
An Evidence-Based Somatic Acupressure Intervention Protocol for Managing the Breast Cancer Fatigue-Sleep Disturbance-Depression Symptom Cluster: Development and Validation following the Medical Research Council Framework
 ,
,
Abstract
:1. Background
2. Methods
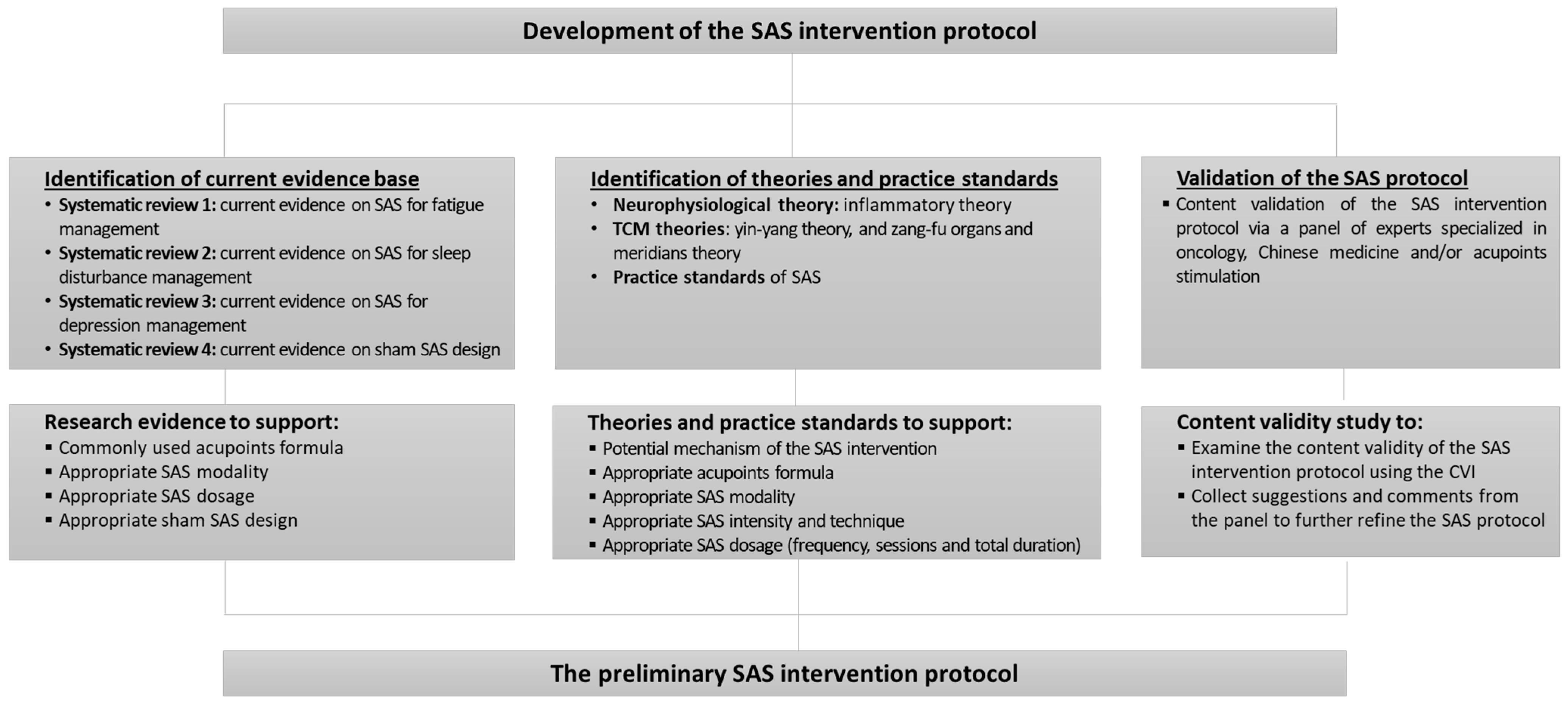
2.1. Study Design
2.2. Study Procedures in Developing and Validating the SAS Intervention Protocol
2.2.1. Identification of Existing Research Evidence Base
2.2.2. Identification of Relevant Theories and Practice Standards
2.2.3. Validation of the SAS Intervention Protocol
3. Results
3.1. True SAS Intervention Protocol
3.1.1. Selecting Appropriate SAS Intervention and Acupoints Formula
3.1.2. Selecting Appropriate SAS Modality
3.1.3. Identifying Appropriate SAS Intensity and Technique
3.1.4. Identifying Appropriate SAS Dosage
3.2. Protocol of the Placebo SAS Intervention
3.2.1. Identifying Appropriate Placebo Acupoints
3.2.2. Identifying Appropriate Placebo SAS Intensity, Technique, Frequency, Session and Total Duration
3.3. Content Validity of the SAS Intervention Protocol
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SAS | Somatic acupoint stimulation |
| FSDSC | Fatigue-Sleep Disturbance-Depression Symptom Cluster |
| BCS | Breast Cancer Survivors |
| RCT | Randomized Control Trial |
| CVI | Content Validity Index |
| MRC framework | Medical Research Council Framework for Developing and Evaluating Complex Intervention |
| CBT | Cognitive Behavioural Therapy |
References
- Berger, A.M.; Mooney, K.; Alvarez-Perez, A.; Breitbart, W.S.; Carpenter, K.M.; Cella, D.; Cleeland, C.; Dotan, E.; Eisenberger, M.A.; Jacobsen, P.B.; et al. Cancer-related fatigue, version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 1012–1039. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Ganz, P.A.; Irwin, M.R.; Kwan, L.; Breen, E.C.; Cole, S.W. Inflammation and Behavioral Symptoms After Breast Cancer Treatment: Do Fatigue, Depression, and Sleep Disturbance Share a Common Underlying Mechanism? J. Clin. Oncol. 2011, 29, 3517–3522. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Fiorentino, L.; Natarajan, L.; Parker, B.A.; Mills, P.J.; Sadler, G.R.; Dimsdale, J.E.; Rissling, M.; He, F.; Ancoli-Israel, S. Pre-treatment symptom cluster in breast cancer patients is associated with worse sleep, fatigue and depression during chemotherapy. Psycho-Oncol. J. Psychol. Soc. Behav. Dimens. Cancer 2009, 18, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Peoples, A.R.; Roscoe, J.A.; Block, R.C.; Heckler, C.E.; Ryan, J.L.; Mustian, K.M.; Janelsins, M.C.; Peppone, L.J.; Moore, D.F.; Coles, C.; et al. Nausea and disturbed sleep as predictors of cancer-related fatigue in breast cancer patients: A multicenter NCORP study. Support. Care Cancer 2017, 25, 1271–1278. [Google Scholar] [CrossRef] [PubMed]
- Accortt, E.E.; Bower, J.E.; Stanton, A.L.; Ganz, P.A. Depression and vasomotor symptoms in young breast cancer survivors: The mediating role of sleep disturbance. Arch. Womens Ment. Health 2015, 18, 565–568. [Google Scholar] [CrossRef]
