
The Potential Impact of a Public Health Approach to Improving the Physical Health of People Living with Mental Illness
 , ,
, ,
Abstract
:1. Introduction
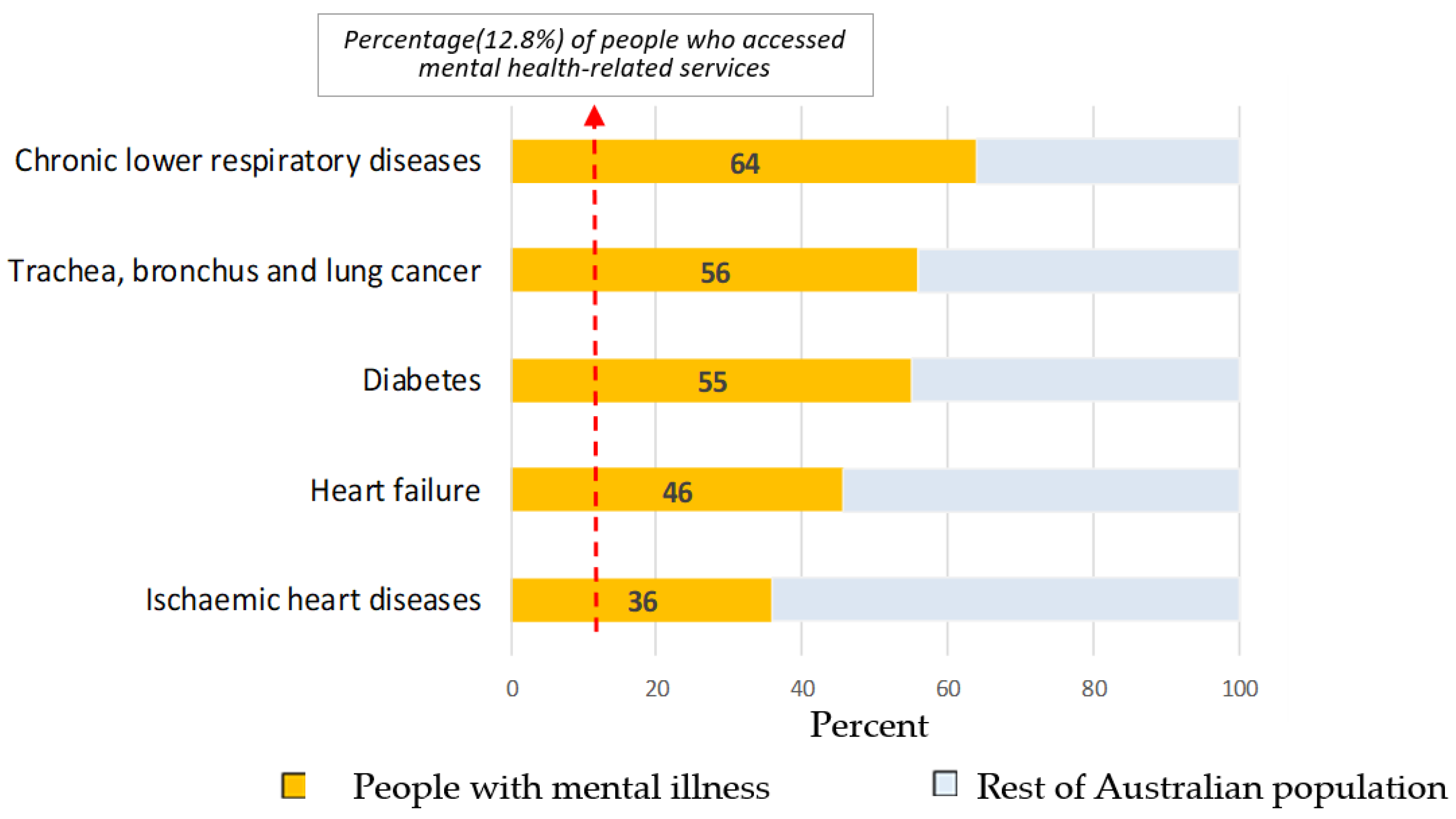
2. Increasing Disparities in Health Service Access
2.1. Heart Disease
2.2. Cancer
2.3. Infectious Diseases and Vaccine Preventable Conditions
2.4. Smoking
3. Social Health, Physical Health and Mental Health
3.1. Social Isolation, Mental Illness and Early Mortality
3.2. Increased Social Disadvantage
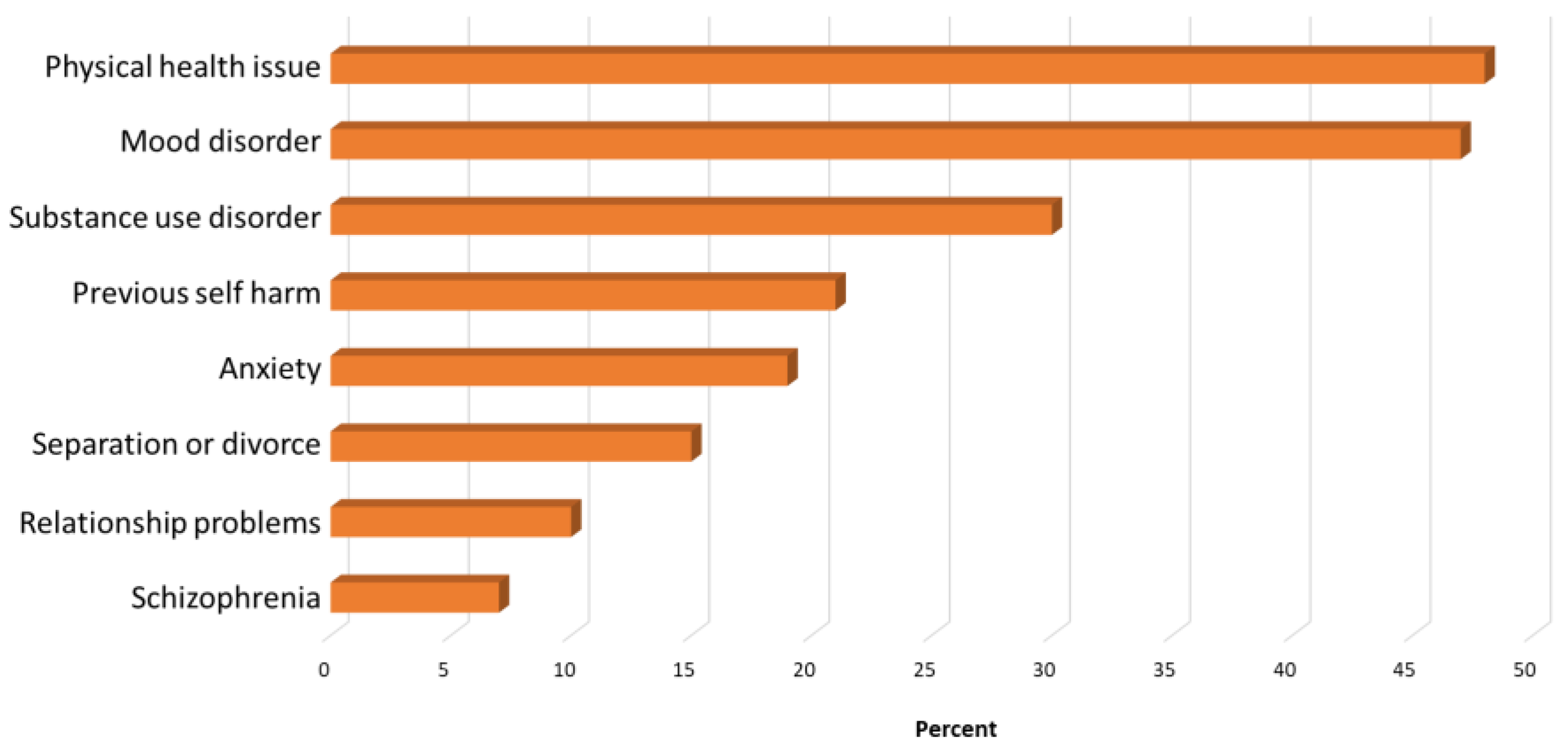
3.3. Physical Health, Mental Illness and Suicidality
4. Estimating Public Health Intervention Impact
4.1. Cancer and Cardiovascular Disease
4.2. Smoking Cessation and Vaccination
5. Discussion
5.1. Policy and Practice Opportunities for Change
5.2. Implications
- People living with severe mental illness should be included as a high-risk group with increased health vulnerabilities requiring targeted screening and treatment for high-risk chronic health conditions, particularly:
- ○
- Cancer;
- ○
- Cardiovascular disease (see for example, the New Zealand, Cardiovascular Disease Risk Assessment and Management for Primary Care guidelines which recommend screening for people with severe mental illness over the age of 25 years) [59];
- ○
- Respiratory disease;
- ○
- Diabetes.
