardiol. 2000, 36, 1303–1309. [Google Scholar] [CrossRef] [Green Version]
- Ruo, B.; Rumsfeld, J.S.; Hlatky, M.A.; Liu, H.; Browner, W.S.; Whooley, M.A. Depressive symptoms and health-related quality of life: The Heart and Soul Study. JAMA 2003, 290, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Karasneh, R.; Al-Azzam, S.; Altawalbeh, S.M.; Alshogran, O.Y.; Hawamdeh, S. Predictors of symptom burden among hemodialysis patients: A cross-sectional study at 13 hospitals. Int. Urol. Nephrol. 2020, 52, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Weisbord, S.D.; Fried, L.F.; Arnold, R.M.; Rotondi, A.J.; Fine, M.J.; Levenson, D.J.; Switzer, G.E. Development of a symptom assessment instrument for chronic hemodialysis patients: The Dialysis Symptom Index. J. Pain Symptom Manag. 2004, 27, 226–240. [Google Scholar] [CrossRef] [PubMed]
- Jablonski, A. The multidimensional characteristics of symptoms reported by patients on hemodialysis. Nephrol. Nurs. J. 2007, 34, 29–37. [Google Scholar] [PubMed]
- Weisbord, S.D.; Carmody, S.S.; Bruns, F.J.; Rotondi, A.J.; Cohen, L.M.; Zeidel, M.L.; Arnold, R.M. Symptom burden, quality of life, advance care planning and the potential value of palliative care in severely ill haemodialysis patients. Nephrol. Dial. Transplant. 2003, 18, 1345–1352. [Google Scholar] [CrossRef] [Green Version]
- Nazar, L.; Herath, C.; Lokugama, H.; Priyadarshani, G.D.D.; De Silva, P.; Sigera, P.C.; Ranasinghe, A.V.; Beane, A.; Haniffa, R. SAT-231 quality of life and burden of symptoms in chronic kidney disease patients undergoing dialysis in Sri Lanka, a population-based study using an electronic renal registry. Kidney Int. Rep. 2019, 4, S103. [Google Scholar] [CrossRef]
- Senanayake, S.; Gunawardena, N.; Palihawadana, P.; Bandara, P.; Haniffa, R.; Karunarathna, R.; Kumara, P. Symptom burden in chronic kidney disease; a population based cross sectional study. BMC Nephrol. 2017, 18, 228. [Google Scholar] [CrossRef]
- Athuraliya, T.N.; Abeysekera, D.T.; Amerasinghe, P.H.; Kumarasiri, P.V.; Dissanayake, V. Prevalence of chronic kidney disease in two tertiary care hospitals: High proportion of cases with uncertain aetiology. Ceylon Med. J. 2009, 54, 23–25. [Google Scholar] [CrossRef] [Green Version]
- Cooray, T.; Wei, Y.; Zhong, H.; Zheng, L.; Weragoda, S.K.; Weerasooriya, A.R. Assessment of groundwater quality in CKDu affected areas of Sri Lanka: Implications for drinking water treatment. Int. J. Environ. Res. Public Health 2019, 16, 1698. [Google Scholar] [CrossRef] [Green Version]
- Wang, N.; Bai, X.; Jin, B.; Han, W.; Sun, X.; Chen, X. The association of serum cathepsin B concentration with age-related cardiovascular-renal subclinical state in a healthy Chinese population. Arch. Gerontol. Geriatr. 2016, 65, 146–155. [Google Scholar] [CrossRef]
- Caplin, B.; Kumar, S.; Davenport, A. Patients’ perspective of haemodialysis-associated symptoms. Nephrol. Dial. Transplant. 2011, 26, 2656–2663. [Google Scholar] [CrossRef] [PubMed]
- Tat, T.S.; Ulusoy, S.; Cansiz, M.; Ozkan, G.; Gul, S.; Bektas, O. Evaluation of nutritional parameters of hemodialysis patients. Hippokratia 2012, 16, 236. [Google Scholar]
