
The Living Alone with Cognitive Impairment Project’s Policy Advisory Group on Long-Term Services and Supports: Setting a Research Equity Agenda

Abstract
:1. Introduction
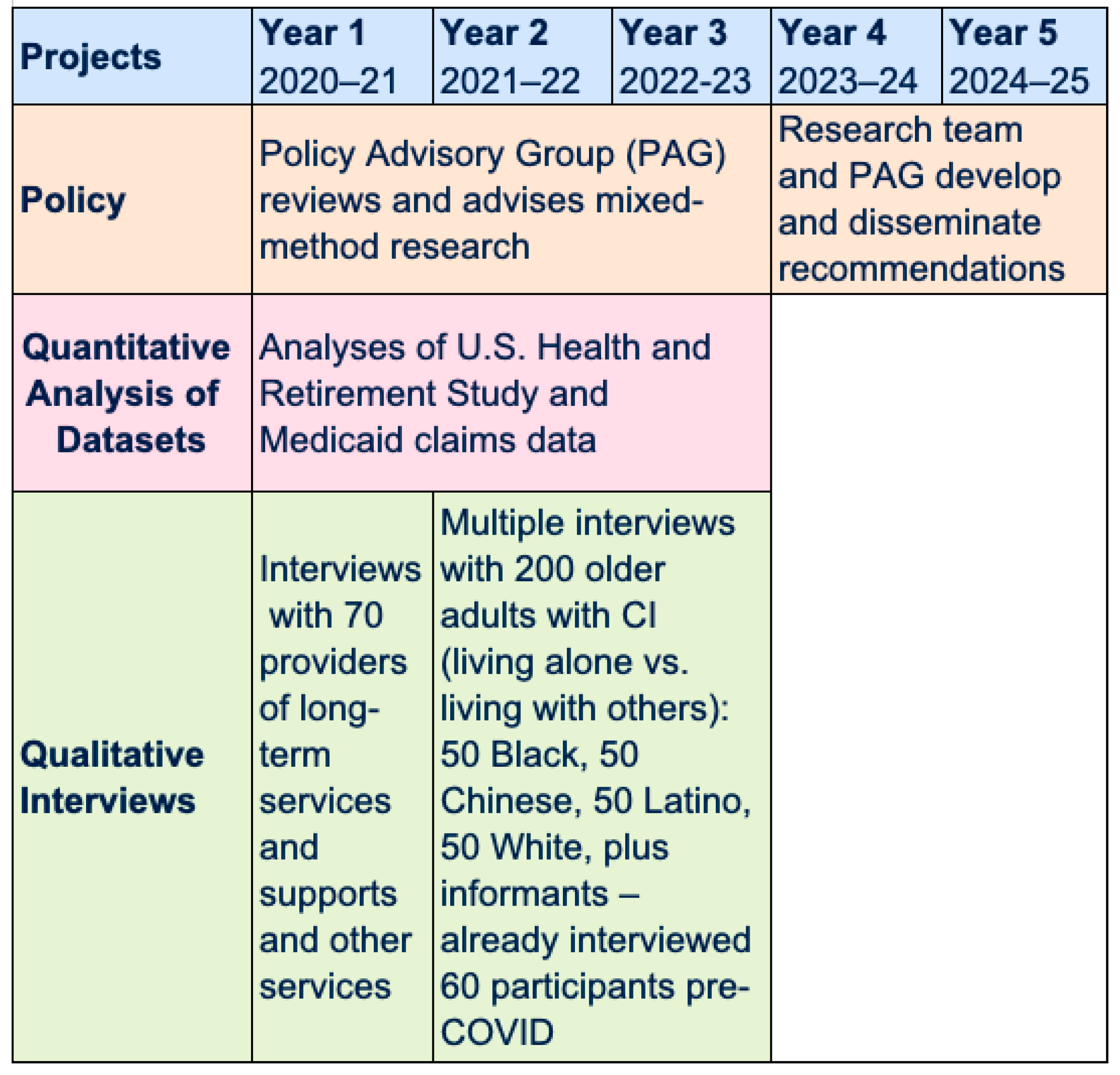
2. Materials and Methods
3. Results
3.1. Better Characterizing PLACI
3.1.1. Limited Understanding of PLACI
3.1.2. Understanding Specific Needs of PLACI
3.2. Leveraging the Diagnosis of CI
3.2.1. Unintended Adverse Consequences of the Diagnosis of CI
3.2.2. Learning How to Empower PLACI at the Point of Diagnosis and Beyond
3.3. Expanding and Enhancing Services
3.3.1. Learning How to Elevate the Status of Home Care Aides
3.3.2. Restrictive Income Eligibility Criteria to Access Medicaid Home- and Community-Based Services (HCBS)
3.3.3. Adapting to Diverse Cultural Values
3.3.4. Learning How to Have a Unique Integrated Point of Reference to Access Services
3.3.5. Learning How to Incorporate Technology into PLACI’s LTSS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Edwards, R.D.; Brenowitz, W.; Portacolone, E.; Covinsky, K.E.; Bindman, A.; Glymour, M.M.; Torres, J.M. Difficulty and help with activities of daily living among older adults living alone with cognitive impairment. Alzheimer Dement. 2020, 16, 1125–1133. [Google Scholar] [CrossRef] [PubMed]
- Tang, M.X.; Cross, P.; Andrews, H.; Jacobs, D.M.; Small, S.; Bell, K.; Merchant, C.; Lantigua, R.; Costa, R.; Stern, Y.; et al. Incidence of AD in African-Americans, Caribbean Hispanics, and Caucasians in northern Manhattan. Neurology 2001, 56, 49–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Potter, G.G.; Plassman, B.L.; Burke, J.R.; Kabeto, M.U.; Langa, K.M. Cognitive performance and informant reports in the diagnosis of cognitive impairment in African Americans and whites. Alzheimers Dement. 2009, 5, 445–453. [Google Scholar] [CrossRef] [Green Version]
- Gurland, B.J.; Wilder, D.E.; Lantigua, R.; Stern, Y.; Chen, J.; Killeffer, E.H.; Mayeux, R. Rates of dementia in three ethnoracial groups. Int. J. Geriatr. Psychiatry 1999, 14, 481–493. [Google Scholar] [CrossRef]
- Chin, A.L.; Negash, S.; Hamilton, R. Diversity and disparity in dementia: The impact of ethnoracial differences in Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2011, 25, 187–195. [Google Scholar] [CrossRef] [Green Version]
- Mayeda, E.R.; Glymour, M.M.; Quesenberry, C.P.; Whitmer, R.A. Inequalities in dementia incidence between six racial and ethnic groups over 14 years. Alzheimers Dement. 2016, 12, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Administration for Community Living. Administration for Community Living; Living AFC: Washington, DC, USA, 2015. [Google Scholar]
