
The Role of Pain Inflexibility and Acceptance among Headache and Temporomandibular Disorders Patients

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Procedures
2.3. Data Analysis
3. Results
3.1. Sample’s Sociodemographic and Clinical Characterization
3.2. Psychological Differences between Groups
3.3. Variables That Contribute to Explaining Psychological Inflexibility in Pain-Headache and TMD-Headache Groups
3.4. Variables That Contribute to Explaining Pain Acceptance in Headache and TMD-Headache Groups
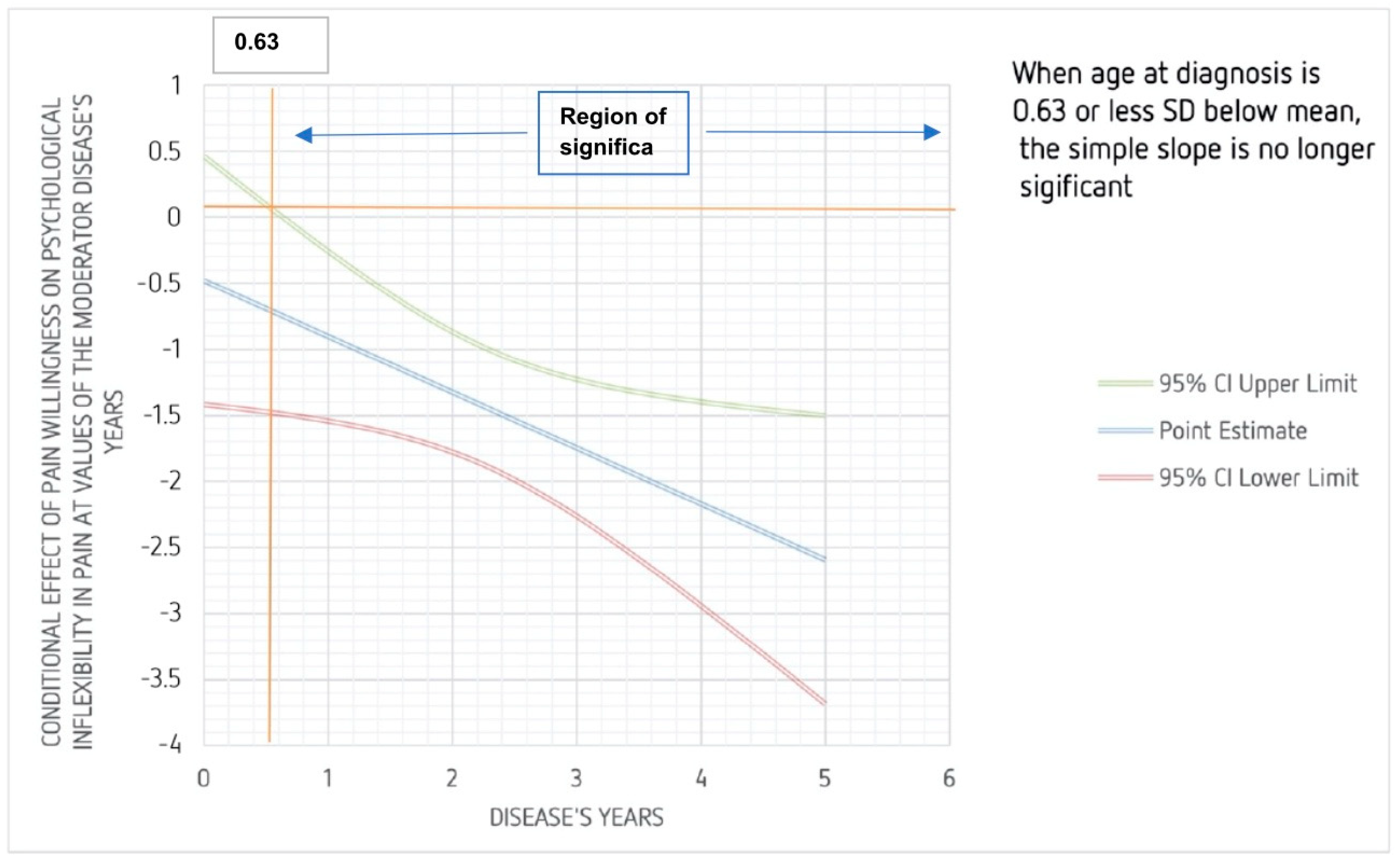
3.5. Illness Years as a Moderator between Pain Willingness and Psychological Inflexibility in Pain in Headache Group
4. Discussion
4.1. Psychological Inflexibility in Chronic Pain
4.2. Pain Triggers in the Fear-Avoidance Model
4.3. Pain Management of TMD-Headache
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Di Paolo, C.; D’Urso, A.; Papi, P.; Di Sabato, F.; Rosella, D.; Pompa, G.; Polimeni, A.; Bianchi, F.A. Temporomandibular Disorders and Headache: A Retrospective Analysis of 1198 Patients. Pain Res. Manag. 2017, 2017, 3203027. [Google Scholar] [CrossRef] [Green Version]
- Garrigós-Pedrón, M.; La Touche, R.; Navarro-Desentre, P.; Gracia-Naya, M.; Segura-Ortí, E. Effects of a Physical Therapy Protocol in Patients with Chronic Migraine and Temporomandibular Disorders: A Randomized, Single-Blinded, Clinical Trial. J. Oral Facial Pain Headache 2018, 32, 137–150. [Google Scholar] [CrossRef] [Green Version]
- Ciancaglini, R.; Radaelli, G. The Relationship between Headache and Symptoms of Temporomandibular Disorder in the General Population. J. Dent. 2001, 29, 93–98. [Google Scholar] [CrossRef]
- Fernandes, G.; Arruda, M.A.; Bigal, M.E.; Camparis, C.M.; Gonçalves, D.A.G. Painful Temporomandibular Disorder Is Associated with Migraine in Adolescents: A Case-Control Study. J. Pain 2019, 20, 1155–1163. [Google Scholar] [CrossRef]
- List, T.; Jensen, R.H. Temporomandibular Disorders: Old Ideas and New Concepts. Cephalalgia 2017, 37, 692–704. [Google Scholar] [CrossRef] [Green Version]
- Speciali, J.G.; Dach, F. Temporomandibular Dysfunction and Headache Disorder. Headache J. Head Face Pain 2015, 55, 72–83. [Google Scholar] [CrossRef]
- Sampaio, P.G.G.; Maracajá, H.D.; Figueiredo, S.R.N.; Figueiredo, V.G.N.; Temoteo, T.C.M.; Melo, N.M.A. de Sociodemographic Characteristics of Patients with Chronic Headache. Headache Med. 2020, 11, 22–24. [Google Scholar] [CrossRef]
- Deuschl, G.; Beghi, E.; Fazekas, F.; Varga, T.; Christoforidi, K.A.; Sipido, E.; Bassetti, C.L.; Vos, T.; Feigin, V.L. The Burden of Neurological Diseases in Europe: An Analysis for the Global Burden of Disease Study 2017. Lancet Public Health 2020, 5, e551–e567. [Google Scholar] [CrossRef]
- Shaefer, J.R.; Khawaja, S.N.; Bavia, P.F. Sex, Gender, and Orofacial Pain. Dent. Clin. N. Am. 2018, 62, 665–682. [Google Scholar] [CrossRef]
- Franco, A.L.; Gonçalves, D.A.G.; Castanharo, S.M.; Speciali, J.G.; Bigal, M.E.; Camparis, C.M. Migraine Is the Most Prevalent Primary Headache in Individuals with Temporomandibular Disorders. J. Orofac. Pain 2010, 24, 287–292. [Google Scholar]
- Conti, P.C.R.; Costa, Y.M.; Gonçalves, D.A.; Svensson, P. Headaches and Myofascial Temporomandibular Disorders: Overlapping Entities, Separate Managements? J. Oral Rehabil. 2016, 43, 702–715. [Google Scholar] [CrossRef] [PubMed]
- Dubner, R.; Harper, D.E.; Schrepf, A.; Clauw, D.J. Pain Mechanisms and Centralized Pain in Temporomandibular Disorders. J. Dent. Res. 2016, 95, 1102–1108. [Google Scholar] [CrossRef] [Green Version]
- Conti, P.C.R. Disfunções Temporomandibulares e Dores Orofaciais: Aplicação Clínica Das Evidências Científicas; Dental Press: Maringá, Brazil, 2021; ISBN 978-65-86395-02-0. [Google Scholar]
- Porporatti, A.L.; Costa, Y.M.; Conti, P.C.R.; Bonjardim, L.R.; Calderon, P. dos S. Primary Headaches Interfere with the Efficacy of Temporomandibular Disorders Management. J. Appl. Oral Sci. 2015, 23, 129–134. [Google Scholar] [CrossRef] [Green Version]