- Colagiuri, B.; Christensen, S.; Jensen, A.B.; Price, M.A.; Butow, P.N.; Zachariae, R. Prevalence and Predictors of Sleep Difficulty in a National Cohort of Women with Primary Breast Cancer Three to Four Months Postsurgery. J. Pain Symptom Manag. 2011, 42, 710–720. [Google Scholar] [CrossRef]
- Reinertsen, K.V.; Engebraaten, O.; Loge, J.H.; Cvancarova, M.; Naume, B.; Wist, E.; Edvardsen, H.; Wille, E.; Bjøro, T.; Kiserud, C.E. Fatigue During and After Breast Cancer Therapy—A Prospective Study. J. Pain Symptom Manag. 2017, 53, 551–560. [Google Scholar] [CrossRef]
- Ho, S.-Y.; Rohan, K.J.; Parent, J.; Tager, F.A.; McKinley, P.S. A Longitudinal Study of Depression, Fatigue, and Sleep Disturbances as a Symptom Cluster in Women with Breast Cancer. J. Pain Symptom Manag. 2015, 49, 707–715. [Google Scholar] [CrossRef]
- Dodd, M.J.; Miaskowski, C.; Paul, S.M. Symptom clusters and their effect on the functional status of patients with cancer. Oncol. Nurs. Forum 2001, 28, 465–470. [Google Scholar]
- Trudel-Fitzgerald, C.; Savard, J.; Ivers, H. Which Symptoms Come First? Exploration of Temporal Relationships Between Cancer-Related Symptoms over an 18-Month Period. Ann. Behav. Med. 2013, 45, 329–337. [Google Scholar] [CrossRef]
- Bower, J.E. Cancer-related fatigue—mechanisms, risk factors, and treatments. Nat. Rev. Clin. Oncol. 2014, 11, 597–609. [Google Scholar] [CrossRef] [PubMed]
- Dodd, M.J.; Cho, M.H.; Cooper, B.A.; Miaskowski, C. The effect of symptom clusters on functional status and quality of life in women with breast cancer. Eur. J. Oncol. Nurs. 2010, 14, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, L.; Rissling, M.; Liu, L.; Ancoli-Israel, S. The symptom cluster of sleep, fatigue and depressive symptoms in breast cancer patients: Severity of the problem and treatment options. Drug Discov. Today Dis. Model. 2011, 8, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Induru, R.R.; Walsh, D. Cancer-related sleep disturbance. Am. J. Hosp. Palliat. Med. 2014, 31, 777–785. [Google Scholar] [CrossRef] [PubMed]
- Sanford, S.D.; Beaumont, J.L.; Butt, Z.; Sweet, J.J.; Cella, D.; Wagner, L.I. Prospective Longitudinal Evaluation of a Symptom Cluster in Breast Cancer. J. Pain Symptom Manag. 2014, 47, 721–730. [Google Scholar] [CrossRef]
- Hansen, M.V.; Andersen, L.T.; Madsen, M.T.; Hageman, I.; Rasmussen, L.S.; Bokmand, S.; Rosenberg, J.; Gögenur, I. Effect of melatonin on depressive symptoms and anxiety in patients undergoing breast cancer surgery: A randomized, double-blind, placebo-controlled trial. Breast Cancer Res. Treat. 2014, 145, 683–695. [Google Scholar] [CrossRef]
- Li, M.; Fitzgerald, P.; Rodin, G. Evidence-Based Treatment of Depression in Patients with Cancer. J. Clin. Oncol. 2012, 30, 1187–1196. [Google Scholar] [CrossRef]
- Bower, J.E. Behavioral symptoms in breast cancer patients and survivors: Fatigue, insomnia, depression, and cognitive disturbance. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2008, 26, 768–777. [Google Scholar] [CrossRef]