- Sanchez-Reilly, S.; Periyakoil, V. (Eds.) Health and Health Care of Hispanic/Latino American Older Adults; eCampus-Geriatrics: Stanford, CA, USA, 2010. [Google Scholar]
- Cantu, P.A.; Angel, J.L. Demography of Living Arrangements Among Oldest-Old Mexican Americans: Evidence From the Hispanic Epidemiologic Study of the Elderly. J. Aging Health 2017, 29, 1015–1038. [Google Scholar] [CrossRef]
- Tierney, M.C. Neuropsychological Predictors of Self-Neglect in Cognitively Impaired Older People Who Live Alone. Am. J. Geriatr. Psychiatry 2007, 15, 140–148. [Google Scholar] [CrossRef]
- Meaney, A.M.; Croke, M.; Kirby, M. Needs assessment in dementia. Int. J. Geriatr. Psychiatry 2005, 20, 322–330. [Google Scholar] [CrossRef]
- Miranda-Castillo, C.; Woods, B.; Orrell, M. People with dementia living alone: What are their needs and what kind of support are they receiving? Int. Psychogeriatr. 2010, 10, 1–11. [Google Scholar] [CrossRef]
- Charles, J.; Naglie, G.; Lee, J.; Moineddin, R.; Jaglal, S.; Tierney, M.C. Self-report measures of well-being predict incident harm due to self-neglect in cognitively impaired seniors who live alone. J. Alzheimers Dis. 2015, 44, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Tuokko, H.; MacCourt, P.; Heath, Y. Home alone with dementia. Aging Ment. Health 1999, 3, 21–27. [Google Scholar] [CrossRef]
- O’Shaughnessy, C.V. National Spending for Long-Term Services and Supports (LTSS): The Basics; National Health Policy Forum: Washington, DC, USA, 2011. [Google Scholar]
- Reaves, E.L.; Musumeci, M. Medicaid and Long-Term Services and Supports: A Primer; Kaiser Family Foundation: Menlo Park, CA, USA, 2015. [Google Scholar]
- Thomas, K.S.; Applebaum, R. Long-term services and supports (LTSS): A growing challenge for an aging America. Public Policy Aging Rep. 2015, 25, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Shih, R.A.; Concannon, T.W.; Liu, J.L.; Friedman, E.M. Improving Dementia Long-Term Care: A Policy Blueprint. Rand. Health Q. 2014, 4, 2. [Google Scholar] [PubMed]
- Reinhard, S.J.; Accius, J.; Houser, A.; Ujvari, K.; Alexis, J.; Fox-Grage, W. Picking Up the Pace of Change: A State Scorecard on Long-Term Services and Supports for Older Adults, People with Physical Disabilities, and Family Caregivers; AARP Public Policy Institute: Washington, DC, USA, 2017. [Google Scholar]
- Tavassoli, N.; Perrin, A.; Berard, E.; Gillette, S.; Vellas, B.; Rolland, Y.; Group, R.F. Factors associated with undertreatment of atrial fibrillation in geriatric outpatients with Alzheimer disease. Am. J. Cardiovasc. Drugs 2013, 13, 425–433. [Google Scholar] [CrossRef]