- Polinder-Bos, H.A.; van Diepen, M.; Dekker, F.W.; Hoogeveen, E.K.; Franssen, C.F.; Gansevoort, R.T. Lower body mass index and mortality in older adults starting dialysis. Sci. Rep. 2018, 8, 1–9. [Google Scholar]
- Lee, E.-H. Review of the psychometric evidence of the perceived stress scale. Asian Nurs. Res. 2012, 6, 121–127. [Google Scholar] [CrossRef] [Green Version]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The brief illness perception questionnaire. J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar] [CrossRef]
- Hettiarachchi, R.; Abeysena, C. Association of poor social support and financial insecurity with psychological distress of chronic kidney disease patients attending national nephrology unit in Sri Lanka. Int. J. Nephrol. 2018, 2018, 5678781. [Google Scholar] [CrossRef]
- Chowdhury, R.; Peel, N.M.; Krosch, M.; Hubbard, R.E. Frailty and chronic kidney disease: A systematic review. Arch. Gerontol. Geriatr. 2017, 68, 135–142. [Google Scholar] [CrossRef] [Green Version]
- Shagina, N.B.; Tolstykh, E.I.; Degteva, M.O.; Anspaugh, L.R.; Napier, B.A. Cortical bone resorption rate in elderly persons: Estimates from long-term in vivo measurements of 90Sr in the skeleton. Arch. Gerontol. Geriatr. 2012, 54, e411–e418. [Google Scholar] [CrossRef]
- Zhang, J.X.; Li, J.; Chen, C.; Yin, T.; Wang, Q.A.; Li, X.X.; Wang, F.X.; Zhao, J.H.; Zhao, Y.; Zhang, Y.H. Reference values of skeletal muscle mass, fat mass and fat-to-muscle ratio for rural middle age and older adults in western China. Arch. Gerontol. Geriatr. 2021, 95, 104389. [Google Scholar] [CrossRef]
- Ranasinghe, A.V.; Kumara, G.W.G.P.; Karunarathna, R.H.; De Silva, A.P.; Sachintani, K.G.D.; Gunawardena, J.M.C.N.; Kumari, S.K.C.R.; Sarjana, M.S.F.; Chandraguptha, J.S.; De Silva, M.V.C. The incidence, prevalence and trends of Chronic Kidney Disease and Chronic Kidney Disease of uncertain aetiology (CKDu) in the North Central Province of Sri Lanka: An analysis of 30,566 patients. BMC Nephrol. 2019, 20, 338. [Google Scholar] [CrossRef]
- Murtagh, F.E.M.; Marsh, J.E.; Donohoe, P.; Ekbal, N.J.; Sheerin, N.S.; Harris, F.E. Dialysis or not? A comparative survival study of patients over 75 years with chronic kidney disease stage 5. Nephrol. Dial. Transplant. 2007, 22, 1955–1962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abeywickrama, H.M.; Wimalasiri, S.; Koyama, Y.; Uchiyama, M.; Shimizu, U.; Kakihara, N.; Chandrajith, R.; Nanayakkara, N. Quality of life and symptom burden among chronic kidney disease of uncertain etiology (CKDu) patients in Girandurukotte, Sri Lanka. Int. J. Environ. Res. Public Health 2020, 17, 4041. [Google Scholar] [CrossRef] [PubMed]
