
Exploring Professionalism Dilemma and Moral Distress through Medical Students’ Eyes: A Mixed-Method Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Context
2.2. Study Design
2.3. Participants
2.3.1. Survey Participants
2.3.2. Interview Participants
2.4. Study Instruments
2.4.1. Survey Measures
2.4.2. Interview Guide
2.5. Data Analysis
2.5.1. Quantitative Analysis
2.5.2. Qualitative Analysis
3. Results
3.1. Survey Findings
3.1.1. Demographic Characteristics of Survey Respondents
3.1.2. Frequency of Professionalism Dilemmas Encountered by Medical Students
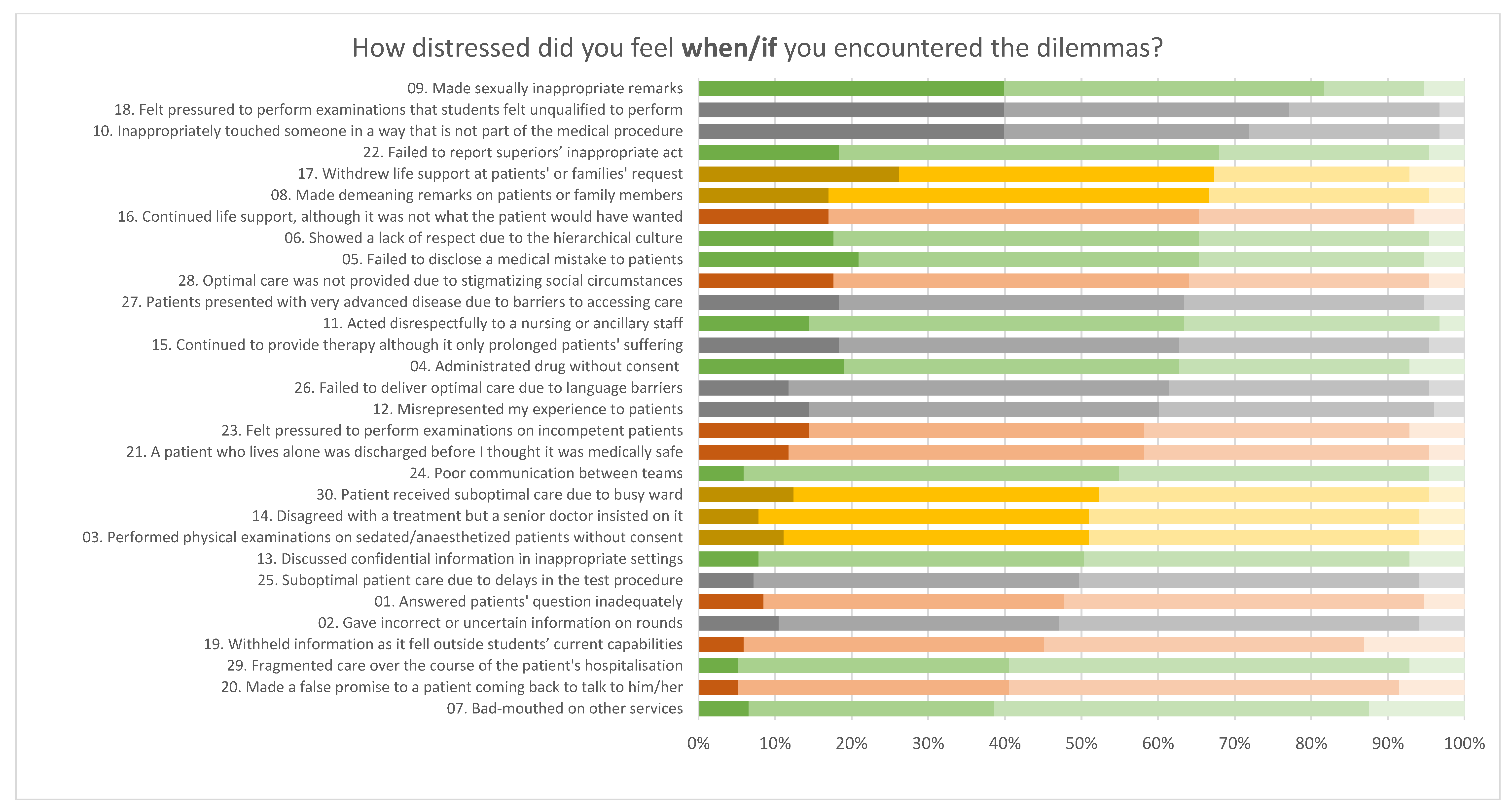
3.1.3. Perceived Level of Moral Distress in the Professionalism Dilemmas
3.2. Interview Findings
3.2.1. Dilemmas or Wrongdoings at the Workplace
- (i)
- Doctor-to-Patient Interaction
“I have seen patients being referred to with “fucked up names like ‘vege vege (choy choy)’ if they are vegetative state. That’s a lack of respect. Or they were calling a patient ‘it,’ like ‘it is a case of cerebral palsy.”(Interview 9, M23, O)
“Talking about the truth is okay. It is okay if they have a reason behind why they are telling them they are fat. The patient might not understand the other words [medical jargon].”(Interview 4, M24, M)
“It is important to let them know. Do not avoid it. It is about how you deliver the message: like ‘clinically overweight and associated health risks’—it’s how they take it: medical advice or judgment? Plus, “obese” in Cantonese is a medical term. So, it is appropriate and encouraged if it is for their health.”(Interview 3, M24, M)
“I am very numb to it, and it is not on my radar anymore. Both are unnecessary, whether calling the patient obese out of concern for health or talking to someone else nearby. Nine out of 10 doctors will say this to a patient, and I’m not sure I’m offended.”(Interview 9, M23, O)
“I was in an abortion clinic, and the doctor did not give any counseling. It was abrupt, saying that ‘the baby’s gone, and this is what you have to do XYZ,’ you could see the patient was emotional, but the doctor did not address the emotions. The management of a sensitive issue requires more care in communication. It’s important to address the emotional part.”(Interview 8, M23, F)
“I was in a cardiology outpatient clinic. The doctor was transiently empathetic and more pragmatic about the problem than consoling. The patient was on the verge of tears, but the doctor just talked about social support and practical issues, saying there was nothing he could do to help the patient.”(Interview 4, M24, M)
“If the patient calls the doctor and there is no response, it is normal. The requests cannot be fulfilled, or it is not your duty. They should get a response, but many times there is no response and pretend they [doctors] do not hear them [the patients].”(Interview 7, M23, F)
