
Elderly Caregiving Quality Improvement: A Pilot Study of the Burdens of Vietnamese Caregivers in Taiwan



Abstract
:1. Introduction
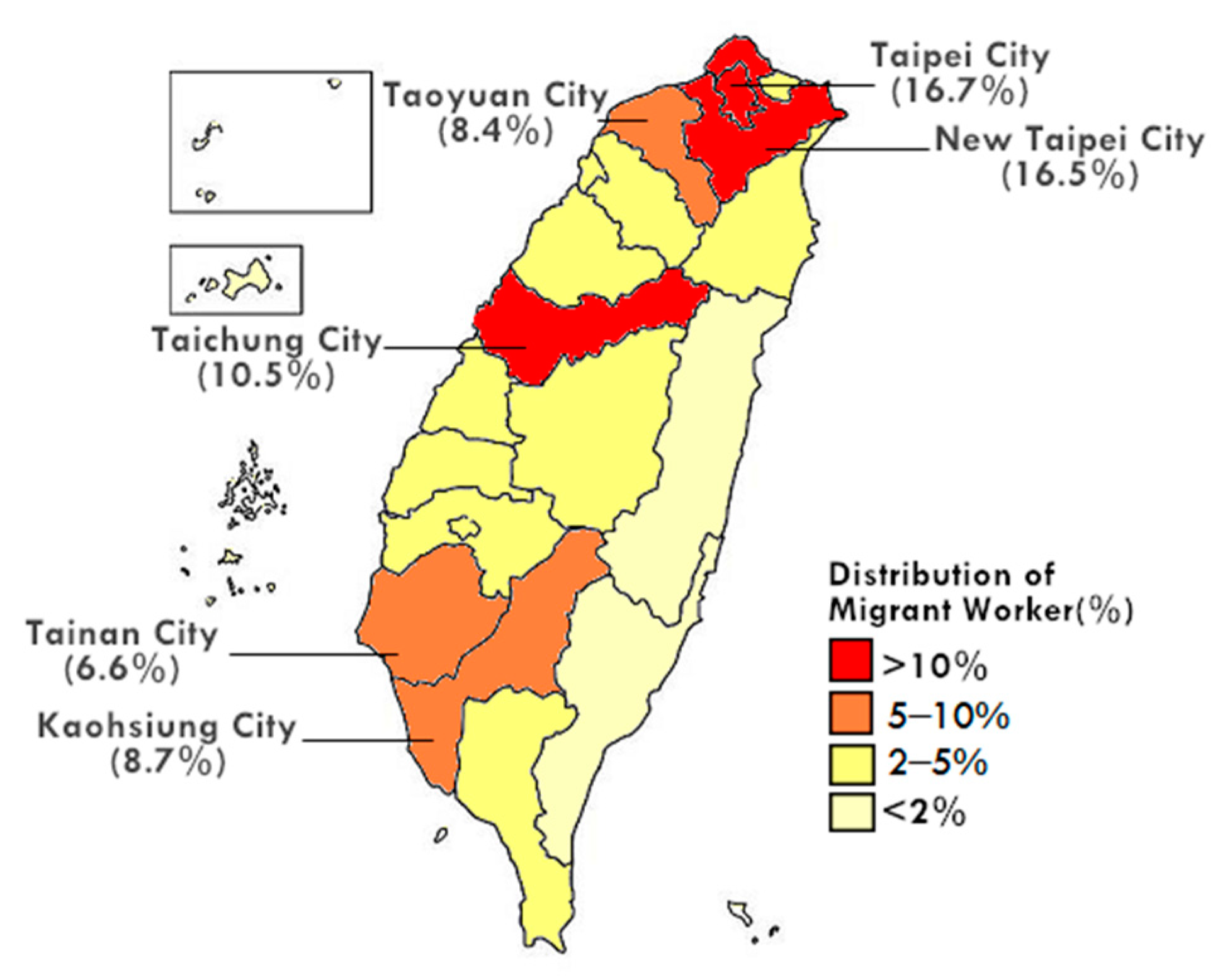
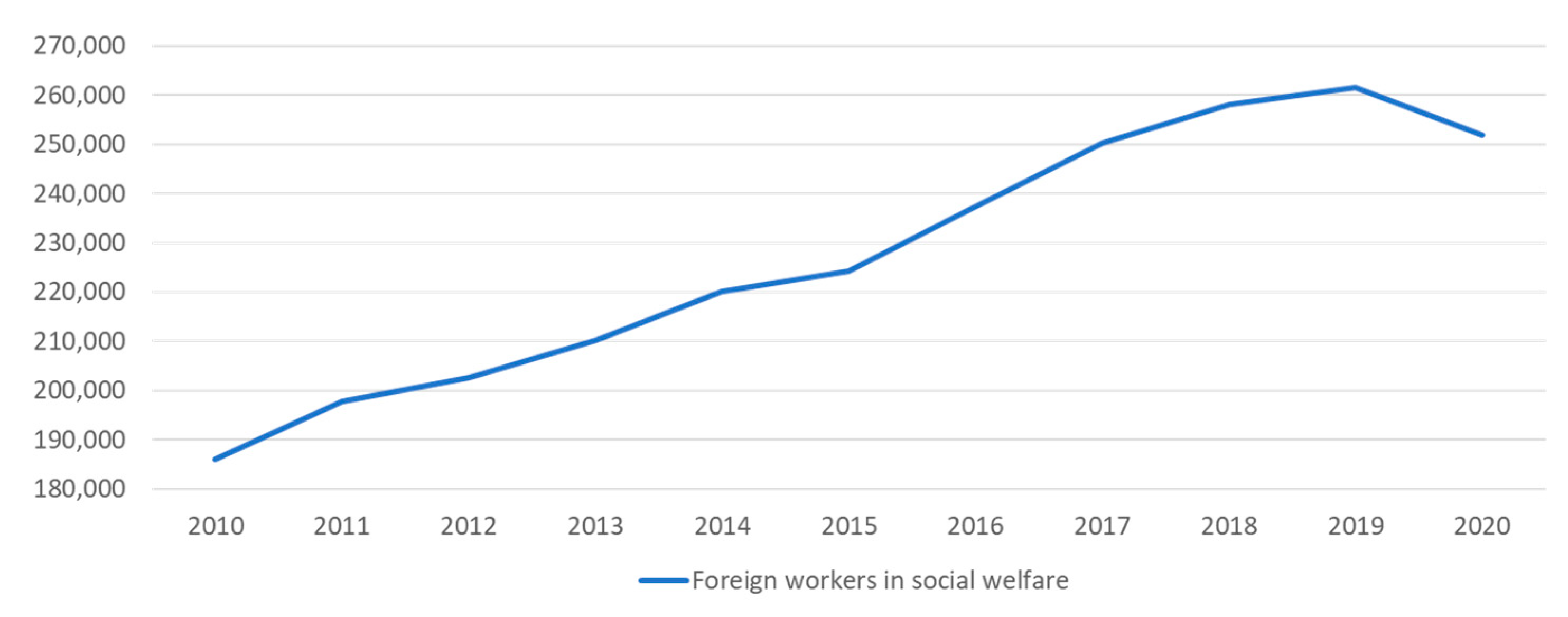
1.1. Foreign Domestic Workers (FDWs) in Taiwan
1.2. Linguistic Competence
1.3. Domains of Learnings and Using Teach-Back as a Method of Health Education
1.4. Burdens
2. Methods
2.1. Recruitment and Participants
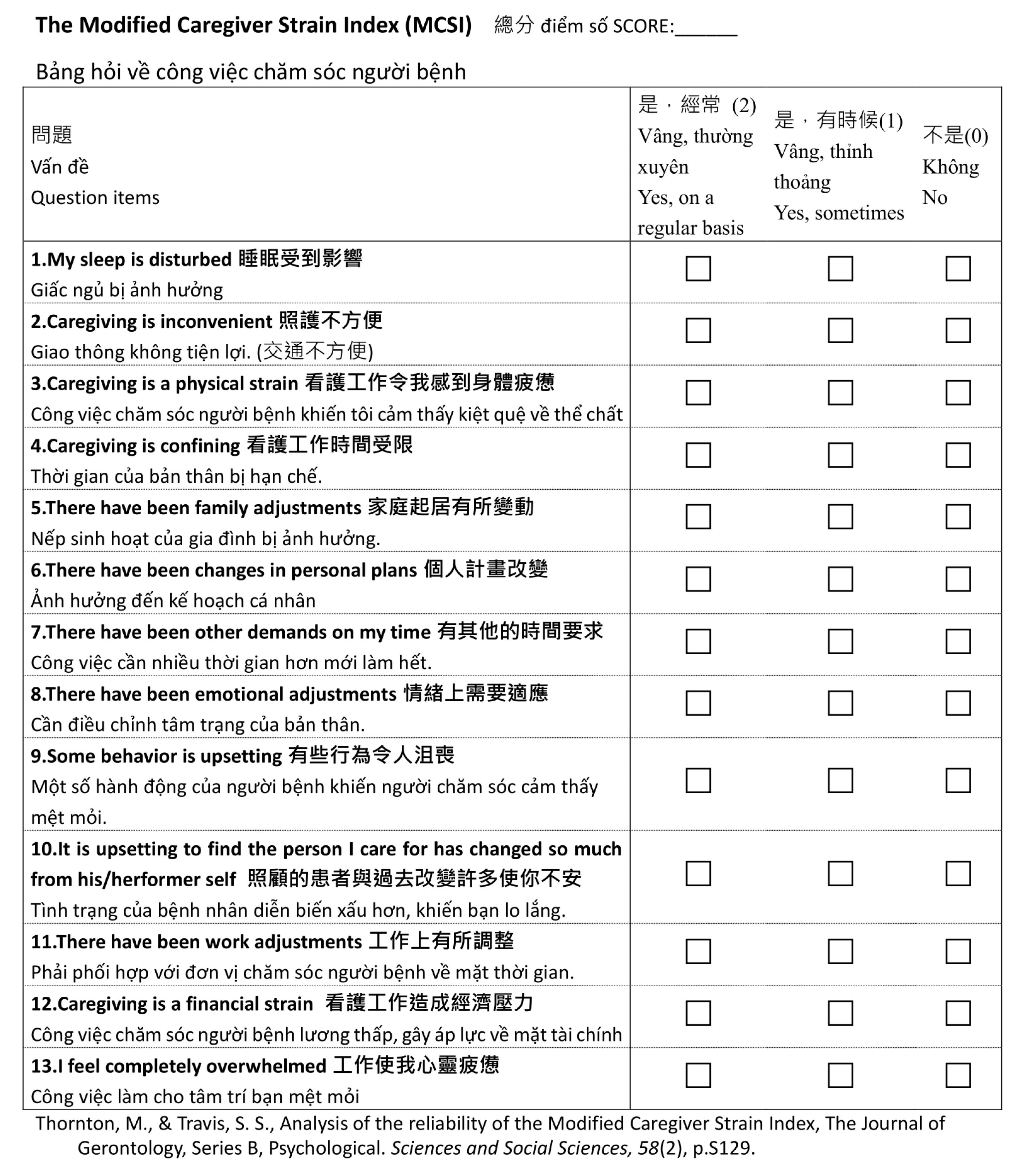
2.2. Using Modified Caregiver Strain Index (MCSI) Revised 2003
2.3. Thematic Analysis
“A theme is an abstract entity that brings meaning and identity to a recurrent experience and its variant manifestations. As such, a theme captures and unifies the nature or basis of the experience into a meaningful whole”.
3. Results
3.1. Participants’ Characteristics
3.2. The Modified Caregiver Strain Index (MCSI)
3.3. Thematic Analysis Major Themes
3.3.1. Theme 1: Language Communication
- Struggling in New Job in a Foreign Country
“When we came to Taiwan, we couldn’t communicate in Chinese at first”.(P01)
