
Innovative Application of Diathermy in Orthodontics: A Case Report

 ,
,  , ,
, ,  , ,
, ,  , , , , ,
, , , , ,  , , ,
, , ,  ,
,  , , ,
, , ,  , , ,
, , ,  and
and  add
Show full author list
add
Show full author list
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
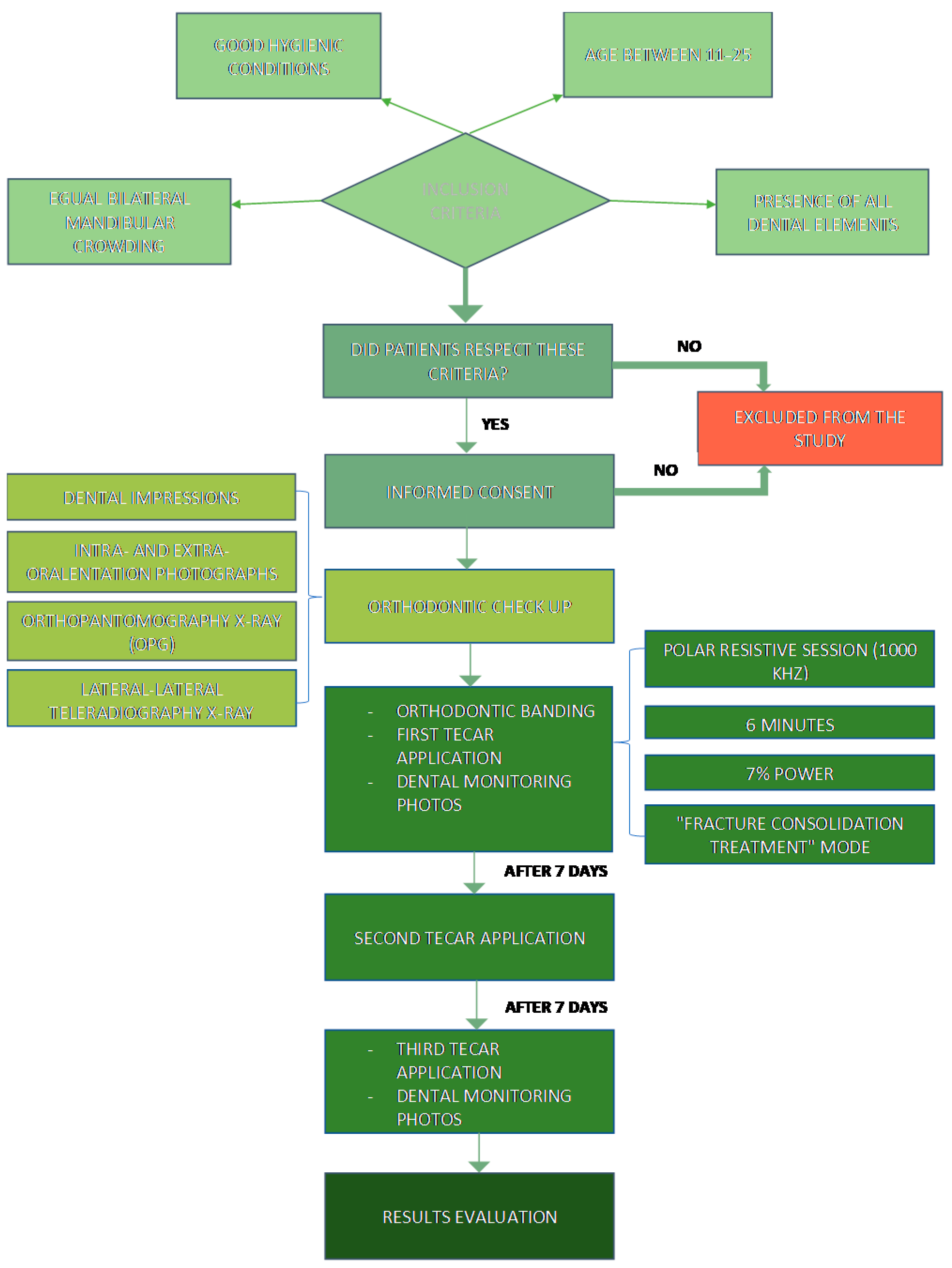
2.1. Inclusion and Exclusion Criteria
- Marked bilateral mandibular dental crowding of equal entity;
- Presence of all dental elements;
- Good hygienic conditions;
- Between 11 and 25 years of age.
- Bilateral uneven right- and left-sided tooth crowding;
- Developmental age.
