
A Literature Review of High-Tech Physiotherapy Interventions in the Elderly with Neurological Disorders




Abstract
:1. Introduction
2. Physiotherapy Interventions in the Elderly with NDs
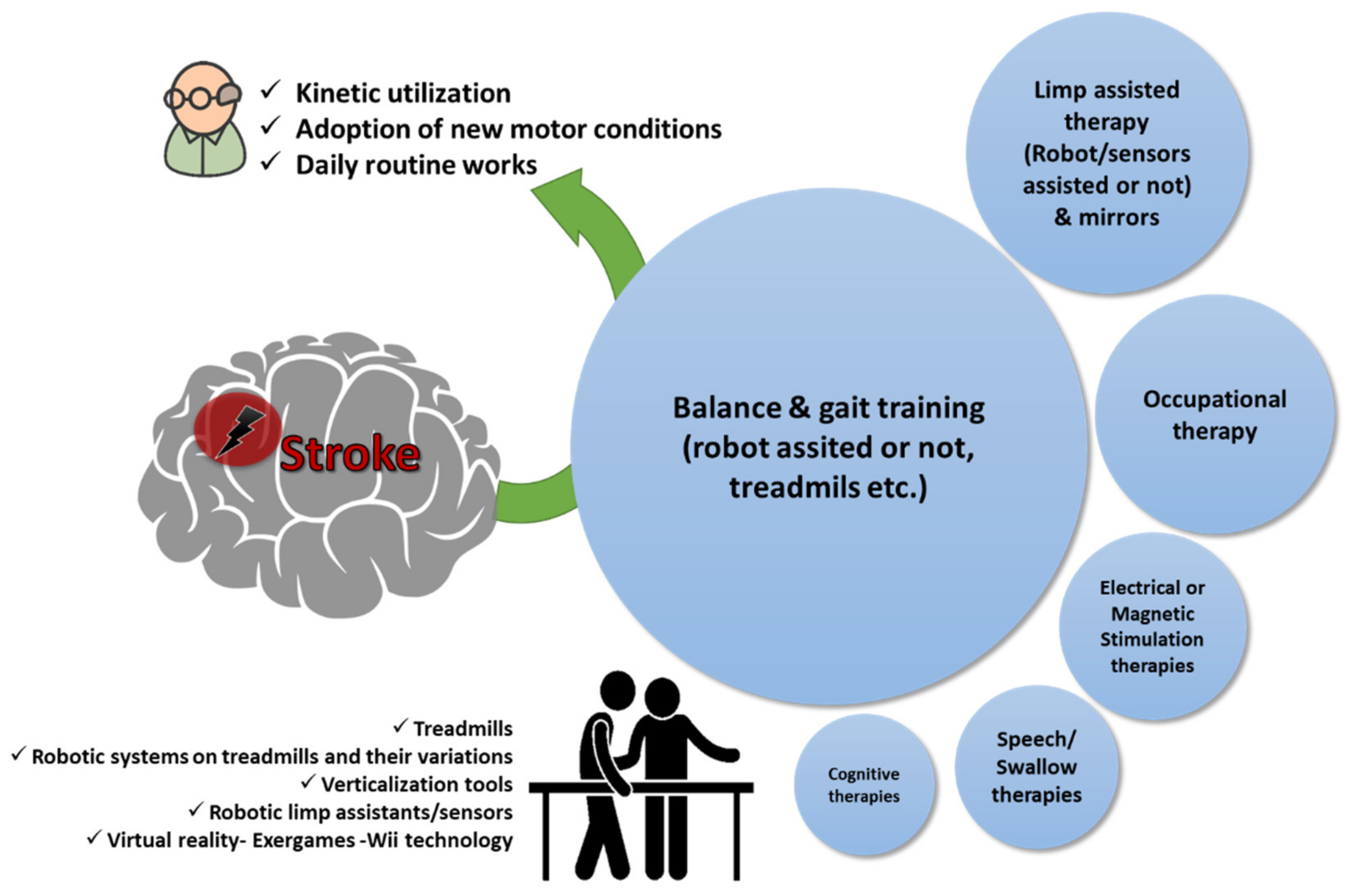
2.1. Stroke
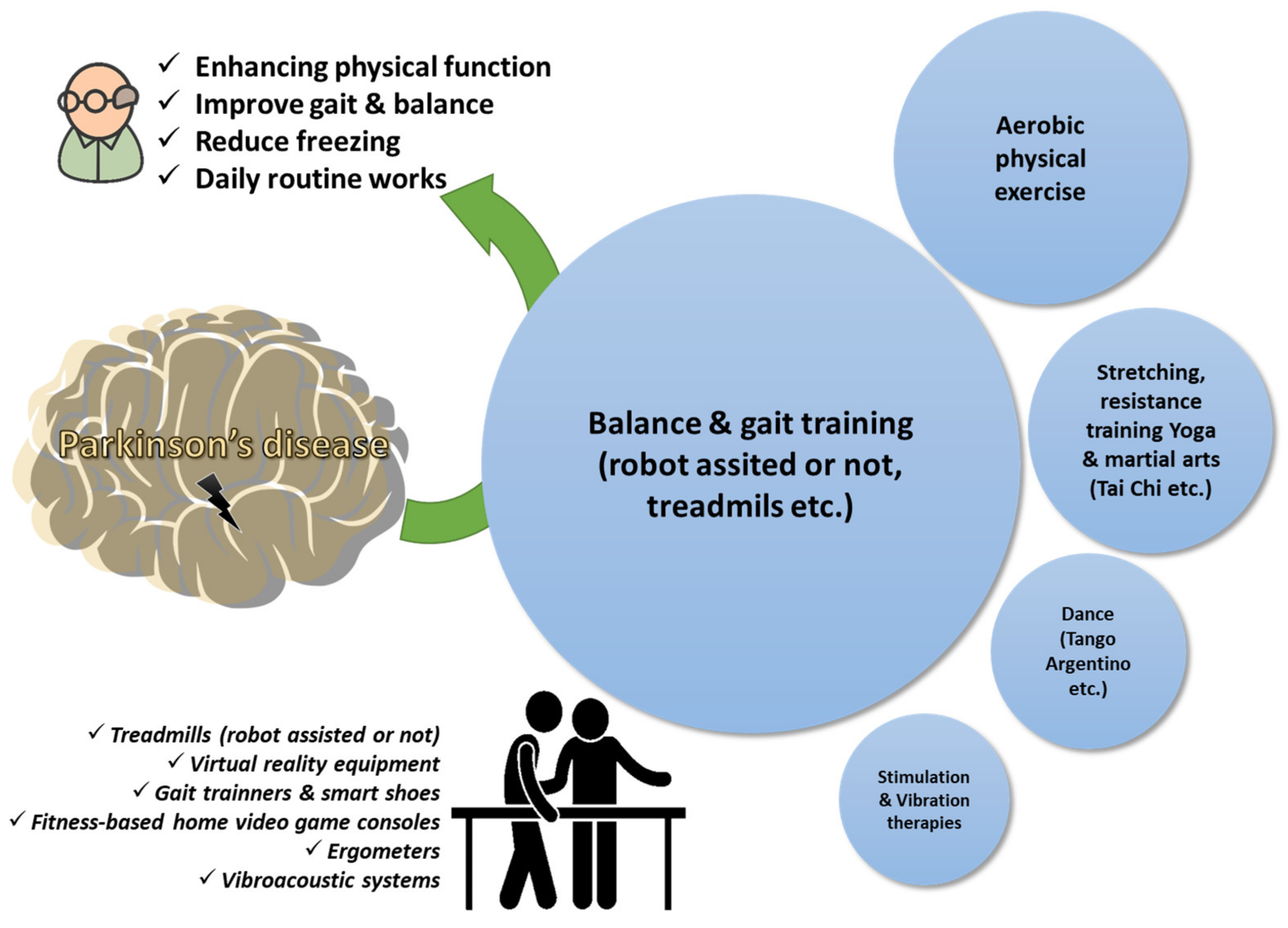
2.2. Parkinson’s Disease
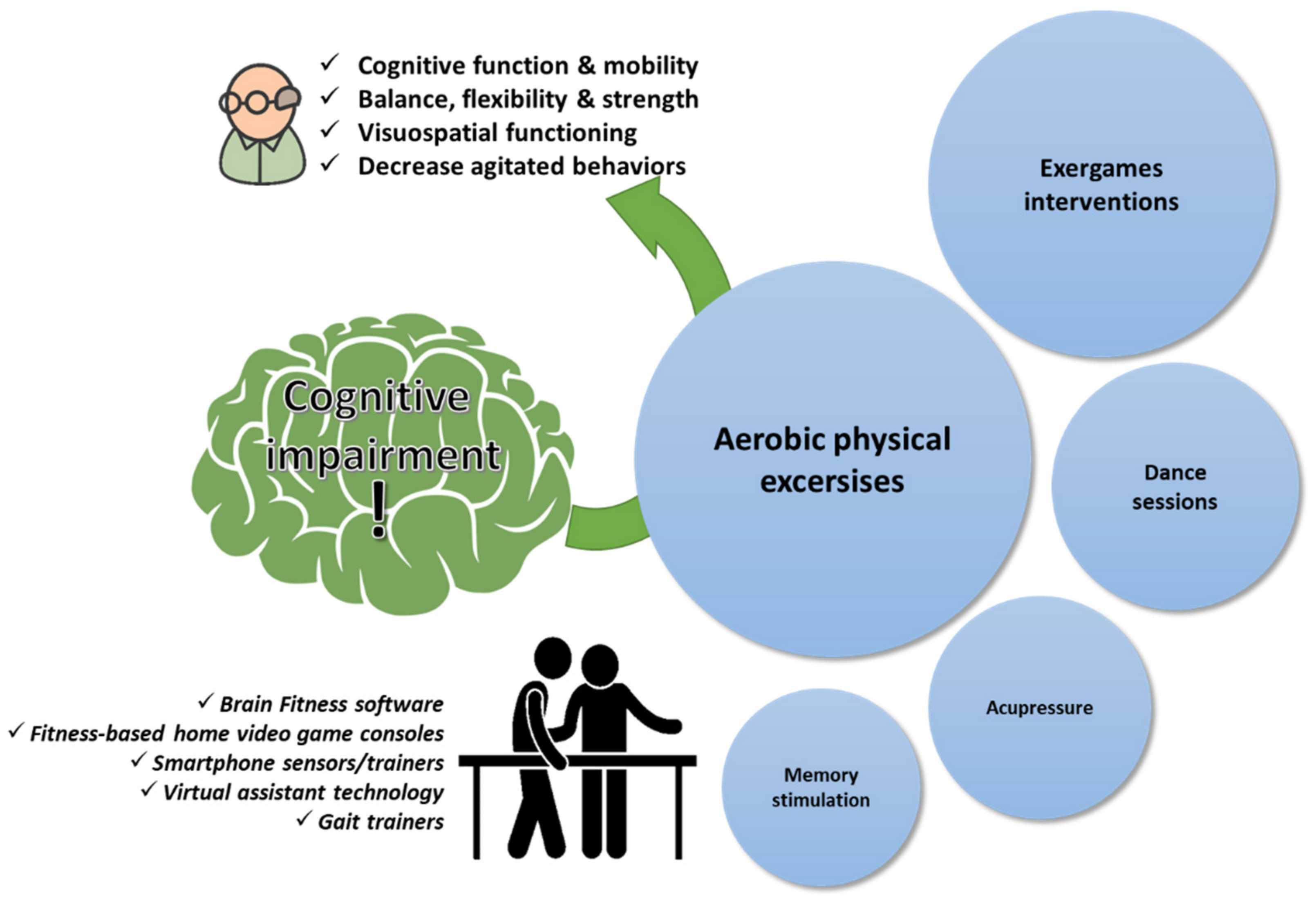
2.3. Age-Related Cognitive Impairment
2.4. Other Types of NDs
3. Discussion
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Han, E.S.; Lee, Y.; Kim, J. Association of cognitive impairment with frailty in community-dwelling older adults. Int. Psychogeriatr. 2014, 26, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Campbell, A.J.; Robertson, M.C.; Gardner, M.M.; Norton, R.N.; Tilyard, M.W.; Buchner, D.M. Randomised controlled trial of a general practice programme of home based exercise to prevent falls in elderly women. BMJ 1997, 315, 1065–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irez, G.B.; Ozdemir, R.A.; Evin, R.; Irez, S.G.; Korkusuz, F. Integrating Pilates Exercise into an Exercise Program for 65+ Year-Old Women to Reduce Falls. J. Sports Sci. Med. 2011, 10, 105. [Google Scholar] [PubMed]
- Wu, C.Y.; Chou, Y.J.C.; Huang, N.; Chou, Y.J.C.; Hu, H.Y.; Li, C.P. Cognitive impairment assessed at annual geriatric health examinations predicts mortality among the elderly. Prev. Med. 2014, 67, 28–34. [Google Scholar] [CrossRef]
- Rudnicka, E.; Napierała, P.; Podfigurna, A.; Męczekalski, B.; Smolarczyk, R.; Grymowicz, M. The World Health Organization (WHO) approach to healthy ageing. Maturitas 2020, 139, 6–11. [Google Scholar] [CrossRef]
- Dua, T.; Garrido-Cumbrera, M.; Mathers, C.; Saxena, S.; World Health Organization. Global Burden of Neurological Disorders: Estimates and Projections. In Neurological Disorders: Public Health Challenges; WHO Press: Geneva, Switzerland, 2006; pp. 27–39. [Google Scholar]
- Butterworth, P.; Rodgers, B.; Windsor, T.D. Financial hardship, socio-economic position and depression: Results from the PATH Through Life Survey. Soc. Sci. Med. 2009, 69, 229–237. [Google Scholar] [CrossRef]
- World Confederation for Physical Therapy. Policy Statement: Description of Physical Therapy. World Physiotherapy. 2011. Available online: https://world.physio/policy/ps-descriptionPT (accessed on 12 March 2022).
- Carter, N.D.; Kannus, P.; Khan, K.M. Exercise in the Prevention of Falls in Older People. Sports Med. 2001, 31, 427–438. [Google Scholar] [CrossRef]
- McDonald, C.M. Clinical Approach to the Diagnostic Evaluation of Hereditary and Acquired Neuromuscular Diseases. Phys. Med. Rehabil. Clin. N. Am. 2012, 23, 495–563. [Google Scholar] [CrossRef] [Green Version]
- Pinto, S.; Swash, M.; de Carvalho, M. Respiratory exercise in amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. 2012, 13, 33–43. [Google Scholar] [CrossRef]
- Anziska, Y.; Sternberg, A. Exercise in neuromuscular disease. Muscle Nerve 2013, 48, 3–20. [Google Scholar] [CrossRef]
- Gallo, J.J.; Lebowitz, B.D. The epidemiology of common late-life mental disorders in the community: Themes for the new century. Psychiatr. Serv. 1999, 50, 1158–1166. [Google Scholar] [CrossRef]
- Md Fadzil, N.H.; Shahar, S.; Rajikan, R.; Singh, D.K.A.; Mat Ludin, A.F.; Subramaniam, P.; Ibrahim, N.; Vanoh, D.; Mohamad Ali, N. A Scoping Review for Usage of Telerehabilitation among Older Adults with Mild Cognitive Impairment or Cognitive Frailty. Int. J. Environ. Res. Public Health 2022, 19, 4000. [Google Scholar] [CrossRef]
- Zak, M.; Sikorski, T.; Wasik, M.; Courteix, D.; Dutheil, F.; Brola, W. Frailty Syndrome-Fall Risk and Rehabilitation Management Aided by Virtual Reality (VR) Technology Solutions: A Narrative Review of the Current Literature. Int. J. Environ. Res. Public Health 2022, 19, 2985. [Google Scholar] [CrossRef]
- De Sire, A.; Ammendolia, A.; Invernizzi, M.; Baricich, A.; Lippi, L.; Invernizzi, M.; Grassi, F.A.; Leigheba, M. Optimization of transdisciplinary management of elderly with femur proximal extremity fracture: A patient-tailored plan from orthopaedics to rehabilitation. World J. Orthop. 2021, 12, 456–466. [Google Scholar] [CrossRef]
- De Diego, C.; Puig, S.; Navarro, X. A sensorimotor stimulation program for rehabilitation of chronic stroke patients. Restor. Neurol. Neurosci. 2013, 31, 361–371. [Google Scholar] [CrossRef]
- Duncan, P.W.; Sullivan, K.J.; Behrman, A.L.; Azen, S.P.; Wu, S.S.; Nadeau, S.E.; Dobkin, B.H.; Rose, D.K.; Tilson, J.K.; Cen, S.; et al. Body-weight-supported treadmill rehabilitation after stroke. N. Engl. J. Med. 2011, 364, 2026–2036. [Google Scholar] [CrossRef] [Green Version]
- Bergmann, J.; Krewer, C.; Bauer, P.; Koenig, A.; Riener, R.; Müller, F. Virtual reality to augment robot-assisted gait training in non-ambulatory patients with a subacute stroke: A pilot randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2018, 54, 397–407. [Google Scholar] [CrossRef]
- Taveggia, G.; Borboni, A.; Mulé, C.; Villafañe, J.H.; Negrini, S. Conflicting results of robot-assisted versus usual gait training during postacute rehabilitation of stroke patients: A randomized clinical trial. Int. J. Rehabil. Res. 2016, 39, 29–35. [Google Scholar] [CrossRef] [Green Version]
- Grecco, L.A.C.; Zanon, N.; Sampaio, L.M.M.; Oliveira, C.S. A comparison of treadmill training and overground walking in ambulant children with cerebral palsy: Randomized controlled clinical trial. Clin. Rehabil. 2013, 27, 686–696. [Google Scholar] [CrossRef]
- Tanaka, N.; Matsushita, S.; Sonoda, Y.; Maruta, Y.; Fujitaka, Y.; Sato, M.; Simomori, M.; Onaka, R.; Harada, K.; Hirata, T.; et al. Effect of Stride Management Assist Gait Training for Poststroke Hemiplegia: A Single Center, Open-Label, Randomized Controlled Trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 477–486. [Google Scholar] [CrossRef] [Green Version]
- Barbeau, H.; Visintin, M. Optimal outcomes obtained with body-weight support combined with treadmill training in stroke subjects. Arch. Phys. Med. Rehabil. 2003, 84, 1458–1465. [Google Scholar] [CrossRef]
- Dean, C.M.; Ada, L.; Bampton, J.; Morris, M.E.; Katrak, P.H.; Potts, S. Treadmill walking with body weight support in subacute non-ambulatory stroke improves walking capacity more than overground walking: A randomised trial. J. Physiother. 2010, 56, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Tinetti, M.E. Performance-Oriented Assessment of Mobility Problems in Elderly Patients. J. Am. Geriatr. Soc. 1986, 34, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Vellone, E.; Savini, S.; Barbato, N.; Carovillano, G.; Caramia, M.; Alvaro, R. Quality of life in stroke survivors: First results from the reliability and validity of the Italian version of the Stroke Impact Scale 3.0. Ann. Ig. 2010, 22, 469–479. [Google Scholar]