“When we first came to Taiwan, we could not understand Chinese very well. Although we have studied it in Vietnam, we found it was different from normal daily conversation”.(P08)
“Before I came to Taiwan, I had learned Chinese in Vietnam. In the beginning, people couldn’t understand what I talked about because of my Vietnamese accent”.(P06)
- 2.
- Communication Difficulties and Its Impact
“At work, some people cannot understand what I mean. It is hard for me to speak Chinese without an accent. When I speak Taiwanese (a Chinese dialect), the situation is even worse”.(P07)
“We can understand what people are saying to us, but we still cannot express ourselves in Chinese clearly”.(P08)
- 3.
- Consequences of Poor Communication
“The communication problem did affect my job … a colleague asked me to take some items, but I got the wrong ones because I did not understand exactly what they meant”.(P06)
“I got into trouble communicating at work … and it has caused many negative impacts. It is hard for me to deal with the communication problem. If it happens, all of my schedules will be delayed. Commutation problems have made the job even more difficult for me”.(P07)
- 4.
- Difficult to Communicate in Taiwanese Hokkien
“I have only learned Chinese (Mandarin Chinese), so I can’t communicate in Taiwanese (a Chinese dialect); it is so difficult. The elderly here speak Taiwanese, but I can’t understand what they are talking about”.(P03)
“I had never heard people speak Taiwanese until I arrived in Taiwan. We didn’t learn it in Vietnam”.(P10)
3.3.2. Theme 2: Work Burden and Job Strain
- Work Responsibility of Caregiver
“… We look after the residents, and sometimes we do the additional work they request. If there is no nurse around, and residents have something urgent, we have to deal with it”.(P02)
“I change their body position, change their diapers, replenish amenities, help them to take baths, feed them, and do nasogastric-tube-feeding for residents. I also help them to do the laundry, move them from bed to a wheelchair, and clean the toilets. There are so many chores to do”.(P04)
- 2.