- Gonc, D.A.G.; Camparis, C.M.; Speciali, J.G.; Franco, A.L.; Castanharo, S.M.; Bigal, M.E. Temporomandibular Disorders Are Differentially Associated with Headache Diagnoses. Headache J. Head Face Pain 2011, 27, 611–615. [Google Scholar]
- Romero-Reyes, M.; Uyanik, J.M. Orofacial Pain Management: Current Perspectives. J. Pain Res. 2014, 7, 99–115. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.R.; Dworkin, R.H.; Sullivan, M.D.; Turk, D.C.; Wasan, A.D. The Role of Psychosocial Processes in the Development and Maintenance of Chronic Pain. J. Pain 2016, 17, T70–T92. [Google Scholar] [CrossRef] [Green Version]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.L.; Fuchs, P.N.; Turk, D.C. The Biopsychosocial Approach to Chronic Pain: Scientific Advances and Future Directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Turk, D.C.; Okifuji, A. Psychological Factors in Chronic Pain: Evolution and Revolution. J. Consult. Clin. Psychol. 2002, 70, 678–690. [Google Scholar] [CrossRef]
- Fillingim, R.B.; Ohrbach, R.; Greenspan, J.D.; Knott, C.; Dubner, R.; Bair, E.; Baraian, C.; Slade, G.D.; Maixner, W. Potential Psychosocial Risk Factors for Chronic TMD: Descriptive Data and Empirically Identified Domains from the OPPERA Case-Control Study. J. Pain 2011, 12, T46–T60. [Google Scholar] [CrossRef] [Green Version]
- Harkness, E.F.; Macfarlane, G.J.; Nahit, E.; Silman, A.J.; McBeth, J. Mechanical Injury and Psychosocial Factors in the Work Place Predict the Onset of Widespread Body Pain: A Two-Year Prospective Study among Cohorts of Newly Employed Workers. Arthritis Rheum. 2004, 50, 1655–1664. [Google Scholar] [CrossRef]
- Linton, S.J. A Review of Psychological Risk Factors in Back and Neck Pain. Spine 2000, 25, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Gil-Martínez, A.; Grande-Alonso, M.; López-de-Uralde-Villanueva, I.; López-López, A.; Fernández-Carnero, J.; La Touche, R. Chronic Temporomandibular Disorders: Disability, Pain Intensity and Fear of Movement. J. Headache Pain 2016, 17, 103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCracken, L.M.; Vowles, K.E. Acceptance of Chronic Pain. Curr. Pain Headache Rep. 2006, 10, 90–94. [Google Scholar] [CrossRef]
- Kanzler, K.E.; Pugh, J.A.; McGeary, D.D.; Hale, W.J.; Mathias, C.W.; Kilpela, L.S.; Karns-Wright, T.E.; Robinson, P.J.; Dixon, S.A.; Bryan, C.J.; et al. Mitigating the Effect of Pain Severity on Activity and Disability in Patients with Chronic Pain: The Crucial Context of Acceptance. Pain Med. 2019, 20, 1509–1518. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Ou, M.; Xie, C.; Cheng, Q.; Chen, Y. Pain Acceptance and Its Associated Factors among Cancer Patients in Mainland China: A Cross-Sectional Study. Pain Res. Manag. 2019, 2019, 9458683. [Google Scholar] [CrossRef]
- Barke, A.; Riecke, J.; Rief, W.; Glombiewski, J.A. The Psychological Inflexibility in Pain Scale (PIPS)-Validation, Factor Structure and Comparison to the Chronic Pain Acceptance Questionnaire (CPAQ) and Other Validated Measures in German Chronic Back Pain Patients. BMC Musculoskelet. Disord. 2015, 16, 171. [Google Scholar] [CrossRef] [Green Version]
- Talaei-Khoei, M.; Fischerauer, S.F.; Lee, S.G.; Ring, D.; Vranceanu, A.M. Pain Catastrophizing Mediates the Effect of Psychological Inflexibility on Pain Intensity and Upper Extremity Physical Function in Patients with Upper Extremity Illness. Pain Pract. 2017, 17, 129–140. [Google Scholar] [CrossRef]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and Commitment Therapy: Model, Processes and Outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef] [Green Version]