- Salbach, N.M.; Mayo, N.E.; Wood-Dauphinee, S.; Hanley, J.A.; Richards, C.L.; Côté, R. A task-orientated intervention enhances walking distance and speed in the first year post stroke: A randomized controlled trial. Clin. Rehabil. 2004, 18, 509–519. [Google Scholar] [CrossRef]
- Dean, C.M.; Richards, C.L.; Malouin, F. Task-related circuit training improves performance of locomotor tasks in chronic stroke: A randomized, controlled pilot trial. Arch. Phys. Med. Rehabil. 2000, 81, 409–417. [Google Scholar] [CrossRef]
- Mayo, N.E.; Mackay-Lyons, M.J.; Scott, S.C.; Moriello, C.; Brophy, J. A randomized trial of two home-based exercise programmes to improve functional walking post-stroke. Clin. Rehabil. 2013, 27, 659–671. [Google Scholar] [CrossRef]
- Thieme, H.; Bayn, M.; Wurg, M.; Zange, C.; Pohl, M.; Behrens, J. Mirror therapy for patients with severe arm paresis after stroke—A randomized controlled trial. Clin. Rehabil. 2013, 27, 314–324. [Google Scholar] [CrossRef]
- Rabadi, M.H.; Galgano, M.; Lynch, D.; Akerman, M.; Lesser, M.; Volpe, B.T. A pilot study of activity-based therapy in the arm motor recovery post stroke: A randomized controlled trial. Clin. Rehabil. 2008, 22, 1071–1082. [Google Scholar] [CrossRef]
- Langhammer, B.; Ada, L.; Gunnes, M.; Ihle-Hansen, H.; Indredavik, B.; Askim, T. A physical activity program is no more effective than standard care at maintaining upper limb activity in community-dwelling people with stroke: Secondary outcomes from a randomized trial. Clin. Rehabil. 2019, 33, 1607–1613. [Google Scholar] [CrossRef] [Green Version]
- Thielman, G.T.; Dean, C.M.; Gentile, A.M. Rehabilitation of reaching after stroke: Task-related training versus progressive resistive exercise. Arch. Phys. Med. Rehabil. 2004, 85, 1613–1618. [Google Scholar] [CrossRef]
- Hesse, S.; Waldner, A.; Mehrholz, J.; Tomelleri, C.; Pohl, M.; Werner, C. Combined transcranial direct current stimulation and robot-assisted arm training in subacute stroke patients: An exploratory, randomized multicenter trial. Neurorehabil. Neural Repair 2011, 25, 838–846. [Google Scholar] [CrossRef]
- Diserens, K.; Perret, N.; Chatelain, S.; Bashir, S.; Ruegg, D.; Vuadens, P.; Vingerhoets, F. The effect of repetitive arm cycling on post stroke spasticity and motor control: Repetitive arm cycling and spasticity. J. Neurol. Sci. 2007, 253, 18–24. [Google Scholar] [CrossRef]
- Ogino, T.; Kanata, Y.; Uegaki, R.; Yamaguchi, T.; Morisaki, K.; Nakano, S.; Domen, K. Effects of gait exercise assist robot (GEAR) on subjects with chronic stroke: A randomized controlled pilot trial. J. Stroke Cerebrovasc. Dis. 2020, 29, 104886. [Google Scholar] [CrossRef]
- Masiero, S.; Celia, A.; Rosati, G.; Armani, M. Robotic-assisted rehabilitation of the upper limb after acute stroke. Arch. Phys. Med. Rehabil. 2007, 88, 142–149. [Google Scholar] [CrossRef]
- Yavuzer, G.; Selles, R.; Sezer, N.; Sütbeyaz, S.; Bussmann, J.B.; Köseoǧlu, F.; Atay, M.B.; Stam, H.J. Mirror therapy improves hand function in subacute stroke: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2008, 89, 393–398. [Google Scholar] [CrossRef]
- Solopova, I.A.; Tihonova, D.Y.; Grishin, A.A.; Ivanenko, Y.P. Assisted leg displacements and progressive loading by a tilt table combined with FES promote gait recovery in acute stroke. NeuroRehabilitation 2011, 29, 67–77. [Google Scholar] [CrossRef]
- Fong, K.N.K.; Yang, N.Y.H.; Chan, M.K.L.; Chan, D.Y.L.; Lau, A.F.C.; Chan, D.Y.W.; Cheung, J.T.Y.; Cheung, H.K.Y.; Chung, R.C.K.; Chan, C.C.H. Combined effects of sensory cueing and limb activation on unilateral neglect in subacute left hemiplegic stroke patients: A randomized controlled pilot study. Clin. Rehabil. 2013, 27, 628–637. [Google Scholar] [CrossRef]
- Abdullah, H.A.; Tarry, C.; Lambert, C.; Barreca, S.; Allen, B.O. Results of clinicians using a therapeutic robotic system in an inpatient stroke rehabilitation unit. J. Neuroeng. Rehabil. 2011, 8, 50. [Google Scholar] [CrossRef] [Green Version]
- Rydwik, E.; Eliasson, S.; Akner, G. The effect of exercise of the affected foot in stroke patients—A randomized controlled pilot trial. Clin. Rehabil. 2006, 20, 645–655. [Google Scholar] [CrossRef]
- Tamburella, F.; Moreno, J.C.; Iosa, M.; Pisotta, I.; Cincotti, F.; Mattia, D.; Pons, J.L.; Molinari, M. Boosting the traditional physiotherapist approach for stroke spasticity using a sensorized ankle foot orthosis: A pilot study. Top. Stroke Rehabil. 2017, 24, 447–456. [Google Scholar] [CrossRef]
- Yeung, L.F.; Lau, C.C.Y.; Lai, C.W.K.; Soo, Y.O.Y.; Chan, M.L.; Tong, R.K.Y. Effects of wearable ankle robotics for stair and over-ground training on sub-acute stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 19. [Google Scholar] [CrossRef]
- Wittenberg, G.F.; Chen, R.; Ishii, K.; Bushara, K.O.; Taub, E.; Gerber, L.H.; Hallett, M.; Cohen, L.G. Constraint-induced therapy in stroke: Magnetic-stimulation motor maps and cerebral activation. Neurorehabil. Neural Repair 2003, 17, 48–57. [Google Scholar] [CrossRef]
- Daniel, L.; Howard, W.; Braun, D.; Page, S.J. Opinions of Constraint-Induced Movement Therapy among Therapists in Southwestern Ohio. Top. Stroke Rehabil. 2012, 19, 268–275. [Google Scholar] [CrossRef]
- Fleet, A.; Page, S.J.; MacKay-Lyons, M.; Boe, S. Modified Constraint-Induced Movement Therapy for Upper Extremity Recovery Post Stroke: What Is the Evidence? Top. Stroke Rehabil. 2014, 21, 319–331. [Google Scholar] [CrossRef]
- Pomeroy, V.M.; Cloud, G.; Tallis, R.C.; Donaldson, C.; Nayak, V.; Miller, S. Transcranial magnetic stimulation and muscle contraction to enhance stroke recovery: A randomized proof-of-principle and feasibility investigation. Neurorehabil. Neural Repair 2007, 21, 509–517. [Google Scholar] [CrossRef]
- Shigematsu, T.; Fujishima, I.; Ohno, K. Transcranial direct current stimulation improves swallowing function in stroke patients. Neurorehabil. Neural Repair 2013, 27, 363–369. [Google Scholar] [CrossRef]
- Sproson, L.; Pownall, S.; Enderby, P.; Freeman, J. Combined electrical stimulation and exercise for swallow rehabilitation post-stroke: A pilot randomized control trial. Int. J. Lang. Commun. Disord. 2018, 53, 405–417. [Google Scholar] [CrossRef] [Green Version]
