
Serum Cholesterol Levels and Risk of Cardiovascular Death: A Systematic Review and a Dose-Response Meta-Analysis of Prospective Cohort Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Selection Criteria
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
3.1. Literature Search
3.2. Study Characteristics
3.3. Total Cholesterol
High versus Low
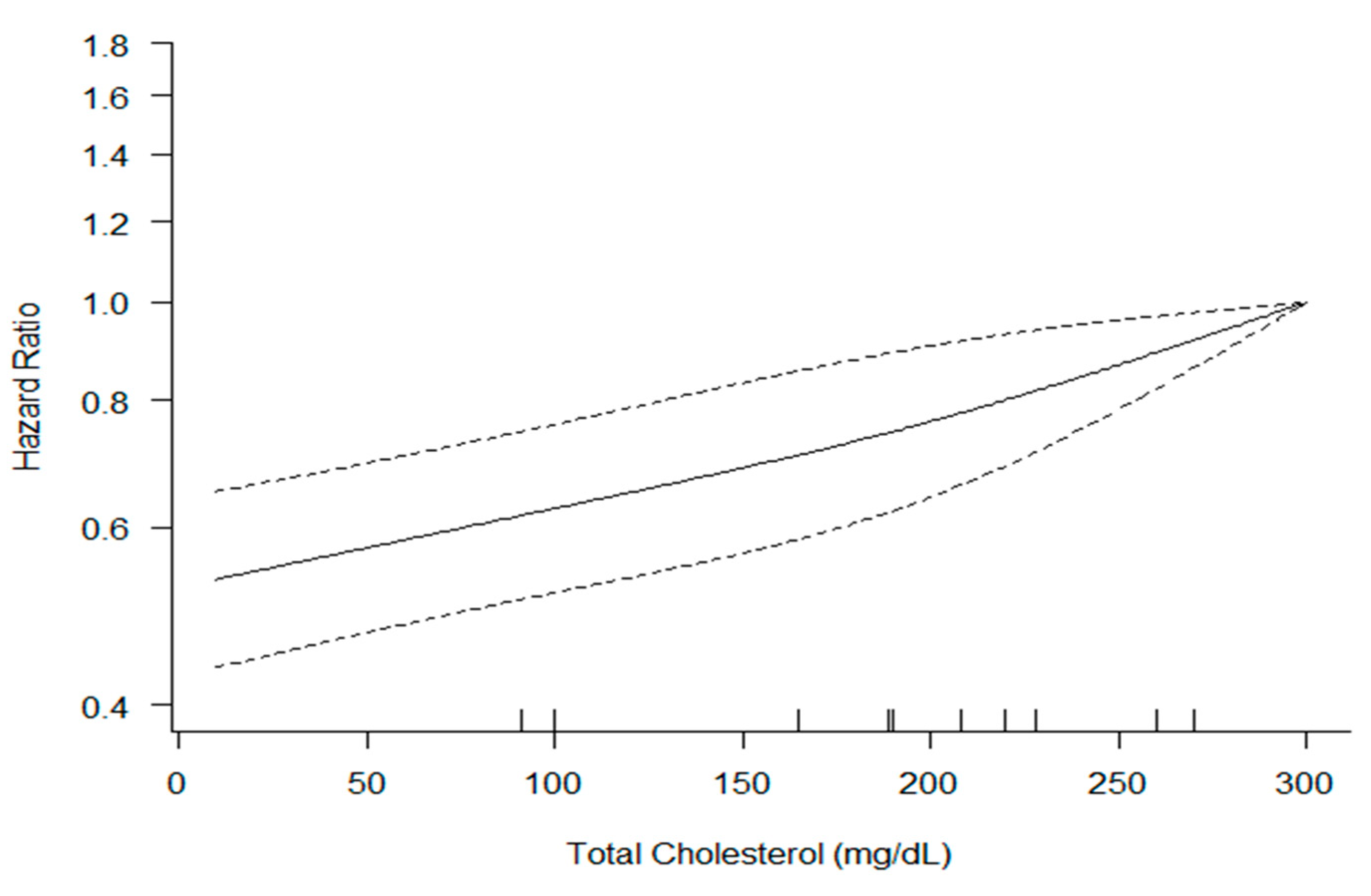
3.4. Dose-Response Analysis
3.5. High-Density Lipoprotein Cholesterol
High versus Low
3.6. Dose-Response Analysis
3.7. Low-Density Lipoprotein Cholesterol
High versus Low
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 385, 117–171.