- Siriwardhana, E.R.I.; Perera, P.A.; Sivakanesan, R.; Abeysekara, T.; Nugegoda, D.B.; Weerakoon, K.G. Is the staple diet eaten in Medawachchiya, Sri Lanka, a predisposing factor in the development of chronic kidney disease of unknown etiology?—A comparison based on urinary β 2-microglobulin measurements. BMC Nephrol. 2014, 15, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbott, K.C.; Glanton, C.W.; Trespalacios, F.C.; Oliver, D.K.; Ortiz, M.I.; Agodoa, L.Y.; Kimmel, P.L. Body mass index, dialysis modality, and survival: Analysis of the United States renal data system dialysis morbidity and mortality wave II study. Kidney Int. 2004, 65, 597–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, K.L.; MacLaughlin, H.L. Unintentional weight loss is an independent predictor of mortality in a hemodialysis population. J. Ren. Nutr. 2010, 20, 414–418. [Google Scholar] [CrossRef]
- Senanayake, S.; Gunawardena, N.; Palihawadana, P.; Suraweera, C.; Karunarathna, R.; Kumara, P. Depression and psychological distress in patients with chronic renal failure: Prevalence and associated factors in a rural district in Sri Lanka. J. Psychosom. Res. 2018, 112, 25–31. [Google Scholar] [CrossRef]
- Tan, T.; Brennan, F.; Brown, M.A. Impact of dialysis on symptom burden and functional state in the elderly. Ren. Soc. Australas. J. 2017, 13, 22–30. [Google Scholar]
- Moskovitch, J.T.; Mount, P.F.; Davies, M.R.P. Changes in symptom burden in dialysis patients assessed using a symptom-reporting questionnaire in clinic. J. Palliat. Care 2020, 35, 59–65. [Google Scholar] [CrossRef]
- Wan Zukiman, W.Z.H.; Yaakup, H.; Zakaria, N.F.; Shah, S.A.B. Symptom prevalence and the negative emotional states in end-stage renal disease patients with or without renal replacement therapy: A cross-sectional analysis. J. Palliat. Med. 2017, 20, 1127–1134. [Google Scholar] [CrossRef]
- Bruce, M.A.; Griffith, D.M.; Thorpe, R.J., Jr. Stress and the kidney. Advances in Chronic Kidney Disease. Natl. Kidney Found. 2015, 22, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Rajapakse, S.; Shivanthan, M.C.; Selvarajah, M. Chronic kidney disease of unknown etiology in Sri Lanka. Int. J. Occup. Environ. Health 2016, 22, 259–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alharbi, A.A.; Alharbi, Y.A.; Alsobhi, A.S.; Alharbi, M.A.; Alharbi, M.A.; Aljohani, A.A.; Alharbi, A.A. Impact of illness perception on the health-related quality of life of patients receiving dialysis: A cross-sectional study. Cureus 2021, 13, e15705. [Google Scholar] [CrossRef]
- Pagels, A.A.; Söderquist, B.K.; Heiwe, S. Differences in illness representations in patients with chronic kidney disease. J. Ren. Care 2015, 41, 146–155. [Google Scholar] [CrossRef] [PubMed]
- Strugała, M.; Talarska, D.; Kalfoss, M.; Niewiadomski, T.; Rozmarynowska, B.; Dyk, D. Perception of illness by patients treated with haemodialysis. Med. Res. J. 2019, 4, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Hagger, M.S.; Orbell, S. A meta-analytic review of the common-sense model of illness representations. Psychol. Health 2003, 18, 141–184. [Google Scholar] [CrossRef]
- Hale, E.D.; Treharne, G.J.; Kitas, G.D. The common-sense model of self-regulation of health and illness: How can we use it to understand and respond to our patients’ needs? Rheumatology 2007, 46, 904–906. [Google Scholar] [CrossRef] [Green Version]