- Au-Yeung, S.S.Y.; Hui-Chan, C.W.Y. Electrical acupoint stimulation of the affected arm in acute stroke: A placebo-controlled randomized clinical trial. Clin. Rehabil. 2014, 28, 149–158. [Google Scholar] [CrossRef]
- Dorsch, S.; Ada, L.; Canning, C.G. EMG-triggered electrical stimulation is a feasible intervention to apply to multiple arm muscles in people early after stroke, but does not improve strength and activity more than usual therapy: A randomized feasibility trial. Clin. Rehabil. 2014, 28, 482–490. [Google Scholar] [CrossRef]
- Ambrosini, E.; Parati, M.; Peri, E.; De Marchis, C.; Nava, C.; Pedrocchi, A.; Ferriero, G.; Ferrante, S. Changes in leg cycling muscle synergies after training augmented by functional electrical stimulation in subacute stroke survivors: A pilot study. J. Neuroeng. Rehabil. 2020, 17, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitsutake, T.; Sakamoto, M.; Nakazono, H.; Horikawa, E. The Effects of Combining Transcranial Direct Current Stimulation and Gait Training with Functional Electrical Stimulation on Trunk Acceleration During Walking in Patients with Subacute Stroke. J. Stroke Cerebrovasc. Dis. 2021, 30, 105635. [Google Scholar] [CrossRef] [PubMed]
- Nicolo, P.; Magnin, C.; Pedrazzini, E.; Plomp, G.; Mottaz, A.; Schnider, A.; Guggisberg, A.G. Comparison of Neuroplastic Responses to Cathodal Transcranial Direct Current Stimulation and Continuous Theta Burst Stimulation in Subacute Stroke. Arch. Phys. Med. Rehabil. 2018, 99, 862–872.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serrezuela, R.R.; Quezada, M.T.; Zayas, M.H.; Pedrón, A.M.; Hermosilla, D.M.; Zamora, R.S. Robotic therapy for the hemiplegic shoulder pain: A pilot study. J. Neuroeng. Rehabil. 2020, 17, 54. [Google Scholar] [CrossRef] [Green Version]
- Carpinella, I.; Lencioni, T.; Bowman, T.; Bertoni, R.; Turolla, A.; Ferrarin, M.; Jonsdottir, J. Effects of robot therapy on upper body kinematics and arm function in persons post stroke: A pilot randomized controlled trial. J. Neuroeng. Rehabil. 2020, 17, 10. [Google Scholar] [CrossRef] [Green Version]
- Franceschini, M.; Mazzoleni, S.; Goffredo, M.; Pournajaf, S.; Galafate, D.; Criscuolo, S.; Agosti, M.; Posteraro, F. Upper limb robot-assisted rehabilitation versus physical therapy on subacute stroke patients: A follow-up study. J. Bodyw. Mov. Ther. 2020, 24, 194–198. [Google Scholar] [CrossRef]
- Ranzani, R.; Lambercy, O.; Metzger, J.C.; Califfi, A.; Regazzi, S.; Dinacci, D.; Petrillo, C.; Rossi, P.; Conti, F.M.; Gassert, R. Neurocognitive robot-assisted rehabilitation of hand function: A randomized control trial on motor recovery in subacute stroke. J. Neuroeng. Rehabil. 2020, 17, 115. [Google Scholar] [CrossRef]
- Gueye, T.; Dedkova, M.; Rogalewicz, V.; Grunerova-Lippertova, M.; Angerova, Y. Early post-stroke rehabilitation for upper limb motor function using virtual reality and exoskeleton: Equally efficient in older patients. Neurol. Neurochir. Pol. 2021, 55, 91–96. [Google Scholar] [CrossRef]
- Kim, M.S.; Kim, S.H.; Noh, S.E.; Bang, H.J.; Lee, K.M. Robotic-Assisted Shoulder Rehabilitation Therapy Effectively Improved Poststroke Hemiplegic Shoulder Pain: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2019, 100, 1015–1022. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Russo, M.; Bramanti, P.; Carioti, L.; Balletta, T.; Buda, A.; Manuli, A.; Filoni, S.; Bramanti, A. Shaping neuroplasticity by using powered exoskeletons in patients with stroke: A randomized clinical trial. J. Neuroeng. Rehabil. 2018, 15, 35. [Google Scholar] [CrossRef]
- Peurala, S.H.; Airaksinen, O.; Huuskonen, P.; Jäkälä, P.; Juhakoski, M.; Sandell, K.; Tarkka, I.M.; Sivenius, J. Effects of intensive therapy using gait trainer or floor walking exercises early after stroke. J. Rehabil. Med. 2009, 41, 166–173. [Google Scholar] [CrossRef] [Green Version]
- Yokota, C.; Yamamoto, Y.; Kamada, M.; Nakai, M.; Nishimura, K.; Ando, D.; Sato, T.; Koga, M.; Ihara, M.; Toyoda, K.; et al. Acute stroke rehabilitation for gait training with cyborg type robot Hybrid Assistive Limb: A pilot study. J. Neurol. Sci. 2019, 404, 11–15. [Google Scholar] [CrossRef] [Green Version]
- Lam, J.M.; Globas, C.; Cerny, J.; Hertler, B.; Uludag, K.; Forrester, L.W.; MacKo, R.F.; Hanley, D.F.; Becker, C.; Luft, A.R. Predictors of response to treadmill exercise in stroke survivors. Neurorehabil. Neural Repair 2010, 24, 567–574. [Google Scholar] [CrossRef] [Green Version]
- Lo, A.C.; Guarino, P.D.; Richards, L.G.; Haselkorn, J.K.; Wittenberg, G.F.; Federman, D.G.; Ringer, R.J.; Wagner, T.H.; Krebs, H.I.; Volpe, B.T.; et al. Robot-assisted therapy for long-term upper-limb impairment after stroke. N. Engl. J. Med. 2010, 362, 1772–1783. [Google Scholar] [CrossRef] [Green Version]
- Sale, P.; Franceschini, M.; Mazzoleni, S.; Palma, E.; Agosti, M.; Posteraro, F. Effects of upper limb robot-assisted therapy on motor recovery in subacute stroke patients. J. Neuroeng. Rehabil. 2014, 11, 104. [Google Scholar] [CrossRef] [Green Version]
- Karttunen, A.H.; Kallinen, M.; Peurala, S.H.; Häkkinen, A. Walking Training and Functioning among Elderly Persons with Stroke: Results of a Prospective Cohort Study. PM&R 2015, 7, 1205–1214. [Google Scholar] [CrossRef]
- Calabrò, R.S.; Naro, A.; Russo, M.; Leo, A.; Balletta, T.; Saccá, I.; De Luca, R.; Bramanti, P. Do post-stroke patients benefit from robotic verticalization? A pilot-study focusing on a novel neurophysiological approach. Restor. Neurol. Neurosci. 2015, 33, 671–681. [Google Scholar] [CrossRef] [Green Version]
- Jeong, Y.G.; Koo, J.W. The effects of treadmill walking combined with obstacle-crossing on walking ability in ambulatory patients after stroke: A pilot randomized controlled trial. Top. Stroke Rehabil. 2016, 23, 406–412. [Google Scholar] [CrossRef]
- Seo, J.S.; Yang, H.S.; Jung, S.; Kang, C.S.; Jang, S.; Kim, D.H. Effect of reducing assistance during robot-assisted gait training on step length asymmetry in patients with hemiplegic stroke: A randomized controlled pilot trial. Medicine 2018, 97, e11792. [Google Scholar] [CrossRef]
- Meester, D.; Al-Yahya, E.; Dennis, A.; Collett, J.; Wade, D.T.; Ovington, M.; Liu, F.; Meaney, A.; Cockburn, J.; Johansen-Berg, H.; et al. A randomized controlled trial of a walking training with simultaneous cognitive demand (dual-task) in chronic stroke. Eur. J. Neurol. 2019, 26, 435–441. [Google Scholar] [CrossRef]