- Kato, T. Effect of Psychological Inflexibility on Depressive Symptoms and Sleep Disturbance among Japanese Young Women with Chronic Pain. Int. J. Environ. Res. Public Health 2020, 17, 7426. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Faria, C.; Coutinho, F.A.; Resende, T.; Ferreira, H.; Gonçalves, M.; Gomes, R.; Gomes, D.P.J. Temporomandibular Disorders: Assessment Instruments. Version 15 May 2016. [Critérios de Diagnóstico Para Disfunção Temporomandibular: Portuguese Version September 2017]. Available online: https://buffalo.app.box.com/s/lrxz9myl5wsrkcy4l0mg7fbuuik4dp36 (accessed on 23 May 2022).
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS). The International Classification of Headache Disorders. Cephalalgia 2018, 38, 1–211. [Google Scholar] [CrossRef]
- Rovner, G.S.; Årestedt, K.; Gerdle, B.; Börsbo, B.; McCracken, L.M. Psychometric Properties of the 8-Item Chronic Pain Acceptance Questionnaire (CPAQ-8) in a Swedish Chronic Pain Cohort. J. Rehabil. Med. 2014, 46, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Cósta, J.; Gouveia, J. Aceitação da dor: Abordagem Psicométrica Do Chronic Pain Acceptance Questionnaire Numa Amostra Portuguesa Com Dor Crónica. Psicologica 2009, 23, 103–126. [Google Scholar] [CrossRef] [Green Version]
- Wicksell, R.K.; Renöfält, J.; Olsson, G.L.; Bond, F.W.; Melin, L. Avoidance and Cognitive Fusion-Central Components in Pain Related Disability? Development and Preliminary Validation of the Psychological Inflexibility in Pain Scale (PIPS). Eur. J. Pain 2008, 12, 491–500. [Google Scholar] [CrossRef]
- Galhardo, A.; Ferreirinha, C.; Massano-Cardosos, I.; Cunha, M. Psychological Inflexibility in Pain Scale–Portuguese version (PIPS-PT) (Wicksell, Lekander, Sorjonen, & Olsson, 2010). Master’s Thesis, University of Coimbra, Coimbra, Portuga, 2018. [Google Scholar]
- Contreras, E.F.R.; Fernandes, G.; Ongaro, P.C.J.; Campi, L.B.; Gonçalves, D.A.G. Systemic Diseases and Other Painful Conditions in Patients with Temporomandibular Disorders and Migraine. Braz. Oral Res. 2018, 32, e77. [Google Scholar] [CrossRef] [Green Version]
- Graff-Radford, S.B.; Abbott, J.J. Temporomandibular Disorders and Headache. Oral Maxillofac. Surg. Clin. N. Am. 2016, 28, 335–349. [Google Scholar] [CrossRef]
- Anderson, G.C.; John, M.T.; Ohrbach, R.; Nixdorf, D.R.; Schiffman, E.L.; Truelove, E.S.; List, T. Influence of Headache Frequency on Clinical Signs and Symptoms of TMD in Subjects with Temple Headache and TMD Pain. Pain 2011, 152, 765–771. [Google Scholar] [CrossRef] [Green Version]
- Grossi, D.B.; Lipton, R.B.; Bigal, M.E. Temporomandibular Disorders and Migraine Chronification. Curr. Pain Headache Rep. 2009, 13, 314–318. [Google Scholar] [CrossRef]
- Kreisberg, M.K. Headache as a Symptom of Craniomandibular Disorders. II: Management. Cranio 1986, 4, 219–228. [Google Scholar] [CrossRef]
- Manrriquez, S.L.; Robles, K.; Pareek, K.; Besharati, A.; Enciso, R. Reduction of Headache Intensity and Frequency with Maxillary Stabilization Splint Therapy in Patients with Temporomandibular Disorders-Headache Comorbidity: A Systematic Review and Meta-Analysis. J. Dent. Anesth. Pain Med. 2021, 21, 183–205. [Google Scholar] [CrossRef]
- Wippert, P.M.; Wiebking, C. Stress and Alterations in the Pain Matrix: A Biopsychosocial Perspective on Back Pain and Its Prevention and Treatment. Int. J. Environ. Res. Public Health 2018, 15, 785. [Google Scholar] [CrossRef] [Green Version]
- Costa, Y.; Porporatti, A.; Stuginski-Barbosa, J.; Bonjardim, L.; Speciali, J.; Conti, P. Headache Attributed to Masticatory Myofascial Pain: Clinical Features and Management Outcomes. J. Oral Facial Pain Headache 2015, 29, 323–330. [Google Scholar] [CrossRef]
- Scher, A.I.; Stewart, W.F.; Lipton, R.B. The Comorbidity of Headache with Other Pain Syndromes. Headache J. Head Face Pain 2006, 46, 1416–1423. [Google Scholar] [CrossRef]
- da Silva Júnior, A.A.; Brandão, K.V.; Faleiros, B.E.; Tavares, R.M.; Lara, R.P.; Januzzi, E.; de Carvalho, A.B.; de Carvalho, E.M.D.; Gomes, J.B.L.; Leite, F.M.G.; et al. Temporo-Mandibular Disorders Are an Important Comorbidity of Migraine and May Be Clinically Difficult to Distinguish Them from Tension-Type Headache. Arq. Neuropsiquiatr. 2014, 72, 99–103. [Google Scholar] [CrossRef] [Green Version]