- People living with severe mental illness should be provided with subsidized access to all major approved vaccines (in addition to COVID-19 vaccines)
- People living with mental illness should have subsidized access to smoking cessation support, including nicotine replacement therapy
- Increased support for telehealth follow-up of people living with severe mental illness and chronic physical health conditions, especially for older persons with mental illness.
5.3. Conclusions and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roberts, R. Equally Well. In Physical Health and Mental Illness. A Narrative Literature Review; National Mental Health Commission, Charles Sturt University: Bathurst, NSW, Australia, 2019. [Google Scholar]
- Australian Bureau of Statistics. Mortality of People Using Mental Health Services and Prescription Medications, Analysis of 2011 Data; ABS: Canberra, ACT, Australia, 2017.
- Momen, N.C.; Plana-Ripoll, O.; Agerbo, E.; Benros, M.E.; Børglum, A.D.; Christensen, M.K.; Dalsgaard, S.; Degenhardt, L.; de Jonge, P.; Debost, J.-C.P. Association between mental disorders and subsequent medical conditions. N. Engl. J. Med. 2020, 382, 1721–1731. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.E.; Adab, P.; Cheng, K.K. COVID-19: Risk factors for severe disease and death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. National Health Survey: Mental Health and Co-Existing Physical Health Conditions, Australia, 2014–2015; ABS: Canberra, ACT, Australia, 2016.
- Sara, G.; Arumuganathan, M.; Chen, W.; Wu, F.; Currow, D.; Large, M.; Mulder, C.; Ramanuj, P.P.; Burgess, P.M. Cohort profile: Mental Health Living Longer: A population-wide data linkage to understand and reduce premature mortality in mental health service users in New South Wales, Australia. BMJ Open 2019, 9, e033588. [Google Scholar] [CrossRef]
- Lawrence, D.; Hancock, K.J.; Kisely, S. The gap in life expectancy from preventable physical illness in psychiatric patients in Western Australia: Retrospective analysis of population based registers. BMJ 2013, 346, f2539. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, L.; Kois, L.E.; Chen, C.; López-Aybar, L.; McCullough, B.; McLaughlin, K.J. Reliability of the Term “Serious Mental Illness”: A Systematic Review. Psychiatr. Serv. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zumstein, N.; Riese, F. Defining severe and persistent mental illness—A pragmatic utility concept analysis. Front. Psychiatr. 2020, 11, 648. [Google Scholar] [CrossRef]
- Chesney, E.; Goodwin, G.M.; Fazel, S. Risks of all—Cause and suicide mortality in mental disorders: A meta review. World Psychiatr. 2014, 13, 153–160. [Google Scholar] [CrossRef]
- Lorenz, R.A.; Norris, M.M.; Norton, L.C.; Westrick, S.C. Factors associated with influenza vaccination decisions among patients with mental illness. Int. J. Psychiatr. Med. 2013, 46, 1–13. [Google Scholar] [CrossRef]