- Broadbent, E.; Ellis, C.J.; Thomas, J.; Gamble, G.; Petrie, K.J. Further development of an illness perception intervention for myocardial infarction patients: A randomized controlled trial. J. Psychosom. Res. 2009, 67, 17–23. [Google Scholar] [CrossRef]
- Song, Y.Y.; Chen, L.; Yu, W.W.; Wang, W.X.; Yang, D.J.; Jiang, X.L. Correlates of symptom burden of hemodialysis patients. West. J. Nurs. Res. 2021, 43, 459–467. [Google Scholar] [CrossRef]
- Kessler, R.C.; Ormel, J.; Demler, O.; Stang, P.E. Comorbid mental disorders account for the role impairment of commonly occurring chronic physical disorders: Results from the National comorbidity Survey. J. Occup. Environ. Med. 2003, 45, 1257–1266. [Google Scholar] [CrossRef]
- Liu, Y.M.; Chang, H.J.; Wang, R.H.; Yang, L.K.; Lu, K.C.; Hou, Y.C. Role of resilience and social support in alleviating depression in patients receiving maintenance hemodialysis. Ther. Clin. Risk Manag. 2018, 14, 441–451. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Baseline n (%) | 6 Months n (%) |
|---|---|---|
| Age groups | ||
| 40–55 years | 67 (44.1) | 57 (37.5) |
| >56 years | 51 (33.6) | 46 (29.6) |
| Gender: | ||
| Male | 75 (63.6) | 64 (62.7) |
| Female | 43 (36.4) | 38 (37.3) |
| Marital status | ||
| Unmarried | 5 (4.2) | 5 (4.9) |
| Ever married | 113 (95.8) | 97 (95.1) |
| Education | ||
| Primary | 16 (13.6) | 12 (11.7) |
| Secondary | 67 (56.8) | 58 (56.8) |
| Tertiary/diploma | 35 (29.7) | 32 (31.5) |
| Occupation: | ||
| Employed in government/private | 37 (31.3) | 33 (32.3) |
| Unemployed | 54 (45.8) | 45 (44.2) |
| Self-employed | 27 (22.9) | 24 (23.5) |
| Income LKR (USD): | ||
| <10,000 LKR (<50) | 17 (14.4) | 16 (13.6) |
| 10,001–25,000 LKR (50–127) | 46 (39) | 41 (34.7) |
| >25,001 LKR (>127) | 55 (46.6) | 45 (38.1) |
| Co-morbidities: | ||
| Diabetes only | 19 (16.1) | 15 (14.7) |
| Hypertension only | 45 (38.1) | 40 (39.2) |
| Diabetes and Hypertension | 39 (33.1) | 35 (34.3) |
| Others | 15 (12.7) | 12 (11.8) |
| Characteristics | Total Mean (SD) | 40–55 Years Mean (SD) | >55 Years Mean (SD) | p |
|---|---|---|---|---|
| Baseline | ||||
| Weight * (kg) a | 58.40 (11.3) | 58.41 (12.6) | 58.40 (8.9) | 0.91 |
| Height (cm) a | 164.01 (10.8) | 163.70 (11.4) | 164.42 (10.1) | 0.72 |
| BMI (kg/m2) b | 21.86 (4.5) | 21.9 (4.8) | 21.8 (4) | 0.89 |
| MpreBP (Hamm) a | 121.79 (20.4) | 122.03 (20.4) | 121.47 (20.6) | 0.88 |
| MpostBP (Hgmm) a | 127.04 (21.9) | 125.26 (20.3) | 129.4 (23.9) | 0.31 |
| Hb (g/dL) a | 9.20 (1.7) | 8.93 (1.8) | 9.57 (1.6) | 0.05 * |
| S.Creatiine (mg/dL) a | 733.23 (329.9) | 750.90 (328.5) | 710 (333.7) | 0.88 |
| S.Albumin (g/dL) b | 3.59 (0.7) | 3.59 (0.7) | 3.58 (0.6) | 0.50 |
| BUN (mg/dL) a | 16.3 (7) | 16.4 (7) | 15.8 (6.5) | 0.64 |
| Stress a | 22.6 (6.5) | 22.64 (6.3) | 22.57 (6.9) | 0.91 |
| Illness perception a | 53.4 (9.3) | 53.04 (8.3) | 53.9 (10.6) | 0.63 |
| Social support a | 27.6 (7.3) | 27.25 (7.6) | 28.2 (7.09) | 0.51 |
| Symptom burden a | 67.04 (22.6) | 66.46 (21.9) | 67.8 (23.7) | 0.74 |
| 6 months | ||||
| Weight * (kg) a | 56.86 (10.6) | 57.4 (11.3) | 56.1 (9.6) | 0.23 |
