
Early Adversity and Changes in Cortisol and Negative Affect in Response to Interpersonal Threats in the Laboratory


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
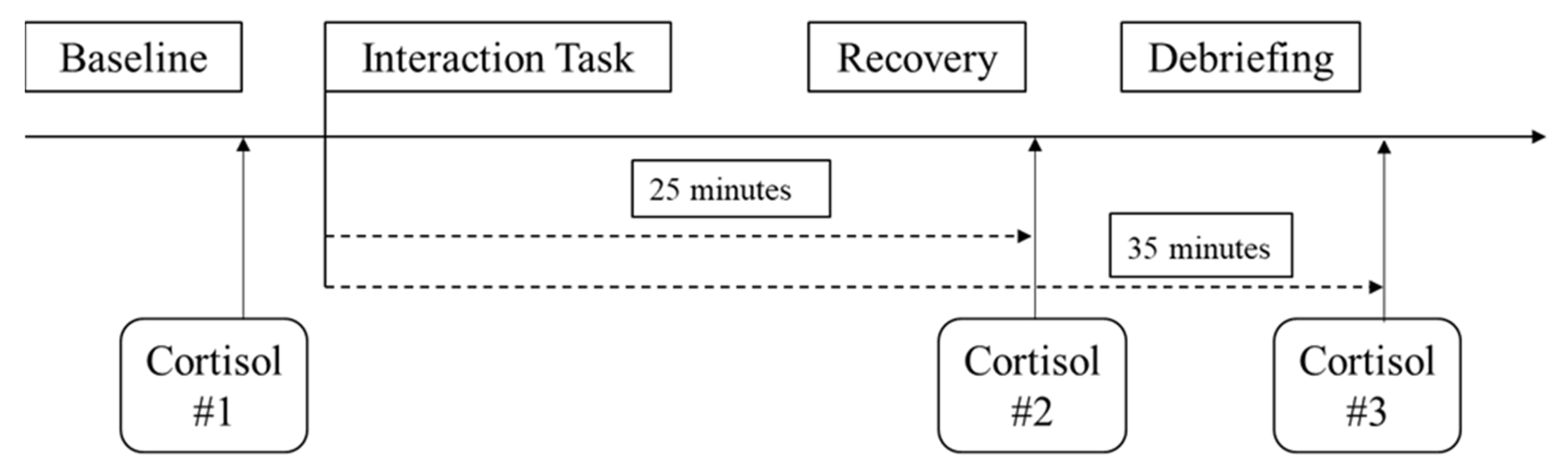
2.2. Design and Procedures
2.3. Manipulated Conditions
2.3.1. Social Evaluative Threat
2.3.2. Participant Relative Social Status Manipulation
2.3.3. Partner Dominance Manipulation
2.4. Measures
2.4.1. Social Status
2.4.2. Adverse Childhood Experiences
2.4.3. Cortisol Reactivity
2.4.4. Changes in Negative Affect
2.5. Overview of Analyses
3. Results
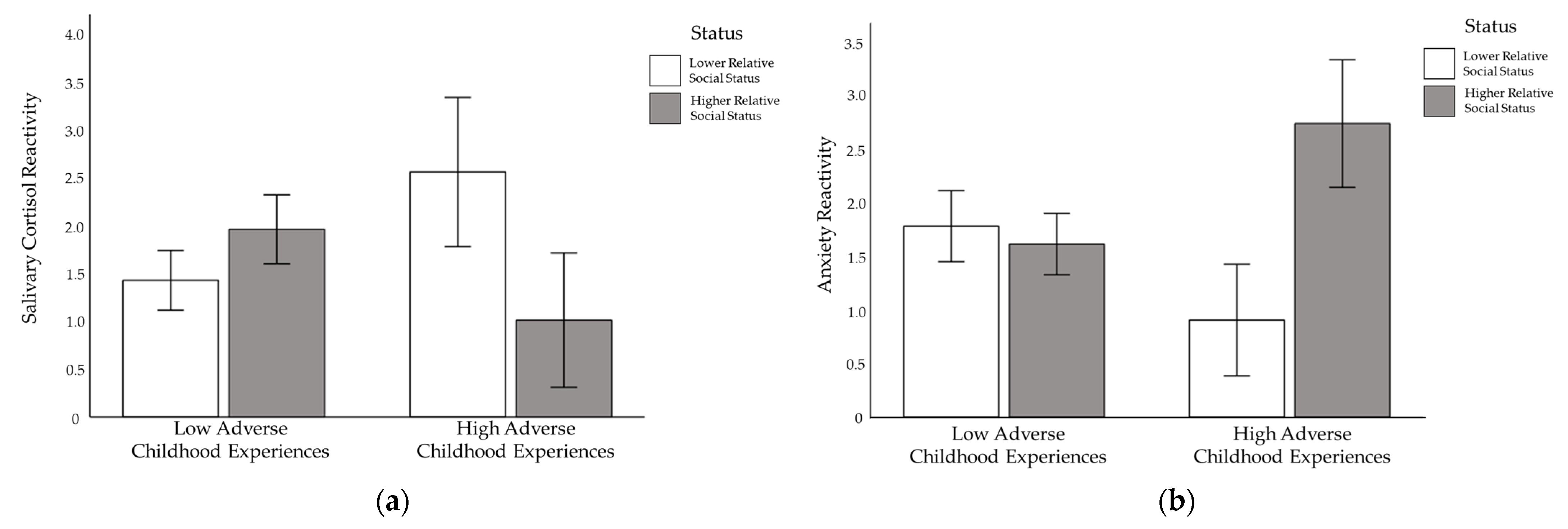
3.1. Cortisol Reactivity
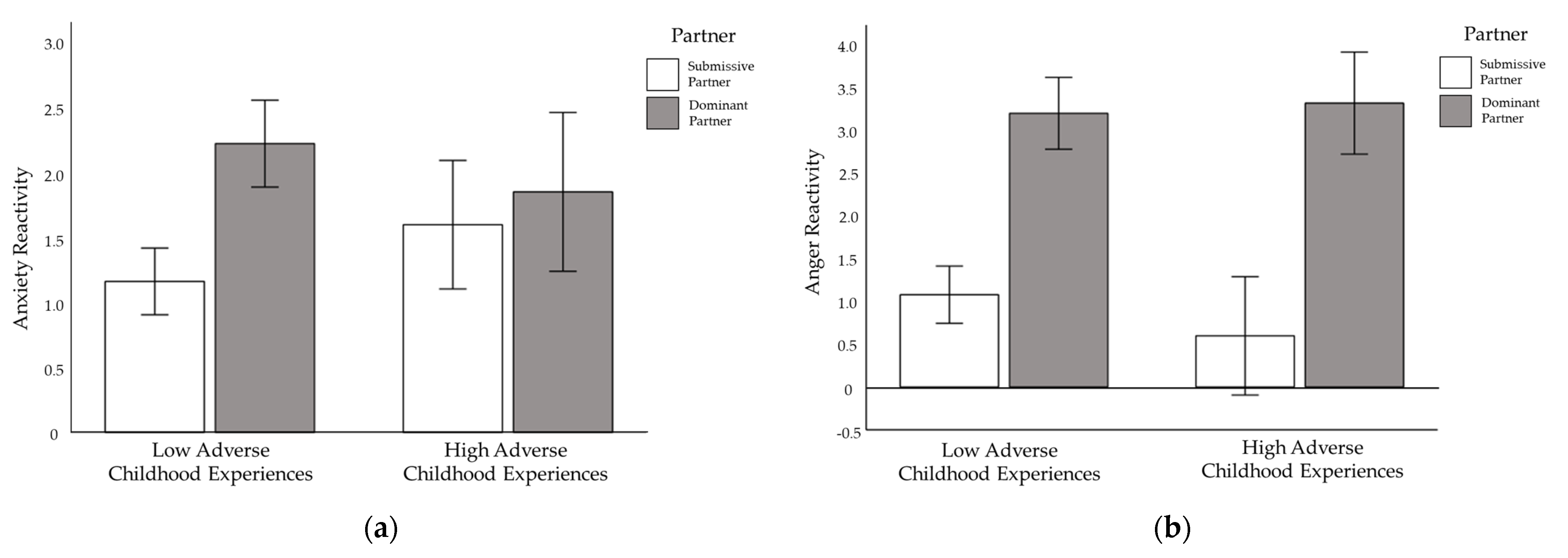
3.2. Negative Affect Reactivity
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Koss, M.P.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The Adverse Childhood Experiences (ACE) Study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Repetti, R.L.; Taylor, S.E.; Seeman, T.E. Risky families: Family Social environments and the Mental and Physical Health of Offspring. Psychol. Bull. 2002, 128, 330–366. [Google Scholar] [CrossRef] [PubMed]
- Shonkoff, J.P.; Boyce, W.T.; McEwen, B.S. Neuroscience, Molecular Biology, and the Childhood Roots of Health Disparities: Building a New Framework for Health Promotion and Disease Prevention. J. Am. Med. Assoc. 2009, 301, 2252–2259. [Google Scholar] [CrossRef] [PubMed]
- Doom, J.R.; Cook, S.H.; Sturza, J.; Kaciroti, N.; Gearhardt, A.N.; Vazquez, D.M.; Lumeng, J.C.; Miller, A.L. Family conflict, chaos, and negative life events predict cortisol activity in low-income children. Dev. Psychobiol. 2018, 60, 364–379. [Google Scholar] [CrossRef] [Green Version]
- Troxel, W.M.; Matthews, K.A. What are the Costs of Marital Conflict and Dissolution to Children’s Physical Health? Clin. Child Fam. Psychol. Rev. 2004, 7, 29–57. [Google Scholar] [CrossRef]
- Bradley, B.; Westen, D.; Mercer, K.B.; Binder, E.B.; Jovanovic, T.; Crain, D.; Wingo, A.; Heim, C. Association between childhood maltreatment and adult emotional dysregulation in a low-income, urban, African American sample: Moderation by oxytocin receptor gene. Dev. Psychopathol. 2015, 23, 439–452. [Google Scholar] [CrossRef] [Green Version]
- Rogosch, F.; Cicchetti, D.; Aber, J. The role of child maltreatment in early deviations in cognitive and affective processing abilities and later peer relationship problems. Dev. Psychopathol. 1995, 7, 591–609. [Google Scholar] [CrossRef]
- Shields, A.; Cicchetti, D. Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Dev. Psychol. 1997, 33, 906–916. [Google Scholar] [CrossRef]
- Shields, A.; Cicchetti, D. Reactive aggression among maltreated children: The contributions of attention and emotion dysregulation. J. Clin. Child Psychol. 1998, 27, 381–395. [Google Scholar] [CrossRef]
