
Convalescents’ Reports on COVID-19 Experience—A Qualitative Study

 , ,
, , {kind=link}
Abstract
:1. Introduction
2. Material and Method
2.1. Study Procedure
2.2. Participants
3. Results
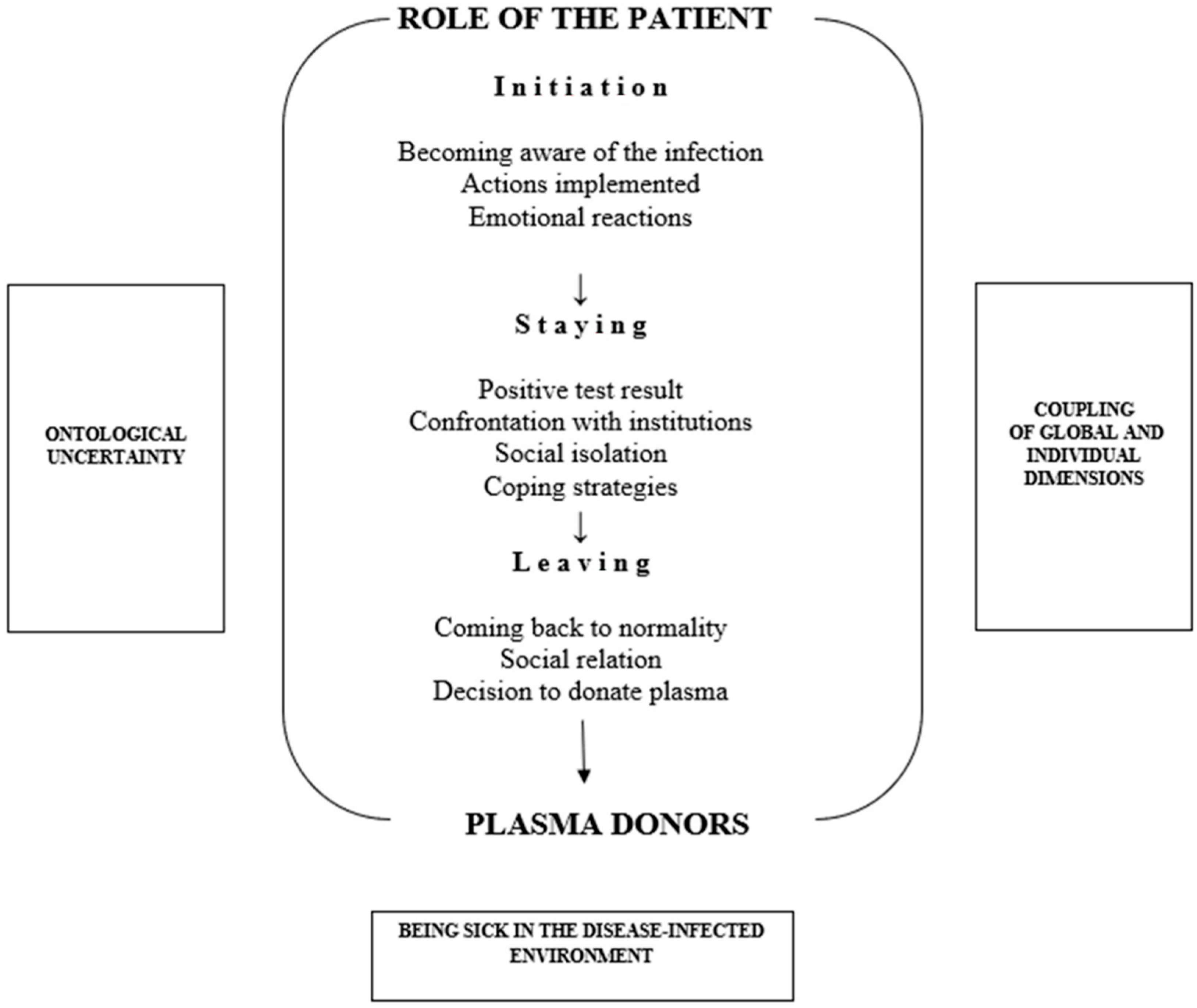
3.1. Stage 1: Initiation to the Role of a Patient
3.1.1. Becoming Aware of the Infection
3.1.2. Actions Implemented
In the first week there was fever (…) muscle pain. (…) we were told that the fever was too low, we do not have typical symptoms, so it was definitely not that (…) later, I lost my sense of smell and taste completely (…) I called the SSI [State Sanitary Inspection-ed], where a lady told me that it could be sinusitis. So we still haven’t been tested. (…) And after 2 weeks my mother started to have fever, cough. And only then Inspection decided to test us and it turned out that the results were positive.[C 9, F]
3.1.3. Emotional Reactions
(…) I was stressed (…) I have a disabled mother. I was less worried about myself, than about my mother (…) more about my parents because they are elderly (…).[C 2, F]
(…) I must admit, I was a bit scared. However, once I lost my taste and smell, it had come to me a bit, I calmed down.[C 6, M]
3.2. Stage 2: Staying in the COVID-19 Patient Role
3.2.1. Positive Test Result
They took my swab, and on Thursday morning they called me saying I’m positive (…) and then the snowball effect continued.[C 1, M]
(…) the information that I am positive (…) did not surprise me in any way.[C 3, M]
I was rather calm (…) I was sure that the result would be negative and that I would eventually go home.[C 7, M]
Somehow it happened that we were not aware that we have COVID. We went through it like through a common cold; the seasonal flu, and that was it. There were no pigs flying, or anything like that.[C 7, M]
3.2.2. Confrontation with Institutions
(…) my phone calls to the PIS (…) no matter what I was asking about, I never met with refusal, snapping back, or lack of assistance, there was always someone trying to help me somehow.[C 7, M]
We were scared; the lady from SSI was shouting at me, asking how is it possible that my son got infected and other children from his class did not.[C 9, F]
(…) the whole situation was new for everyone, as well as for them [SSI-ed] and for all services, so it was an amazing mess. (…) they were overwhelmed with calls, they were unable to cope with them, they sometimes didn’t simply know how to help and what to do next.[C 1, M]
(…) then you have to understand that during that time (…) there were a lot of infected people and a lot of people in quarantine, so… (…) because it looked a bit different then, from a different perspective. Now, when I left there and I am a healthy person, I begin to think differently, begin to understand what was happening there, what we expected, and that it maybe was a bit too much.[C 5, M]
(…) the doctor (…) always called in the morning, asked about the temperature, blood pressure, heart rate, and then informed me what medications I would be administered today and how the treatment would be proceeding.[C 3, M]
3.2.3. Social Isolation