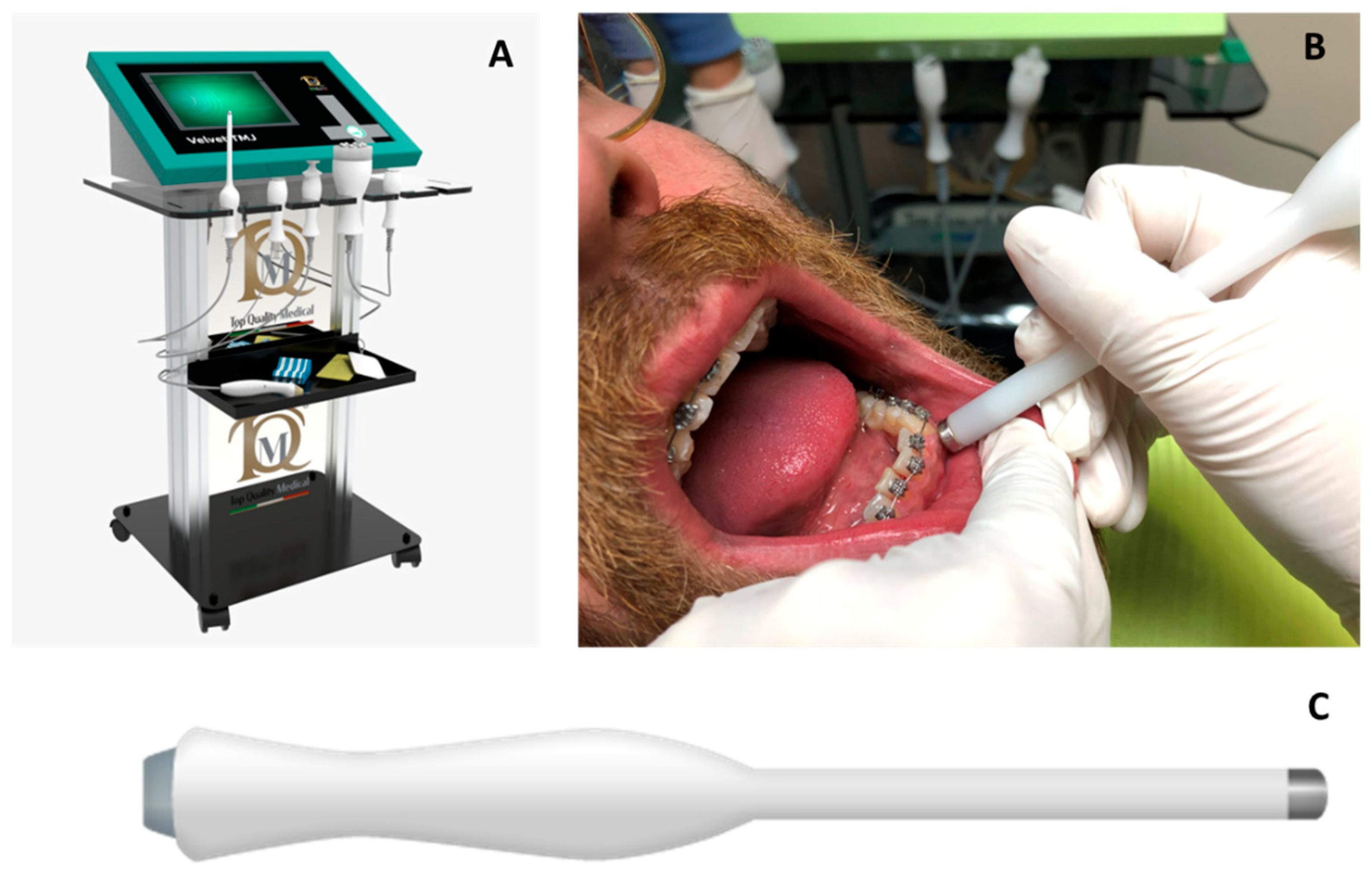
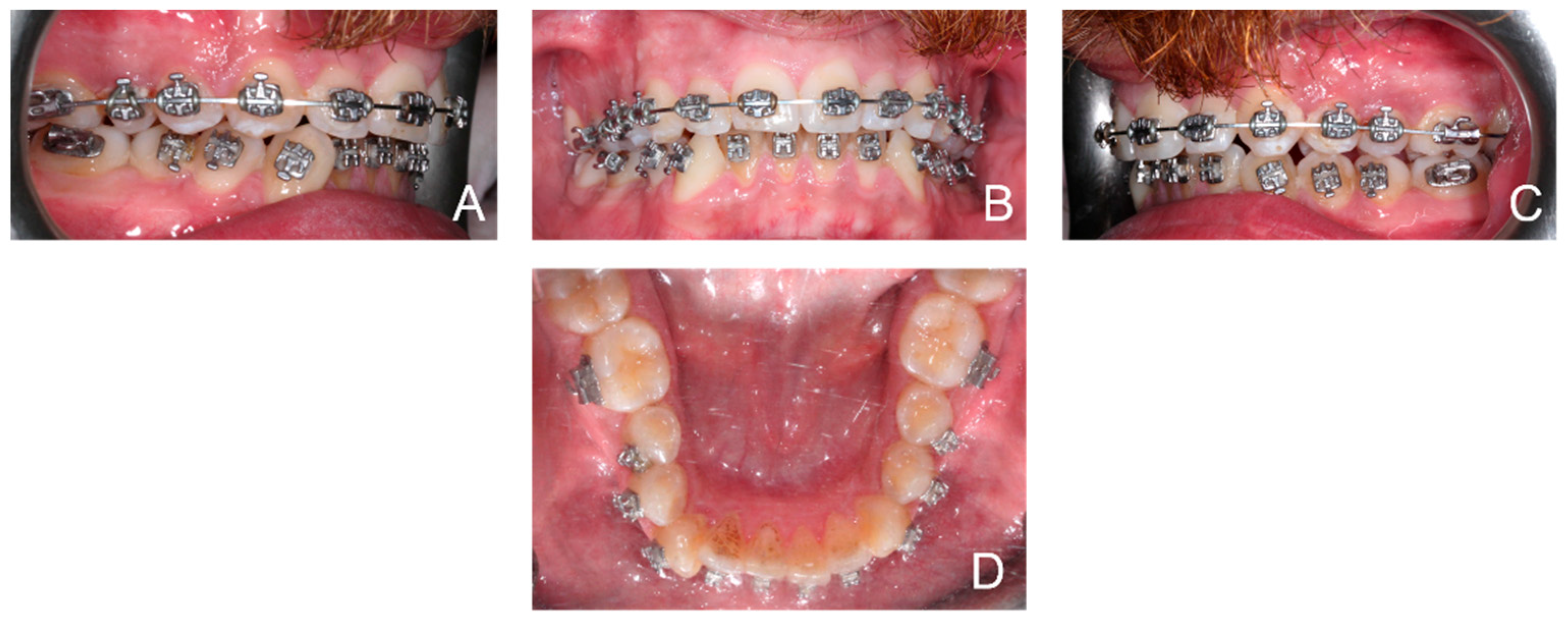
2.2. Case Description and Treatment Protocol