- Yasuda, K.; Saichi, K.; Kaibuki, N.; Harashima, H.; Iwata, H. Haptic-based perception-empathy biofeedback system for balance rehabilitation in patients with chronic stroke: Concepts and initial feasibility study. Gait Posture 2018, 62, 484–489. [Google Scholar] [CrossRef]
- Lotay, R.; Mace, M.; Rinne, P.; Burdet, E.; Bentley, P. Optimizing self-exercise scheduling in motor stroke using Challenge Point Framework theory. IEEE Int. Conf. Rehabil. Robot. 2019, 2019, 435–440. [Google Scholar] [CrossRef]
- Choi, Y.H.; Kim, N.H.; Son, S.M.; Cha, Y.J. Effects of Trunk Stabilization Exercise While Wearing a Pelvic Compression Belt on Walking and Balancing Abilities in Patients with Stroke: An Assessor Blinded, Preliminary, Randomized, Controlled Study. Am. J. Phys. Med. Rehabil. 2020, 99, 1048–1055. [Google Scholar] [CrossRef]
- Mayr, A.; Kofler, M.; Quirbach, E.; Matzak, H.; Fröhlich, K.; Saltuari, L. Prospective, blinded, randomized crossover study of gait rehabilitation in stroke patients using the Lokomat gait orthosis. Neurorehabil. Neural Repair 2007, 21, 307–314. [Google Scholar] [CrossRef]
- Lau, K.W.K.; Mak, M.K.Y. Speed-dependent treadmill training is effective to improve gait and balance performance in patients with sub-acute stroke. J. Rehabil. Med. 2011, 43, 709–713. [Google Scholar] [CrossRef] [Green Version]
- Yoshimoto, T.; Shimizu, I.; Hiroi, Y.; Kawaki, M.; Sato, D.; Nagasawa, M. Feasibility and efficacy of high-speed gait training with a voluntary driven exoskeleton robot for gait and balance dysfunction in patients with chronic stroke: Nonrandomized pilot study with concurrent control. Int. J. Rehabil. Res. 2015, 38, 338–343. [Google Scholar] [CrossRef]
- Rogers, J.M.; Duckworth, J.; Middleton, S.; Steenbergen, B.; Wilson, P.H. Elements virtual rehabilitation improves motor, cognitive, and functional outcomes in adult stroke: Evidence from a randomized controlled pilot study. J. Neuroeng. Rehabil. 2019, 16, 56. [Google Scholar] [CrossRef] [Green Version]
- Henrique, P.P.B.; Colussi, E.L.; De Marchi, A.C.B. Effects of Exergame on Patients’ Balance and Upper Limb Motor Function after Stroke: A Randomized Controlled Trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 2351–2357. [Google Scholar] [CrossRef]
- Shaughnessy, M.; Michael, K.; Resnick, B. Impact of treadmill exercise on efficacy expectations, physical activity, and stroke recovery. J. Neurosci. Nurs. 2012, 44, 27–35. [Google Scholar] [CrossRef]
- Lee, I.H. Does the speed of the treadmill influence the training effect in people learning to walk after stroke? A double-blind randomized controlled trial. Clin. Rehabil. 2015, 29, 269–276. [Google Scholar] [CrossRef]
- Rawson, K.S.; McNeely, M.E.; Duncan, R.P.; Pickett, K.A.; Perlmutter, J.S.; Earhart, G.M. Exercise and Parkinson Disease: Comparing Tango, Treadmill, and Stretching. J. Neurol. Phys. Ther. 2019, 43, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Wingham, J.; Adie, K.; Turner, D.; Schofield, C.; Pritchard, C. Participant and caregiver experience of the Nintendo Wii SportsTM after stroke: Qualitative study of the trial of WiiTM in stroke (TWIST). Clin. Rehabil. 2015, 29, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Unibaso-Markaida, I.; Iraurgi, I.; Ortiz-Marqués, N.; Amayra, I.; Martínez-Rodríguez, S. Effect of the Wii Sports Resort on the improvement in attention, processing speed and working memory in moderate stroke. J. Neuroeng. Rehabil. 2019, 16, 32. [Google Scholar] [CrossRef] [PubMed]
- Hely, M.A.; Morris, J.G.L.; Reid, W.G.J.; Trafficante, R. Sydney multicenter study of Parkinson’s disease: Non-L-dopa–responsive problems dominate at 15 years. Mov. Disord. 2005, 20, 190–199. [Google Scholar] [CrossRef]
- Schrag, A.; Jahanshahi, M.; Quinn, N. How does Parkinson’s disease affect quality of life? A comparison with quality of life in the general population. Mov. Disord. 2000, 15, 1112–1118. [Google Scholar] [CrossRef]
- Ahlskog, J.E. Does vigorous exercise have a neuroprotective effect in Parkinson disease? Neurology 2011, 77, 288–294. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.L.; Patel, S.; Meek, C.; Herd, C.P.; Clarke, C.E.; Stowe, R.; Shah, L.; Sackley, C.M.; Deane, K.H.O.; Wheatley, K.; et al. Physiotherapy versus placebo or no intervention in Parkinson’s disease. Cochrane Database Syst. Rev. 2013, 2013, CD002817. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.L.; Patel, S.; Meek, C.; Herd, C.P.; Clarke, C.E.; Stowe, R.; Shah, L.; Sackley, C.; Deane, K.H.O.; Wheatley, K.; et al. Physiotherapy intervention in Parkinson’s disease: Systematic review and meta-analysis. BMJ 2012, 345, e5004. [Google Scholar] [CrossRef] [Green Version]
- Picelli, A.; Melotti, C.; Origano, F.; Waldner, A.; Gimigliano, R.; Smania, N. Does robotic gait training improve balance in Parkinson’s disease? A randomized controlled trial. Parkinsonism Relat. Disord. 2012, 18, 990–993. [Google Scholar] [CrossRef]
- Picelli, A.; Melotti, C.; Origano, F.; Waldner, A.; Fiaschi, A.; Santilli, V.; Smania, N. Robot-assisted gait training in patients with Parkinson disease: A randomized controlled trial. Neurorehabil. Neural Repair 2012, 26, 353–361. [Google Scholar] [CrossRef]
- Picelli, A.; Melotti, C.; Origano, F.; Neri, R.; Verzè, E.; Gandolfi, M.; Waldner, A.; Smania, N. Robot-assisted gait training is not superior to balance training for improving postural instability in patients with mild to moderate Parkinson’s disease: A single-blind randomized controlled trial. Clin. Rehabil. 2015, 29, 339–347. [Google Scholar] [CrossRef]
- Mirelman, A.; Maidan, I.; Herman, T.; Deutsch, J.E.; Giladi, N.; Hausdorff, J.M. Virtual reality for gait training: Can it induce motor learning to enhance complex walking and reduce fall risk in patients with Parkinson’s disease? J. Gerontol. A. Biol. Sci. Med. Sci. 2011, 66, 234–240. [Google Scholar] [CrossRef] [Green Version]
- Espay, A.J.; Baram, Y.; Dwivedi, A.K.; Shukla, R.; Gartner, M.; Gaines, L.; Duker, A.P.; Revilla, F.J. At-home training with closed-loop augmented-reality cueing device for improving gait in patients with Parkinson disease. J. Rehabil. Res. Dev. 2010, 47, 573–582. [Google Scholar] [CrossRef]
- Carpinella, I.; Cattaneo, D.; Bonora, G.; Bowman, T.; Martina, L.; Montesano, A.; Ferrarin, M. Wearable Sensor-Based Biofeedback Training for Balance and Gait in Parkinson Disease: A Pilot Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2017, 98, 622–630.e3. [Google Scholar] [CrossRef] [Green Version]