- Heleniak, C.; Jeness, J.L.; Stoep, A.V.; McCauley, E.; McLaughlin, K.A. Childhood maltreatment exposure and disruptions in emotion regulation: A transdiagnostic pathway to adolescent internalizing and externalizing psychopathology. Cogn. Ther. Res. 2016, 40, 394–415. [Google Scholar] [CrossRef] [Green Version]
- Suls, J.; Bunde, J. Anger, anxiety, and depression as risk factors for cardiovascular disease: The problems and implications of overlapping affective dispositions. Psychol. Bull. 2005, 131, 260–300. [Google Scholar] [CrossRef] [PubMed]
- Chorpita, B.F.; Barlow, D.H. The development of anxiety: The role of control in the early environment. Psychol. Bull. 1998, 124, 3–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haukkala, A.; Konttinen, H.; Laatikainen, T.; Ichiro, K.; Antti, U. Hostility, anger control, and anger expression as predictors of cardiovascular disease. Psychosom. Med. 2010, 72, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.E.; Way, B.M.; Seeman, T.E. Early adversity and adult health outcomes. Dev. Psychopathol. 2011, 23, 939–954. [Google Scholar] [CrossRef] [Green Version]
- Capobianco, L.; Morris, J.A.; Wells, A. Worry and rumination: Do they prolong physiological and affective recovery from stress? Anxiety Stress Coping 2018, 31, 291–303. [Google Scholar] [CrossRef] [PubMed]
- Nusslock, R.; Miller, G.E. Early-Life Adversity and Physical and Emotional Health across the Lifespan: A Neuroimmune Network Hypothesis. Biol. Psychiatry 2016, 80, 23–32. [Google Scholar] [CrossRef] [Green Version]
- Weaver, I.C. Shaping adult phenotypes through early life environments. Birth Defects Res. Part C Embryo Today 2009, 87, 314–326. [Google Scholar] [CrossRef]
- Tarullo, A.R.; Gunnar, M.R. Child maltreatment and the developing HPA axis. Horm. Behav. 2006, 50, 632–639. [Google Scholar] [CrossRef]
- Bozovic, D.; Racic, M.; Ivkovic, N. Salivary Cortisol Levels as a Biological Marker of Stress Reaction. Med. Arch. 2013, 65, 371–374. [Google Scholar] [CrossRef] [Green Version]
- Schwabe, L.; Haddad, L.; Schachinger, H. HPA axis activation by a socially evaluated cold-pressor test. Psychoneuroendocrinology 2008, 33, 890–895. [Google Scholar] [CrossRef]
- Steptoe, A.; Kivimäki, M. Stress and cardiovascular disease: An update on current knowledge. Annu. Rev. Public Health 2013, 34, 337–354. [Google Scholar] [CrossRef] [PubMed]
- Peckins, M.K.; Dockray, S.; Eckenrode, J.L.; Heaton, J.; Susman, E.J. The longitudinal impact of exposure to violence on cortisol reactivity in adolescents. J. Adolesc. Health 2012, 51, 366–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhlman, K.R.; Geiss, E.G.; Vargas, I.; Lopez-Duran, N.L. Differential associations between childhood trauma subtypes and adolescent HPA-axis functioning. Psychoneuroendocrinology 2014, 54, 103–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dedovic, K.; Renwick, R.; Mahani, N.K.; Engert, V.; Lupien, S.J.; Pruessner, J.C. The Montreal Imaging Stress Task: Using functional imaging to investigate the effects of perceiving and processing psychosocial stress in the human brain. J. Psychiatry Neurosci. JPN 2005, 30, 319–325. [Google Scholar]