- Häggman-Henrikson, B.; Liv, P.; Ilgunas, A.; Visscher, C.M.; Lobbezoo, F.; Durham, J.; Lövgren, A. Increasing Gender Differences in the Prevalence and Chronification of Orofacial Pain in the Population. Pain 2020, 161, 1768–1775. [Google Scholar] [CrossRef]
- Eriksen, J.; Jensen, M.K.; Sjøgren, P.; Ekholm, O.; Rasmussen, N.K. Epidemiology of Chronic Non-Malignant Pain in Denmark. Pain 2003, 106, 221–228. [Google Scholar] [CrossRef]
- Azevedo, L.F.; Costa-Pereira, A.; Mendonça, L.; Dias, C.C.; Castro-Lopes, J.M. Epidemiology of Chronic Pain: A Population-Based Nationwide Study on Its Prevalence, Characteristics and Associated Disability in Portugal. J. Pain 2012, 13, 773–783. [Google Scholar] [CrossRef]
- Mills, S.E.E.; Nicolson, K.P.; Smith, B.H. Chronic Pain: A Review of Its Epidemiology and Associated Factors in Population-Based Studies. Br. J. Anaesth. 2019, 123, e273–e283. [Google Scholar] [CrossRef]
- Sener, S.; Akgunlu, F. Sociodemographic Comparison in Patients with Subjective and Objective Clinical Findings of Temporomandibular Dysfunctions. Eur. J. Dent. 2011, 5, 380–386. [Google Scholar] [CrossRef] [Green Version]
- Bartley, E.J.; Fillingim, R.B. Sex Differences in Pain: A Brief Review of Clinical and Experimental Findings. Br. J. Anaesth. 2013, 111, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Phillips, J.M.; Gatchel, R.J.; Wesley, A.L.; Ellis, E.; Penn, E.H. Clinical Implications of Sex in Acute Temporomandibular Disorders. J. Am. Dent. Assoc. 2001, 132, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Warren, M.P.; Fried, J.L. Temporomandibular Disorders and Hormones in Women. Cells Tissues Organs 2001, 169, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Meints, S.M.; Edwards, R.R. Evaluating Psychosocial Contributions to Chronic Pain Outcomes. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 87, 168–182. [Google Scholar] [CrossRef] [PubMed]
- Gillborg, S.; Åkerman, S.; Lundegren, N.; Ekberg, E. Temporomandibular Disorder Pain and Related Factors in an Adult Population: A Cross-Sectional Study in Southern Sweden. J. Oral Facial Pain Headache 2017, 31, 37–45. [Google Scholar] [CrossRef]
- Jordan, K.P.; Thomas, E.; Peat, G.; Wilkie, R.; Croft, P. Social Risks for Disabling Pain in Older People: A Prospective Study of Individual and Area Characteristics. Pain 2008, 137, 652–661. [Google Scholar] [CrossRef]
- Ferreira, I.R.; Silva, P.L.N.D.; Oliveira, E.D.; Alves, C.D.R.; Bonfim, M.D.L.C.; Nobre, M.C.D.O. Autopercepção de Saúde Bucal Por Idosos Atendidos Pelo Sistema Público de Um Município de Minas Gerais. Rev. Pesqui. Cuid. Fundam. Online 2021, 13, 1290–1295. [Google Scholar] [CrossRef]
- Kalladka, M.; Young, A.; Thomas, D.; Heir, G.M.; Quek, S.Y.P.; Khan, J. The Relation of Temporomandibular Disorders and Dental Occlusion: A Narrative Review. Quintessence Int. 2022, 53, 450–459. [Google Scholar] [CrossRef]
- Bitencourt, S.B.; de Oliveira Cunha, A.I.; da Silva, E.V.F.; Jardim, A.T.B. Análise Da Associação Entre Oclusão e Disfunção Temporomandibular: Estudo Clínico. Arch. Health Investig. 2018, 7, 269–273. [Google Scholar] [CrossRef] [Green Version]
- Palareti, G.; Legnani, C.; Cosmi, B.; Antonucci, E.; Erba, N.; Poli, D.; Testa, S.; Tosetto, A. Comparison between Different D-Dimer Cutoff Values to Assess the Individual Risk of Recurrent Venous Thromboembolism: Analysis of Results Obtained in the DULCIS Study. Int. J. Lab. Hematol. 2016, 38, 42–49. [Google Scholar] [CrossRef]
- Dominick, C.H.; Blyth, F.M.; Nicholas, M.K. Unpacking the Burden: Understanding the Relationships between Chronic Pain and Comorbidity in the General Population. Pain 2012, 153, 293–304. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of Multimorbidity and Implications for Health Care, Research, and Medical Education: A Cross-Sectional Study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Wicksell, R.K.; Lekander, M.; Sorjonen, K.; Olsson, G.L. The Psychological Inflexibility in Pain Scale (PIPS)-Statistical Properties and Model Fit of an Instrument to Assess Change Processes in Pain Related Disability. Eur. J. Pain 2010, 14, 771.e1–771.e14. [Google Scholar] [CrossRef] [PubMed]