“A doctor did a transvaginal exam suspecting a mass and immediately afterward did a transrectal exam without informing the patient. The patient was like, ‘Oh what? That’s not my vagina’. In practice, the only ‘verbal consent’ between doctors and patients is usually ‘I’m going in now,’ and the patient will be silent or just be like ‘okay.’”(Interview 9, M23, O)
“The doctor pressured a male patient to allow medical students to let them listen to the lung, and when the patient said no, the doctor said, ‘are you not feeling well?’ I felt a little uneasy but still quickly listened to the lung.”(Interview 5, M22, M)
“Even a consenting patient usually does not consent to the rectal exam, so it’s very inappropriate for the medical student to do it on a patient who is also ‘out of it.’ To some extent, performing a physical examination benefits the student. In my opinion, it was inappropriate for an unresponsive patient to undergo it repeatedly without their consent. I feel that the medical students’ learning should benefit the patient.”(Interview 7, M23, F)
“In pediatrics, many children are bed-bound and cannot speak. You still have to do it as this is the disease [that they cannot speak/consent]. They have a higher standard in urology, doing DRE, or in OG, relating to your private parts [of consent]. OG has a high standard of consent, and they explain very well and tell you [about the procedure] many times. They should all have the same standard for everything in an ideal world.”(Interview 7, M23, F)
“It’s not good because the patient cannot be mobile, especially for the elderly. They can’t drink water, which leads to dehydration; this affects the patient. Sometimes the doctor agrees [to restrain the patient], even if they don’t know the reason.”(Interview 5, M22, M)
“I asked why we needed to do the test for parasites just out of curiosity, but the doctor said ‘because the patient was that ‘type’ of people. I found it disappointing because the doctor was otherwise really nice, and [they] enjoyed the out-patients clinics until that point.”(Interview 9, M23, O)
“The doctor or healthcare staff get impatient when [patients] can’t explain [their needs] in [Chinese or English]. Although it’s better to write or draw something out, it doesn’t happen all the time. Translation services aren’t always available either.”(Interview 2, M24, F)
- (ii)
- Doctor-to-Student Interaction
“[The doctor said] ‘oh, you have already given up? It’s a long time until next year!’”(Interview 6, M22, M)
“Objectively, I have seen things that would be considered disrespectful, but students who know him would think he’s joking. When one student does one thing wrong in physical examination, he would say it doesn’t matter; go jump out the window. The ward group […] didn’t laugh along.”(Interview 4, M24, M)
“[The difference is] whether they’re trying to teach you something or not. Commenting on anything other than your ability is disrespectful.”(Interview 8, M23, F)