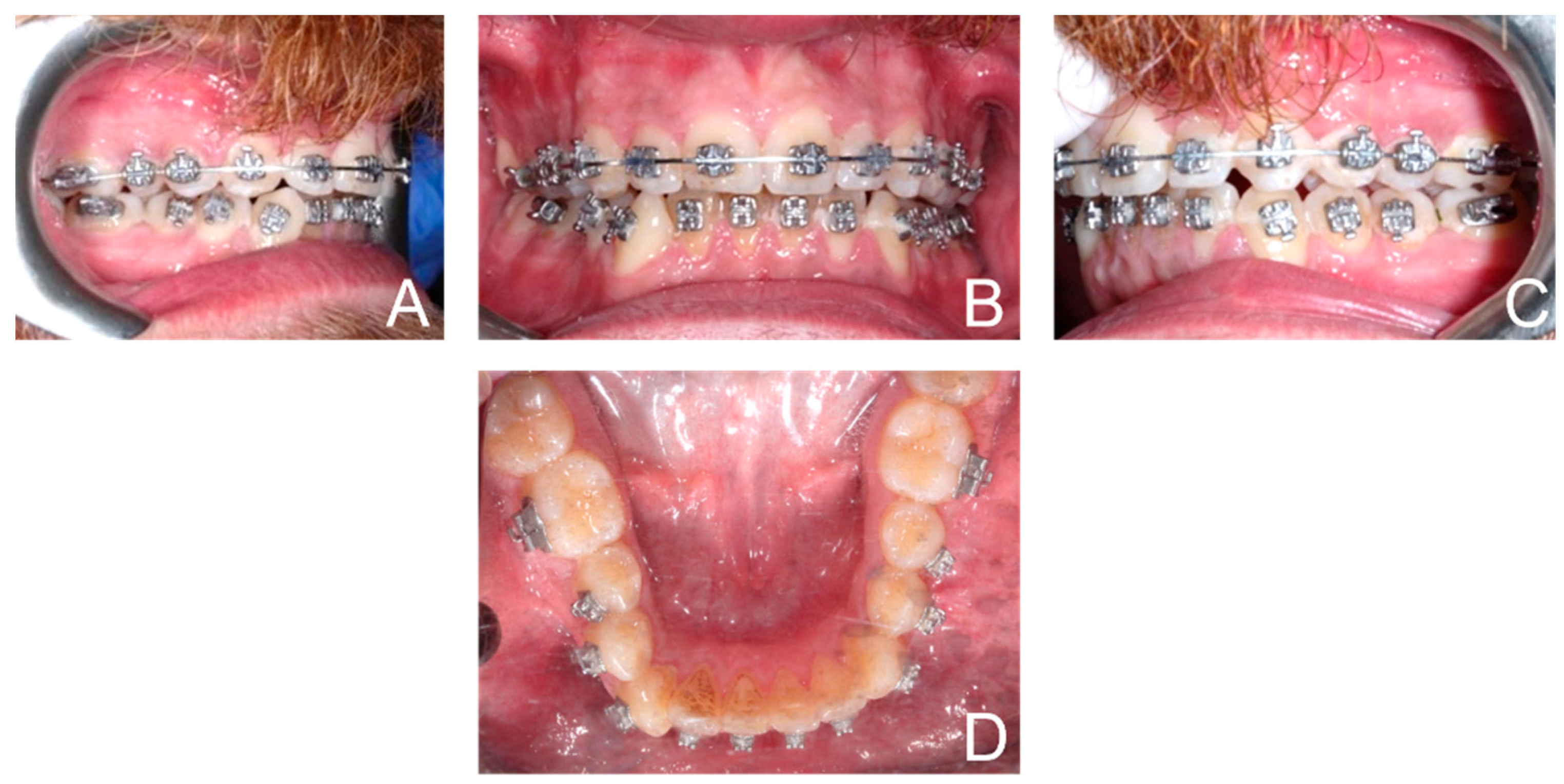
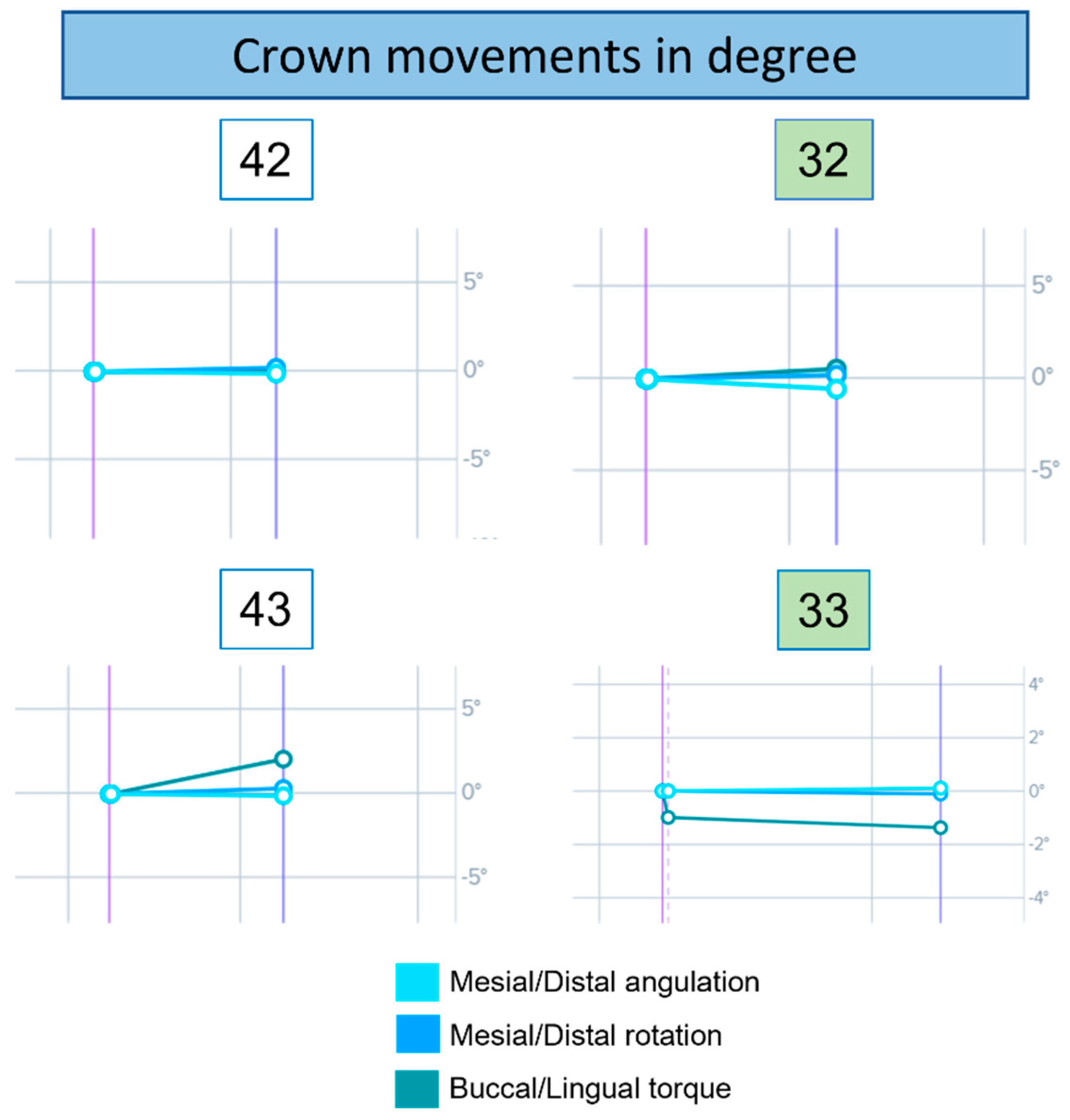
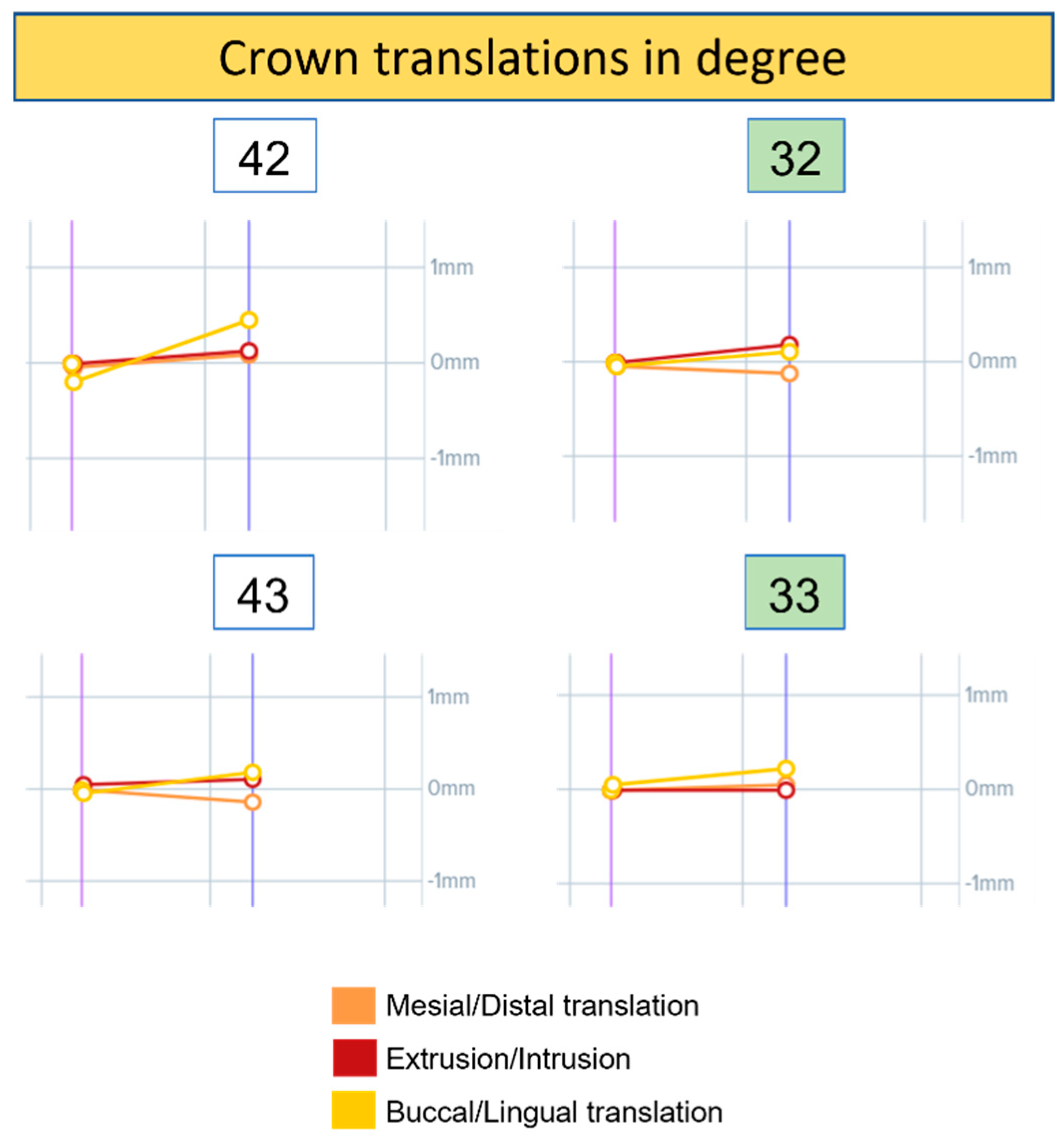
3. Results
- 32 showed a slight variation in angulation and torque compared to 42. The rotation is unchanged in both cases.