- Institute of Medicine Committee on Preventing the Global Epidemic of Cardiovascular Disease: Meeting the Challenges in Developing Countries. The National Academies Collection: Reports funded by National Institutes of Health. In Promoting Cardiovascular Health in the Developing World: A Critical Challenge to Achieve Global Health; Fuster, V., Kelly, B.B., Eds.; National Academies Press (US): Washington, DC, USA, 2010. [Google Scholar]
- Casula, M.; Colpani, O.; Xie, S.; Alberico, L.; Baragetti, A. HDL in Atherosclerotic Cardiovascular Disease: In Search of a Role. Cells 2021, 10, 1869. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Stamler, J.; Daviglus, M.L.; Garside, D.B.; Dyer, A.R.; Greenland, P.; Neaton, J.D. Relationship of baseline serum cholesterol levels in 3 large cohorts of younger men to long-term coronary, cardiovascular, and all-cause mortality and to longevity. JAMA 2000, 284, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Gofman, J.W.; Glazier, F.; Tamplin, A.; Strisower, B.; De Lalla, O. Lipoproteins, coronary heart disease, and atherosclerosis. Physiol. Rev. 1954, 34, 589–607. [Google Scholar] [CrossRef]
- Steinberg, D. The LDL modification hypothesis of atherogenesis: An update. J. Lipid Res. 2009, 50, S376–S381. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.W.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of coronary heart disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [Green Version]
- Gordon, T.; Castelli, W.P.; Hjortland, M.C.; Kannel, W.B.; Dawber, T.R. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am. J. Med. 1977, 62, 707–714. [Google Scholar] [CrossRef]
- Knobloch, K.; Yoon, U.; Vogt, P.M. Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement and publication bias. J. Craniomaxillofacial Surg. 2011, 39, 91–92. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sackett, D.L. Bias in analytic research. J. Chronic Dis. 1979, 32, 51–63. [Google Scholar] [CrossRef]
- Greenland, S.; Longnecker, M.P. Methods for trend estimation from summarized dose-response data, with applications to meta-analysis. Am. J. Epidemiol. 1992, 135, 1301–1309. [Google Scholar] [CrossRef] [PubMed]
- Orsini, N.; Bellocco, R.; Greenland, S. Generalized least squares for trend estimation of summarized dose-response data. Stata J. 2006, 6, 40. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Sedgwick, P.; Marston, L. How to read a funnel plot in a meta-analysis. BMJ 2015, 351, h4718. [Google Scholar] [CrossRef]
- Stewart, L.A.; Clarke, M.; Rovers, M.; Riley, R.D.; Simmonds, M.; Stewart, G.; Tierney, J.F. Preferred Reporting Items for Systematic Review and Meta-Analyses of individual participant data: The PRISMA-IPD Statement. JAMA 2015, 313, 1657–1665. [Google Scholar] [CrossRef]
- Hirata, A.; Okamura, T.; Sugiyama, D.; Kuwabara, K.; Kadota, A.; Fujiyoshi, A.; Miura, K.; Okuda, N.; Ohkubo, T.; Okayama, A.; et al. The Relationship between Very High Levels of Serum High-Density Lipoprotein Cholesterol and Cause-Specific Mortality in a 20-Year Follow-Up Study of Japanese General Population. J. Atheroscler. Thromb. 2016, 23, 800–809. [Google Scholar] [CrossRef] [Green Version]
- Hirata, A.; Sugiyama, D.; Watanabe, M.; Tamakoshi, A.; Iso, H.; Kotani, K.; Kiyama, M.; Yamada, M.; Ishikawa, S.; Murakami, Y.; et al. Association of extremely high levels of high-density lipoprotein cholesterol with cardiovascular mortality in a pooled analysis of 9 cohort studies including 43,407 individuals: The EPOCH-JAPAN study. J. Clin. Lipidol. 2018, 12, 674–684.e675. [Google Scholar] [CrossRef]