“While doing the mastectomy, the doctor pointed to the [female] ward mate, who said she looks like a transgender male. […] He teased that the ward mate must be familiar with mastectomy and have done it in Thailand.”(Interview 1, M24, M)
“I think there has been sexual harassment like calling me pretty by a professional.”(Interview 8, M23, F)
- (iii)
- Student-to-Patient Interaction
“In pediatrics, upon some children with Down’s Syndrome, I heard a ward mate use a teasing attitude to call the patient, ‘this is a Down’s.’ Using the diagnosis to label the patient is inappropriate. I felt that the ward mate did not have bad intentions and was just making a joke, but it’s a form of disrespect.”(Interview 6, M22, M)
“If I were close with the ward mate, I would tell him not to call a patient by their diagnosis even as a joke, but we were not close, so I did not say anything. The reason is that my ward mate and I will cooperate for a year and would not want to compromise the relationship.”(Interview 6, M22, M)
“This guy [the male student] is misogynistic; he makes offensive comments. Then the whole room went silent. He apologized in front of everyone and then to the doctor afterward, but both comments were bad.”(Interview 9, M23, O)
“Taking blood can only be done when the doctor is present, but the technician said that even if the doctor is not here, you can do it, so they technically didn’t follow the rules despite being instructed to do so.”(Interview 5, M22 M)
“I’ve seen him take pictures of the operation theatre list without covering the personal details, and defended himself by saying his iPad is encrypted.”(Interview 3, M24, M)
- (iv)
- Student-to-Student Interaction
“I have a ward mate who does not respect personal boundaries. He would stand very close to ward mates and touch them or stand very close to them. He touched a female war mate’s butt twice, touched their hands, and stood close while looking at an X-ray. Since September, and I feel it’s very problematic.”(Interview 3, M24, M)
“Later in the fall, the ward mate in question reportedly stood too close or touched both boys and girls, but only after a big complaint from the girl, so now there’s a conspiracy of him doing that so that they can’t say he only targets girls.”
“Although [the girls] were disturbed by [the ward mate’s] actions, they did not wish to report it. I think it’s because they thought [the ward mate] would have huge repercussions.”
“It did not feel right to intervene and that it would be strange for me to do this alone … I would feel okay about it if I did it for the girls [if they asked me to].”
“I would take the victim’s point of view, but it was still borderline sexual harassment since the case would be lost in court. I felt burned out and saw a counselor about these situations. I would be very burned out if [the situations] repeat a lot. The support I’ve is okay for now [from the] Wellness Centre for emotional support.”