- Waldron, D.L.; Bramble, D.; Gringras, P. Melatonin: Prescribing practices and adverse events. Arch. Dis. Child. 2005, 90, 1206–1207. [Google Scholar] [CrossRef]
- Haddad, N.E.; Palesh, O. Acupuncture in the treatment of cancer-related psychological symptoms. Integr. Cancer Ther. 2014, 13, 371–385. [Google Scholar] [CrossRef]
- Johnson, J.A.; Rash, J.A.; Campbell, T.S.; Savard, J.; Gehrman, P.R.; Perlis, M.; Carlson, L.E.; Garland, S.N. A systematic review and meta-analysis of randomized controlled trials of cognitive behavior therapy for insomnia (CBT-I) in cancer survivors. Sleep Med. Rev. 2016, 27, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Choi, T.-Y.; Kim, J.I.; Lim, H.-J.; Lee, M.S. Acupuncture for Managing Cancer-Related Insomnia: A Systematic Review of Randomized Clinical Trials. Integr. Cancer Ther. 2017, 16, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Finnegan-John, J.; Molassiotis, A.; Richardson, A.; Ream, E. A systematic review of complementary and alternative medicine interventions for the management of cancer-related fatigue. Integr. Cancer Ther. 2013, 12, 276–290. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.V.R.; Uma, M. Effectiveness of Acupressure on improving the Quality of Sleep among Cancer Patients. Asian J. Nurs. Educ. Res. 2015, 5, 513. [Google Scholar] [CrossRef]
- Wang, T.; Deng, R.; Tan, J.-Y.; Guan, F.-G. Acupoints Stimulation for Anxiety and Depression in Cancer Patients: A Quantitative Synthesis of Randomized Controlled Trials. Evid.-Based Complement. Altern. Med. 2016, 2016, 5645632. [Google Scholar] [CrossRef]
- Zick, S.M.; Sen, A.; Wyatt, G.K.; Murphy, S.L.; Arnedt, J.T.; Harris, R.E. Investigation of 2 types of self-administered acupressure for persistent cancer-related fatigue in breast cancer survivors: A randomized clinical trial. Jama Oncol. 2016, 2, 1470–1476. [Google Scholar] [CrossRef]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef]
- Zick, S.M.; Alrawi, S.; Merel, G.; Burris, B.; Sen, A.; Litzinger, A.; Harris, R.E. Relaxation Acupressure Reduces Persistent Cancer-Related Fatigue. Evid.-Based Complement. Altern. Med. 2010, 2011, 142913. [Google Scholar] [CrossRef]
- Maa, S.-H.; Tsou, T.-S.; Wang, K.-Y.; Wang, C.-H.; Lin, H.-C.; Huang, Y.-H. Self-administered acupressure reduces the symptoms that limit daily activities in bronchiectasis patients: Pilot study findings. J. Clin. Nurs. 2007, 16, 794–804. [Google Scholar] [CrossRef]
- Hsiung, W.T.; Chang, Y.C.; Yeh, M.L.; Chang, Y.H. Acupressure improves the postoperative comfort of gastric cancer patients: A randomised controlled trial. Complementary Ther. Med. 2015, 23, 339–346. [Google Scholar] [CrossRef]