- Okamura, T.; Hayakawa, T.; Kadowaki, T.; Kita, Y.; Okayama, A.; Ueshima, H. The inverse relationship between serum high-density lipoprotein cholesterol level and all-cause mortality in a 9.6-year follow-up study in the Japanese general population. Atherosclerosis 2006, 184, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Satoh, M.; Ohkubo, T.; Asayama, K.; Murakami, Y.; Sakurai, M.; Nakagawa, H.; Iso, H.; Okayama, A.; Miura, K.; Imai, Y.; et al. Combined effect of blood pressure and total cholesterol levels on long-term risks of subtypes of cardiovascular death: Evidence for Cardiovascular Prevention from Observational Cohorts in Japan. Hypertension 2015, 65, 517–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilander, L.; Berglund, L.; Boberg, M.; Vessby, B.; Lithell, H. Education, lifestyle factors and mortality from cardiovascular disease and cancer. A 25-year follow-up of Swedish 50-year-old men. Int. J. Epidemiol. 2001, 30, 1119–1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johan, S.; Zethelrus, U.; Byberg, L.; Zethelius, B.; Lithell, H.; Lind, L. Clinical value of the metabolic syndrome for long term prediction of total and cardiovascular mortality: Prospective, population based cohort study. BMJ 2006, 332, 878–882. [Google Scholar] [CrossRef] [Green Version]
- Kunutsor, S.K.; Zaccardi, F.; Karppi, J.; Kurl, S.; Laukkanen, J.A. Is High Serum LDL/HDL Cholesterol Ratio an Emerging Risk Factor for Sudden Cardiac Death? Findings from the KIHD Study. J. Atheroscler. Thromb. 2017, 24, 600–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oksala, N.; Seppala, I.; Hernesniemi, J.; Lyytikainen, L.P.; Kahonen, M.; Makela, K.M.; Reunanen, A.; Jula, A.; Ala-Korpela, M.; Lehtimaki, T. Complementary prediction of cardiovascular events by estimated apo- and lipoprotein concentrations in the working age population. The Health 2000 Study. Ann. Med. 2013, 45, 141–148. [Google Scholar] [CrossRef]
- Holme, I. Association of coronary heart disease mortality with risk factors according to length of follow-up and serum cholesterol level in men: The Oslo Study cohort. Eur. J. Prev. Cardiol. 2011, 20, 168–175. [Google Scholar] [CrossRef]
- Silbernagel, G.; Schottker, B.; Appelbaum, S.; Scharnagl, H.; Kleber, M.E.; Grammer, T.B.; Ritsch, A.; Mons, U.; Holleczek, B.; Goliasch, G.; et al. High-density lipoprotein cholesterol, coronary artery disease, and cardiovascular mortality. Eur. Heart J. 2013, 34, 3563–3571. [Google Scholar] [CrossRef] [Green Version]
- Tikhonoff, V.; Casiglia, E.; Mazza, A.; Scarpa, R.; Thijs, L.; Pessina, A.C.; Staessen, J.A. Low-density lipoprotein cholesterol and mortality in older people. J. Am. Geriatr. Soc. 2005, 53, 2159–2164. [Google Scholar] [CrossRef]
- Hu, W.S.; Lee, J.H.; Tsai, M.K.; Wen, C.P. A novel cardiovascular death prediction model for Chinese individuals: A prospective cohort study of 381,963 study participants. Atherosclerosis 2017, 264, 19–28. [Google Scholar] [CrossRef]
- Thorgeirsson, G.; Thorgeirsson, G.; Sigvaldason, H.; Witteman, J. Risk factors for out-of-hospital cardiac arrest: The Reykjavik Study. Eur. Heart J. 2005, 26, 1499–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harari, G.; Green, M.S.; Magid, A.; Zelber-Sagi, S. Usefulness of Non-High-Density Lipoprotein Cholesterol as a Predictor of Cardiovascular Disease Mortality in Men in 22-Year Follow-Up. Am. J. Cardiol. 2017, 119, 1193–1198. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldstein, J.L.; Brown, M.S. A century of cholesterol and coronaries: From plaques to genes to statins. Cell 2015, 161, 161–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewington, S.; Whitlock, G.; Clarke, R.; Sherliker, P.; Emberson, J.; Halsey, J.; Qizilbash, N.; Peto, R.; Collins, R. Blood cholesterol and vascular mortality by age, sex, and blood pressure: A meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet 2007, 370, 1829–1839. [Google Scholar] [CrossRef] [PubMed]