3.2.2. Coping Strategies in Response to the Difficult Dilemmas
Students’ Inaction in Dilemmas
[A student whose female ward mate received a comment about being transgender with breast augmentation surgery] “I would not report this personal attack because I’m a student and he’s a trained doctor; if I had a chance to work with him in the future, reporting the doctor might impact my career, and give other people the impression that ‘this guy is a whistle-blower,’ it leaves a bad reputation for him.”(Interview 1, M24, M)
[Situation in which the patient was unaware that the doctor was going to perform a per rectal exam after the vaginal exam] “The doctor was yelling at the students afterward, so there was the feeling that she wasn’t going to be kind to either patient or student, and the students didn’t speak up.”(Interview 9, M23, O)
“I don’t know when it’s disrespectful and what’s being too sensitive, but when I tell my friends, they are surprised by it.”(Interview 9, M23, O)
“A doctor was directly yelling at [my ward group], calling us stupid, but I was not sure if the doctor was being funny, judging by his tone, or felt superior and entitled to do so.”(Interview 5, M22, M)
“I would ask […] if she’s okay in private, but I would not confront the doctor, if the ward mates are not feeling okay then talk it out.”(Interview 1, M24, M)
[Students who were told to “jump out the window” by a doctor] “[My ward mates] didn’t get upset, but we talked about it and thought it was inappropriate.”(Interview 4, M24, M)
“You see so many of these [situations], so maybe it’s part of [medical] education.”(Interview 9, M23, O)
“This is how it is … but really? Is it even helpful? It did not help me remember [the material I was scolded for].”(Interview 8, M23, F)
Helplessness in the Hierarchical Health Care System
“It’s part of the culture. If you see someone do this, you will do it too; it’s quite convenient, but if a nurse were to ask me to sign to restrain a patient when I become a doctor, I would say no.”(Interview 5, M22, M)
“The hierarchy of the doctor being the one with the most authority is a big component [of why I went along with the physical exam]. It would have been awkward if I had said something.”(Interview 5, M22, M)
“I’m nobody; I cannot change this situation unless everyone has an awakening of conscience that restraining without proper reason is bad.”(Interview 6, M22, M)
Students’ Reflection on Uneasy Situations
“I don’t think I’ll burn out, but I will be more tactful when dealing with patients, try to be less blunt”(Interview 1, M24, M)
“It’s common to call them [patients] derogatory terms like “obese” to the point that I’m desensitized. I’m to some degree desensitized, but at the beginning, I was shocked. I would say it in the future as I’m desensitized now. As a friend, it’s not acceptable, but it’s accepted in the ward environment”(Interview 7, M23, F)
Practical Application of Knowledge Learned from Professionalism and Bioethics Classes
“To be honest, not much can be applied from the bioethics course. Usually what the doctor says from experience and practical advice is more helpful.”(Interview 5, M22, M)
“As a medical student, the four principles are less used, maybe when there is decision-making, e.g., when to admit what patient in the ICU; if there are not enough beds, then when to discharge patients, they would be more relevant.”(Interview 5 M22, M)
“[What is missing is] good role models, who will not call a patient ‘it’ and show you ‘this is how to make a patient comfortable.’ When they explicitly state these things and show that they prioritize warmth, people become more compassionate. A long-winded doctor will go through consent.”(Interview 8, M23, F)
4. Discussion
4.1. The Incongruity between Medical Education and Patient Care
4.2. Students’ Inaction in Professionalism Dilemmas
4.3. Sexually Inappropriate Remarks in Medical Education