- Voellmin, A.; Winzeler, K.; Hug, E.; Wilhelm, F.H.; Schaefer, V.; Gaab, J.; Marca, R.L.; Pruessner, J.C.; Bader, K. Blunted endocrine and cardiovascular reactivity in young healthy women reporting a history of childhood adversity. Psychoneuroendocrinology 2015, 51, 58–67. [Google Scholar] [CrossRef] [Green Version]
- Thastum, M.; Zachariae, R.; Bjerring, P.; Herlin, T. Cold pressor pain: Comparing responses of juvenile arthritis patients and their parents. Scand. J. Rheumatol. 1997, 26, 272–279. [Google Scholar] [CrossRef]
- Kirschbaum, C.; Pirke, K.M.; Hellhammer, D.H. The ‘Trier Social Stress Test’—A tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology 1993, 28, 76–81. [Google Scholar] [CrossRef]
- Dickerson, S.S.; Kemeny, M.E. Acute Stressors and Cortisol Responses: A Theoretical Integration and Synthesis of Laboratory Research. Psychol. Bull. 2004, 130, 355–391. [Google Scholar] [CrossRef] [Green Version]
- Moons, W.G.; Eisenberger, N.I.; Taylor, S.E. Anger and fear responses to stress have different biological profiles. Brain Behav. Immun. 2010, 24, 215–219. [Google Scholar] [CrossRef]
- Hood, C.O.; Badour, C.L. The Effects of Posttraumatic Stress and Trauma-Focused Disclosure on Experimental Pain Sensitivity among Trauma-Exposed Women. J. Trauma. Stress 2020, 33, 1071–1081. [Google Scholar] [CrossRef]
- Beckham, J.C.; Vrana, S.R.; Barefoot, J.C.; Feldman, M.E.; Fairbank, J.A.; Moore, S.D. Magnitude and duration of cardiovascular response to anger in combat veterans with and without chronic posttraumatic stress disorder. J. Consult. Clin. Psychol. 2002, 70, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, E.B.; Kolb, L.C.; Pallmeyer, T.P.; Gerardi, R.J. A psychophysiological study of Post-Traumatic Stress Disorder in Vietnam veterans. Psychiatr. Q. 1982, 54, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Castro-Chapman, P.L.; Orr, S.P.; Berg, J.; Pineles, S.L.; Yanson, J.; Salomon, K. Heart rate reactivity to trauma-related imagery as a measure of PTSD symptom severity: Examining a new cohort of Veterans. Psychiatry Res. 2018, 261, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Malcolm, L.R. Cardiovascular Reactivity in Posttraumatic Stress Disorder and Depression. Ph.D. Thesis, Nova Southeastern University, Fort Lauderdale, FL, USA, 2015. [Google Scholar]
- Tucker, P.M.; Pfefferbaum, B.; North, C.S.; Kent, A.; Burgin, C.E.; Parker, D.E.; Hossain, A.; Jeon-Slaughter, H.; Trautman, R.P. Physiologic reactivity despite emotional resilience several years after direct exposure to terrorism. Am. J. Psychiatry 2007, 164, 230–235. [Google Scholar] [CrossRef]