- Alcock, L.; Galna, B.; Hausdorff, J.M.; Lord, S.; Rochester, L. Gait & Posture Special Issue: Gait adaptations in response to obstacle type in fallers with Parkinson’s disease. Gait Posture 2018, 61, 368–374. [Google Scholar] [CrossRef]
- Yun, S.J.; Lee, H.H.; Lee, W.H.; Lee, S.H.; Oh, B.M.; Seo, H.G. Effect of robot-assisted gait training on gait automaticity in Parkinson disease: A prospective, open-label, single-arm, pilot study. Medicine 2021, 100, e24348. [Google Scholar] [CrossRef]
- Byl, N.; Zhang, W.; Coo, S.; Tomizuka, M. Clinical impact of gait training enhanced with visual kinematic biofeedback: Patients with Parkinson’s disease and patients stable post stroke. Neuropsychologia 2015, 79, 332–343. [Google Scholar] [CrossRef] [Green Version]
- Raccagni, C.; Goebel, G.; Gaßner, H.; Granata, R.; Ndayisaba, J.P.; Seebacher, B.; Schoenherr, G.; Mitterhuber, J.; Hendriks, P.; Kaindlstorfer, C.; et al. Physiotherapy improves motor function in patients with the Parkinson variant of multiple system atrophy: A prospective trial. Parkinsonism Relat. Disord. 2019, 67, 60–65. [Google Scholar] [CrossRef]
- Follett, K.A.; Weaver, F.M.; Stern, M.; Hur, K.; Harris, C.L.; Luo, P.; Marks, W.J.; Rothlind, J.; Sagher, O.; Moy, C.; et al. Pallidal versus subthalamic deep-brain stimulation for Parkinson’s disease. N. Engl. J. Med. 2010, 362, 2077–2091. [Google Scholar] [CrossRef] [Green Version]
- Barboza, N.M.; Terra, M.B.; Bueno, M.E.B.; Christofoletti, G.; Smaili, S.M. Physiotherapy Versus Physiotherapy Plus Cognitive Training on Cognition and Quality of Life in Parkinson Disease: Randomized Clinical Trial. Am. J. Phys. Med. Rehabil. 2019, 98, 460–468. [Google Scholar] [CrossRef]
- Furnari, A.; Calabrò, R.S.; De Cola, M.C.; Bartolo, M.; Castelli, A.; Mapelli, A.; Buttacchio, G.; Farini, E.; Bramanti, P.; Casale, R. Robotic-assisted gait training in Parkinson’s disease: A three-month follow-up randomized clinical trial. Int. J. Neurosci. 2017, 127, 996–1004. [Google Scholar] [CrossRef]
- Kapur, S.S.; Stebbins, G.T.; Goetz, C.G. Vibration therapy for Parkinson’s disease: Charcot’s studies revisited. J. Parkinsons. Dis. 2012, 2, 23–27. [Google Scholar] [CrossRef]
- Agari, T.; Date, I. Spinal cord stimulation for the treatment of abnormal posture and gait disorder in patients with Parkinson’s disease. Neurol. Med. Chir. (Tokyo) 2012, 52, 470–474. [Google Scholar] [CrossRef] [Green Version]
- Amara, A.W.; Wood, K.H.; Joop, A.; Memon, R.A.; Pilkington, J.; Tuggle, S.C.; Reams, J.; Barrett, M.J.; Edwards, D.A.; Weltman, A.L.; et al. Randomized, Controlled Trial of Exercise on Objective and Subjective Sleep in Parkinson’s Disease. Mov. Disord. 2020, 35, 947–958. [Google Scholar] [CrossRef]
- Landers, M.R.; Navalta, J.W.; Murtishaw, A.S.; Kinney, J.W.; Pirio Richardson, S. A High-Intensity Exercise Boot Camp for Persons With Parkinson Disease: A Phase II, Pragmatic, Randomized Clinical Trial of Feasibility, Safety, Signal of Efficacy, and Disease Mechanisms. J. Neurol. Phys. Ther. 2019, 43, 12–25. [Google Scholar] [CrossRef]
- Silveira, C.R.A.; Roy, E.A.; Intzandt, B.N.; Almeida, Q.J. Aerobic exercise is more effective than goal-based exercise for the treatment of cognition in Parkinson’s disease. Brain Cogn. 2018, 122, 1–8. [Google Scholar] [CrossRef]
- Braun, S.; Beurskens, A.; Kleynen, M.; Schols, J.; Wade, D. Rehabilitation with mental practice has similar effects on mobility as rehabilitation with relaxation in people with Parkinson’s disease: A multicentre randomised trial. J. Physiother. 2011, 57, 27–34. [Google Scholar] [CrossRef] [Green Version]
- Kwok, J.Y.Y.; Kwan, J.C.Y.; Auyeung, M.; Mok, V.C.T.; Lau, C.K.Y.; Choi, K.C.; Chan, H.Y.L. Effects of Mindfulness Yoga vs Stretching and Resistance Training Exercises on Anxiety and Depression for People With Parkinson Disease: A Randomized Clinical Trial. JAMA Neurol. 2019, 76, 755–763. [Google Scholar] [CrossRef] [PubMed]
- McKee, K.E.; Hackney, M.E. The effects of adapted tango on spatial cognition and disease severity in Parkinson’s disease. J. Mot. Behav. 2013, 45, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Duncan, R.P.; Earhart, G.M. Randomized controlled trial of community-based dancing to modify disease progression in Parkinson disease. Neurorehabil. Neural Repair 2012, 26, 132–143. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Harmer, P.; Fitzgerald, K.; Eckstrom, E.; Stock, R.; Galver, J.; Maddalozzo, G.; Batya, S.S. Tai chi and postural stability in patients with Parkinson’s disease. N. Engl. J. Med. 2012, 366, 511–519. [Google Scholar] [CrossRef] [Green Version]
- Schmitz-Hübsch, T.; Pyfer, D.; Kielwein, K.; Fimmers, R.; Klockgether, T.; Wüllner, U. Qigong exercise for the symptoms of Parkinson’s disease: A randomized, controlled pilot study. Mov. Disord. 2006, 21, 543–548. [Google Scholar] [CrossRef]
- Burt, J.; Ravid, E.; Bradford, S.; Fisher, N.J.; Zeng, Y.; Chomiak, T.; Brown, L.; McKeown, M.J.; Hu, B.; Camicioli, R. The Effects of Music-Contingent Gait Training on Cognition and Mood in Parkinson Disease: A Feasibility Study. Neurorehabil. Neural Repair 2020, 34, 82–92. [Google Scholar] [CrossRef]
- Poier, D.; Rodrigues Recchia, D.; Ostermann, T.; Büssing, A. A Randomized Controlled Trial to Investigate the Impact of Tango Argentino versus Tai Chi on Quality of Life in Patients with Parkinson Disease: A Short Report. Complement. Med. Res. 2019, 26, 398–403. [Google Scholar] [CrossRef]
- Fogarty, J.N.; Murphy, K.J.; McFarlane, B.; Montero-Odasso, M.; Wells, J.; Troyer, A.K.; Trinh, D.; Gutmanis, I.; Hansen, K.T. Taoist Tai Chi® and Memory Intervention for Individuals with Mild Cognitive Impairment. J. Aging Phys. Act. 2016, 24, 169–180. [Google Scholar] [CrossRef]
- Schlick, C.; Ernst, A.; Bötzel, K.; Plate, A.; Pelykh, O.; Ilmberger, J. Visual cues combined with treadmill training to improve gait performance in Parkinson’s disease: A pilot randomized controlled trial. Clin. Rehabil. 2016, 30, 463–471. [Google Scholar] [CrossRef] [Green Version]
- Bekkers, E.M.J.; Mirelman, A.; Alcock, L.; Rochester, L.; Nieuwhof, F.; Bloem, B.R.; Pelosin, E.; Avanzino, L.; Cereatti, A.; Della Croce, U.; et al. Do Patients With Parkinson’s Disease With Freezing of Gait Respond Differently Than Those Without to Treadmill Training Augmented by Virtual Reality? Neurorehabil. Neural Repair 2020, 34, 440–449. [Google Scholar] [CrossRef]