5. Study Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wiggleton, C.; Petrusa, E.; Loomis, K.; Tarpley, J.; Tarpley, M.; O’Gorman, M.L.; Miller, B. Medical students’ experiences of moral distress: Development of a web-based survey. Acad. Med. 2010, 85, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Rees, C.E.; Monrouxe, L.V.; McDonald, L.A. Narrative, emotion and action: Analysing ‘most memorable’ professionalism dilemmas. Med. Educ. 2013, 47, 80–96. [Google Scholar] [CrossRef] [PubMed]
- Feudtner, C.; Christakis, D.A.; Christakis, N.A. Do clinical clerks suffer ethical erosion? Students’ perceptions of their ethical environment and personal development. Acad. Med. 1994, 69, 670–679. [Google Scholar] [CrossRef]
- D’eon, M.; Lear, N.; Turner, M.; Jones, C. Perils of the hidden curriculum revisited. Med. Teach. 2007, 29, 295–296. [Google Scholar] [CrossRef]
- Weurlander, M.; Lönn, A.; Seeberger, A.; Broberger, E.; Hult, H.; Wernerson, A. How do medical and nursing students experience emotional challenges during clinical placements? Int. J. Med. Educ. 2018, 9, 74–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monrouxe, L.V.; Rees, C.E.; Dennis, I.; Wells, S.E. Professionalism dilemmas, moral distress and the healthcare student: Insights from two online uk-wide questionnaire studies. BMJ Open 2015, 5, e007518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christakis, D.A.; Feudtner, C. Ethics in a short white coat: The ethical dilemmas that medical students confront. Acad. Med. 1993, 68, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Giannetta, N.; Villa, G.; Pennestrì, F.; Sala, R.; Mordacci, R.; Manara, D.F. Ethical problems and moral distress in primary care: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 7565. [Google Scholar] [CrossRef]
- Wilkinson, J.M. Moral distress in nursing practice: Experience and effect. Nurs. Forum 1987, 23, 16–29. [Google Scholar] [CrossRef]
- Morley, G.; Ives, J.; Bradbury-Jones, C.; Irvine, F. What is ‘moral distress’? A narrative synthesis of the literature. Nurs. Ethics 2019, 26, 646–662. [Google Scholar] [CrossRef] [Green Version]
- Corley, M.C.; Elswick, R.K.; Gorman, M.; Clor, T. Development and evaluation of a moral distress scale. J. Adv. Nurs. 2001, 33, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Benbassat, J.; Baumal, R.; Chan, S.; Nirel, N. Sources of distress during medical training and clinical practice: Suggestions for reducing their impact. Med. Teach. 2011, 33, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, J.R.; Bradley, E.H.; Holmboe, E.S.; Farrell, M.H.; Krumholz, H.M. Sources of ethical conflict in medical housestaff training: A qualitative study. Am. J. Med. 2004, 116, 402–407. [Google Scholar] [CrossRef]
- Salehi, P.P.; Jacobs, D.; Suhail-Sindhu, T.; Judson, B.L.; Azizzadeh, B.; Lee, Y.H. Consequences of medical hierarchy on medical students, residents, and medical education in otolaryngology. Otolaryngol. Head Neck Surg. 2020, 163, 906–914. [Google Scholar] [CrossRef]
- Perni, S.; Pollack, L.R.; Gonzalez, W.C.; Dzeng, E.; Baldwin, M.R. Moral distress and burnout in caring for older adults during medical school training. BMC Med. Educ. 2020, 20, 84. [Google Scholar] [CrossRef]
- McDonald, J.; Graves, J.; Abrahams, N.; Thorneycroft, R.; Hegazi, I. Moral judgement development during medical student clinical training. BMC Med. Educ. 2021, 21, 140. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, D.L.; Costa, M.; Helmich, E.; Jaarsma, D.; de Carvalho-Filho, M.A. ‘I found myself a despicable being!’: Medical students face disturbing moral dilemmas. Med. Educ. 2021, 55, 857–871. [Google Scholar] [CrossRef]
- Thurn, T.; Anneser, J. Medical students’ experiences of moral distress in end-of-life care. J. Palliat. Med. 2020, 23, 116–120. [Google Scholar] [CrossRef]
- Webster, G.; Francoise, E. Moral Residue. In Margin of Error: The Ethics of Mistakes in the Practice of Medicine; Rubin, S.B., Zoloth, L., Eds.; University Publishing Group: Hagerstown, MD, USA, 2000; pp. 217–230. Available online: http://hdl.handle.net/10822/931017 (accessed on 15 July 2022).