- 33 and 43 reached the same absolute torque value at the end of the observation period. However, 43 had a greater variation. Angulation and mesiodistal rotation were almost unchanged in both cases.
- 32 showed a greater variation in mesiodistal translation and intrusion–extrusion than element 42. The latter, however, had a little variation in buccolingual translation.
- 33 showed a greater variation in buccolingual translation compared to 43. The latter had a greater variation in mesiodistal translation than 33.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAP | DiathermyCapacitive mode |
| EGF | Epidermal Growth Factor |
| HFA | High Frequency Acceleration |
| MCSF | Macrophage colony-stimulating factor |
| NITI | Nickel–Titanium |
| OPG | Orthopantomogram |
| PDL | Periodontal ligament |
| PGE | Prostaglandin E |
| PTH | Parathyroid hormone |
| RANK-L | Receptor activator of nuclear factor kappa-Β ligand |
| RES | Diathermy Resistive mode |
| TECAR | Capacitive and Resistive Energy Transfer |
References
- Young, L.; Binderman, I.; Yaffe, A.; Beni, L.; Vardimon, A.D. Fiberotomy Enhances Orthodontic Tooth Movement and Diminishes Relapse in a Rat Model. Orthod. Craniofacial Res. 2013, 16, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Limpanichkul, W.; Godfrey, K.; Srisuk, N.; Rattanayatikul, C. Effects of Low-Level Laser Therapy on the Rate of Orthodontic Tooth Movement. Orthod. Craniofacial Res. 2006, 9, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Bartzela, T.; Türp, J.C.; Motschall, E.; Maltha, J.C. Medication Effects on the Rate of Orthodontic Tooth Movement: A Systematic Literature Review. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Khurshid, Z.; Asiri, F.Y. Influence of Intermittent Parathyroid Hormone (PTH) Administration on the Outcomes of Orthodontic Tooth Movement—A Systematic Review. Appl. Sci. 2021, 11, 5268. [Google Scholar] [CrossRef]
- Davidovitch, Z. Tooth Movement. Crit. Rev. Oral Biol. Med. 1991, 2, 411–450. [Google Scholar] [CrossRef]
- Di Venere, D.; Pettini, F.; Nardi, G.M.; Laforgia, A.; Stefanachi, G.; Notaro, V.; Rapone, B.; Grassi, F.R.; Corsalini, M. Correlation between Parodontal Indexes and Orthodontic Retainers: Prospective Study in a Group of 16 Patients. Oral Implantol. 2017, 10, 78–86. [Google Scholar] [CrossRef]
- Fatima, T.; Khurshid, Z.; Rehman, A.; Imran, E.; Srivastava, K.C.; Shrivastava, D. Gingival Crevicular Fluid (GCF): A Diagnostic Tool for the Detection of Periodontal Health and Diseases. Molecules 2021, 26, 1208. [Google Scholar] [CrossRef]
- Nimeri, G.; Kau, C.H.; Abou-Kheir, N.S.; Corona, R. Acceleration of Tooth Movement during Orthodontic Treatment—A Frontier in Orthodontics. Prog. Orthod. 2013, 14, 42. [Google Scholar] [CrossRef] [Green Version]
- Maspero, C.; Cappella, A.; Dolci, C.; Cagetti, M.G.; Inchingolo, F.; Sforza, C. Is Orthodontic Treatment with Microperforations Worth It? A Scoping Review. Children 2022, 9, 208. [Google Scholar] [CrossRef]
- Coloccia, G.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Montenegro, V.; Patano, A.; Marinelli, G.; Laudadio, C.; Limongelli, L.; Di Venere, D.; et al. Effectiveness of Dental and Maxillary Transverse Changes in Tooth-Borne, Bone-Borne, and Hybrid Palatal Expansion through Cone-Beam Tomography: A Systematic Review of the Literature. Medicina 2021, 57, 288. [Google Scholar] [CrossRef]
- Patianna, A.G.; Ballini, A.; Meneghello, M.; Cantore, S.; Inchingolo, A.M.; Dipalma, G.; Inchingolo, A.D.; Inchingolo, F.; Malcangi, G.; Lucchese, A.; et al. Comparison of Conventional Orthognathic Surgery and “Surgery-First” Protocol: A New Weapon against Time. J. Biol. Regul. Homeost. Agents 2019, 33, 59–67. [Google Scholar] [PubMed]
- Kumaran, B.; Watson, T. Thermal Build-up, Decay and Retention Responses to Local Therapeutic Application of 448 KHz Capacitive Resistive Monopolar Radiofrequency: A Prospective Randomised Crossover Study in Healthy Adults. Int. J. Hyperth. 2015, 31, 883–895. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Tatullo, M.; Marrelli, M.; Inchingolo, A.M.; Tarullo, A.; Inchingolo, A.D.; Dipalma, G.; Brunetti, S.P.; Tarullo, A.; Cagiano, R. Combined Occlusal and Pharmacological Therapy in the Treatment of Temporo-Mandibular Disorders. Eur. Rev. Med. Pharmacol. Sci. 2011, 15, 1296–1300. [Google Scholar] [PubMed]