- Leppala, J.M.; Virtamo, J.; Fogelholm, R.; Albanes, D.; Heinonen, O.P. Different risk factors for different stroke subtypes: Association of blood pressure, cholesterol, and antioxidants. Stroke 1999, 30, 2535–2540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahar, E.; Chambless, L.E.; Rosamond, W.D.; Boland, L.L.; Ballantyne, C.M.; McGovern, P.G.; Sharrett, A.R. Plasma lipid profile and incident ischemic stroke: The Atherosclerosis Risk in Communities (ARIC) study. Stroke 2003, 34, 623–631. [Google Scholar] [CrossRef] [Green Version]
- Ravnskov, U. High cholesterol may protect against infections and atherosclerosis. QJM 2003, 96, 927–934. [Google Scholar] [CrossRef]
- Ulmer, H.; Kelleher, C.; Diem, G.; Concin, H. Why Eve is not Adam: Prospective follow-up in 149650 women and men of cholesterol and other risk factors related to cardiovascular and all-cause mortality. J. Women’s Health 2004, 13, 41–53. [Google Scholar] [CrossRef]
- Hecht, H.S.; Superko, H.R. Electron beam tomography and National Cholesterol Education Program guidelines in asymptomatic women. J. Am. Coll. Cardiol. 2001, 37, 1506–1511. [Google Scholar] [CrossRef] [Green Version]
- Ravnskov, U. Is atherosclerosis caused by high cholesterol? QJM 2002, 95, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Kastelein, J.J.; Boekholdt, S.M.; Nicholls, S.J.; Khaw, K.T.; Ballantyne, C.M.; Catapano, A.L.; Reiner, Z.; Luscher, T.F. The ACC/AHA 2013 guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular disease risk in adults: The good the bad and the uncertain: A comparison with ESC/EAS guidelines for the management of dyslipidaemias 2011. Eur. Heart J. 2014, 35, 960–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brugts, J.; Yetgin, T.; Hoeks, S.; Gotto, A.; Shepherd, J.; Westendorp, R.; De Craen, A.; Knopp, R.; Nakamura, H.; Ridker, P. The benefits of statins in people without established cardiovascular disease but with cardiovascular risk factors: Meta-analysis of randomised controlled trials. BMJ 2009, 338, b2376. [Google Scholar] [CrossRef] [Green Version]
- Taylor, F.; Ward, K.; Moore, T.H.; Burke, M.; Davey Smith, G.; Casas, J.P.; Ebrahim, S. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2011, Cd004816. [Google Scholar] [CrossRef] [Green Version]
- Pignone, M.; Phillips, C.; Mulrow, C. Use of lipid lowering drugs for primary prevention of coronary heart disease: Meta-analysis of randomised trials. BMJ 2000, 321, 983–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kannel, W.B.; Dawber, T.R.; Friedman, G.D.; Glennon, W.E.; McNamara, P.M. Risk factors in coronary heart disease: An evaluation of several serum lipids as predictors of coronary heart disease: The framingham study. Ann. Intern. Med. 1964, 61, 888–899. [Google Scholar] [CrossRef] [PubMed]
- Di Angelantonio, E.; Gao, P.; Pennells, L.; Kaptoge, S.; Caslake, M.; Thompson, A.; Butterworth, A.S.; Sarwar, N.; Wormser, D.; Saleheen, D.; et al. Lipid-related markers and cardiovascular disease prediction. JAMA 2012, 307, 2499–2506. [Google Scholar] [CrossRef] [Green Version]
- Lu, Q.; Tian, G.; Zhang, Y.; Lu, M.; Lin, X.; Ma, A. Low HDL-C predicts risk and PCI outcomes in the Han Chinese population. Atherosclerosis 2013, 226, 193–197. [Google Scholar] [CrossRef]
- Rubin, E.M.; Krauss, R.M.; Spangler, E.A.; Verstuyft, J.G.; Clift, S.M. Inhibition of early atherogenesis in transgenic mice by human apolipoprotein AI. Nature 1991, 353, 265–267. [Google Scholar] [CrossRef]
