
Physical Activity Level, Depression, Anxiety, and Self-Perceived Health in Spanish Adults with Migraine: A Cross-Sectional Study
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design of the Study
2.2. Participants
2.3. Procedures
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Future Considerations
4.2. Limitations and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Quesada Vázquez, A.J.; Contreras Maure, L.J.; Álvarez Aliaga, A.; Traba Tamayo, E.R. Prevalencia de cefaleas primarias en una población rural cubana. Rev. Neurol. 2009, 49, 131. [Google Scholar] [CrossRef] [PubMed]
- Peters, G.L. Descripción general de la migraña y resumen de las opciones de tratamiento actuales y emergentes. Am. J. Manag. Care 2019, 25, 23–34. [Google Scholar]
- Baloh, R.W. Vestibular Migraine I: Mechanisms, Diagnosis, and Clinical Features. Semin. Neurol. 2020, 40, 076–082. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, M.; Obermann, M.; Celebisoy, N. Vestibular Migraine: The Most Frequent Entity of Episodic Vertigo. J. Neurol. 2016, 263, 82–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karsan, N.; Prabhakar, P.; Goadsby, P.J. Premonitory Symptoms of Migraine in Childhood and Adolescence. Curr. Pain Headache Rep. 2017, 21, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wijeratne, T.; Tang, H.M.; Crewther, D.; Crewther, S. Prevalence of Migraine in the Elderly: A Narrated Review. Neuroepidemiology 2019, 52, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Deza Bringas, L. La Migraña. Acta Media Peru. 2010, 27, 129–136. [Google Scholar]
- Stewart, W.F.; Wood, G.C.; Manack, A.; Varon, S.F.; Buse, D.C.; Lipton, R.B. Employment and Work Impact of Chronic Migraine and Episodic Migraine. J. Occup. Environ. Med. 2010, 52, 8–14. [Google Scholar] [CrossRef] [PubMed]
- May, A.; Schulte, L.H. Chronic Migraine: Risk Factors, Mechanisms and Treatment. Nat. Rev. Neurol. 2016, 12, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Burch, R.C.; Buse, D.C.; Lipton, R.B. Migraine. Neurol. Clin. 2019, 37, 631–649. [Google Scholar] [CrossRef] [PubMed]
- Charles, A. The Pathophysiology of Migraine: Implications for Clinical Management. Lancet Neurol. 2018, 17, 174–182. [Google Scholar] [CrossRef]
- Zhang, Q.; Shao, A.; Jiang, Z.; Tsai, H.; Liu, W. The Exploration of Mechanisms of Comorbidity between Migraine and Depression. J. Cell. Mol. Med. 2019, 23, 4505–4513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amiri, S.; Behnezhad, S.; Azad, E. Migraine Headache and Depression in Adults: A Systematic Review and Meta-Analysis. Neuropsychiatrie 2019, 33, 131–140. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.J.; Charlson, F.J.; Norman, R.E.; Patten, S.B.; Freedman, G.; Murray, C.J.L.; Vos, T.; Whiteford, H.A. Burden of Depressive Disorders by Country, Sex, Age, and Year: Findings from the Global Burden of Disease Study 2010. PLoS Med. 2013, 10, e1001547. [Google Scholar] [CrossRef] [Green Version]
- Rakel, R.E. Depression. Prim. Care Clin. Off. Pract. 1999, 26, 211–224. [Google Scholar] [CrossRef]
- Alwhaibi, M.; Alhawassi, T.M. Humanistic and Economic Burden of Depression and Anxiety among Adults with Migraine: A Systematic Review. Depress. Anxiety 2020, 37, 1146–1159. [Google Scholar] [CrossRef]
- Antonaci, F.; Nappi, G.; Galli, F.; Manzoni, G.C.; Calabresi, P.; Costa, A. Migraine and Psychiatric Comorbidity: A Review of Clinical Findings. J. Headache Pain 2011, 12, 115–125. [Google Scholar] [CrossRef] [Green Version]
- Ayele, B.A.; Yifru, Y.M. Migraine-Related Disability and Co-Morbid Depression among Migraineurs in Ethiopia: A Cross-Sectional Study. BMC Neurol. 2018, 18, 95. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, Â.; Ribeiro, J.P.; von Doellinger, O. Depression and Psychodynamic Psychotherapy. Rev. Bras. Psiquiatr. 2017, 40, 105–109. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.X.; Wang, S.R.; Zhao, J.S.; Chu, Z.H. Truncal Pattern of Subcutaneous Fat Distribution Is Associated with Obesity and Elevated Blood Pressure among Children and Adolescents. Blood Press 2018, 27, 25–31. [Google Scholar] [CrossRef]
- Balsamo, M.; Cataldi, F.; Carlucci, L.; Fairfield, B. Assessment of Anxiety in Older Adults: A Review of Self-Report Measures. Clin. Interv. Aging 2018, 13, 573–593. [Google Scholar] [CrossRef] [Green Version]