- Cozzani, M.; Sadri, D.; Nucci, L.; Jamilian, P.; Pirhadirad, A.P.; Jamilian, A. The Effect of Alexander, Gianelly, Roth, and MBT Bracket Systems on Anterior Retraction: A 3-Dimensional Finite Element Study. Clin. Oral Investig. 2020, 24, 1351–1357. [Google Scholar] [CrossRef]
- Farronato, M.; Dolci, C.; Boccalari, E.; Izadi, S.; Salvatierra Rios, L.H.; Festa, M.; Panetta, V.; De Vito, D.; Tartaglia, G.M. Serological Profile of Children and Young Adults with at Least One SARS-CoV-2 Positive Cohabitant: An Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 1488. [Google Scholar] [CrossRef]
- Clijsen, R.; Leoni, D.; Schneebeli, A.; Cescon, C.; Soldini, E.; Li, L.; Barbero, M. Does the Application of Tecar Therapy Affect Temperature and Perfusion of Skin and Muscle Microcirculation? A Pilot Feasibility Study on Healthy Subjects. J. Altern. Complementary Med. 2020, 26, 147–153. [Google Scholar] [CrossRef]
- Montenegro, V. Compliance of Children with Removable Functional Appliance with Microchip Integrated during COVID-19 Pandemic: A Systematic Review. J. Biol. Regul. Homeost. Agents 2021, 35, 365–377. [Google Scholar] [CrossRef]
- Cirulli, N.; Ballini, A.; Cantore, S.; Farronato, D.; Inchingolo, F.; Dipalma, G.; Gatto, M.R.; Alessandri Bonetti, G. Mixed Dentition Space Analysis of a Southern Italian Population: New Regression Equations for Unerupted Teeth. J. Biol. Regul. Homeost. Agents 2015, 29, 515–520. [Google Scholar]
- Farronato, M.; Tadakamadla, S.K.; Ali Quadri, M.F.; Acharya, S.; Tadakamadla, J.; Love, R.M.; Jamal, M.; Mulder, R.; Maspero, C.; Farronato, D.; et al. A Call for Action to Safely Deliver Oral Health Care during and Post COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6704. [Google Scholar] [CrossRef]
- Kuriakose, P.; Greenlee, G.M.; Heaton, L.J.; Khosravi, R.; Tressel, W.; Bollen, A.-M. The Assessment of Rapid Palatal Expansion Using a Remote Monitoring Software. J. World Fed. Orthod. 2019, 8, 165–170. [Google Scholar] [CrossRef]
- Moylan, H.B.; Carrico, C.K.; Lindauer, S.J.; Tüfekçi, E. Accuracy of a Smartphone-Based Orthodontic Treatment–Monitoring Application: A Pilot Study. Angle Orthod. 2019, 89, 727–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoreibah, E.A.; Salama, A.E.; Attia, M.S.; Abu-Seida, S.M.A.-M. Corticotomy-Facilitated Orthodontics in Adults Using a Further Modified Technique. J. Int. Acad. Periodontol. 2012, 14, 97–104. [Google Scholar]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Palmieri, G.; et al. Genetic Pattern, Orthodontic and Surgical Management of Multiple Supplementary Impacted Teeth in a Rare, Cleidocranial Dysplasia Patient: A Case Report. Medicina 2021, 57, 1350. [Google Scholar] [CrossRef] [PubMed]
- Laudadio, C. Management of Anterior Open-Bite in the Deciduous, Mixed and Permanent Dentition Stage: A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Isacco, C.G.; Ballini, A.; De Vito, D.; Nguyen, K.C.D.; Cantore, S.; Bottalico, L.; Quagliuolo, L.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; et al. Rebalancing the Oral Microbiota as an Efficient Tool in Endocrine, Metabolic and Immune Disorders. Endocr. Metab. Immune Disord. Drug Targets 2021, 21, 777–784. [Google Scholar] [CrossRef]
- Neyt, N.M.F.; Mommaerts, M.Y.; Abeloos, J.V.S.; De Clercq, C.A.S.; Neyt, L.F. Problems, Obstacles and Complications with Transpalatal Distraction in Non-Congenital Deformities. J. Cranio-Maxillofac Surg. 2002, 30, 139–143. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Jacox, L.A.; Little, S.H.; Ko, C.-C. Orthodontic Tooth Movement: The Biology and Clinical Implications. Kaohsiung J. Med. Sci. 2018, 34, 207–214. [Google Scholar] [CrossRef] [Green Version]
- d’Apuzzo, F.; Minervini, G.; Grassia, V.; Rotolo, R.P.; Perillo, L.; Nucci, L. Mandibular Coronoid Process Hypertrophy: Diagnosis and 20-Year Follow-Up with CBCT, MRI and EMG Evaluations. Appl. Sci. 2021, 11, 4504. [Google Scholar] [CrossRef]
- De Felice, M.E.; Nucci, L.; Fiori, A.; Flores-Mir, C.; Perillo, L.; Grassia, V. Accuracy of Interproximal Enamel Reduction during Clear Aligner Treatment. Prog. Orthod. 2020, 21, 28. [Google Scholar] [CrossRef]