- Gil-Martínez, A.; Navarro-Fernández, G.; Mangas-Guijarro, M.Á.; Lara-Lara, M.; López-López, A.; Fernández-Carnero, J.; La Touche, R. Comparison between Chronic Migraine and Temporomandibular Disorders in Pain-Related Disability and Fear-Avoidance Behaviors. Pain Med. 2017, 18, 2214–2223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kashdan, T.B.; Rottenberg, J. Psychological Flexibility as a Fundamental Aspect of Health. Clin. Psychol. Rev. 2010, 30, 865–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasiliou, V.S.; Karademas, E.C.; Christou, Y.; Papacostas, S.; Karekla, M. Acceptance and Commitment Therapy for Primary Headache Sufferers: A Randomized Controlled Trial of Efficacy. J. Pain 2021, 22, 143–160. [Google Scholar] [CrossRef]
- Emshoff, R.; Bertram, F.; Schnabl, D.; Emshoff, I. Association between Chronic Tension-Type Headache Coexistent with Chronic Temporomandibular Disorder Pain and Limitations in Physical and Emotional Functioning: A Case-Control Study. J. Oral Facial Pain Headache 2017, 31, 55–60. [Google Scholar] [CrossRef]
- Gonçalves, D.A.G.; Bigal, M.E.; Jales, L.C.F.; Camparis, C.M.; Speciali, J.G. Headache and Symptoms of Temporomandibular Disorder: An Epidemiological Study: Research Submission. Headache J. Head Face Pain 2010, 50, 231–241. [Google Scholar] [CrossRef]
- Hoffmann, J.; Baca, S.M.; Akerman, S. Neurovascular Mechanisms of Migraine and Cluster Headache. J. Cereb. Blood Flow Metab. 2019, 39, 573–594. [Google Scholar] [CrossRef]
- Lillis, J.; Graham Thomas, J.; Lipton, R.B.; Rathier, L.; Roth, J.; Pavlovic, J.; O’Leary, K.C.; Bond, D.S. The Association of Changes in Pain Acceptance and Headache-Related Disability. Ann. Behav. Med. 2019, 53, 686–690. [Google Scholar] [CrossRef]
- Turner, D.P.; Houle, T.T. Influences on Headache Trigger Beliefs and Perceptions. Cephalalgia 2018, 38, 1545–1553. [Google Scholar] [CrossRef]
- Martin, P.R.; MacLeod, C. Behavioral Management of Headache Triggers: Avoidance of Triggers Is an Inadequate Strategy. Clin. Psychol. Rev. 2009, 29, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Black, A.K.; Fulwiler, J.C.; Smitherman, T.A. The Role of Fear of Pain in Headache. Headache J. Head Face Pain 2015, 55, 669–679. [Google Scholar] [CrossRef] [PubMed]
- Leeuw, M.; Goossens, M.E.J.B.; Linton, S.J.; Crombez, G.; Boersma, K.; Vlaeyen, J.W.S. The Fear-Avoidance Model of Musculoskeletal Pain: Current State of Scientific Evidence. J. Behav. Med. 2007, 30, 77–94. [Google Scholar] [CrossRef] [Green Version]
- Crombez, G.; Vlaeyen, J.W.S.; Heuts, P.H.T.G.; Lysens, R. Pain-Related Fear Is More Disabling than Pain Itself: Evidence on the Role of Pain-Related Fear in Chronic Back Pain Disability. Pain 1999, 80, 329–339. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Linton, S.J. Fear-Avoidance and Its Consequences in Chronic Musculoskeletal Pain: A State of the Art. Pain 2000, 85, 317–332. [Google Scholar] [CrossRef] [Green Version]
- Norton, P.J.; Asmundson, G.J.G. Anxiety Sensitivity, Fear, and Avoidance Behavior in Headache Pain. Pain 2004, 111, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Ocañez, K.L.; Kathryn McHugh, R.; Otto, M.W. A Meta-Analytic Review of the Association between Anxiety Sensitivity and Pain. Depress. Anxiety 2010, 27, 760–767. [Google Scholar] [CrossRef]
- Gonçalves, M.C.; Florencio, L.L.; Chaves, T.C.; Speciali, J.G.; Bigal, M.E.; Bevilaqua-Grossi, D. Do Women with Migraine Have Higher Prevalence of Temporomandibular Disorders? Braz. J. Phys. Ther. 2013, 17, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, D.A.G.; Camparis, C.M.; Franco, A.L.; Fernandes, G.; Speciali, J.G.; Bigal, M.E. How to Investigate and Treat: Migraine in Patients with Temporomandibular Disorders. Curr. Pain Headache Rep. 2012, 16, 359–364. [Google Scholar] [CrossRef]