- Ordeals at Work
“Sometimes we ask the residents to do something they don’t want to do; they will get irritated. Due to their illness, the elderly remains annoyed and cannot calm down. I will feel irritated! This is not an easy job”.(P01)
“There are problems between my colleagues … I get incomplete work tasks from my colleagues sometimes”.(P05)
“Some of the elderly don’t want to go to the toilet frequently, so they decide not to drink any water. I will ask them to drink some, but no matter how hard I try, they refuse”.(P07)
“It is impossible to handle each of them at the same time. Some of the elderly have a bad temper. They will scold us. And it is annoying if they murmur during the break time”.(P09)
- 3.
- Difficult Clients
“It is more stressful to take care of the residents who are in wheelchairs … they may fall down without any notice. We are worried and have to prevent falls. It really makes me stressed”.(P01)
“The elderly will be harder to take care of if they have just come here recently because we know nothing about them”.(P02)
“We have done things to help the residents, but they forgot, and they told their family members that we are unwilling to help them. It causes misunderstandings. They say something rude, too”.(P03)
“The elderly who suffer from dementia may sometimes hit others. We are not afraid of being hurt ourselves. Instead, we are worried that the other elderly residents may get hurt”.(P06)
“The residents keep calling my name, but they cannot remember why they asked me to come. They immediately forget what they said… they request us to do the same thing again and again”.(P10)
- 4.
- Physical Burden
“We are more understaffed now (in the COVID-19 pandemic). We don’t have enough caregivers here, so we need to do more tasks. It makes me a little bit tired”.(P03)
“Changing the elderly residents’ position is tiring for me. My shoulder hurts. If I lift something heavy, my shoulder will be more painful”.(P04)
“I feel tired of my job, and I want to get a new one. I need to walk around very frequently, and my legs hurt”(P10)
3.3.3. Theme 3: FDWs’ Responsibility and Risk
- Fear of Blame or Punishment
“We are responsible for the patients’ safety. If they fall, we will be punished and have to notify their family immediately”.(P01)
“We will need to tell their family and explain what happened. Although the nurse will deal with it, we think we also need to take responsibility for it. We will blame ourselves because we have not taken good care of them and caused them to get hurt. If any accidents happen, we will feel very sorry”.(P06)
“I hope that the families and supervisors can be more compassionate. We have a lot of work to do, and it is hard to do everything perfectly”.(P09)
- 2.
- Supervisors and Care Recipients’ Families
“Some of the families of the elderly are picky. For example, the hairdresser only comes in at a fixed time. The elderly cannot get their haircut whenever they want. Their families are always complaining about the length of their hair. Their families can complain about everything!”(P07)
“Some families of the elderly have a world of requirements. For example, skin problems are common and they are usually dissatisfied about this. They think the diapers must be cleaned and be changed more often. We follow their instructions, but they still make complaints. Some elderly lie in bed for a long time, so their skin may be in bad condition; if we move them, they will get a scrape and the family will scold us”(P09)
“Their family members will scold us if they find any wounds. Some elderly will even complain to their family members instead of telling us directly. It makes us stressed because the family would complain to the head nurse and other nurses”.(P10)
- 3.
- Occupational Exposure to Unknown Sources
“There is one thing that I worry about and that is if the resident is sick, but we don’t notice it immediately. We work with them closely and even live together. It is easy to get infected in our daily life, it is the most stressful thing in my work”.(P01)
“We have been infected by the residents before. Sometimes the residents feel itchy under their skin or have skin problems that are contagious. Or when the weather is bad, the residents may catch colds and then we may be infected too”.(P05)
3.3.4. Theme 4: Stress and Resilience
- Emotions and Feelings
“It makes me stressed if I can’t understand what the work assignments are. I don’t know what I should do at that moment”.(P01)
“If we were unfamiliar with our job routine after working here for a while, the colleagues who lead us would blame us. I feel stressed when this happens”.(P09)
“I feel very stressed when I cannot understand other people’s meanings or … I cannot handle my job well … the elderly also scold us too. I couldn’t understand what I am supposed to do at work, I even couldn’t understand what the elderly scold us, it is very stressful”.(P10)
- 2.
- Way to Relieve Stresses
“I go shopping when I feel tired from work, sometimes I enjoy playing on my cell phone, and hanging out with my friends. It will make me feel relaxed”.(P02)
“I will share stories with my friends, talk to them about something interesting, and tease them. They will make me feel happy”.(P04)
“I take a good rest, lie on my bed and sleep more when I face frustrations at work or suffer from fatigue. Going shopping after work can also make me happier”.(P05)
“When I am upset, I will get something to drink, or listen to music”.(P07)
- 3.