| Height (cm) a | 164.01 (10.7) | 163.6 (11.5) | 164.59 (9.7) | 0.16 |
| BMI (kg/m2) b | 21.33 (4.6) | 27.7 (5.1) | 20.9 (1.09) | 0.57 |
| MpreBP (Hgmm) a | 117.4 (18.4) | 121.36 (19.65) | 112.04 (15.7) | 0.03 * |
| MpostBP (Hgmm) a | 120.1 (16.8) | 122.76 (17.7) | 116.8 (15.8) | 0.63 |
| Hb (g/dL) a | 9.45 (1.8) | 9.2 (1.9) | 9.8 (1.6) | 0.47 |
| S.Creatiine (mg/dL) a | 703.45 (253.1) | 711.8 (263.4) | 692.9 (241.9) | 0.71 |
| S.Albumin (g/dL) b | 4.05 (1.02) | 4.08 (0.9) | 4.01 (1.04) | 0.30 |
| BUN (mg/dL) a | 15.48 (5.2) | 14.73 (5.3) | 16.42 (5.1) | 0.49 |
| Stress a | 27.3 (5.1) | 27.94 (4.9) | 26.5 (5.3) | 0.11 |
| Illness perception a | 56.5 (12.3) | 57.3 (11.7) | 55.56 (13) | 0.43 |
| Social support a | 28.6 (6.2) | 28.5 (5.9) | 28.8 (6.7) | 0.70 |
| Symptom burden a | 53.1 (29.7) | 55.3 (28.4) | 51.1 (30.8) | 0.41 |
| Symptom | Frequency (%) | Prevalence by Age Group n (%) | p | |
|---|---|---|---|---|
| 40–45 Years | >55 Years | |||
| Baseline | n = 118 | n = 67 | n = 51 | |
| Fatigue b | 115 (97.5) | 64 (95.5) | 51 (100) | 0.17 |
| Loss/decreased libido b | 107 (90.7) | 64 (95.5) | 47 (92.2) | 0.55 |
| Loss of appetite b | 108 (91.5) | 64 (95.5) | 44 (86.3) | 0.06 |
| Swelling b | 109 (94.2) | 61 (91) | 48 (94.1) | 0.39 |
| Dry skin b | 109 (94.2) | 61 (91) | 48 (94.1) | 0.38 |
| Insomnia b | 107 (90.7) | 61 (91) | 46 (90.2) | 0.56 |
| Impotence b | 107 (90.7) | 61 (91) | 46 (90.2) | 0.35 |
| Difficulty keeping legs still b | 109 (94.2) | 60 (89.6) | 46 (90.2) | 0.33 |
| Nausea b | 107 (90.7) | 60 (89.6) | 47 (92.2) | 0.44 |
| 6 months | n = 102 | n = 57 | n = 45 | |
| Fatigue b | 95 (94.5) | 55 (92.9) | 40 (88.8) | 0.49 |
| Insomnia b | 94 (92.2) | 52 (91.2) | 42 (93.3) | 0.21 |
| Loss of appetite b | 92 (90.2) | 52 (91.2) | 40 (88.8) | 0.06 |
| Difficulty keeping legs still b | 92 (90.2) | 51 (89.5) | 41 (91.1) | 0.52 |
| Sadness b | 88 (86.3) | 51 (89.5) | 37 (82.2) | 0.22 |
| Dry skin b | 87 (85.3) | 50 (87.7) | 37 (82.2) | 0.31 |
| Changes in skin color b | 84 (82.4) | 50 (87.7) | 34 (75.6) | 0.09 |
| Lethargy b | 86 (84.3) | 49 (86) | 37 (82.2) | 0.41 |
| Joint pain b | 91 (89.2) | 48 (84.2) | 43 (95.6) | 0.06 |
| Loss/decreased libido b | 77 (75.5) | 48 (84.2) | 29 (64.4) | 0.02* |
| Impotence | 77 (75.5) | 48 (84.2) | 29 (64.4) | 0.02* |
| Characteristics | Baseline (n = 118) | 6 Months (n = 102) | ||
|---|---|---|---|---|
| Mean Rank | U/H/r (p) | Mean Rank | U/H/r (p) | |
| Socio-demographic factors | ||||
| Age groups: 40–55 years | 58.4 | 1633 c (0.6) | 53.7 | 1155 c (0.4) |
| >55 years | 61 | 48.6 | ||
| Gender: Male | 60.1 | 1585 c (0.8) | 51 | 1198 c (0.9) |
| Female | 59.1 | 51.7 | ||
| Marital status: Unmarried | 70.8 | 226 c (0.4) | 56 | 220 c (0.7) |
| Ever married | 59 | 51.3 | ||
| Education: Up to primary | 59.34 | 1.4 b (0.5) | 45.8 | 1.01 b (0.6) |
| Up to secondary | 56.6 | 50.6 | ||
| Tertiary | 65 | 55.2 | ||
| Income: <10,000 (<50) | 66.8 | 1.09 b (0.6) | 55.7 | 0.4 b (0.8) |
| 10,000–25000 (50–127) | 59.9 | 51.2 | ||
| >25,000 (>127) | 56.9 | 50.3 | ||
| Occupation: Employed | 52.2 | 2.8 b (0.2) | 52.2 | 2.8 b (0.2) |