- Sara, G.; Chen, W.; Large, M.; Ramanuj, P.; Curtis, J.; McMillan, F.; Mulder, C.; Currow, D.; Burgess, P. Potentially preventable hospitalisations for physical health conditions in community mental health service users: A population-wide linkage study. Epidemiol. Psychiatr. Sci. 2021, 30, e22. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Das, S.; Young-Wolff, K.C. Smoking, Mental Illness, and Public Health. Ann. Rev. Public Health 2017, 38, 165–185. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.; Broughan, J.; Crowley, D.; O’Kelly, B.; Fawsitt, R.; Burke, M.C.; McCombe, G.; Lambert, J.S.; Cullen, W. COVID-19’s impact on primary care and related mitigation strategies: A scoping review. Eur. J. Gen. Prac. 2021, 27, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Priester, M.; Browne, T.; Iachini, A.; Clone, S.; DeHart, D.; Seay, K. Treatment Access Barriers and Disparities Among Individuals with Co-Occurring Mental Health and Substance Use Disorders: An Integrative Literature Review. J. Subst. Abuse Treat. 2016, 61, 47–59. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Parker, C.; Coupland, C.; Vinogradova, Y. Inequalities in the primary care of patients with coronary heart disease and serious mental health problems: A cross-sectional study. Heart 2007, 93, 1256. [Google Scholar] [CrossRef] [PubMed]
- Einstein, A.J.; Shaw, L.J.; Hirschfeld, C.; Williams, M.C.; Villines, T.C.; Better, N.; Vitola, J.V.; Cerci, R.; Dorbala, S.; Raggi, P. International impact of COVID-19 on the diagnosis of heart disease. J. Am. Coll. Cardiol. 2021, 77, 173–185. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, R.; Poppe, K.; Peterson, D.; Every-Palmer, S.; Soosay, I.; Jackson, R. Prediction of cardiovascular disease risk among people with severe mental illness: A cohort study. PLoS ONE 2019, 14, e0221521. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Causes of Death, Australia. 2021. Available online: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/latest-release (accessed on 4 May 2022).
- Nielsen, R.E.; Banner, J.; Jensen, S.E. Cardiovascular disease in patients with severe mental illness. Nat. Rev. Cardiol. 2021, 18, 136–145. [Google Scholar] [CrossRef]
- Laursen, T.M.; Nordentoft, M. Heart disease treatment and mortality in schizophrenia and bipolar disorder–changes in the Danish population between 1994 and 2006. J. Psychiatr. Res. 2011, 45, 29–35. [Google Scholar] [CrossRef]
- Kisely, S.; Forsyth, S.; Lawrence, D. Why do psychiatric patients have higher cancer mortality rates when cancer incidence is the same or lower? Aust. N. Z. J. Psychiatr. 2016, 50, 254–263. [Google Scholar] [CrossRef]
- Solmi, M.; Firth, J.; Miola, A.; Fornaro, M.; Frison, E.; Fusar-Poli, P.; Dragioti, E.; Shin, J.I.; Carvalho, A.F.; Stubbs, B. Disparities in cancer screening in people with mental illness across the world versus the general population: Prevalence and comparative meta-analysis including 4 717 839 people. Lancet Psychiatr. 2020, 7, 52–63. [Google Scholar] [CrossRef]
- Tuesley, K.M.; Jordan, S.J.; Siskind, D.J.; Kendall, B.J.; Kisely, S. Colorectal, cervical and prostate cancer screening in Australians with severe mental illness: Retrospective nation-wide cohort study. Aust. N. Z. J. Psychiatr. 2019, 53, 550–558. [Google Scholar] [CrossRef]