- Yuan, R.Y.; Chen, S.C.; Peng, C.W.; Lin, Y.N.; Chang, Y.T.; Lai, C.H. Effects of interactive video-game-based exercise on balance in older adults with mild-to-moderate Parkinson’s disease. J. Neuroeng. Rehabil. 2020, 17, 91. [Google Scholar] [CrossRef]
- Pennington, C.; Ball, H.; Swirski, M. Functional Cognitive Disorder: Diagnostic Challenges and Future Directions. Diagnostics 2019, 9, 131. [Google Scholar] [CrossRef] [Green Version]
- Judge, D.; Roberts, J.; Khandker, R.; Ambegaonkar, B.; Black, C.M. Physician Perceptions about the Barriers to Prompt Diagnosis of Mild Cognitive Impairment and Alzheimer’s Disease. Int. J. Alzheimers. Dis. 2019, 2019, 3637954. [Google Scholar] [CrossRef] [Green Version]
- Enoka, R.M. Neural adaptations with chronic physical activity. J. Biomech. 1997, 30, 447–455. [Google Scholar] [CrossRef]
- Colcombe, S.J.; Erickson, K.I.; Raz, N.; Webb, A.G.; Cohen, N.J.; McAuley, E.; Kramer, A.F. Aerobic fitness reduces brain tissue loss in aging humans. J. Gerontol. A. Biol. Sci. Med. Sci. 2003, 58, 176–180. [Google Scholar] [CrossRef] [Green Version]
- Uijen, I.L.; Aaronson, J.A.; Karssemeijer, E.G.A.; Olde Rikkert, M.G.M.; Kessels, R.P.C. Individual Differences in the Effects of Physical Activity on Cognitive Function in People with Mild to Moderate Dementia. J. Alzheimers. Dis. 2020, 74, 435–439. [Google Scholar] [CrossRef] [Green Version]
- Savica, R.; Wennberg, A.M.V.; Hagen, C.; Edwards, K.; Roberts, R.O.; Hollman, J.H.; Knopman, D.S.; Boeve, B.F.; Machulda, M.M.; Petersen, R.C.; et al. Comparison of Gait Parameters for Predicting Cognitive Decline: The Mayo Clinic Study of Aging. J. Alzheimers. Dis. 2017, 55, 559. [Google Scholar] [CrossRef] [Green Version]
- Styliadis, C.; Kartsidis, P.; Paraskevopoulos, E.; Ioannides, A.A.; Bamidis, P.D. Neuroplastic effects of combined computerized physical and cognitive training in elderly individuals at risk for dementia: An eLORETA controlled study on resting states. Neural Plast. 2015, 2015, 172192. [Google Scholar] [CrossRef] [Green Version]
- Yoon, D.H.; Lee, J.Y.; Song, W. Effects of Resistance Exercise Training on Cognitive Function and Physical Performance in Cognitive Frailty: A Randomized Controlled Trial. J. Nutr. Health Aging 2018, 22, 944–951. [Google Scholar] [CrossRef]
- Netz, Y.; Yekutieli, Z.; Arnon, M.; Argov, E.; Tchelet, K.; Benmoha, E.; Jacobs, J.M. Personalized Exercise Programs Based upon Remote Assessment of Motor Fitness: A Pilot Study among Healthy People Aged 65 Years and Older. Gerontology 2022, 68, 465–479. [Google Scholar] [CrossRef]
- Jansons, P.; Dalla Via, J.; Daly, R.M.; Fyfe, J.J.; Gvozdenko, E.; Scott, D. Delivery of Home-Based Exercise Interventions in Older Adults Facilitated by Amazon Alexa: A 12-week Feasibility Trial. J. Nutr. Health Aging 2022, 26, 96–102. [Google Scholar] [CrossRef]
- Taylor, M.E.; Close, J.C.T.; Lord, S.R.; Kurrle, S.E.; Webster, L.; Savage, R.; Delbaere, K. Pilot feasibility study of a home-based fall prevention exercise program (StandingTall) delivered through a tablet computer (iPad) in older people with dementia. Australas. J. Ageing 2020, 39, e278–e287. [Google Scholar] [CrossRef]
- Delbaere, K.; Valenzuela, T.; Lord, S.R.; Clemson, L.; Zijlstra, G.A.R.; Close, J.C.T.; Lung, T.; Woodbury, A.; Chow, J.; McInerney, G.; et al. E-health StandingTall balance exercise for fall prevention in older people: Results of a two year randomised controlled trial. BMJ 2021, 373, n740. [Google Scholar] [CrossRef]
- Netz, Y.; Argov, E.; Yekutieli, Z.; Ayalon, M.; Tchelet, K.; Ben-Sira, D.; Amar, Y.; Jacobs, J.M. Personalized multicomponent exercise programs using smartphone technology among older people: Protocol for a randomized controlled trial. BMC Geriatr. 2021, 21, 605. [Google Scholar] [CrossRef] [PubMed]
- Daly, R.M.; Gianoudis, J.; Hall, T.; Mundell, N.L.; Maddison, R. Feasibility, Usability, and Enjoyment of a Home-Based Exercise Program Delivered via an Exercise App for Musculoskeletal Health in Community-Dwelling Older Adults: Short-term Prospective Pilot Study. JMIR MHealth UHealth 2021, 9, e21094. [Google Scholar] [CrossRef] [PubMed]
- Pitkänen, A.; Alanen, H.M.; Kampman, O.; Suontaka-Jamalainen, K.; Leinonen, E. Implementing physical exercise and music interventions for patients suffering from dementia on an acute psychogeriatric inpatient ward. Nord. J. Psychiatry 2019, 73, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Wu, H.; Qi, M.; Wang, S.; Zhang, Q.; Zhou, L.; Wang, S.; Wang, W.; Wu, T.; Xiao, M.; et al. Effects of a specially designed aerobic dance routine on mild cognitive impairment. Clin. Interv. Aging 2018, 13, 1691–1700. [Google Scholar] [CrossRef] [Green Version]
- Tremont, G.; Davis, J.; Ott, B.R.; Uebelacker, L.; Kenney, L.; Gillette, T.; Britton, K.; Sanborn, V. Feasibility of a Yoga Intervention for Individuals with Mild Cognitive Impairment: A Randomized Controlled Trial. J. Integr. Complement. Med. 2022, 28, 250–260. [Google Scholar] [CrossRef]
- Lin, L.C.; Yang, M.H.; Kao, C.C.; Wu, S.C.; Tang, S.H.; Lin, J.G. Using acupressure and Montessori-based activities to decrease agitation for residents with dementia: A Cross-over trial. J. Am. Geriatr. Soc. 2009, 57, 1022–1029. [Google Scholar] [CrossRef]
- Sobol, N.A.; Dall, C.H.; Høgh, P.; Hoffmann, K.; Frederiksen, K.S.; Vogel, A.; Siersma, V.; Waldemar, G.; Hasselbalch, S.G.; Beyer, N. Change in Fitness and the Relation to Change in Cognition and Neuropsychiatric Symptoms After Aerobic Exercise in Patients with Mild Alzheimer’s Disease. J. Alzheimers. Dis. 2018, 65, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Yu, F.; Vock, D.M.; Zhang, L.; Salisbury, D.; Nelson, N.W.; Chow, L.S.; Smith, G.; Barclay, T.R.; Dysken, M.; Wyman, J.F. Cognitive Effects of Aerobic Exercise in Alzheimer’s Disease: A Pilot Randomized Controlled Trial. J. Alzheimers. Dis. 2021, 80, 233–244. [Google Scholar] [CrossRef]
- Kalron, A.; Allali, G. Gait and cognitive impairments in multiple sclerosis: The specific contribution of falls and fear of falling. J. Neural Transm. 2017, 124, 1407–1416. [Google Scholar] [CrossRef]
- Sebastião, E.; McAuley, E.; Shigematsu, R.; Adamson, B.C.; Bollaert, R.E.; Motl, R.W. Home-based, square-stepping exercise program among older adults with multiple sclerosis: Results of a feasibility randomized controlled study. Contemp. Clin. Trials 2018, 73, 136–144. [Google Scholar] [CrossRef] [Green Version]