- Ohrbach, R.; Dworkin, S.F. The Evolution of TMD Diagnosis: Past, Present, Future. J. Dent. Res. 2016, 95, 1093–1101. [Google Scholar]
- Durham, J. Summary of Royal College of Surgeons’(England) Clinical Guidelines on Management of Temporomandibular Disorders in Primary Care. Br. Dent. J. 2015, 218, 355–356. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, A.C.; Duarte Moura, D.M.; Da Silva, L.G.D.; De Almeida, E.O.; Barbosa, G.A.S. Acupuncture in Temporomandibular Disorder Myofascial Pain Treatment: A Systematic Review. J. Oral Facial Pain Headache 2017, 31, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Garbelotti, T.O.; Turci, A.M.; Serigato, J.M.V.; Pizzol, K.E.D.C.; Franco-Micheloni, A.L. Effectiveness of Acupuncture for Temporomandibular Disorders and Associated Symptoms. Rev. Dor 2016, 17, 223–227. [Google Scholar] [CrossRef]
- Garrigós-Pedrón, M.; Elizagaray-García, I.; Domínguez-Gordillo, A.A.; Del-Castillo-Pardo-de-Vera, J.L.; Gil-Martínez, A. Temporomandibular Disorders: Improving Outcomes Using a Multidisciplinary Approach. J. Multidiscip. Healthc. 2019, 12, 733–747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wicksell, R.K.; Kemani, M.; Jensen, K.; Kosek, E.; Kadetoff, D.; Sorjonen, K.; Ingvar, M.; Olsson, G.L. Acceptance and Commitment Therapy for Fibromyalgia: A Randomized Controlled Trial. Eur. J. Pain 2013, 17, 599–611. [Google Scholar] [CrossRef]
- Grazzi, L.; Bernstein, C.; Raggi, A.; Sansone, E.; Grignani, E.; Searl, M.; Rizzoli, P. ACT for Migraine: Effect of Acceptance and Commitment Therapy (ACT) for High-Frequency Episodic Migraine without Aura: Preliminary Data of a Phase-Ii, Multicentric, Randomized, Open-Label Study. Neurol. Sci. 2019, 40, 191–192. [Google Scholar] [CrossRef]
- Thilander, B.; Rubio, G.; Pena, L.; De Mayorga, C. Prevalence of Temporomandibular Dysfunction and Its Association with Malocclusion in Children and Adolescents: An Epidemiologic Study Related to Specified Stages of Dental Development. Angle Orthod. 2002, 72, 146–154. [Google Scholar] [CrossRef]
- Mohlin, B.O.; Derweduwen, K.; Pilley, R.; Kingdon, A.; Shaw, W.C.; Kenealy, P. Malocclusion and Temporomandibular Disorder: A Comparison of Adolescents with Moderate to Severe Dysfunction with Those without Signs and Symptoms of Temporomandibular Disorder and Their Further Development to 30 Years of Age. Angle Orthod. 2004, 74, 319–327. [Google Scholar]
- Magnusson, T.; Egermark, I.; Carlsson, G.E. A Prospective Investigation over Two Decades on Signs and Symptoms of Temporomandibular Disorders and Associated Variables. A Final Summary. Acta Odontol. Scand. 2005, 63, 99–109. [Google Scholar] [CrossRef]
- Stone, J.C.; Hannah, A.; Nagar, N. Dental Occlusion and Temporomandibular Disorders. Evid. Based. Dent. 2017, 18, 86–87. [Google Scholar] [CrossRef]
- Sartoretto, S.C.; Bello, Y.D.; Bona, A.D.; Azevedo, M.S. Evidências Científicas Para o Diagnóstico e Tratamento Da DTM e a Relação Com a Oclusão e a Ortodontia. Rev. Fac. Odontol. UPF 2012, 17. [Google Scholar] [CrossRef]


{kind=link}
| Total | Control | Headaches | TMD-Headache | Differences | ||||
|---|---|---|---|---|---|---|---|---|
| Sociodemographic Variables | n (%) | n (%) | n (%) | n (%) | χ2 | p | φ | |
| Sample | 120 (100.0) | 25 (20.83) | 61 (50.83) | 34 (28.33) | ||||
| Gender | Female | 80 (66.7) | 13 (52.0) | 40 (65.6) | 27 (79.4) | 4.94 | 0.085 | 0.20 |
| Male | 40 (33.3) | 12 (48.0) | 21 (34.4) | 7 (20.6) | ||||
| Marital status | No relation | 49 (40.8) | 9 (36.0) | 27 (44.3) | 13 (38.2) | 0.63 | 0.728 | 0.07 |
| In a relation | 71 (59.2) | 16 (64.0) | 34 (55.7) | 21 (61.8) | ||||
| Education | Without university studies | 78 (65.0) | 17 (68.0) | 40 (65.6) | 21 (61.8) | 0.264 | 0.876 | 0.05 |
| With university studies | 42 (35.0) | 8 (32.0) | 21 (34.4) | 13 (38.2) | ||||
| F | p | η2 | ||||||