- Liu, X.-L.; Cheng, H.L.; Moss, S.; Wang, C.C.; Turner, C.; Tan, J.-Y. Somatic Acupoint Stimulation for Cancer-Related Sleep Disturbance: A Systematic Review of Randomized Controlled Trials. Evid.-Based Complement. Altern. Med. 2020, 2020, 2591320. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.Y.; Wang, T.; Kirshbaum, M.N.; Zhao, I.; Eliseeva, S.; Polotan, M.J.; Yao, L.Q.; Huang, H.Q.; Zheng, S.L. Acupoint stimulation for cancer-related fatigue: A quantitative synthesis of randomised controlled trials. Complementary Ther. Clin. Pract. 2021, 45, 101490. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Gu, J.; Liu, J.; Hong, H. Clinical evidence for acupressure with the improvement of sleep disorders in hemodialysis patients: A systematic review and meta-analysis. Complement. Ther. Clin. Pract. 2020, 39, 101151. [Google Scholar] [CrossRef]
- Tan, J.-Y.; Suen, L.K.P.; Wang, T.; Molassiotis, A. Sham Acupressure Controls Used in Randomized Controlled Trials: A Systematic Review and Critique. PLoS ONE 2015, 10, e0132989. [Google Scholar] [CrossRef] [PubMed]
- Dincer, F.; Linde, K. Sham interventions in randomized clinical trials of acupuncture—a review. Complementary Ther. Med. 2003, 11, 235–242. [Google Scholar] [CrossRef]
- Blackwood, B. Methodological issues in evaluating complex healthcare interventions. J. Adv. Nurs. 2006, 54, 612–622. [Google Scholar] [CrossRef]
- Watson, M. A framework for development and evaluation of RCTs for complex interventions to improve health. Int. J. Pharm Pract. 2000, 14, 233–234. [Google Scholar]
- Liang, F.R.; Wang, H. Acupuncture and Moxibustion, 4th ed.; China Press of Traditional Chinese Medicine Co., Ltd.: Beijing, China, 2016. (In Chinese) [Google Scholar]
- Shen, X.Y. Meridians and Acupoints, 4th ed.; China Press of Traditional Chinese Medicine Co., Ltd.: Beijing, China, 2008. (In Chinese) [Google Scholar]
- Lynn, M.R. Determination and quantification of content validity. Nurs. Res. 1986, 35, 382–385. [Google Scholar] [CrossRef]
- Rubio, D.M.; Berg-Weger, M.; Tebb, S.S.; Lee, E.S.; Rauch, S. Objectifying content validity: Conducting a content validity study in social work research. Soc. Work Res. 2003, 27, 94–104. [Google Scholar] [CrossRef]
- Polit, D.F.; Beck, C.T.; Owen, S.V. Is the CVI an acceptable indicator of content validity? Appraisal and recommendations. Res. Nurs. Health 2007, 30, 459–467. [Google Scholar] [CrossRef]
- Cleeland, C.S.; Bennett, G.J.; Dantzer, R.; Dougherty, P.M.; Dunn, A.J.; Meyers, C.A.; Miller, A.H.; Payne, R.; Reuben, J.M.; Wang, X.S.; et al. Are the symptoms of cancer and cancer treatment due to a shared biologic mechanism? A cytokine-immunologic model of cancer symptoms. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2003, 97, 2919–2925. [Google Scholar] [CrossRef] [PubMed]
- Rong, P.; Zhu, B.; Li, Y.; Gao, X.; Ben, H.; Li, Y.; Li, L.; He, W.; Liu, R.; Yu, L. Mechanism of acupuncture regulating visceral sensation and mobility. Front. Med. 2011, 5, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Yeh, M.-H.; Chao, C.-H.; Koo, M.; Chen, C.-Y.; Yeh, C.-C.; Li, T.-M. Association of traditional Chinese medicine body constitution and moderate-to-severe cancer-related fatigue in cancer patients. Complement. Ther. Med. 2019, 43, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Ju, Y.L.; Xu, C.H.; Liu, J.X. Forty cases of insomnia treated by suspended moxibustion at Baihui (GV 20). J. Tradit. Chin. Med. 2009, 29, 95–96. [Google Scholar] [CrossRef]