- Brudvik, P.; Rygh, P. Root Resorption after Local Injection of Prostaglandin E2 during Experimental Tooth Movement. Eur. J. Orthod. 1991, 13, 255–263. [Google Scholar] [CrossRef]
- Di Venere, D.; Nardi, G.M.; Lacarbonara, V.; Laforgia, A.; Stefanachi, G.; Corsalini, M.; Grassi, F.R.; Rapone, B.; Pettini, F. Early Mandibular Canine-Lateral Incisor Transposition: Case Report. Oral Implantol. 2017, 10, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Di Venere, D.; Corsalini, M.; Nardi, G.M.; Laforgia, A.; Grassi, F.R.; Rapone, B.; Pettini, F. Obstructive Site Localization in Patients with Obstructive Sleep Apnea Syndrome: A Comparison between Otolaryngologic Data and Cephalometric Values. Oral Implantol. 2017, 10, 295–310. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Montenegro, V.; Laudadio, C.; Pede, C.D.; et al. The Efficacy of a New AMCOP® Elastodontic Protocol for Orthodontic Interceptive Treatment: A Case Series and Literature Overview. Int. J. Environ. Res. Public Health 2022, 19, 988. [Google Scholar] [CrossRef]
- Bavetta, G.; Bavetta, G.; Randazzo, V.; Cavataio, A.; Paderni, C.; Grassia, V.; Dipalma, G.; Gargiulo Isacco, C.; Scarano, A.; De Vito, D.; et al. A Retrospective Study on Insertion Torque and Implant Stability Quotient (ISQ) as Stability Parameters for Immediate Loading of Implants in Fresh Extraction Sockets. Biomed Res. Int. 2019, 2019, 9720419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alves, J.B.; Ferreira, C.L.; Martins, A.F.; Silva, G.A.B.; Alves, G.D.; Paulino, T.P.; Ciancaglini, P.; Thedei, G.; Napimoga, M.H. Local Delivery of EGF-Liposome Mediated Bone Modeling in Orthodontic Tooth Movement by Increasing RANKL Expression. Life Sci. 2009, 85, 693–699. [Google Scholar] [CrossRef]
- Li, F.; Li, G.; Hu, H.; Liu, R.; Chen, J.; Zou, S. Effect of Parathyroid Hormone on Experimental Tooth Movement in Rats. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 523–532. [Google Scholar] [CrossRef]
- Cardarelli, F.; Patano, A.; Montenegro, V.; Malcangi, G.; Coloccia, G.; Inchingolo, A.D.; Marinelli, G.; Laudadio, C.; Dipalma, G.; Di Venere, D.; et al. Elastodontic therapy un nuovo approccio alla terapia ortodontica funzionale. Il Dent. Mod. 2021, 10, 48–63. [Google Scholar]
- Takano-Yamamoto, T.; Kawakami, M.; Kobayashi, Y.; Yamashiro, T.; Sakuda, M. The Effect of Local Application of 1,25-Dihydroxycholecalciferol on Osteoclast Numbers in Orthodontically Treated Rats. J. Dent. Res. 1992, 71, 53–59. [Google Scholar] [CrossRef]
- Hashimoto, F.; Kobayashi, Y.; Mataki, S.; Kobayashi, K.; Kato, Y.; Sakai, H. Administration of Osteocalcin Accelerates Orthodontic Tooth Movement Induced by a Closed Coil Spring in Rats. Eur. J. Orthod. 2001, 23, 535–545. [Google Scholar] [CrossRef]
- Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Inchingolo, A.M.; Marinelli, G.; Malcangi, G.; Di Pede, C.; Garibaldi, M.; Ciocia, A.M.; et al. Treatment of Class III Malocclusion and Anterior Crossbite with Aligners: A Case Report. Medicina 2022, 58, 603. [Google Scholar] [CrossRef]
- Alikhani, M.; Alansari, S.; Hamidaddin, M.A.; Sangsuwon, C.; Alyami, B.; Thirumoorthy, S.N.; Oliveira, S.M.; Nervina, J.M.; Teixeira, C.C. Vibration Paradox in Orthodontics: Anabolic and Catabolic Effects. PLoS ONE 2018, 13, e0196540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patano, A.; Cirulli, N.; Beretta, M.; Plantamura, P.; Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Malcangi, G.; Marinelli, G.; Scarano, A.; et al. Education Technology in Orthodontics and Paediatric Dentistry during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 6056. [Google Scholar] [CrossRef] [PubMed]
- Adina, S. Orthopedic Joint Stability Influences Growth and Maxillary Development: Clinical Aspects. J. Biol. Regul. Homeost. Agents 2020, 34, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Cirulli, N.; Cantore, S.; Ballini, A.; Perillo, L.; Giannico, O.V.; Tafuri, S.; De Vito, D. Prevalence of Caries and Dental Malocclusions in the Apulian Paediatric Population: An Epidemiological Study. Eur. J. Paediatr. Dent. 2019, 20, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Osti, R.; Pari, C.; Salvatori, G.; Massari, L. Tri-Length Laser Therapy Associated to Tecar Therapy in the Treatment of Low-Back Pain in Adults: A Preliminary Report of a Prospective Case Series. Lasers. Med. Sci. 2015, 30, 407–412. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; Farronato, D.; Malcangi, G.; Dipalma, G.; Assandri, F.; Garagiola, U.; Inchingolo, F.; De Vito, D.; Cirulli, N. Evaluation of an Oral Appliance in Patients with Mild to Moderate Obstructive Sleep Apnea Syndrome Intolerant to Continuous Positive Airway Pressure Use: Preliminary Results. Int. J. Immunopathol. Pharmacol. 2016, 29, 267–273. [Google Scholar] [CrossRef] [Green Version]