| Age | M ± SD; Min–Max | 46.89 ± 16.64; 10–89 | 52.00 ± 19.12; 18–89 | 45.92 ± 15.70; 10–72 | 44.88 ± 16.09; 15–71 | 1.54 | 0.218 | 0.03 |
| Clinical variables | χ2 | p | φ | |||||
| Systemic disease | No | 57 (47.5) | 9 (36.0) | 32 (52.5) | 16 (47.1) | 1.93 | 0.381 | 0.13 |
| Yes | 63 (52.5) | 16 (64.0) | 29 (47.5) | 18 (52.9) | ||||
| Medication | No | 40 (33.3) | 7 (28.0) | 25 (41.0) | 8 (23.5) | 3.40 | 0.183 | 0.17 |
| Yes | 80 (66.7) | 18 (72.0) | 36 (59.0) | 26 (76.5) | ||||
| Headaches | No | 22 (18.3) | 21 (84.0) | 1 (1.6) | 0 (0.0) | 90.99 | <0.001 | 0.87 |
| Yes | 98 (81.7) | 4 (16.0) | 60 (98.4) | 34 (100.0) | ||||
| Attendance to doctor | Not applicable | 22 (18.3) | 21 (84.0) | 1 (1.6) | 0 (0.0) | 91.01 | <0.001 | 0.87 |
| No | 43 (35.8) | 2 (8.0) | 26 (42.6) | 15 (44.1) | ||||
| Yes | 55 (45.8) | 2 (8.0) | 34 (55.7) | 19 (55.9) | ||||
| Illness duration | Not applicable | 31 (25.8) | 21 (84.0) | 4 (6.6) | 6 (17.6) | 63.29 | <0.001 | 0.73 |
| ≤20 years | 62 (51.7) | 3 (12.0) | 35 (57.4) | 24 (70.6) | ||||
| >20 years | 27 (22.5) | 1 (4.0) | 22 (36.1) | 4 (11.8) | ||||
| Headaches and Anxiety/Stress/Nervousness | Not applicable | 31 (25.8) | 21 (84.0) | 10 (16.4) | 0 (0.0) | 59.70 | <0.001 | 0.71 |
| No | 54 (45.0) | 2 (8.0) | 33 (54.1) | 19 (55.9) | ||||
| Yes | 35 (29.2) | 2 (8.0) | 18 (29.5) | 15 (44.1) | ||||
| Family with headache | Not applicable | 9 (7.5) | 8 (32.0) | 1 (1.6) | 0 (0.0) | 28.40 | <0.001 | 0.49 |
| No | 12 (10.0) | 2 (8.0) | 5 (8.2) | 5 (14.7) | ||||
| Yes | 99 (82.5) | 15 (60.0) | 55 (90.2) | 29 (85.3) | ||||
| Pain severity | Not applicable | 23 (19.2) | 21 (84.0) | 2 (3.2) | 0 (0.0) | 87.75 | <0.001 | 0.86 |
| Light | 37 (30.8) | 0 (0.0) | 24 (39.3) | 13 (38.2) | ||||
| Moderate | 28 (23.3) | 3 (12.0) | 17 (27.9) | 8 (23.5) | ||||
| Severe | 32 (26.7) | 1 (4.0) | 18 (29.5) | 13 (38.2) | ||||
| F | p | η2 | ||||||
| Pain intensity | M ± SD; Min–Max | 5.82 ± 3.45; 0–10 | 1.24 ± 2.96; 0–10 | 7.10 ± 2.34; 0–10 | 6.91 ± 2.54; 2–10 | 51.79 | <0.001 | 0.47 |
| χ2 | p | φ | ||||||
| Pain frequency | Not permanent | 32 (27.7) | 21 (84.0) | 7 (11.5) | 4 (11.8) | 53.08 | <0.001 | 0.67 |
| Permanent | 88 (73.3) | 4 (16.0) | 54 (88.5) | 30 (88.2) | ||||
| F | p | η2 | ||||||
| Pain years | M ± SD; Min–Max | 21.22 ± 16.61; 0–60 | 21.50 ± 24.34; 0–60 | 21.38 ± 15.92; 1–55 | 20.91 ± 17.44; 0–60 | 0.01 | 0.991 | 0.00 |
| χ2 | p | φ | ||||||
| Medical exam | Not applicable | 22 (18.3) | 21 (84.0) | 1 (1.6) | 0 (0.0) | 91.07 | <0.001 | 0.87 |
| No | 68 (56,7) | 3 (12.0) | 41 (67.2) | 24 (70.6) | ||||
| Yes | 30 (25.0) | 1 (4.0) | 19 (31.1) | 10 (29.4) | ||||
| Previous treatment | Not applicable | 22 (18.3) | 21 (84.0) | 1 (1.6) | 0 (0.0) | 91.31 | <0.001 | 0.87 |
| No | 21 (17.5) | 0 (0) | 13 (21.3) | 8 (23.5) | ||||
| Yes | 67 (64.2) | 4 (16.0) | 47 (77.1) | 26 (76.5) | ||||
| Preventive treatment | Not applicable | 22 (18.3) | 21 (84.0) | 1 (1.6) | 0 (18.3) | 91.01 | <0.001 | 0.87 |
| No | 78 (65.0) | 3 (12.0) | 48 (78.7) | 27 (79.4) | ||||
| Yes | 20 (16.7) | 1 (4.0) | 12 (19.7) | 7 (20.6) | ||||
| Visual changes | Not applicable | 22 (18.3) | 21 (84.0) | 1 (1.6) | 0 (0.0) | 91.06 | <0.001 | 0.87 |
| No | 56 (46.7) | 2 (8.0) | 34 (55.7) | 20 (58.8) | ||||
| Yes | 42 (35.0) | 2 (8.0) | 26 (42.6) | 14 (41.2) | ||||
| Sensitive changes | Not applicable | 22 (18.3) | 21 (84.0) | 1 (1.6) | 0 (0.0) | 91.58 | <0.001 | 0.87 |
| No | 90 (75.0) | 3 (12.0) | 55 (90.2) | 32 (94.1) | ||||
| Yes | 8 (6.7) | 1 (4.0) | 5 (8.2) | 2 (5.6) | ||||
| Motor changes | Not applicable | 22 (18.3) | 21 (84.0) | 1 (1.6) | 0 (0.0) | 91.30 | <0.001 | 0.87 |
| No | 91 (75.8) | 4 (16.0) | 55 (90.2) | 32 (94.1) | ||||
| Yes | 7 (5.8) | 0 (0) | 5 (8.2) | 2 (5.6) | ||||
| Anxiety/nervousness causes headaches | Not applicable | 21 (17.5) | 20 (80.0) | 1 (1.6) | 0 (17.5) | 85.69 | <0.001 | 0.85 |
| No | 46 (38.6) | 2 (8.0) | 29 (47.5) | 15 (44.1) | ||||
| Yes | 53 (44.2) | 3 (12.0) | 31 (50.8) | 19 (55.9) | ||||