- Tangirala, R.K.; Tsukamoto, K.; Chun, S.H.; Usher, D.; Pure, E.; Rader, D.J. Regression of atherosclerosis induced by liver-directed gene transfer of apolipoprotein A-I in mice. Circulation 1999, 100, 1816–1822. [Google Scholar] [CrossRef] [Green Version]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riley, R.D.; Higgins, J.P.; Deeks, J.J. Interpretation of random effects meta-analyses. BMJ 2011, 342, d549. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Author, Year) | Country | Duration of Follow-Up (Years) | Age (Years) | Total N (Cases) | Setting | Clinical Endpoints | Effect Size (HR, 95% CI) |
|---|---|---|---|---|---|---|---|
| Ingar Holme (2011) [28] | Norway | 33 | 45 | 14,846 (1655) | Oslo study | CHD mortality | <TC>: 1.24 (1.19–1.29) |
| Johan S (2006) [25] | Sweden | 32.7 | 50 70 | 2841 (1078) 168 (302) | Uppsala County | CVD mortality | <TC> age 50: 1.16 (1.07–1.26) age 70: 0.96 (0.80–1.16) |
| Michihiro. S (2015) [23] | Japan | 15 | 56.9 | 73,916 (770) | EPOCH-JAPAN group | CHD mortality | <TC>: 1.26 (1.16–1.34) |
| Nicu Oksala (2012) [27] | Finland | 7.8 | 30–65 | 5956 (55) | Health 2000 survey | SCD | <TC>: 1.29 (0.89–1.88) <LDL>: 1.28 (0.97–1.70) <HDL>: 0.65 (0.47–0.91) |
| Kilander. L (2001) [24] | Sweden | 25.7 | 50 | 2301 (301) | CVD mortality | <TC>: 1.27 (1.15–1.41) | |
| Silbernagel. G (2013) [29] | Germany | 8.9 | 62.6 | 3141 (590) | LURIC study | CVD mortality | <HDL>: 0.37 (0.18–0.74) |
| Tomonori. O (2005) [22] | Japan | 9.6 | 52.8 | 7175 (174) | The Nippon General DATA 90 research group | CVD mortality | <HDL>: 0.27 (0.14–0.52) |
| Kunutsor. S. K (2017) [26] | Finland | 23 | 42–61 | 2616 (228) | KIHD risk factor study | Sudden death | <LDL>: 1.43 (0.93–2.19) <HDL>: 0.52 (0.34–0.78) |
| Tikhonoff. V (2005) [30] | Italy | 12 | 73.8 | 3120 (327) | CVD mortality | <LDL>: 1.06 (0.94–1.18) | |
| Wei-Syun. H (2017) [31] | Taiwan | 8.8 | Over 20 | 381,963 (1894) | The MJ health group | CVD mortality | <TC>: 1.68 (1.38–2.04) |
| Thorgeirsson. G (2005) [32] | Iceland | 25 | M: 66.8 W: 65.8 | 8806 (137) 9435 (44) | The Reykjavik study | CVD mortality | <TC> M: 1.41 (1.21–1.63) W: 1.42 (1.14–1.76) |
| Gil Harari (2017) [33] | Israel | 22 | 42.1 | 4832 (172) | CORDIS | CVD mortality | <TC>: 3.58 (2.49–5.14) <LDL>: 1.82 (1.15–2.89) <HDL>: 0.90 (0.51–1.59) |
| Aya Hirata (2016) [20] | Japan | 18 | 52.5 | 7019 (450) | NIPPON DATA study | CVD mortality | <HDL>: 0.64 (0.42–0.96) |
| Aya Hirata (2018) [21] | Japan | 12.1 | 57.1 | 525,661 (1280) | EPOCH-JAPAN group | CVD mortality | <HDL>: 0.56 (0.39–0.82) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, E.; Kong, S.Y.; Ro, Y.S.; Ryu, H.H.; Shin, S.D. Serum Cholesterol Levels and Risk of Cardiovascular Death: A Systematic Review and a Dose-Response Meta-Analysis of Prospective Cohort Studies. Int. J. Environ. Res. Public Health 2022, 19, 8272. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19148272
Jung E, Kong SY, Ro YS, Ryu HH, Shin SD. Serum Cholesterol Levels and Risk of Cardiovascular Death: A Systematic Review and a Dose-Response Meta-Analysis of Prospective Cohort Studies. International Journal of Environmental Research and Public Health. 2022; 19(14):8272. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19148272
Chicago/Turabian StyleJung, Eujene, So Yeon Kong, Young Sun Ro, Hyun Ho Ryu, and Sang Do Shin. 2022. "Serum Cholesterol Levels and Risk of Cardiovascular Death: A Systematic Review and a Dose-Response Meta-Analysis of Prospective Cohort Studies" International Journal of Environmental Research and Public Health 19, no. 14: 8272. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19148272