(…) I organized the day for myself so that I would get up at eight or seven (…) after breakfast, I read a book, then did some physical exercise (…) then read a book again, had lunch, and after lunch, maybe watched a movie (…) I also tried to stick to my own schedule, so to speak. (…) And it was easier if you planned your whole day there and stuck to that plan.[C 5, M]
3.2.4. Coping Strategies
(…) apart from the nervousness connected with the need to spend another two weeks in quarantine (…) it’s basically nothing. (…) We were all already healthy (…) when we had positive results, we were at the end of the disease.[C 7, M]
I had darkness before my eyes, back then no one knew much about this disease. I didn’t know what would happen to me; nobody knew, (…) how it would happen, what would happen with me, how many people I infected (…) So many unpleasant emotions.[C 2, F]
I had a lot of such conversations, and friends from work were calling every now and then, and I had to repeat the same to everyone. (…) it is not that a person is malicious or something, but it was the same thing over and over again. “Well, I’m fine, all right. I don’t know what the test results are. No. I don’t know when I will be able to leave.” And so on.[C 8, M]
I tried not to read any messages or look at any information about it because it made me even more stressed.[C 2, F]
3.3. Stage 3: Leaving the Role of Patient
3.3.1. Coming Back to Normality
I was released home from the isolation and recognized as a person who was already healthy, and I also felt as if nothing had happened. I didn’t experience any symptoms myself, everything was fine.[C 4, M]
Theoretically, it was all over for me. Then, even after the negative results, I felt, deep in my chest, that it was much harder to breathe, but that was gone too. On the other hand… my allergy exacerbated.[C 10, F]
In the beginning, I wasn’t seeing anyone, not a person. I didn’t even see my own boyfriend for a month… I didn’t leave the house. Only after a month did I go out for some short shopping. But then I was so stressed out, because people were still afraid then.[C 2, F]
3.3.2. Social Relations
Here people are afraid, they are still really afraid.[C 9, F]
(…) our relations are good, very good. I think they’re even better now between those who got infected. We supported each other, we called each other, we talked about the symptoms.[C 1, M]
(…) at work from a distance, this is how we talked to each other—from a distance, because they knew that I was sick. Well, that’s how they try to avoid me.[C 8, M]
3.3.3. Decision to Donate Plasma
What made me do this? Just a willing to help. Well, if someone who is not so lucky and this disease affects him in a different way than me, i.e., has some more serious symptoms, something happens that his health, and perhaps even life, is at risk, and my time devoted to donating plasma can help with this and save someone, so it doesn’t cost me a lot of effort or an enormous amount of time, so why shouldn’t I agree?[C 4, M]
4. Discussion
5. Conclusions