| Self employed | 61.2 | 61.2 | ||
| Unemployed | 66 | 66.1 | ||
| Co-morbidities: DM | 67.7 | 8.6 b (0.03) * | 59.5 | 9.5 b (0.02) * |
| HT | 48.6 | 40.8 | ||
| DM and HT | 62.6 | 55.8 | ||
| Others | 73.9 | 64.6 | ||
| Anthropometric and clinical parameters | ||||
| Weight (post dialysis) | - | −0.15 a (0.1) | - | −0.22 a (0.02) * |
| Height | - | −0.11 a (0.2) | - | −0.06 a (0.5) |
| BMI | - | −0.05 a (0.5) | - | −0.15 a (0.14) |
| MpreBP | - | 0.07 a (0.5) | - | 0.11 a (0.25) |
| MpostBP | - | 0.05 a (0.6) | - | 0.02 a (0.8) |
| Hemoglobin (mg/dl) | - | −0.17 a (0.07) | - | −0.16 a (0.9) |
| Creatinine (mg/dl) | - | −0.08 a (0.3) | - | −0.05 a (0.6) |
| Albumin (mg/dl) | - | 0.03 a (0.8) | - | 0.1 a (0.3) |
| BUN | - | 0.14 a (0.1) | - | −0.06 a (0.5) |
| Psychosocial factors | ||||
| Stress | - | 0.8 a (<0.005) ** | - | 0.34 a (<0.005) ** |
| Illness perception | - | 0.7 a (<0.005) | - | 0.24 a (<0.01) * |
| Social support | - | −0.14 a (0.14) | - | −0.2 a (0.04) * |
| Determinant | 95% CI for β | |||||
|---|---|---|---|---|---|---|
| USC B | SE | β | p | Lower Bound | Upper Bound | |
| Baseline | ||||||
| Having hypertension | 1.91 | 2.9 | 0.04 | 0.4 | −3.9 | 7.8 |
| Having diabetes and hypertension | −2.75 | 3.3 | −0.05 | 0.5 | −9.2 | 3.7 |
| Perceived stress score | 2.26 | 0.3 | 0.65 | <0.005 ** | 1.7 | 2.8 |
| Illness perception score | 0.5 | 0.21 | 0.21 | 0.02 * | 0.09 | 0.9 |
| 6 months | ||||||
| Having hypertension | −6.48 | 6.4 | −0.11 | 0.3 | −19.16 | 6.2 |
| Having diabetes and hypertension | −7.3 | 7.1 | −0.11 | 0.3 | −21.16 | 6.63 |
| Post dialysis body weight | −0.54 | 0.25 | −0.19 | 0.03 * | −1.04 | −0.04 |
| Perceived stress score | 1.7 | 0.53 | 0.28 | 0.003 ** | 0.57 | 2.66 |
| Illness perception score | 0.5 | 0.23 | 0.2 | 0.03 * | 0.18 | 1.93 |
| Social support | −1.05 | 0.44 | −0.22 | 0.02 * | 0.18 | 1.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gunarathne, T.G.N.S.; Tang, L.Y.; Lim, S.K.; Nanayakkara, N.; Damayanthi, H.D.W.T.; Abdullah, K.L. Factors Associated with Symptom Burden in Adults with Chronic Kidney Disease Undergoing Hemodialysis: A Prospective Study. Int. J. Environ. Res. Public Health 2022, 19, 5540. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095540
Gunarathne TGNS, Tang LY, Lim SK, Nanayakkara N, Damayanthi HDWT, Abdullah KL. Factors Associated with Symptom Burden in Adults with Chronic Kidney Disease Undergoing Hemodialysis: A Prospective Study. International Journal of Environmental Research and Public Health. 2022; 19(9):5540. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095540
Chicago/Turabian StyleGunarathne, Thalwaththe Gedara Nadeeka Shayamalie, Li Yoong Tang, Soo Kun Lim, Nishantha Nanayakkara, Hewaratne Dassanayakege Wimala Thushari Damayanthi, and Khatijah L. Abdullah. 2022. "Factors Associated with Symptom Burden in Adults with Chronic Kidney Disease Undergoing Hemodialysis: A Prospective Study" International Journal of Environmental Research and Public Health 19, no. 9: 5540. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095540