- Dealing with Deaths
“I have seen some deaths before. I felt stressed when I faced this kind of situation. Thus, I am worried about my family in Vietnam, and I miss them very much”.(P04)
“I felt very nervous and scared to look after the dying seniors. I worked in a factory in Vietnam before, so I had never encountered this kind of problem”.(P08)
“When I take care of the elderly who are dying, I am terrified. I am afraid of ghosts. Because of this reason, I hate to work the night shift especially in the Ghost Month. I would even bring a garlic in my pocket”.(P09)
3.3.5. Theme 5: Homesickness among Expatriates
- Expatriates Worried about Their Families
“I have started to worry about the elderly in my family since I began working here. My grandmother is even over 90 years old. I am afraid that I can’t keep them (my family members) company when they are sick”.(P01)
“Since I began working in Taiwan, I have started to worry about my family. I cannot travel back to my home country whenever I want. I am worried about them because I cannot see them face to face”.(P06)
- 2.
- Missing Home
“Although I love my job in Taiwan, I always feel homesick. At this moment, I am eager to go back to Vietnam and work there”.(P02)
“I miss my children, family, and friends very much, but I can’t go back”.(P07)
“I’m married, and my husband is in Vietnam. Even though I miss him, I cannot meet him”.(P08)
- 3.
- Returning Home
“I must be working here for three years then I can go back to my country. With the regulations in Vietnam, I cannot buy a flight ticket whenever I want”.(P02)
“If the COVID-19 situation improves, I can go back, but I still need to quarantine so it will take much time. People who want to travel back to Vietnam need to get vaccinated and quarantine, and when I travel back to Taiwan I need to quarantine again. The fee for quarantine is expensive and I also need to pay for flight tickets. It is very expensive”.(P05)
“Because of COVID-19, there is only one flight per week to Vietnam, and rarely a flight back to Taiwan”.(P10)
- 4.
- Support from Family and Friends
“In the past, my family members and my friends thought working in Taiwan was better than in Vietnam. Both my husband and my younger brother work here. However, now, my parents want me to go back to Vietnam and stay with my sister after the pandemic. Her salary is pretty good in Vietnam now”.(P06)
“My family would like me to go back to Vietnam, but they still support me to stay in Taiwan”.(P08)
“My friends in Vietnam hope I will go back. I only get minimum wage in this job. My classmates have their own homes and cars in Vietnam, but I have nothing here (in Taiwan)”.(P09)
4. Discussion
“All long-term care personnel should receive appropriate and adequate training programs. The training, continuing education, and on-the-job training programs for long-term care personnel shall consider the differences among regions, ethnic groups, genders, specific illnesses and care experiences”.[44]
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Workforce Development Agency. International Labor Statistics. Available online: https://english.mol.gov.tw/21004/21107/21113/lpsimplelist (accessed on 30 January 2022).
- Ministry of the Interior. Weekly Report. Available online: https://www.moi.gov.tw/cp.aspx?n=3909 (accessed on 30 January 2022).
- Liu, L.H. Personal Information, Autonomy, and Life Satisfation among Residents Living in Long-Term Care Facilities; I-Shou University: Kaohsiung, Taiwan, 2012. [Google Scholar]
- Lee, A.H.I.; Kang, H.Y.; Liu, Y.A. A Pilot Study on the Satisfaction of Long-Term Care Services in Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 90. [Google Scholar] [CrossRef] [PubMed]
- Troy, C.; Anna, T.; Perez, C.J.; Liu, J. Personal Determinants of Burden Among Indonesian Female Caregivers of Older Adults in Taiwan. J. Appl. Gerontol. 2022, 41, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Barry, T.T.; Brannon, D.; Mor, V. Nurse aide empowerment strategies and staff stability: Effects on nursing home resident outcomes. Gerontologist 2005, 45, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Castle, N.G.; Engberg, J. Staff turnover and quality of care in nursing homes. Med. Care 2005, 43, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Mansfield, J. Turnover among nursing home staff. A review. Nurs. Manag. 1997, 28, 59–62, 64. [Google Scholar] [CrossRef]
- Ministry of Labor. The Taiwan Case on the Influence for the Foreign Nursing Aid Services and the Specific of Labor Competencies Improvement. Available online: https://perma.cc/7DJG-Q8ND (accessed on 30 January 2022).
- National Development Council. Population Projections for the R.O.C. (Taiwan): 2018~2065. Available online: https://www.ndc.gov.tw/en/cp.aspx?n=2e5dcb04c64512cc (accessed on 30 January 2022).