- Venkataraman, K.; Tai, B.C.; Khoo, E.Y.H.; Tavintharan, S.; Chandran, K.; Hwang, S.W.; Phua, M.S.L.A.; Wee, H.L.; Koh, G.C.H.; Tai, E.S. Short-term strength and balance training does not improve quality of life but improves functional status in individuals with diabetic peripheral neuropathy: A randomised controlled trial. Diabetologia 2019, 62, 2200–2210. [Google Scholar] [CrossRef] [Green Version]
- Pahwa, R.; Dhall, R.; Ostrem, J.; Gwinn, R.; Lyons, K.; Ro, S.; Dietiker, C.; Luthra, N.; Chidester, P.; Hamner, S.; et al. An Acute Randomized Controlled Trial of Noninvasive Peripheral Nerve Stimulation in Essential Tremor. Neuromodulation 2019, 22, 537–545. [Google Scholar] [CrossRef] [Green Version]
- World Confederation for Physical Therapy. Physical Therapy Services for Older People; World Confederation for Physical Therapy: London, UK, 2017. [Google Scholar]
- Clark, D.J.; Christou, E.A.; Ring, S.A.; Williamson, J.B.; Doty, L. Enhanced somatosensory feedback reduces prefrontal cortical activity during walking in older adults. J. Gerontol. A. Biol. Sci. Med. Sci. 2014, 69, 1422–1428. [Google Scholar] [CrossRef] [Green Version]
- Ahlskog, J.E.; Geda, Y.E.; Graff-Radford, N.R.; Petersen, R.C. Physical exercise as a preventive or disease-modifying treatment of dementia and brain aging. Mayo Clin. Proc. 2011, 86, 876–884. [Google Scholar] [CrossRef] [Green Version]
- Takeuchi, N.; Oouchida, Y.; Izumi, S.I. Motor control and neural plasticity through interhemispheric interactions. Neural Plast. 2012, 2012, 823285. [Google Scholar] [CrossRef]
- Maes, C.; Gooijers, J.; Orban de Xivry, J.J.; Swinnen, S.P.; Boisgontier, M.P. Two hands, one brain, and aging. Neurosci. Biobehav. Rev. 2017, 75, 234–256. [Google Scholar] [CrossRef]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of combined physical and cognitive training on cognition: A systematic review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef] [Green Version]
- Ballesteros, S.; Kraft, E.; Santana, S.; Tziraki, C. Maintaining older brain functionality: A targeted review. Neurosci. Biobehav. Rev. 2015, 55, 453–477. [Google Scholar] [CrossRef]
- Best, J.R.; Rosano, C.; Aizenstein, H.J.; Tian, Q.; Boudreau, R.M.; Ayonayon, H.N.; Satterfield, S.; Simonsick, E.M.; Studenski, S.; Yaffe, K.; et al. Long-term changes in time spent walking and subsequent cognitive and structural brain changes in older adults. Neurobiol. Aging 2017, 57, 153–161. [Google Scholar] [CrossRef]
- Oh, D.S.; Choi, J.D. The effect of motor imagery training for trunk movements on trunk muscle control and proprioception in stroke patients. J. Phys. Ther. Sci. 2017, 29, 1224–1228. [Google Scholar] [CrossRef] [Green Version]
- Shimamura, N.; Katagai, T.; Kakuta, K.; Matsuda, N.; Katayama, K.; Fujiwara, N.; Watanabe, Y.; Naraoka, M.; Ohkuma, H. Rehabilitation and the Neural Network After Stroke. Transl. Stroke Res. 2017, 8, 507–514. [Google Scholar] [CrossRef]
- Carmeli, E. Frailty and Primary Sarcopenia: A Review. Adv. Exp. Med. Biol. 2017, 1020, 53–68. [Google Scholar] [CrossRef]
- Langhorne, P.; Baylan, S.; Early Supported Discharge Trialists. Early supported discharge services for people with acute stroke. Cochrane Database Syst. Rev. 2017, 7, CD000443. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, S.; Sniehotta, F.F.; Van Wijck, F.; Greig, C.A.; Johnston, M.; Mcmurdo, M.E.T.; Dennis, M.; Mead, G.E. A systematic review of perceived barriers and motivators to physical activity after stroke. Int. J. Stroke 2013, 8, 357–364. [Google Scholar] [CrossRef]
- Haworth, J.; Young, C.; Thornton, E. The effects of an “exercise and education” programme on exercise self-efficacy and levels of independent activity in adults with acquired neurological pathologies: An exploratory, randomized study. Clin. Rehabil. 2009, 23, 371–383. [Google Scholar] [CrossRef]
- Severinsen, K.D.; Tufton, A.; Hannan, E.; Schwind, J.S.; Schmucker, D.; Cutler, A. Evaluating outcomes from an integrated health service for older patients. Ochsner J. 2015, 15, 423–428. [Google Scholar]
- Pantell, M.; Rehkopf, D.; Jutte, D.; Syme, S.L.; Balmes, J.; Adler, N. Social isolation: A predictor of mortality comparable to traditional clinical risk factors. Am. J. Public Health 2013, 103, 2056–2062. [Google Scholar] [CrossRef]
- Pelicioni, P.H.S.; Schulz-Moore, J.S.; Hale, L.; Canning, C.G.; Lord, S.R. Lockdown During COVID-19 and the Increase of Frailty in People With Neurological Conditions. Front. Neurol. 2020, 11, 604299. [Google Scholar] [CrossRef]
- Garner, I.W.; Varey, S.; Navarro-Pardo, E.; Marr, C.; Holland, C.A. An observational cohort study of longitudinal impacts on frailty and well-being of COVID-19 lockdowns in older adults in England and Spain. Health Soc. Care Community 2022. [Google Scholar] [CrossRef]
- Sahin, S.; Karsidag, S.; Cinar, N.; Ates, M.F.; Demir, S.; Eren, F.; Neyal, A.; Kisabay Ak, A.; Bora Tokcaer, A.; Erkoc Ataoglu, E.; et al. The Impact of the COVID-19 Lockdown on the Quality of Life in Chronic Neurological Diseases: The Results of a COVQoL-CND Study. Eur. Neurol. 2021, 84, 450–459. [Google Scholar] [CrossRef]
- Helmich, R.C.; Bloem, B.R. The Impact of the COVID-19 Pandemic on Parkinson’s Disease: Hidden Sorrows and Emerging Opportunities. J. Parkinsons. Dis. 2020, 10, 351–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambercy, O.; Lehner, R.; Chua, K.; Wee, S.K.; Rajeswaran, D.K.; Kuah, C.W.K.; Ang, W.T.; Liang, P.; Campolo, D.; Hussain, A.; et al. Neurorehabilitation from a Distance: Can Intelligent Technology Support Decentralized Access to Quality Therapy? Front. Robot. AI 2021, 8, 612415. [Google Scholar] [CrossRef] [PubMed]
- Galna, B.; Jackson, D.; Schofield, G.; McNaney, R.; Webster, M.; Barry, G.; Mhiripiri, D.; Balaam, M.; Olivier, P.; Rochester, L. Retraining function in people with Parkinson’s disease using the Microsoft kinect: Game design and pilot testing. J. Neuroeng. Rehabil. 2014, 11, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Almasi, S.; Ahmadi, H.; Asadi, F.; Shahmoradi, L.; Arji, G.; Alizadeh, M.; Kolivand, H. Kinect-Based Rehabilitation Systems for Stroke Patients: A Scoping Review. Biomed Res. Int. 2022, 2022, 4339054. [Google Scholar] [CrossRef]
- Korhonen, O.; Väyrynen, K.; Krautwald, T.; Bilby, G.; Broers, H.A.T.; Giunti, G.; Isomursu, M. Data-Driven Personalization of a Physiotherapy Care Pathway: Case Study of Posture Scanning. JMIR Rehabil. Assist. Technol. 2020, 7, e18508. [Google Scholar] [CrossRef]