- Arena, J.G.; Schwartz, M.S. Psychophysiological assessment and 91 biofeedback baselines: A primer. In Biofeedback: A Practitioner’s Guide; Schwartz, M.S., Andrasik, F., Eds.; Guilford Press: Guildford, UK, 2003; pp. 128–158. [Google Scholar]
- Augustin, D. PTSD Subtypes, Depressive Presentation, Dissociation, and Cognitive Appraisals and their Impact on Cardiovascular Reactivity Responses to Stress. Ph.D. Thesis, Nova Southeastern University, Fort Lauderdale, FL, USA, 2017. [Google Scholar]
- Orr, S.P.; Metzger, L.J.; Lasko, N.B.; Macklin, M.L.; Hu, F.B.; Shalev, A.Y.; Pittman, R.K.; Harvard/Veterans Affairs Post-traumatic Stress Disorder Twin Study Investigators. Physiologic responses to sudden, loud tones in monozygotic twins discordant for combat exposure: Association with Posttraumatic Stress Disorder. JAMA Psychiatry 2003, 60, 283–288. [Google Scholar] [CrossRef] [Green Version]
- Hyde, J.; Ryan, K.M.; Waters, A.M. Psychophysiological Markers of Fear and Anxiety. Curr. Psychiatry Rep. 2019, 21, 56. [Google Scholar] [CrossRef]
- Rodriguez, C.M. Parent-child aggression: Association with child abuse potential and parenting styles. Violence Vict. 2010, 25, 728–741. [Google Scholar] [CrossRef] [Green Version]
- Waters, A.M.; Craske, M.G. Towards a cognitive-learning formulation of youth anxiety: A narrative review of theory and evidence and implications for treatment. Clin. Psychol. Rev. 2016, 50, 50–66. [Google Scholar] [CrossRef]
- Pelcovitz, D.; Kaplan, S.J.; Ellenberg, A.; Labruna, V.; Salzinger, S.; Mandel, F.; Weiner, M. Adolescent physical abuse: Age at time of abuse and adolescent perception of family functioning. J. Fam. Violence 2000, 15, 375–389. [Google Scholar] [CrossRef]
- Liu, J.J.; Ein, N.; Peck, K.; Huang, V.; Pruessner, J.C.; Vickers, K. Sex differences in salivary cortisol reactivity to the Trier Social Stress Test (TSST): A meta-analysis. Psychoneuroendocrinology 2017, 82, 26–37. [Google Scholar] [CrossRef] [Green Version]
- Stoltenborgh, M.; Ijzendoorn, M.H.V.; Euser, E.M.; Bakermans-Kranenburg, M.J. A global perspective on child sexual abuse: Meta-analysis of prevalence around the world. Child Maltreat. 2011, 16, 79–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackman, D.A.; Farah, M.J.; Meaney, M.J. Socioeconomic status and the brain: Mechanistic insights from human and animal research. Nat. Rev. Neurosci. 2010, 11, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Lê-Scherban, F.; Brenner, A.B.; Hicken, M.T.; Needham, B.L.; Seeman, T.; Sloan, R.P.; Wang, X.; Roux, A.V.D. Child and adult socioeconomic status and the cortisol response to acute stress: Evidence from the multi-ethnic study of atherosclerosis. Psychosom. Med. 2018, 80, 184. [Google Scholar] [CrossRef] [PubMed]