- Mareš, J. Moral distress: Terminology, theories and models. Kontakt 2016, 18, e137–e144. [Google Scholar] [CrossRef]
- Khan, M.W. Breach of confidentiality: Unintentional common practice due to misunderstanding and unawareness. Bangladesh J. Bioeth. 2011, 2, 16–18. [Google Scholar] [CrossRef]
- Yadav, H.; Jegasothy, R.; Ramakrishnappa, S.; Mohanraj, J.; Senan, P. Unethical behavior and professionalism among medical students in a private medical university in Malaysia. BMC Med. Educ. 2019, 19, 218. [Google Scholar] [CrossRef] [PubMed]
- Zafar, W. Moral experience and ethical challenges in an emergency department in Pakistan: Emergency physicians’ perspectives. Emerg. Med. J. 2015, 32, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Norman, N.B.M.; Soo, J.M.P.; Lam, M.Y.K.; Thirumoorthy, T. Unprofessional behavior of junior doctors: A retrospective analysis of outcomes by the Singapore medical council disciplinary tribunals. Singapore Med. J. 2021, 62, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Ngan, O.M.Y.; Sim, J.H. Evolution of bioethics education in the medical programme: A tale of two medical schools. Int. J. Ethics Educ. 2021, 6, 37–50. [Google Scholar] [CrossRef]
- Joynt, G.M.; Wong, W.T.; Ling, L.; Lee, A. Medical students and professionalism–do the hidden curriculum and current role models fail our future doctors? Med. Teach. 2018, 40, 395–399. [Google Scholar] [CrossRef]
- Creswell, J.; Clark, V.L.P.; Gutmann, M.L.; Hanson, W.E. Advanced mixed methods research designs. In Handbook of Mixed Methods in Social and Behavioral Research; Tashakkori, A., Teddlie, C., Eds.; Sage: Thousand Oaks, CA, USA, 2003; pp. 209–240. [Google Scholar]
- Lomis, K.D.; Carpenter, R.O.; Miller, B.M. Moral distress in the third year of medical school: A descriptive review of student case reflections. Am. J. Surg. 2009, 197, 107–112. [Google Scholar] [CrossRef]
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Kiger, M.E.; Varpio, L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med. Teach. 2020, 242, 846–854. [Google Scholar] [CrossRef]
- Medical Registration Ordinance (Chapter 161) Medical Registration (Amendment) Bill 2021 (fh cr 1/f/3261/92). Legislative Council Brief. Available online: https://www.legco.gov.hk/yr20-21/english/brief/fhcr1f326192_20210518-e.pdf (accessed on 10 June 2022).
- Hicks, L.K.; Lin, Y.; Robertson, D.W.; Robinson, D.L.; Woodrow, S.I. Understanding the clinical dilemmas that shape medical students’ ethical development: Questionnaire survey and focus group study. BMJ 2001, 322, 709–710. [Google Scholar] [CrossRef] [Green Version]
- Gaufberg, E.H.; Batalden, M.; Sands, R.; Bell, S.K. The hidden curriculum: What can we learn from third-year medical student narrative reflections? Acad. Med. 2010, 85, 1709–1716. [Google Scholar] [CrossRef]
- Riedel, P.L.; Kreh, A.; Kulcar, V.; Lieber, A.; Juen, B. A scoping review of moral stressors, moral distress and moral injury in healthcare workers during COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 1666. [Google Scholar] [CrossRef] [PubMed]
- Burston, A.S.; Tuckett, A.G. Moral distress in nursing: Contributing factors, outcomes and interventions. Nurs. Ethics 2013, 20, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Dyrbye, L.N.; Thomas, M.R.; Shanafelt, T.D. Medical student distress: Causes, consequences, and proposed solutions. Mayo Clin. Proc. 2005, 80, 1613–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stratta, E.C.; Riding, D.M.; Baker, P. Ethical erosion in newly qualified doctors: Perceptions of empathy decline. Int. J. Med. Educ. 2016, 7, 286. [Google Scholar] [CrossRef] [Green Version]
- Soemantri, D.; Greviana, N.; Findyartini, A.; Azzahra, T.B.; Suryoadji, K.A.; Mustika, R.; Felaza, E. “To obey or not to obey”—Medical students’ response towards professional dilemmas in a hierarchical and collectivist culture. PLoS ONE 2021, 16, e0261828. [Google Scholar] [CrossRef]
- Mavis, B.; Sousa, A.; Lipscomb, W.; Rappley, M.D. Learning about medical student mistreatment from responses to the medical school graduation questionnaire. Acad. Med. 2014, 89, 705–711. [Google Scholar] [CrossRef]
- Hsiao, C.J.; Akhavan, N.N.; Ospina, N.S.; Yagnik, K.J.; Neilan, P.; Hahn, P.; Zaidi, Z. Sexual harassment experiences across the academic medicine hierarchy. Cureus 2021, 13, e13508. [Google Scholar] [CrossRef]
- Phillips, S.P.; Webber, J.; Imbeau, S.; Quaife, T.; Hagan, D.; Maar, M.; Abourbih, J. Sexual harassment of Canadian medical students: A national survey. EClinicalMedicine 2019, 7, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Schoenefeld, E.; Marschall, B.; Paul, B.; Ahrens, H.; Sensmeier, J.; Coles, J.; Pfleiderer, B. Medical education too: Sexual harassment within the educational context of medicine—Insights of undergraduates. BMC Med. Educ. 2021, 21, 81. [Google Scholar] [CrossRef]