- Wijma, A.J.; Bletterman, A.N.; Clark, J.R.; Vervoort, S.C.J.M.; Beetsma, A.; Keizer, D.; Nijs, J.; Van Wilgen, C.P. Patient-centeredness in physiotherapy: What does it entail? A systematic review of qualitative studies. Physiother. Theory Pract. 2017, 33, 825–840. [Google Scholar] [CrossRef]
- Miller, K.L. Patient centered care: A path to better health outcomes through engagement and activation. NeuroRehabilitation 2016, 39, 465–470. [Google Scholar] [CrossRef]
- Neibling, B.A.; Jackson, S.M.; Hayward, K.S.; Barker, R.N. Perseverance with technology-facilitated home-based upper limb practice after stroke: A systematic mixed studies review. J. Neuroeng. Rehabil. 2021, 18, 43. [Google Scholar] [CrossRef]
- Keesara, S.; Jonas, A.; Schulman, K. COVID-19 and Health Care’s Digital Revolution. N. Engl. J. Med. 2020, 382, e82. [Google Scholar] [CrossRef]
- Meulenberg, C.J.W.; de Bruin, E.D.; Marusic, U. A Perspective on Implementation of Technology-Driven Exergames for Adults as Telerehabilitation Services. Front. Psychol. 2022, 13, 840863. [Google Scholar] [CrossRef]
- Hung, L.; Levine, H.; Randhawa, P.; Park, J. Technology-based group exercise interventions for people living with dementia or mild cognitive impairment: A scoping review protocol. BMJ Open 2022, 12, e055990. [Google Scholar] [CrossRef]
- Keel, S.; Schmid, A.; Keller, F.; Schoeb, V. Investigating the use of digital health tools in physiotherapy: Facilitators and barriers. Physiother. Theory Pract. 2022, 1–20. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Physiotherapy Interventions | Physiotherapy’s Goal |
|---|---|
| Balance and gait training | Enhance mobility |
| Robot-assisted gait training | Enhance mobility |
| Occupational therapy and physiotherapy | Enhance mobility and limb function |
| Walking and treadmill training | Enhance mobility |
| Upper limb robot-assisted therapy | Enhance mobility and limb function |
| Body-weight-supported walking training | Enhance mobility |
| Transcranial direct current Stimulation | Enhance limb function and swallow |
| Electrical stimulation therapy | Enhance limb function |
| Arm rehabilitation therapy | Enhance mobility |
| Cognitive training | Enhance cognitive function |
| Mirror therapy | Enhance mobility |
| Speech and language therapy | Enhance cognitive function |
| Verticalization treatment | Enhance mobility and limb function |
| Functional electrical stimulation | Enhance mobility and limb function |
| Ankle treatment | Enhance mobility and limb function |
| Neurocognitive robot-assisted rehabilitation | Enhance mobility and limb function |
| Robot-assisted arm training | Enhance mobility and limb function |
| Swallow therapy | Enhance cognitive function and swallow |
| Transcranial magnetic stimulation | Enhance mobility and limb function |
| Continuous theta burst stimulation | Enhance cognitive function |
| Equipment utilized in rehabilitation physiotherapy sessions | |
| Treadmills | Wii Sports Resort |
| Virtual reality equipment | Stride Management Assistant |
| Lokomat™ | Mobile hoist (ROPOX ALL IN ONE) |
| GAITRite® Portable Walkway System | GripAble |
| Constant current stimulator | Com-Pressor Belt |
| InMotion | BIORescue |
| NintendoΤΜ Wii balance board | Vibrotactile BF device |
| Ankle Foot Orthosis | MagPro X100 stimulator |
| ERIGO® | Wireless joint angle sensors |
| MIT-Manus | Stimulo |
| Arm ergometer | All-In-One Walking Trainer |
| Stationary bicycle | NintendoTM Wii Sports games |
| Walkbot | Electrical stimulation machines |
| Robot system for upper limb impairment | Robot-assisted Bi-Manu Track |
| Ekso wearable exoskeleton | GEAR system |
| Planar Robotic Manipulandum | ReHapticKnob |
| NeReBot | |
| Physiotherapy Interventions | Physiotherapy’s Goal |
|---|---|
| Balance and gait training | Enhance motor function |
| Robot-assisted gait training | Enhance motor function |
| Walking and treadmill training | Enhance motor function |
| Aerobic dance therapy | Enhance cognitive function |
| Stretching and resistance training | Enhance motor and cognitive function |
| Body-weight-supported walking training | Enhance motor function |
| Physical activity and treatment therapy | Enhance motor function |
| Tai chi | Enhance motor function and emotional status |
| Argentine tango | Enhance motor function and emotional status |
| Obstacle-crossing training | Enhance motor function |
| Retraining function therapy | Enhance motor function |
| Spinal cord stimulation therapy | Enhance motor function |
| Vibration therapy | Enhance motor function |
| Equipment utilized in rehabilitation physiotherapy sessions | |
| Treadmills | Gamepad with wearable internal sensors |
| Gait Trainer GT1 | Recumbent Cycle Ergometers |
| Virtual reality equipment | SMART Lounge vibroacoustic system |
| Lokomat™ | Smart shoes |
| GAITRite® Portable Walkway System | Microsoft Kinect and Xbox gaming console |
| XaviX system | |
| Physiotherapy Interventions | Physiotherapy’s Goal |
|---|---|
| Exergames therapy | Enhance changes in the cortical activity |
| Aerobic dance therapy | Enhance cognitive function and mobility |
| Acupressure | Decrease agitated behaviors |
| Memory intervention | Enhance cognitive function and mobility |
| Exercise programs | Enhance balance, flexibility, and strength |
| Yoga | Enhance visuospatial functioning |
| Equipment utilized in rehabilitation physiotherapy sessions | |
| Brain Fitness software | GAITRite |
| Smartphone sensors/trainers | Stationary bikes |
| Amazon Alexa | iPad |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spanakis, M.; Xylouri, I.; Patelarou, E.; Patelarou, A. A Literature Review of High-Tech Physiotherapy Interventions in the Elderly with Neurological Disorders. Int. J. Environ. Res. Public Health 2022, 19, 9233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159233
Spanakis M, Xylouri I, Patelarou E, Patelarou A. A Literature Review of High-Tech Physiotherapy Interventions in the Elderly with Neurological Disorders. International Journal of Environmental Research and Public Health. 2022; 19(15):9233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159233
Chicago/Turabian StyleSpanakis, Marios, Ioanna Xylouri, Evridiki Patelarou, and Athina Patelarou. 2022. "A Literature Review of High-Tech Physiotherapy Interventions in the Elderly with Neurological Disorders" International Journal of Environmental Research and Public Health 19, no. 15: 9233. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159233