- Cundiff, J.M.; Smith, T.W.; Baron, C.E.; Uchino, B.N. Hierarchy and Health: Physiological Effects of Interpersonal Experiences Associated with Socioeconomic Position. Health Psychol. 2016, 35, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Wiemers, U.S.; Schoofs, D.; Wolf, O.T. A friendly version of the trier social stress test does not activate the HPA axis in healthy men and women. Stress 2013, 16, 254–260. [Google Scholar] [CrossRef]
- Adler, N.; Singh-Manoux, A.; Schwartz, J.; Stewart, J.; Matthews, K.; Marmot, M.G. Social status and health: A comparison of British civil servants in Whitehall-II with European- and African-Americans in CARDIA. Soc. Sci. Med. 2008, 66, 1034–1045. [Google Scholar] [CrossRef]
- Operario, D.; Adler, N.E.; Williams, D.R. Subjective social status: Reliability and predictive utility for global health. Psychol. Health 2004, 19, 237–246. [Google Scholar] [CrossRef]
- Cundiff, J.M.; Smith, T.W.; Uchino, B.N.; Berg, C.A. Subjective social status: Construct validity and associations with psychosocial vulnerability and self-rated health. Int. J. Behav. Med. 2013, 20, 148–158. [Google Scholar] [CrossRef]
- Hoebel, J.; Maske, U.E.; Zeeb, H.; Lampert, T. Social Inequalities and Depressive Symptoms in Adults: The Role of Objective and Subjective Socioeconomic Status. PLoS ONE 2017, 12, e0169764. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.E.; Lerner, J.S.; Sage, R.M.; Lehman, B.J.; Seeman, T.E. Early Environment, Emotions, Responses to Stress, and Health. J. Personal. 2004, 72, 1365–1394. [Google Scholar] [CrossRef]
- Loucks, E.B.; Taylor, S.E.; Polak, J.F.; Wilhelm, A.; Kalra, P.; Matthews, K.A. Childhood family psychosocial environment and carotid intima media thickness: The CARDIA study. Soc. Sci. Med. 2014, 104, 15–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehman, B.J.; Taylor, S.E.; Kiefe, C.I.; Seeman, T.E. Relation of childhood socioeconomic status and family environment to adult metabolic functioning in the CARDIA study. Psychosom. Med. 2005, 67, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.E.; Lehman, B.J.; Kiefe, C.I.; Seeman, T.E. Relationship of Early Life Stress and Psychological Functioning to Adult C-Reactive Protein in the Coronary Artery Risk Development in Young Adults Study. Biol. Psychiatry 2006, 60, 819–824. [Google Scholar] [CrossRef]
- Loucks, E.B.; Almeida, N.D.; Taylor, S.E.; Matthews, K.A. Childhood family psychosocial environment and coronary heart disease risk. Psychosom. Med. 2011, 73, 563–571. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, E.; Lamster, I.B. The Diagnostic Applications of Saliva—A Review. Crit. Rev. Oral Biol. Med. 2002, 13, 197–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirschbaum, C.; Hellhammer, D.H. Salivary Cortisol. In Encyclopedia of Stress, 1st ed.; Fink, G., Ed.; Academic Press: San Diego, CA, USA, 2000; pp. 379–384. [Google Scholar]
- Kirschbaum, C.; Hellhammer, D.H. Salivary Cortisol. In Encyclopedia of Stress, 2nd ed.; Fink, G., Ed.; Academic Press: San Diego, CA, USA, 2007; pp. 405–409. [Google Scholar]