- Wattmo, C.; Londos, E.; Minthon, L. Solitary living in Alzheimer’s disease over 3 years: Association between cognitive and functional impairment and community-based services. Clin. Interv. Aging 2014, 9, 1951–1962. [Google Scholar] [CrossRef] [Green Version]
- Ficker, L.J.; MacNeill, S.E.; Bank, A.L.; Lichtenberg, P.A. Cognition and perceived social support among live-alone urban elders. J. Appl. Gerontol. 2002, 21, 437–451. [Google Scholar] [CrossRef]
- Durand, M.; James, A.; Ravishankar, A.; Bamrah, J.S.; Purandare, N.B. Domiciliary and day care services: Why do people with dementia refuse? Aging Ment. Health 2009, 13, 414–419. [Google Scholar] [CrossRef]
- Portacolone, E.; Johnson, J.K.; Covinsky, K.E.; Halpern, J.; Rubinstein, R.L. The effects and meanings of receiving a diagnosis of mld cognitive Impairment or Alzheimer’s disease when one lives alone. J. Alzheimers Dis. 2018, 61, 1517–1529. [Google Scholar] [CrossRef] [Green Version]
- Portacolone, E.; Covinsky, K.E.; Rubinstein, R.L.; Halpern, J.; Johnson, J.K. The precarity of older adults living alone with cognitive impairment. Gerontologist 2019, 59, 271–280. [Google Scholar] [CrossRef]
- Portacolone, E.; Covinsky, K.E.; Johnson, J.K.; Rubinstein, R.L.; Halpern, J. Walking the Tightrope Between Study Participant Autonomy and Researcher Integrity: The Case Study of a Research Participant with Alzheimer’s Disease Pursuing Euthanasia in Switzerland. J. Empir. Res. Hum. Res. Ethics 2019, 14, 483–486. [Google Scholar] [CrossRef] [PubMed]
- Portacolone, E. On Living Alone with Alzheimer’s Disease. Care Wkly. 2018, 2018, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Portacolone, E.; Chodos, A.; Halpern, J.; Covinsky, K.E.; Keiser, S.; Fung, J.; Rivera, E.; Bykhovsky, C.; Johnson, J.K. The effects of the COVID-19 pandemic in the lived experience of diverse older adults with cognitive impairment living alone. Gerontologist 2021, 61, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Portacolone, E.; Byers, A.; Halpern, J.; Barnes, D. Addressing suicide risk in patients with dementia during COVID-19 pandemic and beyond. Gerontologist 2022, 2, gnac042. [Google Scholar] [CrossRef] [PubMed]
- Knapp, M.; Chua, K.C.; Broadbent, M.; Chang, C.K.; Fernandez, J.L.; Milea, D.; Romeo, R.; Lovestone, S.; Spencer, M.; Thompson, G.; et al. Predictors of care home and hospital admissions and their costs for older people with Alzheimer’s disease: Findings from a large London case register. BMJ Open 2016, 6, e013591. [Google Scholar] [CrossRef] [Green Version]
- Prescop, K.L.; Dodge, H.H.; Morycz, R.K.; Schulz, R.M.; Ganguli, M. Elders with dementia living in the community with and without caregivers: An epidemiological study. Int. Psychogeriatr. 1999, 11, 235–250. [Google Scholar] [CrossRef]