- Potter, P.A.; Perry, A.G.; Stockert, P.; Hall, A. Fundamentals of Nursing; Elsevier Health Sciences: St. Louis, MO, USA, 2016. [Google Scholar]
- Ekman, S.L.; Wahlin, T.B.; Norberg, A.; Winblad, B. Relationship between bilingual demented immigrants and bilingual/monolingual caregivers. Int. J. Aging Hum. Dev. 1993, 37, 37–54. [Google Scholar] [CrossRef] [PubMed]
- Ha, N.H.L.; Chong, M.S.; Choo, R.W.M.; Tam, W.J.; Yap, P.L.K. Caregiving burden in foreign domestic workers caring for frail older adults in Singapore. Int. Psychogeriatr. 2018, 30, 1139–1147. [Google Scholar] [CrossRef]
- Bastable, S.B. Nurse as Educator: Principles of Teaching and Learning for Nursing Practice; Jones & Bartlett Learning: Burlington, MA, USA, 2014. [Google Scholar]
- Klingbeil, C.; Gibson, C. The Teach Back Project: A System-wide Evidence Based Practice Implementation. J. Pediatr. Nurs. 2018, 42, 81–85. [Google Scholar] [CrossRef]
- Talevski, J.; Wong Shee, A.; Rasmussen, B.; Kemp, G.; Beauchamp, A. Teach-back: A systematic review of implementation and impacts. PLoS ONE 2020, 15, e0231350. [Google Scholar] [CrossRef]
- Ho, K.H.M.; Wilson, I.M.; Wong, J.Y.H.; McKenna, L.; Reisenhofer, S.; Efendi, F.; Smith, G.D. Health stressors, problems and coping strategies of migrant domestic workers: A scoping review. Res. Sq. 2021. [Google Scholar] [CrossRef]
- Anjara, S.G.; Nellums, L.B.; Bonetto, C.; Van Bortel, T. Stress, health and quality of life of female migrant domestic workers in Singapore: A cross-sectional study. BMC Womens Health 2017, 17, 98. [Google Scholar] [CrossRef] [PubMed]
- Alves, L.C.S.; Monteiro, D.Q.; Bento, S.R.; Hayashi, V.D.; Pelegrini, L.N.C.; Vale, F.A.C. Burnout syndrome in informal caregivers of older adults with dementia: A systematic review. Dement. Neuropsychol. 2019, 13, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Stroka, M.A. The Mental and Physical Burden of Caregiving. Ruhr Econ. Pap. 2014. [Google Scholar] [CrossRef] [Green Version]
- Schulz, R.; Sherwood, P.R. Physical and mental health effects of family caregiving. Am. J. Nurs. 2008, 108, 23–27. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.Y.; Chiou, C.J.; Chen, N.S. Impact of mental health and caregiver burden on family caregivers’ physical health. Arch. Gerontol. Geriatr. 2010, 50, 267–271. [Google Scholar] [CrossRef]
- Robinson, B.C. Validation of a Caregiver Strain Index. J. Gerontol. 1983, 38, 344–348. [Google Scholar] [CrossRef] [PubMed]
- Thornton, M.; Travis, S.S. Analysis of the reliability of the modified caregiver strain index. J. Gerontol. B Psychol. Sci. Soc. Sci. 2003, 58, S127–S132. [Google Scholar] [CrossRef] [Green Version]
- Onega, L.L. The Modified Caregiver Strain Index (MCSI). Available online: https://www.sralab.org/sites/default/files/2017-07/issue-14.pdf (accessed on 15 October 2021).
- Dhandapani, M.; Gupta, S.; Dhandapani, S.; Kaur, P.; Samra, K.; Sharma, K.; Dolma, K.; Mohanty, M.; Singla, N.; Gupta, S.K. Study of factors determining caregiver burden among primary caregivers of patients with intracranial tumors. Surg. Neurol. Int. 2015, 6, 160. [Google Scholar] [CrossRef] [Green Version]
- Onega, L.L. Helping Those Who Help Others: The Modified Caregiver Strain Index. AJN Am. J. Nurs. 2008, 108, 62–69. [Google Scholar] [CrossRef]
- Kiger, M.E.; Varpio, L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med. Teach. 2020, 42, 846–854. [Google Scholar] [CrossRef]
- Terry, G.; Hayfield, N.; Clarke, V.; Braun, V. Thematic analysis. In The SAGE Handbook of Qualitative Research in Psychology, 2nd ed.; Willig, C., Rogers, W.S., Eds.; SAGE: London, UK, 2017; pp. 17–37. [Google Scholar]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis. Int. J. Qual. Methods 2017, 16, 1–13. [Google Scholar] [CrossRef]
- Attride-Stirling, J. Thematic networks: An analytic tool for qualitative research. Qual. Res. 2001, 1, 385–405. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- King, N. Using Templates in the Thematic Analysis of Text. In Essential Guide to Qualitative Methods in Organizational Research; Cassell, C., Symon, G., Eds.; SAGE: London, UK, 2004; pp. 256–270. [Google Scholar]
- DeSantis, L.; Ugarriza, D.N. The concept of theme as used in qualitative nursing research. West. J. Nurs. Res. 2000, 22, 351–372. [Google Scholar] [CrossRef] [PubMed]
- Boyatzis, R.E. Transforming Qualitative Information: Thematic Analysis and Code Development; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Suthendran, S.; Wessels, A.; Wong, M.; Keng, S.L. How to implement peer-based mental health services for foreign domestic workers in Singapore? In Proceedings of the Migrating Out of Poverty: From Evidence to Policy Conference, London, UK, 28 March 2017. [Google Scholar]
- Wessels, A. Home Sweet Home? Work, Life and Well-Being of Foreign Domestic Workers in Singapore; Humanitarian Organization for Migration Economics (HOME): Singapore, 2015. [Google Scholar]
- The Joint Commission. Core Measures. Available online: http://www.jointcommission.org/core_measure_sets.aspx (accessed on 15 January 2022).