- Chien, T.-J.; Song, Y.-L.; Lin, C.-P.; Hsu, C.-H. The Correlation of Traditional Chinese Medicine Deficiency Syndromes, Cancer Related Fatigue, and Quality of Life in Breast Cancer Patients. J. Tradit. Complement. Med. 2012, 2, 204–210. [Google Scholar] [CrossRef]
- Weaver, M.T. Acupressure: An overview of theory and application. Nurse Pract. 1985, 10, 38–39. [Google Scholar] [CrossRef]
- Zhao, J.-P.; Chen, S.; Marmori, F.; Guo, S.-N.; Wang, Y.-P.; Wang, J.; Bai, P. Disease location identification as a major guide to acupoint selection. Chin. J. Integr. Med. 2013, 19, 894–899. [Google Scholar] [CrossRef]
- Yuan, H.-W.; Ma, L.-X.; Zhang, P.; Lin, C.; Qi, D.-D.; Li, J.; Xin, S.-Y.; Hu, N.-J.; Li, C.-H.; Liu, Y.-Q.; et al. An Exploratory Survey of Deqi Sensation from the Views and Experiences of Chinese Patients and Acupuncturists. Evid.-Based Complement. Altern. Med. 2013, 2013, 430851. [Google Scholar] [CrossRef]
- Tang, W.-R.; Chen, W.-J.; Yu, C.-T.; Chang, Y.-C.; Chen, C.-M.; Wang, C.-H.; Yang, S.-H. Effects of acupressure on fatigue of lung cancer patients undergoing chemotherapy: An experimental pilot study. Complement. Ther. Med. 2014, 22, 581–591. [Google Scholar] [CrossRef]
- Lun, X. Dian Xue Liao Fa (Therapy of Acupressure); Wan Li Book Co.: Hong Kong, China, 2012. [Google Scholar]
- Lund, I.; Näslund, J.; Lundeberg, T. Minimal acupuncture is not a valid placebo control in randomised controlled trials of acupuncture: A physiologist’s perspective. Chin. Med. 2009, 4, 1–9. [Google Scholar] [CrossRef]
- Pan, L.-J.; Chen, B.; Zhao, X.; Guo, Y. Thinking on designation of sham acupuncture in clinical research. Chin. Acupunct. Moxibustion 2014, 34, 83–86. [Google Scholar]
- O’Cathain, A.; Croot, L.; Duncan, E.; Rousseau, N.; Sworn, K.; Turner, K.M.; Yardley, L.; Hoddinott, P. Guidance on how to develop complex interventions to improve health and healthcare. BMJ Open 2019, 9, e029954. [Google Scholar] [CrossRef] [PubMed]
- Bleijenberg, N.; Janneke, M.; Trappenburg, J.C.; Ettema, R.G.; Sino, C.G.; Heim, N.; Hafsteindóttir, T.B.; Richards, D.A.; Schuurmans, M.J. Increasing value and reducing waste by optimizing the development of complex interventions: Enriching the development phase of the Medical Research Council (MRC) Framework. Int. J. Nurs. Stud. 2018, 79, 86–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacPherson, H.; Schroer, S. Acupuncture as a complex intervention for depression: A consensus method to develop a standardised treatment protocol for a randomised controlled trial. Complement. Ther. Med. 2007, 15, 92–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Contents | Details | Justifications | Sources of Evidence |
|---|---|---|---|
| Acupoints formula |
|
|
|
| SAS modality |
|
|
|
| SAS intensity and technique |
|
|
|