- McClain, T.S.; Kammer-Kerwick, M.; Wood, L.; Temple, J.R.; Busch-Armendariz, N. Sexual harassment among medical students: Prevalence, prediction, and correlated outcomes. Workplace Health Saf. 2021, 69, 257–267. [Google Scholar] [CrossRef]
- Jordan, C.E.; Combs, J.L.; Smith, G.T. An exploration of sexual victimisation and academic performance among college women. Trauma Violence Abuse 2014, 15, 191–200. [Google Scholar] [CrossRef] [PubMed]
- Stratton, T.D.; McLaughlin, M.A.; Witte, F.M.; Fosson, S.E.; Nora, L.M. Does students’ exposure to gender discrimination and sexual harassment in medical school affect specialty choice and residency program selection? Acad. Med. 2005, 80, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, C.D.; Bergen, M.R.; Korn, D. Impact of a program to diminish gender insensitivity and sexual harassment at a medical school. Acad. Med. 2000, 75, 464–469. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Themes | Descriptions | |
|---|---|---|
| Involvement in Care Perceived to be Substandard | ||
| 01 | Answered patients’ questions inadequately | The attending physician or resident answered patients’ questions inadequately, e.g., rushed through the consultation or simply ignored them |
| 02 | Gave incorrect or uncertain information on rounds | A member of my ward group/consulting team gave incorrect or uncertain information on rounds |
| 03 | Performed physical examinations on sedated/anaesthetized patients without consent | The consulting physician performed examinations on sedated or anaesthetized patients without their consent |
| 04 | Administered drug without consent | The consulting physician administered drugs without obtaining the patient’s consent |
| 05 | Failed to disclose a medical mistake to patients | An error was made in the care of a patient that was not fully or truthfully disclosed |
| Professionalism Lapses | ||
| 06 | Showed a lack of respect due to the hierarchical culture | A member of my ward group/consulting team was disrespectful to someone below himself or herself on the team ranking, e.g., student or other staff. (Disrespect defined as: receiving or witnessing covert, status-related abuse, verbal abuse, physical abuse, and ⁄ or harassment or discrimination, e.g., sexual, racial, religious, age, gender) |
| 07 | Bad-mouthed other services | Members of my ward group/consulting team “bad-mouthed” other services, e.g., other specialties, departments |
| 08 | Made demeaning remarks towards patients or family members | A member of my ward group/consulting team made disparaging or demeaning remarks about one of our patients or their family members. (Examples of “disparaging/demeaning remarks”: any kind of unnecessary judgment towards the patient, e.g., commenting on weight (“You’re too skinny/fat!”), commenting on behavior/lifestyle in a disparaging way (“Are you trying to kill yourself by [behavior]?” “Who raised you?”), commenting on the appearance in an unnecessary or unprofessional manner (“You look sickly.”) |
| 09 | Made sexually inappropriate remarks | A member of my ward group/consulting team made sexually inappropriate remarks about a patient, family member, other staff, or a student, e.g., flirting, giving inappropriate comments about physical appearance |
| 10 | Inappropriately touched someone in a way that is not part of the medical procedure | A member of my ward group/consulting team touched a patient, family member, other staff, or a student inappropriately, i.e., not as a part of any necessary medical procedure |
| 11 | Acted disrespectfully to a nursing or ancillary staff | A member of my ward group/consulting team was disrespectful to the nursing and/or ancillary staff |
| 12 | Misrepresented my experience to patients | A senior doctor misrepresented the degree of my experience in performing a procedure to the patient |
| 13 | Discussed confidential information in inappropriate settings | Members of my ward group/consulting team discussed confidential information about the patient in an inappropriate setting, e.g., public spaces, with friends or family, on social media, or messaging apps |
| Responsibility Exceeding Students’ Capabilities | ||
| 14 | Disagreed with a treatment but a senior doctor insisted on it | My ward group/team went along with a treatment that we did not believe was indicated, because a senior doctor insisted on it |
| 15 | Continued to provide therapy although it only prolonged patients’ suffering | I witnessed that staff/my consulting team continued to provide therapy, even though I thought it only prolonged the patient’s suffering |