- Hwang, K.; Williams, S.; Zucchi, E.; Chong, T.W.H.; Mascitti-Meuter, M.; Logiudice, D.; Goh, A.M.Y.; Panayiotou, A.; Batchelor, F. Testing the use of translation apps to overcome everyday healthcare communication in Australian aged-care hospital wards—An exploratory study. Nurs. Open 2022, 9, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.; Davies, P. Use of Google Translate in medical communication: Evaluation of accuracy. BMJ Br. Med. J. 2014, 349, g7392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, J.; Shi, K.; Yang, C.; Niu, Y.; Zeng, Y.; Zhang, N.; Liu, T.; Chu, C.H. Ethical issues of smart home-based elderly care: A scoping review. J. Nurs. Manag. 2021. [Google Scholar] [CrossRef]
- Majumder, S.; Aghayi, E.; Noferesti, M.; Memarzadeh-Tehran, H.; Mondal, T.; Pang, Z.; Deen, M.J. Smart Homes for Elderly Healthcare-Recent Advances and Research Challenges. Sensors 2017, 17, 2496. [Google Scholar] [CrossRef] [Green Version]
- Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences Engineering and Medicine. Families Caring for an Aging America; National Academies Press: Washington, DC, USA, 2016. [Google Scholar]
- Long-Term Care Services Act. Amended 2021 (Taiwan). Available online: https://law.moj.gov.tw/ENG/LawClass/LawAll.aspx?pcode=L0070040#:~:text=This%20Act%20is%20established%20in,the%20services%20and%20the%20care (accessed on 30 January 2022).
- Amankwaa, B.M.A. Informal Caregiver Stress. ABNF J. 2017, 28, 92–95. [Google Scholar]
- Malhotra, R.; Arambepola, C.; Tarun, S.; de Silva, V.; Kishore, J.; Østbye, T. Health issues of female foreign domestic workers: A systematic review of the scientific and gray literature. Int. J. Occup. Environ. Health 2013, 19, 261–277. [Google Scholar] [CrossRef]
- Nienhaus, A.; Kesavachandran, C.; Wendeler, D.; Haamann, F.; Dulon, M. Infectious diseases in healthcare workers-an analysis of the standardised data set of a German compensation board. J. Occup. Med. Toxicol. 2012, 7, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mok, K.Y.D. Foreign Domestic Workers in Hong Kong: Identifying Risk Factors, Resilience, and Psychological Well-Being; Brigham Young University: Provo, UT, USA, 2019. [Google Scholar]
- Iyer, A.; Devasahayam, T.W.; Yeoh, B.S.A. A Clean Bill of Health: Filipinas as Domestic Workers in Singapore. Asian Pac. Migr. J. 2004, 13, 11–38. [Google Scholar] [CrossRef]
- Shiba, Y.; Santangelo, A.M.; Roberts, A.C. Beyond the Medial Regions of Prefrontal Cortex in the Regulation of Fear and Anxiety. Front. Syst. Neurosci. 2016, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Jones, S. Medical aspects of expatriate health: Health threats. Occup. Med. 2000, 50, 572–578. [Google Scholar] [CrossRef] [Green Version]
- Deng, J.B.; Wahyuni, H.I.; Yulianto, V.I. Labor migration from Southeast Asia to Taiwan: Issues, public responses and future development. Asian Educ. Dev. Stud. 2020, 10, 69–81. [Google Scholar] [CrossRef]
- Trading Economics. Minimum Wages in Taiwan Increased to 24000 TWD/Month in 2021 from 23800 TWD/Month in 2020. Available online: https://tradingeconomics.com/taiwan/minimum-wages (accessed on 15 January 2022).