- Tierney, M.C.; Charles, J.; Naglie, G.; Jaglal, S.; Kiss, A.; Fisher, R. Risk Factors for Harm in Cognitively Impaired Seniors Who Live Alone: A Prospective Study. J. Am. Geriatr. Soc. 2004, 52, 1435–1441. [Google Scholar] [CrossRef]
- Pongan, E.; Dorey, J.M.; Krolak-Salmon, P.; Federico, D.; Sellier, C.; Auguste, N.; Fabre, F.; Laurent, B.; Trombert-Paviot, B.; Rouch, I. Predictors of Discharge Destinations and Three-Month Evolution of Patients Initially Hospitalized in a Cognitive Behavioral Unit. J. Alzheimers Dis. 2017, 60, 1259–1266. [Google Scholar] [CrossRef]
- Rosenwohl-Mack, A.; Dubbin, L.; Chodos, A.; Dulaney, S.; Fang, M.-L.; Merrilees, J.; Portacolone, E. Use of services by people living alone with cognitive impairment: A systematic review. Innov. Aging 2021, 5, igab004. [Google Scholar] [CrossRef]
- Widera, E.; Steenpass, V.; Marson, D.; Sudore, R. Finances in the older patient with cognitive impairment: “He didn’t want me to take over”. JAMA J. Am. Med. Assoc. 2011, 305, 698–706. [Google Scholar] [CrossRef] [Green Version]
- El-Saifi, N.; Moyle, W.; Jones, C.; Tuffaha, H. Medication Adherence in Older Patients With Dementia: A Systematic Literature Review. J. Pharm. Pract. 2018, 31, 322–334. [Google Scholar] [CrossRef] [PubMed]
- Aranda, M.P.; Kremer, I.N.; Hinton, L.; Zissimopoulos, J.; Whitmer, R.A.; Hummel, C.H.; Trejo, L.; Fabius, C. Impact of dementia: Health disparities, population trends, care interventions, and economic costs. J. Am. Geriatr. Soc. 2021, 69, 1774–1783. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.; Morris, J.C. Alone and confused: Community-residing older African Americans with dementia. Dementia 2007, 6, 489–506. [Google Scholar] [CrossRef]
- Collyer, T.A.; Smith, K.E. An atlas of health inequalities and health disparities research: “How is this all getting done in silos, and why?”. Soc. Sci. Med. 2020, 264, 113330. [Google Scholar] [CrossRef] [PubMed]
- Forman, J.; Damschroder, J. Qualitative Content Analysis. In Empirical Methods for Bioethics: A Primer; Jacoby, L., Siminoff, L., Eds.; Jai Press Elsevier: Amsterdam, The Netherlands, 2008; pp. 39–62. [Google Scholar]
- Elo, S.; Kyngas, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.; Barlow, S.; Hoe, J.; Aitken, L. Persistent barriers and facilitators to seeking help for a dementia diagnosis: A systematic review of 30 years of the perspectives of carers and people with dementia. Int. Psychogeriatr. 2020, 6, 1–24. [Google Scholar] [CrossRef]
- Mercer, M. Can you Afford a Home-Care Worker? AARP. Available online: https://www.aarp.org/caregiving/financial-legal/info-2017/afford-a-homecare-worker.html (accessed on 3 September 2021).