- The disease, despite its mild course, generated a number of non-medical issues, and the entire process of being ill was burdened with emotional and institutional struggles.
- The role of a COVID-19 patient during the first stage of the pandemic has been defined by: ontological uncertainty, the coupling of the global and individual dimensions, and being sick in the disease-infected environment. The experience of mild COVID-19 is significantly modified by disease institutionalization. The decisions of sanitary authorities and the results of genetic tests have a strong influence on the subjective feelings of the beginning and end of the disease.
- Results may contribute to a better understanding of the psychosocial dimension of COVID-19, in particular, the specificity of functioning in it and recovery from it, and to the development of a strategy to support patients during subsequent waves of the COVID-19 pandemic and convalescents’ motivations for plasma donation.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| [C] | Convalescent |
| [GT] | Grounded Theory |
| [SSI] | State Sanitary Inspection |
| [PIS] | Polska Inspekcja Sanitarna |
| [RCKiK] | Regional Centre for Blood Donation and Blood Treatment |
References
- Moradi, Y.; Mollazadeh, F.; Karimi, P.; Hosseingholipour, K.; Baghaei, R. Psychological disturbances of survivors throughout COVID-19 crisis: A qualitative study. BMC Psychiatry 2020, 20, 594. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, X.; Hu, X.; Ekumi, I.O.; Wang, J.; An, Y.; Li, Z.; Yuan, B. Psychological Distress and Its Correlates Among COVID-19 Survivors During Early Convalescence across Age Groups. Am. J. Geriatr. Psychiatry 2020, 28, 1030–1039. [Google Scholar] [CrossRef]
- Prokop, J.; Reid, C.; Palmateer, B. Experiences with COVID-19. Nurs. Res. 2022, 5–6, E21–E27. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.; Lee, S.Y.; Kim, M.S.; Jung, H.; Kim, K.H.; Kim, K.-N.; Park, H.Y.; Lee, Y.J.; Cho, B.; Sohn, J.H. The Psychological Burden of COVID-19 Stigma: Evaluation of the Mental Health of Isolated Mild Condition COVID-19 Patients. J. Korean Med. Sci. 2021, 36, e33. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Liu, J. Living with COVID-19: A phenomenological study of hospitalised patients involved in family cluster transmission. BMJ Open 2021, 11, e046128. [Google Scholar] [CrossRef]
- Roberts, M.E.; Knestrick, J.; Resick, L. The Lived Experience of COVID-19. J. Nurse Pract. 2021, 17, 828–832. [Google Scholar] [CrossRef]
- Roth, J.; Conrad, P. The experience and management of chronic illness. In Research in the Sociology of Health Care: The Experience and Management of Chronic Illness; Roth, J.A., Conrad, P., Eds.; JAI Press: Greenwich, CT, USA, 1987; Volume 6, pp. 1–33. [Google Scholar]
- Freidson, E. Patients’ Views of Medical Practice: A Study of Subscribers to a Prepaid Medical Plan in the Bronx; Russell Sage Foundation: New York, NY, USA, 1961. [Google Scholar]
- Strauss, A.; Glaser, B.G. Chronic Illness and the Quality of Life; CV Mosby: St Louis, MI, USA, 1975. [Google Scholar]