- Fedewa, S.A.; Star, J.; Bandi, P.; Minihan, A.; Han, X.; Yabroff, K.R.; Jemal, A. Changes in Cancer Screening in the US During the COVID-19 Pandemic. JAMA Netw. Open 2022, 5, e2215490. [Google Scholar] [CrossRef] [PubMed]
- Duffy, S.W.; Seedat, F.; Kearins, O.; Press, M.; Walton, J.; Myles, J.; Vulkan, D.; Sharma, N.; Mackie, A. The projected impact of the COVID-19 lockdown on breast cancer deaths in England due to the cessation of population screening: A national estimation. Br. J. Cancer 2022, 126, 1355–1361. [Google Scholar] [CrossRef]
- Control, C.f.D. Prevention. Hepatitis B vaccination coverage among adults--United States, 2004. MMWR. Morb. Mortal. Wkly. Rep. 2006, 55, 509–511. [Google Scholar]
- Lewis, K.J.S.; Lewis, C.; Roberts, A.; Richards, N.A.; Evison, C.; Pearce, H.A.; Lloyd, K.; Meudell, A.; Edwards, B.M.; Robinson, C.A.; et al. The effect of the COVID-19 pandemic on mental health in individuals with pre-existing mental illness. BJPsych Open 2022, 8, e59. [Google Scholar] [CrossRef] [PubMed]
- Fekadu, A.; Medhin, G.; Kebede, D.; Alem, A.; Cleare, A.J.; Prince, M.; Hanlon, C.; Shibre, T. Excess mortality in severe mental illness: 10-year population-based cohort study in rural Ethiopia. Br. J. Psychiatr. 2015, 206, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Pandemic Insights into Australian Smokers, 2020–2021; ABS: Canberra, ACT, Australia, 2022.
- Lawrence, D.; Mitrou, F.; Zubrick, S.R. Smoking and mental illness: Results from population surveys in Australia and the United States. BMC Public Health 2009, 9, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18, 20. [Google Scholar] [CrossRef]
- Richter, D.; Hoffmann, H. Social exclusion of people with severe mental illness in Switzerland: Results from the Swiss Health Survey. Epidemiol. Psychiatr. Sci. 2019, 28, 427–435. [Google Scholar] [CrossRef]
- Mann, F.; Wang, J.; Pearce, E.; Ma, R.; Schleif, M.; Lloyd-Evans, B.; Johnson, S. Loneliness and the onset of new mental health problems in the general population: A systematic review. MedRxiv 2021. [CrossRef]
- Rico-Uribe, L.A.; Caballero, F.F.; Martin-Maria, N.; Cabello, M.; Ayuso-Mateos, J.L.; Miret, M. Association of loneliness with all-cause mortality: A meta-analysis. PLoS ONE 2018, 13, e0190033. [Google Scholar] [CrossRef]
- Dahlberg, L.; McKee, K.J.; Frank, A.; Naseer, M. A systematic review of longitudinal risk factors for loneliness in older adults. Aging Ment. Health 2022, 26, 225–249. [Google Scholar] [CrossRef] [PubMed]
- Marmot, M. Recreating Society for Better Health. American Public Health Association: Washington, DC, USA, 2022. [Google Scholar]
- Marmot, M. Health equity in England: The Marmot review 10 years on. BMJ 2020, 368, m693. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.; Marmot, M. Social Determinants and Mental Health; Oxford University Press: Oxford, UK, 2022; p. 171. [Google Scholar]
- Australian Bureau of Statistics. Causes of Death Australia 2017 Intentional Self-Harm Key Characteristics; ABS: Canberra, ACT, Australia, 2018.
- Australian Bureau of Statistics. Psychosocial Risk Factors as They Relate to Coroner-Referred Deaths in Australia 2017; ABS: Canberra, ACT, Australia, 2019.