- Rapp, T.; Sicsic, J. The contribution of the immigrant population to the U.S. long-term care workforce. Soc. Sci. Med. 2020, 263, 113305. [Google Scholar] [CrossRef]
- Musumeci, M.; O’Malley Watts, M.; Chidambaram, P. Key State Policy Choices About Medicaid Home and Community-Based Services. KFF. Available online: https://www.kff.org/medicaid/issue-brief/key-state-policy-choices-about-medicaid-home-and-community-based-services/ (accessed on 3 September 2021).
- Rote, S.; Angel, J.; Hinton, L. Characteristics and Consequences of Family Support in Latino Dementia Care. J. Cross Cult. Gerontol. 2019, 34, 337–354. [Google Scholar] [CrossRef]
- Chang, Y.P.; Schneider, J.K.; Sessanna, L. Decisional conflict among Chinese family caregivers regarding nursing home placement of older adults with dementia. J. Aging Stud. 2011, 25, 436–444. [Google Scholar] [CrossRef]
- OECD. Health Policy Studies; OECD: Paris, France, 2020. [Google Scholar]
- Reuben, D.B.; Tan, Z.S.; Romero, T.; Wenger, N.S.; Keeler, E.; Jennings, L.A. Patient and Caregiver Benefit From a Comprehensive Dementia Care Program: 1-Year Results From the UCLA Alzheimer’s and Dementia Care Program. J. Am. Geriatr. Soc. 2019, 67, 2267–2273. [Google Scholar] [CrossRef] [Green Version]
- Gleckman, H. What You Need To Know About Washington State’s Public Long-Term Care Insurance Program. Forbes 2019 [Magazine issued of May 15 2019]. Available online: https://www.forbes.com/sites/howardgleckman/2019/05/15/what-you-need-to-know-about-washington-states-public-long-term-care-insurance-program/?sh=840589a2cdca (accessed on 14 April 2022).