| Anxiety/nervousness aggravates headaches | Not applicable | 21 (17.5) | 20 (80.0) | 1 (1.6) | 0 (17.5) | 93.37 | <0.001 | 0.88 |
| No | 58 (56.7) | 3 (12.0) | 47 (77.0) | 18 (52.9) | ||||
| Yes | 31 (25.8) | 2 (8.0) | 13 (21.3) | 16 (47.1) | ||||
| Headache diagnosis | No | 25 (20.8) | 25 (100.0) | 0 (00.0) | 0 (0.0) | 120.00 | <0.001 | 1.00 |
| Yes | 95 (79.2) | 0 (0.0) | 61 (100.0) | 34 (100.0) | ||||
| Total | Control | Headache | TMD-Headache | Differences | |||
|---|---|---|---|---|---|---|---|
| M (SD) | M (SD) | M (SD) | M (SD) | F | p | η2 | |
| Psychological Inflexibility in Pain Scale (PIPS) Total | 35.86 (12.18) | 30.72 (20.16) 1 | 32.10 (12.23) 2 | 46.38 (18.51) 1,2 | 6.43 | 0.002 | 0.10 |
| PIPS Avoidance of Pain | 20.08 (13.43) | 17.32 (12.96) 1 | 18.11 (12.77) 2 | 25.62 (13.68) 1,2 | 4.30 | 0.016 | 0.07 |
| PIPS Pain Cognitive Fusion | 15.78 (9.22) | 13.40 (8.42) 1 | 13.98 (9.52) 2 | 20.76 (7.36) 1,2 | 7.76 | 0.001 | 0.12 |
| Chronic Pain Acceptance Questionnaire (CPAQ) Total | 25.35 (5.69) | 24.96 (3.51) | 25.34 (6.57) | 25.65 (5.40) | 0.10 | 0.902 | 0.00 |
| CPAQ Activity Engagement | 14.12 (9.42) | 13.56 (10.68) | 13.03 (9.78) | 16.47 (7.39) | 1.52 | 0.222 | 0.03 |
| CPAQ Pain Willingness | 11.23 (9.09) | 11.40 (10.19) | 12.31 (9.41) | 9.18 (7.40) | 1.31 | 0.273 | 0.02 |
| Variables | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| B | SE B | ß | B | SE B | ß | |
| Pain intensity | 4.33 | 1.04 | 0.48 | 3.55 | 0.84 | 0.39 |
| Pain willingness | −1.23 | 0.21 | −0.55 | |||
| R2(R2Aj.) | 0.23 (0.21) | 0.52 (0.50) | ||||
| F for change in R2 | 17.31 *** | 35.05 *** | ||||
| Variables | Model 1 | ||
|---|---|---|---|
| B | SE B | ß | |
| Pain intensity | 3.82 | 1.02 | 0.52 |
| Anxiety/nervousness that causes headache | 10.94 | 5.11 | 0.30 |
| R2(R2Aj.) | 0.47 (0.44) | ||
| F for change in R2 | 13.84 *** | ||
| Variables | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| B | SE B | ß | B | SE B | ß | |
| Gender (Male) | −3.25 | 1.76 | −0.24 | −5.78 | 1.69 | −0.42 |
| Systemic disease | −4.89 | 1.50 | −0.37 | |||
| Pain severity | −2.22 | 0.83 | −0.31 | |||
| Pain frequency | 5.87 | 2.68 | 0.28 | |||
| Illness duration | 0.10 | 0.05 | 0.24 | |||
| Sensitive changes | 4.12 | 1.62 | 0.31 | |||
| R2(R2Aj.) | 0.06 (0.04) | 0.35 (0.28) | ||||
| F for change in R2 | 3.42 (ns) | 4.83 ** | ||||
| Variables | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| B | SE B | ß | B | SE B | ß | |
| Gender (Female) | 2.65 | 2.20 | 0.20 | 5.44 | 2.23 | 0.41 |
| Education | 0.67 | 0.39 | 0.29 | 0.81 | 0.35 | 0.35 |
| Family with headache | −5.73 | 2.62 | −0.38 | |||
| Pain frequency | −5.26 | 2.54 | −2.07 | |||
| Motor changes | −8.43 | 3.59 | −0.37 | |||
| R2(R2Aj.) | 0.13 (0.07) | 0.38 (0.27) | ||||
| F for change in R2 | 2.30 (ns) | 3.77 * | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcelino, V.; Paço, M.; Dias, A.; Almeida, V.; Rocha, J.C.; Azevedo, R.; Alves-Ferreira, M.; Lemos, C.; Pinho, T. The Role of Pain Inflexibility and Acceptance among Headache and Temporomandibular Disorders Patients. Int. J. Environ. Res. Public Health 2022, 19, 7974. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19137974
Marcelino V, Paço M, Dias A, Almeida V, Rocha JC, Azevedo R, Alves-Ferreira M, Lemos C, Pinho T. The Role of Pain Inflexibility and Acceptance among Headache and Temporomandibular Disorders Patients. International Journal of Environmental Research and Public Health. 2022; 19(13):7974. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19137974
Chicago/Turabian StyleMarcelino, Vanessa, Maria Paço, Andreia Dias, Vera Almeida, José Carlos Rocha, Rui Azevedo, Miguel Alves-Ferreira, Carolina Lemos, and Teresa Pinho. 2022. "The Role of Pain Inflexibility and Acceptance among Headache and Temporomandibular Disorders Patients" International Journal of Environmental Research and Public Health 19, no. 13: 7974. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19137974