- Parsons, T. The Social System; Routledge and Kegan Paul: London, UK, 1951. [Google Scholar]
- Twaddle, A.C. Sickness and the sickness career: Some implications. In The Relevance of Social Science for Medicine; Culture Illness and Healing; Eisenberg, L., Kleinman, A., Eds.; D. Reidel Publishing Company: Dordrecht, The Netherlands, 1981; pp. 111–133. [Google Scholar]
- Foley, G.; Timonen, V. Using Grounded Theory Method to Capture and Analyze Health Care Experiences. Health Serv. Res. 2015, 50, 1195–1210. [Google Scholar] [CrossRef] [Green Version]
- Glaser, B.G.; Strauss, A.L. The Discovery of Grounded Theory; Strategies for Qualitative Research; Aldine: Chicago, IL, USA, 1967. [Google Scholar]
- Charmaz, K. Constructing Grounded Theory, A Practical Guide Through Qualitative Analysis; Sage: London, UK, 2006. [Google Scholar]
- Chen, L.; Xiong, J.; Bao, L.; Shi, Y. Convalescent plasma as a potential therapy for COVID-19. Lancet Infect. Dis. 2020, 20, 398–400. [Google Scholar] [CrossRef]
- Piechotta, V.; Chai, K.L.; Valk, S.J.; Doree, C.; Monsef, I.; Wood, E.M.; Lamikanra, A.; Kimber, C.; McQuilten, Z.; So-Osman, C.; et al. Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: A living systematic review. Cochrane Database Syst. Rev. 2021, 5, CD013600. [Google Scholar] [CrossRef]
- Zeng, Q.L.; Yu, Z.J.; Gou, J.J.; Li, G.-M.; Ma, S.-H.; Zhang, G.-F.; Xu, J.-H.; Lin, W.-B.; Cui, G.-L.; Zhang, M.-M.; et al. Effect of Convalescent Plasma Therapy on Viral Shedding and Survival in Patients with Coronavirus Disease 2019. J. Infect. Dis. 2020, 222, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.D.; Shukla, S.; Chung, Y.H.; Beiss, V.; Chan, S.K.; Ortega-Rivera, O.A.; Wirth, D.M.; Chen, A.; Sack, M.; Pokorski, J.K.; et al. COVID-19 vaccine development and a potential nanomaterial path forward. Nat. Nanotechnol. 2020, 15, 646–655. [Google Scholar] [CrossRef] [PubMed]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Bavishi, C.; Bonow, R.O.; Trivedi, V.; Abbott, J.D.; Messerli, F.H.; Bhatt, D.L. Acute myocardial injury in patients hospitalized with COVID-19 infection: A review. Prog. Cardiovasc. Dis. 2020, 63, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Hayek, S.; Wang, W.; Chan, L.; Mathews, K.S.; Melamed, M.L.; Brenner, S.K.; Leonberg-Yoo, A.; Schenck, E.J.; Radbel, J.; et al. Factors Associated with Death in Critically Ill Patients With Coronavirus Disease 2019 in the US. JAMA Intern. Med. 2020, 180, 1436–1447. [Google Scholar] [CrossRef]
- Varatharaj, A.; Thomas, N.; Ellul, M.A.; Davies, N.W.S.; Pollak, T.A.; Tenorio, E.L.; Sultan, M.; Easton, A.; Breen, G.; Zandi, M.; et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: A UK-wide surveillance study. Lancet Psychiatry 2020, 7, 875–882. [Google Scholar] [CrossRef]
- Paules, C.I.; Marston, H.D.; Fauci, A.S. Coronavirus Infections—More Than Just the Common Cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Ministerstwo Zdrowia, Koronawirus w Europie. Przypadki hospitalizacji w Przeliczeniu na 100 tys. Mieszkańców. Available online: https://twitter.com/MZ_GOV_PL (accessed on 26 July 2020).