- Poll, E.M.; Kreitschmann-Andermahr, I.; Langejuergen, Y.; Stanzel, S.; Gilsbach, J.M.; Gressner, A.; Yagmur, E. Saliva collection method affects predictability of serum cortisol. Int. J. Clin. Chem. 2007, 382, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Ouellet-Morin, I.; Danese, A.; Bowes, L.; Shakoor, S.; Ambler, A.; Pariante, C.M.; Papadopoulos, A.S.; Caspi, A.; Moffitt, T.E.; Arseneault, L. A discordant monozygotic twin design shows blunted cortisol reactivity among bullied children. J. Am. Acad. Child Adolesc. Psychiatry 2011, 50, 574–582. [Google Scholar] [CrossRef] [Green Version]
- Way, B.; Taylor, S.E. The serotonin transporter promoter polymorphism (5-HTTLPR) is associated with cortisol response to psychosocial stress. Biol. Psychiatry 2011, 67, 487–492. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.; Plessow, F.; Rauh, M.; Gröschl, M.; Kirschbaum, C. Challenge and threat responses during downward and upward social comparisons. Psychoneuroendocrinology 2013, 38, 50–57. [Google Scholar] [CrossRef]
- Llabre, M.M.; Spitzer, S.B.; Saab, P.G.; Ironson, G.H.; Schneiderman, N. The reliability and specificity of delta versus residualized change as measures of cardiovascular reactivity to behavioral challenges. Psychophysiology 1991, 28, 701–711. [Google Scholar] [CrossRef]
- Pruessner, J.C.; Kirschbaum, C.; Meinlschmid, G.; Hellhammer, D.H. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 2003, 28, 916–931. [Google Scholar] [CrossRef]
- Spielberger, C.D. Manual for the State-Trait Anxiety Inventory (STAI); Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Nealey-Moore, J.B.; Smith, T.W.; Uchino, B.N.; Hawkins, M.W.; Olson-Cerny, C. Cardiovascular reactivity during positive and negative marital interactions. J. Behav. Med. 2007, 30, 505–519. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Dickerson, S.S.; Mycek, P.J.; Zaldivar, F. Negative social evaluation, but not mere social presence, elicits cortisol responses to a laboratory stressor task. Health Psychol. 2008, 27, 116–121. [Google Scholar] [CrossRef]
- Lewis, H.B. Shame and Guilt in Neurosis; International Universities Press: New York, NY, USA, 1971. [Google Scholar]
- Hostinar, C.E.; Johnson, A.E.; Gunnar, M.R. Parent support is less effective in buffering stress reactivity for adolescents compared to children. Dev. Sci. 2016, 18, 281–297. [Google Scholar] [CrossRef] [Green Version]
- Verma, R.; Balhara, Y.P.; Gupta, C.S. Gender differences in stress response: Role of developmental and biological determinants. Ind. Psychiatry J. 2011, 20, 4–10. [Google Scholar] [CrossRef]
- Kraft, A.J.; Luecken, L.J. Childhood parental divorce and cortisol in young adulthood: Evidence for mediation by family income. Psychoneuroendocrinology 2009, 34, 1363–1369. [Google Scholar] [CrossRef]
- IBM SPSS Statistics for Windows; Version 25.0; IBM Corp.: Armonk, NY, USA, 2017.