- Braun, V.; Clarke, V. Successful Qualitative Research: A Practical Guide for Beginners, 1st ed.; SAGE Publications: London, UK, 2013. [Google Scholar]
- Smith, J.A. Qualitative Psychology: A Practical Guide to Research Methods, 3rd ed.; SAGE Publications: London, UK, 2015. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Outline |
|---|
| “What do you usually do for your care recipient?” |
| “How did you learn to provide care for your care recipient?” |
| ” What difficulties did you face when providing care?” |
| “How do you overcome the difficulties you have faced?” |
| Participants | ||
|---|---|---|
| N (%) | Mean (SD) | |
| Gender | ||
| Female | 10 (100) | |
| Age (years) | 37.50 ± 8.23 | |
| 20–29 | 1 (10) | |
| 30–39 | 6 (60) | |
| 40–49 | 2 (20) | |
| 50–59 | 1 (10) | |
| Nationality | ||
| Vietnamese | 10 (100) | |
| Highest education level | ||
| Secondary (Junior High School) | 2 (20) | |
| High school | 6 (60) | |
| University or college | 2 (20) | |
| Marital status | ||
| Married | 8 (80) | |
| Single | 2 (20) | |
| Number of children | 1.00 ± 0.82 | |
| 0 | 3 (30) | |
| 1 | 4 (40) | |
| 2 | 3 (30) | |
| Language for communication | ||
| Chinese | 10 (100) | |
| Taiwanese | 8 (80) | |
| English | 3 (30) | |
| Vietnamese | 10 (100) | |
| Caregiving experience in their current position (years) | 5.80 ± 2.83 | |
| <1 | 1 (10) | |
| 1–2 | 1 (10) | |
| 3–4 | 1 (10) | |
| 5–10 | 7 (70) | |
| Daily hours spent for caregiving (hours) | 13.30 ± 2.53 | |
| 6–11 | 2 (20) | |
| 12–17 | 8 (80) | |
| Prior caregiving experience | ||
| Yes | 7 (70) | |
| No | 3 (30) | |
| Prior caregiving training | ||
| Yes | 10 (100) | |
| No | 0 (0) | |
| Average Score | ||||
|---|---|---|---|---|
| Pre-Test (First Week) | Mid-Test (6 Week) | Post-Test (12 Week) | ||
| Physical | 1. My sleep is disturbed | 0.7 | 1 | 0.9 |
| 2. Caregiving is inconvenient | 0.9 | 0.3 | 0.6 | |
| 3. Caregiving is a physical strain | 0.9 | 0.6 | 1.0 | |
| Social/personal | 4. Caregiving is confining | 0 | 0.8 | 0.9 |
| 5. There have been family adjustments | 0.1 | 0.6 | 0.5 | |
| 6. There have been changes in personal plans | 0 | 0.8 | 0.6 | |
| 7. There have been other demands on my time | 0.4 | 0.9 | 1.1 | |
| 8. There have been work adjustments | 0.2 | 1.1 | 1.4 | |
| Psychological | 9. There have been emotional adjustments | 0.5 | 0.7 | 1.0 |
| 10. Some behavior is upsetting | 0.2 | 1.1 | 1.1 | |
| 11. It is upsetting to find the person I care for has changed so much from his/her former self | 0.7 | 0.6 | 0.6 | |
| 12. I feel completely overwhelmed | 0.3 | 0.7 | 1.3 | |
| Financial | 13. Caregiving is a financial strain | 0.4 | 0.8 | 1.1 |
| Total (maximum 26) low (0–8), moderate (9–18), and high (19–26) | 5.3 | 10 | 12.1 | |
| Themes | Subthemes |
|---|---|
|
|
|
|
|
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-Y.; Li, Y.-Y.; Lyver, M.J. Elderly Caregiving Quality Improvement: A Pilot Study of the Burdens of Vietnamese Caregivers in Taiwan. Int. J. Environ. Res. Public Health 2022, 19, 6293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106293
Wu C-Y, Li Y-Y, Lyver MJ. Elderly Caregiving Quality Improvement: A Pilot Study of the Burdens of Vietnamese Caregivers in Taiwan. International Journal of Environmental Research and Public Health. 2022; 19(10):6293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106293
Chicago/Turabian StyleWu, Chang-Yu, Yu-Ying Li, and Maurice J. Lyver. 2022. "Elderly Caregiving Quality Improvement: A Pilot Study of the Burdens of Vietnamese Caregivers in Taiwan" International Journal of Environmental Research and Public Health 19, no. 10: 6293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19106293