- CDA Centres for Disease Control and Prevention, COVID View. Available online: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/index.html (accessed on 26 July 2020).
- Peng, M. Outbreak of COVID-19: An emerging global pandemic threat. Biomed. Pharmacother. 2020, 129, 110499. [Google Scholar] [CrossRef]
- Giddens, A. Nowoczesność i Tożsamość. “Ja” i Społeczeństwo w Epoce Późnej Nowoczesności, (Modernity and Identity. “I” and Society in the Late Modern Era); Wydawnictwo Naukowe PWN: Warszawa, Polska, 2010. [Google Scholar]
- Tang, X.; Wu, C.; Li, X.; Song, Y.; Yao, X.; Wu, X.; Duan, Y.; Zhang, H.; Wang, Y.; Qian, Z.; et al. On the origin and continuing evolution of SARS-CoV-2. Natl. Sci. Rev. 2020, 7, 1012–1023. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA Intern. Med. 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamun, M.A.; Griffiths, M.D. First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: Possible suicide prevention strategies. Asian J. Psychiatry 2020, 51, 102073. [Google Scholar] [CrossRef]
- Isaacs, D.; Britton, P.N.; Preisz, A. Ethical reflections on the COVID-19 pandemic: The epidemiology of panic. J. Paediatr. Child Health 2020, 56, 690–691. [Google Scholar] [CrossRef] [PubMed]
- Kirkcaldy, R.D.; King, B.A.; Brooks, J.T. COVID-19 and Postinfection Immunity: Limited Evidence, Many Remaining Questions. JAMA 2020, 323, 2245–2246. [Google Scholar] [CrossRef] [PubMed]
- Roy, S. COVID-19 reinfection: Myth or truth? SN Compr. Clin. Med. 2020, 2, 710–713. [Google Scholar] [CrossRef]
- Chandrashekar, A.; Liu, J.; Martinot, A.J.; Mcmahan, K.; Mercado, N.B.; Peter, L.; Tostanoski, L.H.; Yu, J.; Maliga, Z.; Nekorchuk, M.; et al. SARS-CoV-2 infection protects against rechallenge in rhesus macaques. Science 2020, 369, 812–817. [Google Scholar] [CrossRef] [PubMed]
- Adom, D.; Mensah, J.A. The Psychological Distress and Mental Health Disorders from COVID-19 Stigmatization in Ghana. Soc. Sci. Humanit. Open 2020, 4, 100186. [Google Scholar] [CrossRef]
- Sahooa, S.; Mehraa, A.; Surib, V.; Malhotrab, P.; Narayana, L.; Goverdhan, Y.; Puric, D.; Grovera, S. Lived experiences of the corona survivors (patients admitted in COVID wards): A narrative real-life documented summaries of internalized guilt, shame, stigma, anger. Asian J. Psychiatr. 2020, 53, 102187. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 27, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, A.R.; Murad, H.R. The Impact of Social Media on Panic during the COVID-19 Pandemic in Iraqi Kurdistan: Online Questionnaire Study. J. Med. Internet Res. 2020, 22, e19556. [Google Scholar] [CrossRef]
- Garfin, D.R.; Silver, R.C.; Holman, E.A. The Novel Coronavirus (COVID-2019) Outbreak: Amplification of Public Health Consequences by Media Exposure. Health Psychol. 2020, 39, 355–357. [Google Scholar] [CrossRef] [PubMed]
- WHO. Speech of Vice President Věra Jourová on Countering Disinformation amid COVID-19 “From Pandemic to Infodemic” SPEECH/20/1000, Brussels. 2020. Available online: https://ec.europa.eu/commission/presscorner/detail/en/speech_20_1000. (accessed on 22 September 2020).