- Chen, E.; Miller, G.E. Socioeconomic Status and Health: Mediating and Moderating Factors. Annu. Rev. Clin. Psychol. 2013, 9, 723–749. [Google Scholar] [CrossRef] [Green Version]
- Halfon, N.; Larson, K.; Son, J.; Lu, M.; Bethell, C. Income inequality and the differential effect of adverse childhood experiences in US children. Acad. Pediatrics 2017, 17, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Hayward, L.E.; Vartanian, L.R.; Kwok, C.; Newby, J.M. How might childhood adversity predict adult psychological distress? Applying the Identity Disruption Model to understanding depression and anxiety disorders. J. Affect. Disord. 2020, 265, 112–119. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Hayward, L.E.; Smyth, J.M.; Paxton, S.J.; Touyz, S.W. Risk and resiliency factors related to body dissatisfaction and disordered eating: The identity disruption model. Int. J. Eat. Disord. 2018, 51, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Poletti, S.; Aggio, V.; Brioschi, S.; Bollettini, I.; Falini, A.; Colombo, C.; Bendetti, F. Impact of early and recent stress on white matter microstructure in major depressive disorder. J. Affect. Disord. 2018, 225, 289–297. [Google Scholar] [CrossRef]
- Morris, A.M.; Barr, M.L.; Famodu, O.A.; Colby, S.E.; Zhou, W.; Hagedorn, R.L.; Clark, R.L.; Riggsbee, K.; Olfert, M.D. Wellness Characteristics of College Freshmen at West Virginia University. FASEB J. 2018, 31, 640. [Google Scholar] [CrossRef]
- Skoluda, N.; Strahler, J.; Schlotz, W.; Niederberger, L.; Marques, S.; Fischer, S.; Thoma, M.V.; Spoerri, C.; Ehlert, U.; Nater, U.M. Intra-individual psychological and physiological responses to acute laboratory stressors of different intensity. Psychoneuroendocrinology 2015, 51, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.S.; Sullivan, M.W.; Lewis, M. Neglected children, shame-proneness, and depressive symptoms. Child Maltreatment 2010, 15, 305–314. [Google Scholar] [CrossRef]
- Slavich, G.M.; Monroe, S.M.; Gotlib, I.H. Early parental loss and depression history: Associations with recent life stress in major depressive disorder. J. Psychiatr. Res. 2011, 45, 1146–1152. [Google Scholar] [CrossRef] [Green Version]
- Visser, L.N.; Tollenaar, M.S.; Bosch, J.A.; Doornen, L.J.V.; Haes, H.C.D.; Smets, E.M. Analogue patients’ self-reported engagement and psychophysiological arousal in a video-vignettes design: Patients versus disease-naïve individuals. Patient Educ. Couns. 2016, 99, 1724–1732. [Google Scholar] [CrossRef] [Green Version]
- Crick, N.R.; Dodge, K.A. Social information-processing mechanisms in reactive and proactive aggression. Child Dev. 1996, 67, 993–1002. [Google Scholar] [CrossRef]
- Dodge, K.A.; Crick, N.R. Social information-processing of aggressive behavior in children. Personal. Soc. Psychol. Bull. 1990, 16, 8–22. [Google Scholar] [CrossRef]
- Lavi, I.; Katz, L.F.; Ozer, E.J.; Gross, J.J. Emotion Reactivity and Regulation in Maltreated Children: A Meta-Analysis. Child Dev. 2019, 90, 1503–1524. [Google Scholar] [CrossRef]