- Productivity Commission. Mental Health Inquiry Report; Commonwealth of Australia: Canberra, ACT, Australia, 2020. [Google Scholar]
- McNamara, B.J.; Banks, E.; Gubhaju, L.; Joshy, G.; Williamson, A.; Raphael, B.; Eades, S. Factors relating to high psychological distress in Indigenous Australians and their contribution to Indigenous-non-Indigenous disparities. Aust. N. Z. J. Public Health 2018, 42, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Braam, A.W.; Prince, M.J.; Beekman, A.T.; Delespaul, P.; Dewey, M.E.; Geerlings, S.; Kivelä, S.-L.; Lawlor, B.; Magnússon, H.; Meller, I. Physical health and depressive symptoms in older Europeans: Results from EURODEP. Br. J. Psychiatr. 2005, 187, 35–42. [Google Scholar] [CrossRef]
- Erlangsen, A.; Vach, W.; Jeune, B. The effect of hospitalization with medical illnesses on the suicide risk in the oldest old: A population-based register study. J. Am. Geriatr. Soc. 2005, 53, 771–776. [Google Scholar] [CrossRef]
- Skivington, K.; Matthews, L.; Simpson, S.A.; Craig, P.; Baird, J.; Blazeby, J.M.; Boyd, K.A.; Craig, N.; French, D.P.; McIntosh, E.; et al. A new framework for developing and evaluating complex interventions: Update of Medical Research Council guidance. BMJ 2021, 374, n2061. [Google Scholar] [CrossRef]
- Barreto, M.L. Efficacy, effectiveness, and the evaluation of public health interventions. BMJ 2005, 59, 342–345. [Google Scholar] [CrossRef]
- Lawrence, D.; Coghlan, R. Health inequalities and the health needs of people with mental illness. N. S. W. Public Health Bull. 2002, 13, 155–158. [Google Scholar] [CrossRef]
- Chou, R.; Cantor, A.; Dana, T.; Wagner, J.; Ahmed, A.Y.; Fu, R.; Ferencik, M. Statin use for the primary prevention of cardiovascular dis-ease in adults: Updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2022, 328, 754–771. [Google Scholar] [CrossRef]
- Access Economics. Smoking and Mental Illness: Costs; SANE Australia: Canberra, ACT, Australia, 2007. [Google Scholar]
- Australian Institute of Health and Welfare. Australian Burden of Disease Study: Impact and Causes of Illness and Death in Australia 2015—Summary Report; AIHW: Canberra, ACT, Australia, 2019.
- Queensland Health. Cardiovascular Disease. Report of the Chief Health Officer. Brisbane, Qld: Qld Health. 2017. Available online: https://www.health.qld.gov.au/__data/assets/pdf_file/0031/644854/cardiovascular-disease-factsheet.pdf (accessed on 17 June 2022).
- Liu, N.; Daumit, G.; Dua, T.; Aquila, R.; Charlson, F.; Cuijpers, P.; Druss, B.; Dudek, K.; Freeman, M.; Fujii, C.; et al. Excess mortality in persons with severe mental disorders: A multilevel intervention framework and priorities for clinical practice, policy and research agendas. World Psychiatr. 2017, 16, 30–40. [Google Scholar] [CrossRef]
- Firth, J.; Siddiqi, N.; Koyanagi, A.; Siskind, D.; Rosenbaum, S.; Galletly, C.; Allan, S.; Caneo, C.; Carney, R.; Carvalho, A.F.; et al. The Lancet Psychiatry Commission: A blueprint for protecting physical health in people with mental illness. Lancet Psychiatr. 2019, 6, 675–712. [Google Scholar] [CrossRef] [Green Version]
- Walker, E.; McGee, R.; Druss, B. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatr. 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Desborough, J.; Hall, S.L.; de Toca, L.; Davis, S.; Roberts, L.; Kelaher, C.; Kidd, M. Australia’s National COVID-19 Primary Care Response. Med. J. Aust. 2020, 213, 104–106.e101. [Google Scholar] [CrossRef] [PubMed]
- Australian Government. National Mental Health and Wellbeing Pandemic Response Plan; Australian Government: Canberra, ACT, Australia, 2020; Volume 2020.