- Truog, R.D.; Mitchell, C.; Daley, G.Q. The toughest triage—Allocating ventilators in a pandemic. N. Engl. J. Med. 2020, 382, 1973–1975. [Google Scholar] [CrossRef]
- Pawlikowski, J. The ethical dimension of prioritization and allocation decisions within the context of the COVID-19 pandemic. Pol. Arch. Intern. Med. 2020, 130, 466–472. [Google Scholar] [CrossRef] [PubMed]
- Shamasunder, S.; Holmes, S.M.; Goronga, T.; Carrasco, H.; Katz., E.; Frankfurter., R.; Salmaan Keshavjee, S. COVID-19 reveals weak health systems by design: Why we must re-make global health in this historic moment. Glob. Public Health 2020, 15, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Greer, S.L.; King, E.J.; Massard da Fonseca, E.; Santos, A.P. The comparative politics of COVID-19: The need to understand government responses. Glob. Public Health 2020, 15, 1413–1416. [Google Scholar] [CrossRef]
- Razai, M.S.; Oakeshott, P.; Kankam, H.; Galea, S.; Stokes-Lampard, H. Mitigating the psychological effects of social isolation during the COVID-19 pandemic. BMJ 2020, 369, m1904. [Google Scholar] [CrossRef]
- Haider, I.I.; Tiwana, F.; Tahir, S.M. Impact of the COVID-19 Pandemic on Adult Mental Health. Pak. J. Med. Sci. 2020, 36, S90–S94. [Google Scholar] [CrossRef]
- Brookes, S.; Webster, R.; Smith, L.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Masser, B.M.; Ferguson, E.; Thorpe, R.; Lawrence, C.; Davison, T.E.; Hoad, V.; Gosbell, I.B. Motivators of and barriers to becoming a COVID-19 convalescent plasma donor: A survey study. Transfus. Med. 2021, 31, 176–185. [Google Scholar] [CrossRef]
- Sullivan, D.I.; Gebo, K.A.; Shoham, S.; Bloch, E.M.; Lau, B.; Shenoy, A.G.; Mosnaim, G.S.; Gniadek, T.J.; Fukuta, Y.; Patel, B.; et al. Early Outpatient Treatment for COVID-19 with Convalescent Plasma. N. Engl. J. Med. 2022, 386, 1700–1711. [Google Scholar] [CrossRef]
- Piechotta, V.; Chai, K.L.; Valk, S.J.; Doree, C.; Monsef, I.; Wood, E.M.; Lamikanra, A.; Kimber, C.; McQuilten, Z.; So-Osman, C.; et al. Convalescent plasma or hyperimmune immunoglobulin for people with COVID-19: A rapid review. Cochrane Database Syst. Rev. 2020, 5, CD013600. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bogusz, R.; Nowakowska, L.; Majchrowska, A.; Patryn, R.; Pawlikowski, J.; Zagaja, A.; Kiciński, P.; Pacyna, M.; Puacz, E. Convalescents’ Reports on COVID-19 Experience—A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 6147. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106147
Bogusz R, Nowakowska L, Majchrowska A, Patryn R, Pawlikowski J, Zagaja A, Kiciński P, Pacyna M, Puacz E. Convalescents’ Reports on COVID-19 Experience—A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(10):6147. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106147
Chicago/Turabian StyleBogusz, Renata, Luiza Nowakowska, Anita Majchrowska, Rafał Patryn, Jakub Pawlikowski, Anna Zagaja, Paweł Kiciński, Magdalena Pacyna, and Elżbieta Puacz. 2022. "Convalescents’ Reports on COVID-19 Experience—A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 10: 6147. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106147