- Pollak, S.D.; Sinha, P. Effects of early experience on children’s recognition of facial displays of emotion. Dev. Psychol. 2002, 38, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, M.A. Retrospectively reported childhood adversity is associated with asthma and chronic bronchitis, independent of mental health. J. Psychosom. Res. 2018, 114, 50–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Age | -- | |||||||
| 2. BMI | 0.202 ** | -- | ||||||
| 3. Family Income | −0.078 | 0.100 | -- | |||||
| 4. ACEs | 0.045 | −0.102 | −0.193 * | -- | ||||
| 5. Cortisol Reactivity | 0.028 | 0.074 | −0.112 | 0.027 | -- | |||
| 6. Anxiety Reactivity | −0.104 | −0.183 * | 0.115 | 0.043 | 0.082 | -- | ||
| 7. SCE Reactivity | −0.021 | −0.212 ** | 0.034 | 0.127 | 0.038 | 0.403 ** | -- | |
| 8. Anger Reactivity | 0.109 | −0.025 | 0.049 | 0.078 | 0.045 | 0.450 ** | 0.199 * | -- |
| M | 21.86 | 23.01 | 6.97 | 21.58 | 1.69 | 1.70 | 1.37 | 2.14 |
| SD | 3.47 | 3.39 | 2.73 | 6.10 | 4.50 | 3.32 | 5.74 | 4.10 |
| Predictor | Cortisol Reactivity | Anxiety Reactivity | SCE Reactivity | Anger Reactivity | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| F | p | η2 | F | p | η2 | F | p | η2 | F | p | η2 | |
| Time Since Waking | 0.07 | 0.798 | 0 | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| BMI | 0.89 | 0.347 | 0.01 | -- | -- | -- | -- | -- | -- | -- | -- | -- |
| Family Income | 4.51 | 0.036 | 0.05 | 0.09 | 0.762 | 0 | 0.01 | 0.942 | 0 | 0.73 | 0.395 | 0.01 |
| Sex | 0.02 | 0.884 | 0 | 4.05 | 0.047 | 0.04 | 0.32 | 0.571 | 0 | 13.17 | <0.001 | 0.12 |
| Status | 5.28 | 0.024 | 0.05 | 1.76 | 0.187 | 0.02 | 2.16 | 0.145 | 0.02 | 0 | 0.997 | 0 |
| Dominance | 0 | 0.946 | 0 | 0.05 | 0.815 | 0 | 2.19 | 0.142 | 0.02 | 7.63 | 0.007 | 0.08 |
| SET | 1.73 | 0.192 | 0.02 | 2.51 | 0.117 | 0.03 | 1.28 | 0.261 | 0.01 | 3.87 | 0.052 | 0.04 |
| ACEs | 1.75 | 0.028 | 0.32 | 1.98 | 0.010 | 0.34 | 1.94 | 0.012 | 0.34 | 1.69 | 0.037 | 0.31 |
| Status∗Sex | -- | -- | -- | -- | -- | -- | -- | -- | -- | 0.15 | 0.695 | 0 |
| Status∗ACEs | 2.27 | 0.010 | 0.25 | 2.01 | 0.025 | 0.23 | 0.84 | 0.621 | 0.11 | 1.54 | 0.111 | 0.19 |
| Dominance∗ACEs | 0.96 | 0.504 | 0.13 | 1.95 | 0.027 | 0.24 | 0.89 | 0.574 | 0.12 | 2.21 | 0.011 | 0.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wendel, C.J.; Cundiff, J.M.; Cribbet, M.R. Early Adversity and Changes in Cortisol and Negative Affect in Response to Interpersonal Threats in the Laboratory. Int. J. Environ. Res. Public Health 2022, 19, 5934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19105934
Wendel CJ, Cundiff JM, Cribbet MR. Early Adversity and Changes in Cortisol and Negative Affect in Response to Interpersonal Threats in the Laboratory. International Journal of Environmental Research and Public Health. 2022; 19(10):5934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19105934
Chicago/Turabian StyleWendel, Christopher J., Jenny M. Cundiff, and Matthew R. Cribbet. 2022. "Early Adversity and Changes in Cortisol and Negative Affect in Response to Interpersonal Threats in the Laboratory" International Journal of Environmental Research and Public Health 19, no. 10: 5934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19105934