- Bingham, J.M.; Black, M.; Anderson, E.J.; Li, Y.; Toselli, N.; Fox, S.; Martin, J.R.; Axon, D.R.; Silva-Almodovar, A. Impact of Telehealth Interventions on Medication Adherence for Patients With Type 2 Diabetes, Hypertension, and/or Dyslipidemia: A Systematic Review. Ann. Pharmacother. 2021, 55, 637–649. [Google Scholar] [CrossRef] [PubMed]
- Neeman, E.; Kumar, D.; Lyon, L.; Kolevska, T.; Reed, M.; Sundaresan, T.; Arora, A.; Li, Y.; Seaward, S.; Kuehner, G.; et al. Attitudes and Perceptions of Multidisciplinary Cancer Care Clinicians Toward Telehealth and Secure Messages. JAMA Netw. Open 2021, 4, e2133877. [Google Scholar] [CrossRef] [PubMed]
- Portacolone, E.; Halpern, J.; Luxenberg, J.; Harrison, K.; Covinsky, K.E. Ethical issues raised by the introduction of artificial companions to older adults with cognitive impairment: A call for interdisciplinary collaborations. J. Alzheimers Disease. 2020, 76, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Portacolone, E.; Johnson, J.K.; Halpern, J.; Kotwal, A. Seeking a Sense of Belonging: Becoming an integral part of a community is a better solution for social isolation than many volunteer programs. Gener. J. Am. Soc. Aging 2020, 44, 1–8. [Google Scholar]
- Portacolone, E.; Covinsky, K.E.; Johnson, J.K.; Halpern, J. Expectations and concerns of older adults with cognitive impairment about their relationship with medical providers: A call for therapeutic alliances. Qual. Health Res. 2020, 30, 1584–1595. [Google Scholar] [CrossRef]
- Steenfeldt, V.O.; Aagerup, L.C.; Jacobsen, A.H.; Skjodt, U. Becoming a Family Caregiver to a Person With Dementia: A Literature Review on the Needs of Family Caregivers. SAGE Open Nurs. 2021, 7, 23779608211029073. [Google Scholar] [CrossRef]
- Bott, N.T.; Sheckter, C.C.; Milstein, A.S. Dementia Care, Women’s Health, and Gender Equity: The Value of Well-Timed Caregiver Support. JAMA Neurol. 2017, 74, 757–758. [Google Scholar] [CrossRef]


{kind=link}
| LTSS | Examples of Support |
|---|---|
| Home-care aides | House cleaning, buying/cooking food, reminders, errands, dressing, bathing, transportation, cognitive stimulation |
| Support coordinators (e.g., social workers, nurses, case managers) | Service coordination, needs assessments, managing safety, as well as legal, financial and housing matters |
| Adult day healthcare centers | Medical services, service coordination, safety, finances, cognitive stimulation |
| Meal services | Nutrition |
| In-home medical services (e.g., medical providers) | Managing medications, health assessment and monitoring |
| Transportation services | Transportation to services (e.g., medical, social, personal) |
| Factors and Sub-Sections | Barriers (B) and Facilitators (F) | Research Directions | Policy Directions |
|---|---|---|---|
| 1. Better characterizing PLACI | |||
| Limited understanding of PLACI |
|
| |
| |||
| Understanding specific needs of PLACI |
|
|
|
| 2. Leveraging the diagnosis of CI | |||
| Unintended adverse consequences of the diagnosis of CI |
|
| |
| Learning how to empower PLACI at the point of diagnosis and beyond |
|
|
|
| 3. Expanding and enhancing services | |||
| Learning how to elevate the status of home care aides |
|
|
|
| Restrictive income eligibility criteria to access Medicaid home and community-based services |
|
| |
| Adapting to diverse cultural values |
|
| |
| Learning how to have a unique integrated point of reference to access services |
|
| |
| Learning how to incorporate technology in PLACI’s LTSS |
|
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Portacolone, E.; Torres, J.M.; Johnson, J.K.; Benton, D.; Rapp, T.; Tran, T.; Martinez, P.; Graham, C. The Living Alone with Cognitive Impairment Project’s Policy Advisory Group on Long-Term Services and Supports: Setting a Research Equity Agenda. Int. J. Environ. Res. Public Health 2022, 19, 6021. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106021
Portacolone E, Torres JM, Johnson JK, Benton D, Rapp T, Tran T, Martinez P, Graham C. The Living Alone with Cognitive Impairment Project’s Policy Advisory Group on Long-Term Services and Supports: Setting a Research Equity Agenda. International Journal of Environmental Research and Public Health. 2022; 19(10):6021. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106021
Chicago/Turabian StylePortacolone, Elena, Jacqueline M. Torres, Julene K. Johnson, Donna Benton, Thomas Rapp, Thi Tran, Paula Martinez, and Carrie Graham. 2022. "The Living Alone with Cognitive Impairment Project’s Policy Advisory Group on Long-Term Services and Supports: Setting a Research Equity Agenda" International Journal of Environmental Research and Public Health 19, no. 10: 6021. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106021