- Morgan, M.; Peters, D.; Hopwood, M.; Castle, D.; May, C.; Fehily, C.; Sharma, A.; Rocks, T.; McNamara, K.; Cobb, L.; et al. Being Equally Well. A National Policy Roadmap to Better Physical Health Care and Longer Lives for People Living with Serious Mental Illness; Victoria University: Melbourne, VIC, Australia, 2021. [Google Scholar]
- Ministry of Health. Cardiovascular Disease Risk Assessment and Management for Primary Care; Ministry of Health: Wellington, New Zealand, 2018.
- National Mental Health Commission. Equally Well Consensus Statement. Improving the Physical Health and Wellbeing of People Living with Mental Illness in Australia; NMHC: Washington, DC, USA, 2016.




{kind=link}
{kind=link}
{kind=link}
| Underlying Cause of Death | Mental Illness | Rest of Population | Total Population | |||
|---|---|---|---|---|---|---|
| No. | Row % | No. | Row % | No. | Row % | |
| Trachea, bronchus, and lung cancer | 2567 | 56 | 2031 | 44 | 4598 | 100 |
| Colon, sigmoid, rectum and anus cancer | 1064 | 51 | 1018 | 49 | 2082 | 100 |
| Breast cancer | 1012 | 56 | 785 | 44 | 1797 | 100 |
| Blood and lymph cancer | 895 | 51 | 876 | 49 | 1771 | 100 |
| Prostate cancer | 523 | 61 | 332 | 39 | 856 | 100 |
| Total cancer caused deaths | 6061 | 55 | 5042 | 45 | 11,103 | 100 |
| 0 | 0 | |||||
| Total number accessing MBS/PBS | 2.8 Mil | 12 | 21.5 Mil | 88 | 24.3 Mil | 100 |
| Annual Deaths per 100 k | Annual Deaths per 100 k | Annual Deaths per 100 k | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Preventable | Preventable | Preventable | |||||||
| Intervention Efficacy | Total CVD, Cancer & Respiratory Disease | 69% | 38% * | Total Top 10 Causes (Excl. Suicide) | 69% | 38% * | Total All Causes | 69% | 38% * |
| 330 | 231.12 | 125.47 | 369 | 258.38 | 140.27 | 827 | 578.60 | 314.10 | |
| 25% | 57.78 | 31.37 | 64.60 | 35.07 | 144.65 | 78.52 | |||
| 10% | 23.11 | 12.55 | 25.84 | 14.03 | 57.86 | 31.41 | |||
| 5% | 11.56 | 6.27 | 12.92 | 7.01 | 28.93 | 15.70 | |||
| 1% | 2.31 | 1.25 | 2.58 | 1.40 | 5.79 | 3.14 | |||
| 0.1% | 0.23 | 0.13 | 0.26 | 0.14 | 0.58 | 0.31 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roberts, R.; Johnson, C.; Hopwood, M.; Firth, J.; Jackson, K.; Sara, G.; Allan, J.; Calder, R.; Manger, S. The Potential Impact of a Public Health Approach to Improving the Physical Health of People Living with Mental Illness. Int. J. Environ. Res. Public Health 2022, 19, 11746. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191811746
Roberts R, Johnson C, Hopwood M, Firth J, Jackson K, Sara G, Allan J, Calder R, Manger S. The Potential Impact of a Public Health Approach to Improving the Physical Health of People Living with Mental Illness. International Journal of Environmental Research and Public Health. 2022; 19(18):11746. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191811746
Chicago/Turabian StyleRoberts, Russell, Caroline Johnson, Malcolm Hopwood, Joseph Firth, Kate Jackson, Grant Sara, John Allan, Rosemary Calder, and Sam Manger. 2022. "The Potential Impact of a Public Health Approach to Improving the Physical Health of People Living with Mental Illness" International Journal of Environmental Research and Public Health 19, no. 18: 11746. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191811746