- Marra, P.; Nucci, L.; Abdolreza, J.; Perillo, L.; Itro, A.; Grassia, V. Odontoma in a Young and Anxious Patient Associated with Unerupted Permanent Mandibular Cuspid: A Case Report. J. Int. Oral Health 2020, 12, 182. [Google Scholar] [CrossRef]
- Cantore, S.; Ballini, A.; De Vito, D.; Abbinante, A.; Altini, V.; Dipalma, G.; Inchingolo, F.; Saini, R. Clinical Results of Improvement in Periodontal Condition by Administration of Oral Probiotics. J. Biol. Regul. Homeost. Agents 2018, 32, 1329–1334. [Google Scholar]
- Inchingolo, A.D.; Ceci, S.; Patano, A.; Inchingolo, A.M.; Montenegro, V.; Di Pede, C.; Malcangi, G.; Marinelli, G.; Coloccia, G.; Garibaldi, M.; et al. Elastodontic Therapy of Hyperdivergent Class II Patients Using AMCOP® Devices: A Retrospective Study. Appl. Sci. 2022, 12, 3259. [Google Scholar] [CrossRef]
- Ballini, A.; Cantore, S.; Fotopoulou, E.A.; Georgakopoulos, I.P.; Athanasiou, E.; Bellos, D.; Paduanelli, G.; Saini, R.; Dipalma, G.; Inchingolo, F. Combined Sea Salt-Based Oral Rinse with Xylitol in Orthodontic Patients: Clinical and Microbiological Study. J. Biol. Regul. Homeost. Agents 2019, 33, 263–268. [Google Scholar]
- Marinelli, G. White Spot Lesions in Orthodontics: Prevention and Treatment. A Descriptive Review. J. Biol. Regul. Homeost. Agents 2021, 35, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Di Venere, D.; Rapone, B.; Corsalini, M. Dental Trauma in the Anterior Sector: An Analysis of the Predisposing Factors in a Group of Orthodontic Patients. Clin. Ther. 2020, 171, e481–e485. [Google Scholar] [CrossRef]
- d’Apuzzo, F.; Nucci, L.; Strangio, B.M.; Inchingolo, A.D.; Dipalma, G.; Minervini, G.; Perillo, L.; Grassia, V. Dento-Skeletal Class III Treatment with Mixed Anchored Palatal Expander: A Systematic Review. Appl. Sci. 2022, 12, 4646. [Google Scholar] [CrossRef]
- Militi, A.; Cicciù, M.; Sambataro, S.; Bocchieri, S.; Cervino, G.; De Stefano, R.; Fiorillo, L. Dental Occlusion and Sport Performance. Minerva Stomatol. 2020, 69, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Impellizzeri, A.; Midulla, G.; Romeo, U.; La Monaca, C.; Barbato, E.; Galluccio, G. Delayed Eruption of Permanent Dentition and Maxillary Contraction in Patients with Cleidocranial Dysplasia: Review and Report of a Family. Int. J. Dent. 2018, 2018, 6591414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayama, A.; Seiryu, M.; Takano-Yamamoto, T. Effect of Vibration on Orthodontic Tooth Movement in a Double Blind Prospective Randomized Controlled Trial. Sci. Rep. 2022, 12, 1288. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cirulli, N.; Inchingolo, A.D.; Patano, A.; Ceci, S.; Marinelli, G.; Malcangi, G.; Coloccia, G.; Montenegro, V.; Di Pede, C.; Ciocia, A.M.; et al. Innovative Application of Diathermy in Orthodontics: A Case Report. Int. J. Environ. Res. Public Health 2022, 19, 7448. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127448
Cirulli N, Inchingolo AD, Patano A, Ceci S, Marinelli G, Malcangi G, Coloccia G, Montenegro V, Di Pede C, Ciocia AM, et al. Innovative Application of Diathermy in Orthodontics: A Case Report. International Journal of Environmental Research and Public Health. 2022; 19(12):7448. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127448
Chicago/Turabian StyleCirulli, Nunzio, Alessio Danilo Inchingolo, Assunta Patano, Sabino Ceci, Grazia Marinelli, Giuseppina Malcangi, Giovanni Coloccia, Valentina Montenegro, Chiara Di Pede, Anna Maria Ciocia, and et al. 2022. "Innovative Application of Diathermy in Orthodontics: A Case Report" International Journal of Environmental Research and Public Health 19, no. 12: 7448. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19127448