| SAS frequency, sessions and total duration |
|
|
| Basic Information of the Expert Panel | Percentage (%) |
|---|---|
| Working institution | |
| University | 3 (42.9%) |
| Hospital | 4 (57.1%) |
| Age | |
| 30–40 years old | 3 (42.9%) |
| 40–50 years old | 2 (28.5%) |
| 50–60 years old | 2 (28.5%) |
| Highest academic degree | |
| PhD or MD | 4 (57.1%) |
| Master’s degree | 2 (28.5%) |
| Bachelor’s degree | 1 (14.3%) |
| Academic and professional title | |
| Full professor | 3 (42.9%) |
| Associate chief physician or associate consultant | 4 (57.1%) |
| Years of professional experience | |
| 5–10 years | 1 (14.3%) |
| 11–15 years | 2 (28.5%) |
| 16–20 years | 1 (14.3%) |
| Over 20 years | 3 (42.9%) |
| Item | Description of Each Item | Content Validity Assessment | CVI | ||
|---|---|---|---|---|---|
| No. of Experts Rating as “(4) Very Appropriate” | No. of Experts Rating as “(3) Appropriate” | No. of Experts Rating as (3) or (4) | |||
| True SAS intervention protocol | |||||
| 1 | Selection of acupoints formula | 5 | 2 | 7 | I-CVI 1.00 |
| 2 | SAS modality | 5 | 2 | 7 | I-CVI 1.00 |
| 3 | SAS intensity and technique | 4 | 3 | 7 | I-CVI 1.00 |
| 4 | SAS frequency and sessions | 3 | 4 | 7 | I-CVI 1.00 |
| 5 | SAS total duration | 4 | 2 | 6 | I-CVI 0.86 |
| Scale level CVI | S-CVI 1.00 | ||||
| Placebo SAS intervention protocol | |||||
| 1 | Selection of acupoints formula | 5 | 1 | 6 | I-CVI 0.86 |
| 2 | SAS modality | 6 | 1 | 7 | I-CVI 1.00 |
| 3 | SAS intensity and technique | 6 | 1 | 7 | I-CVI 1.00 |
| 4 | SAS frequency and sessions | 3 | 4 | 7 | I-CVI 1.00 |
| 5 | SAS total duration | 4 | 2 | 6 | I-CVI 0.86 |
| Scale level CVI | S-CVI 1.00 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, J.-Y.; Wang, T.; Zhao, I.; Polotan, M.J.; Eliseeva, S. An Evidence-Based Somatic Acupressure Intervention Protocol for Managing the Breast Cancer Fatigue-Sleep Disturbance-Depression Symptom Cluster: Development and Validation following the Medical Research Council Framework. Int. J. Environ. Res. Public Health 2022, 19, 11934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191911934
Tan J-Y, Wang T, Zhao I, Polotan MJ, Eliseeva S. An Evidence-Based Somatic Acupressure Intervention Protocol for Managing the Breast Cancer Fatigue-Sleep Disturbance-Depression Symptom Cluster: Development and Validation following the Medical Research Council Framework. International Journal of Environmental Research and Public Health. 2022; 19(19):11934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191911934
Chicago/Turabian StyleTan, Jing-Yu (Benjamin), Tao Wang, Isabella Zhao, Mary Janice Polotan, and Sabina Eliseeva. 2022. "An Evidence-Based Somatic Acupressure Intervention Protocol for Managing the Breast Cancer Fatigue-Sleep Disturbance-Depression Symptom Cluster: Development and Validation following the Medical Research Council Framework" International Journal of Environmental Research and Public Health 19, no. 19: 11934. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191911934