| 16 | Continued life support, although it was not what the patient would have wanted | I witnessed that staff/my consulting team continued life support, even though I thought it was not what the patient would have wanted |
| 17 | Withdrew life support at patients’ or families’ request | I witnessed that staff/my consulting team withdrew life support at the patient’s or family’s request, even though I thought the patient could have survived with continued treatment |
| 18 | Felt pressured to perform examinations that students felt unqualified to perform | I performed a procedure that I did not feel qualified to do because I was afraid of being perceived as incompetent or I felt pressured by a senior doctor |
| 19 | Withheld information as it fell outside students’ current capabilities | I withheld information from a patient who requested it because I felt it was not my responsibility or place to provide it |
| 20 | Made a false promise to a patient coming back to talk to him/her | I promised one of my patients that someone would come back to speak to him or her, even though I was not sure it would actually happen |
| 21 | A patient who lives alone was discharged before I thought it was medically safe | A patient was discharged before I thought it was medically safe because there was no one at home to care for the patient |
| 22 | Failed to report superiors’ inappropriate act | One of my superiors behaved inappropriately, but I did not report it because I was afraid of negative consequences, e.g., it would affect my evaluation, or because I was not confident that I was right |
| 23 | Felt pressured to perform examinations on incompetent patients | I performed examinations on a patient who was incompetent (e.g., a minor, sedated, or had a mental disorder) because I felt pressured by a senior doctor |
| System Constraints | ||
| 24 | Poor communication between teams | Poor communication between multiple consulting teams that negatively affected his or her care |
| 25 | Suboptimal care due to delays in the test procedure | Delays occurred in the performance of tests or procedures, or the return of laboratory data or radiology reports because of scheduling problems or lost requests. Such delays resulted in suboptimal patient care |
| 26 | Failed to deliver optimal care due to language barriers | Optimal care was not provided to one of my patients (e.g., ethnic minorities) because of language barriers |
| 27 | Patients presented with very advanced disease due to barriers to accessing care | A patient presented with a very advanced disease because he or she faced barriers to accessing care |
| 28 | Optimal care was not provided due to stigmatizing social circumstances | Optimal care was not provided to a patient as a result of stigmatizing social circumstances or conditions (e.g., age, alcoholism, drug abuse, homelessness, religion, or obesity) |
| 29 | Fragmented care over the course of the patient’s hospitalization | Over the course of a patient’s hospitalization or long-term treatment, he or she was cared for by multiple doctors and services, which led to fragmented, discontinuous care. E.g., Roles were not explained adequately, or the patient had to explain their condition repeatedly |
| 30 | Patient received suboptimal care due to busy ward | Suboptimal care was provided to a patient because my ward group/consulting team was too tired and overworked |
| Questions |
|---|
|
| Demographics | n (%) |
|---|---|
| Class Year | |
| Year 4 | 19 (12.4%) |
| Year 5 | 8 (5.23%) |
| Year 6 | 126 (82.4%) |
| Gender | |
| Female | 81 (52.9%) |
| Male | 68 (44.4%) |
| Non-binary | 2 (1.3%) |
| I prefer not to say | 2 (1.3%) |
| Age | |
| Mean | 23.5 |
| Range | 20–31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, C.; Ko, W.Y.K.; Ngan, O.M.Y.; Wong, W.T. Exploring Professionalism Dilemma and Moral Distress through Medical Students’ Eyes: A Mixed-Method Study. Int. J. Environ. Res. Public Health 2022, 19, 10487. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191710487
Cho C, Ko WYK, Ngan OMY, Wong WT. Exploring Professionalism Dilemma and Moral Distress through Medical Students’ Eyes: A Mixed-Method Study. International Journal of Environmental Research and Public Health. 2022; 19(17):10487. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191710487
Chicago/Turabian StyleCho, Cordelia, Wendy Y. K. Ko, Olivia M. Y. Ngan, and Wai Tat Wong. 2022. "Exploring Professionalism Dilemma and Moral Distress through Medical Students’ Eyes: A Mixed-Method Study" International Journal of Environmental Research and Public Health 19, no. 17: 10487. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191710487