- El-Gabalawy, R.; Mackenzie, C.S.; Thibodeau, M.A.; Asmundson, G.J.G.; Sareen, J. Health Anxiety Disorders in Older Adults: Conceptualizing Complex Conditions in Late Life. Clin. Psychol. Rev. 2013, 33, 1096–1105. [Google Scholar] [CrossRef] [PubMed]
- Baxter, A.J.; Scott, K.M.; Vos, T.; Whiteford, H.A. Global Prevalence of Anxiety Disorders: A Systematic Review and Meta-Regression. Psychol. Med. 2013, 43, 897–910. [Google Scholar] [CrossRef] [PubMed]
- Karimi, L.; Crewther, S.G.; Wijeratne, T.; Evans, A.E.; Afshari, L.; Khalil, H. The Prevalence of Migraine With Anxiety Among Genders. Front. Neurol. 2020, 11, 569405. [Google Scholar] [CrossRef] [PubMed]
- Karimi, L.; Wijeratne, T.; Crewther, S.G.; Evans, A.E.; Ebaid, D.; Khalil, H. The Migraine-Anxiety Comorbidity Among Migraineurs: A Systematic Review. Front. Neurol. 2021, 11, 613372. [Google Scholar] [CrossRef]
- Pascual Gómez, J. Migraña crónica: Tratamiento. Rev. Neurol. 2012, 54, 31. [Google Scholar] [CrossRef] [Green Version]
- Schrader, H. Prophylactic Treatment of Migraine with Angiotensin Converting Enzyme Inhibitor (Lisinopril): Randomised, Placebo Controlled, Crossover Study. BMJ 2001, 322, 19. [Google Scholar] [CrossRef] [Green Version]
- Busch, V.; Gaul, C. Exercise in Migraine Therapy—Is There Any Evidence for Efficacy? A Critical Review. Headache J. Head Face Pain 2008, 48, 890–899. [Google Scholar] [CrossRef]
- Adamson, B.C.; Ensari, I.; Motl, R.W. Effect of Exercise on Depressive Symptoms in Adults With Neurologic Disorders: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2015, 96, 1329–1338. [Google Scholar] [CrossRef]
- Oliveira, A.B.; Bachi, A.L.L.; Ribeiro, R.T.; Mello, M.T.; Vaisberg, M.; Peres, M.F.P. Exercise-Induced Change in Plasma IL-12p70 Is Linked to Migraine Prevention and Anxiolytic Effects in Treatment-Naïve Women: A Randomized Controlled Trial. Neuroimmunomodulation 2017, 24, 293–299. [Google Scholar] [CrossRef]
- Thompson, P.D.; Buchner, D.; Piña, I.L.; Balady, G.J.; Williams, M.A.; Marcus, B.H.; Berra, K.; Blair, S.N.; Costa, F.; Franklin, B.; et al. Exercise and Physical Activity in the Prevention and Treatment of Atherosclerotic Cardiovascular Disease: A Statement From the Council on Clinical Cardiology (Subcommittee on Exercise, Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity). Circulation 2003, 107, 3109–3116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Köseoglu, E.; Akboyraz, A.; Soyuer, A.; Ersoy, A. Aerobic Exercise and Plasma Beta Endorphin Levels in Patients with Migrainous Headache Without Aura. Cephalalgia 2003, 23, 972–976. [Google Scholar] [CrossRef] [PubMed]
- Carek, P.J.; Laibstain, S.E.; Carek, S.M. Exercise for the Treatment of Depression and Anxiety. Int. J. Psychiatry Med. 2011, 41, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Consumo y Bienestar Social. Encuesta Nacional De Salud 2017 Cuestionario De Adultos; Ministerio de Sanidad, Consumo y Bienestar Social: Madrid, Spain, 2017; pp. 1–61.
- Cabezas-Rodríguez, A.; Bacigalupe, A.; Martín, U. Diagnosis and Treatment of Depression in Spain: Are There Gender Inequalities? Int. J. Environ. Res. Public. Health 2020, 17, 9232. [Google Scholar] [CrossRef]
- Fernandez-Piciochi, C.; Martín-Saborido, C.; Bimbela-Pedrola, J.L.; Sarria-Santamera, A. The Economic Burden of Anxiety and Depression on the Working Age Population with Diabetes in Spain. Int. J. Health Plann. Manage. 2022, 37, 715–724. [Google Scholar] [CrossRef]
- Nes, B.M.; Janszky, I.; Vatten, L.J.; Nilsen, T.I.L.; Aspenes, S.T.; Wisløff, U. Estimating V−O2peak from a Nonexercise Prediction Model: The HUNT Study, Norway. Med. Sci. Sports Exerc. 2011, 43, 2024–2030. [Google Scholar] [CrossRef]
- Denche-Zamorano, Á.; Franco-García, J.M.; Carlos-Vivas, J.; Mendoza-Muñoz, M.; Pereira-Payo, D.; Pastor-Cisneros, R.; Merellano-Navarro, E.; Adsuar, J.C. Increased Risks of Mental Disorders: Youth with Inactive Physical Activity. Healthcare 2022, 10, 237. [Google Scholar] [CrossRef]
- Vetvik, K.G.; MacGregor, E.A. Sex Differences in the Epidemiology, Clinical Features, and Pathophysiology of Migraine. Lancet Neurol. 2017, 16, 76–87. [Google Scholar] [CrossRef]
- Shyti, R.; de Vries, B.; van den Maagdenberg, A. Migraine Genes and the Relation to Gender: June 2011. Headache J. Head Face Pain 2011, 51, 880–890. [Google Scholar] [CrossRef]
- Schroeder, R.A.; Brandes, J.; Buse, D.C.; Calhoun, A.; Eikermann-Haerter, K.; Golden, K.; Halker, R.; Kempner, J.; Maleki, N.; Moriarty, M.; et al. Sex and Gender Differences in Migraine—Evaluating Knowledge Gaps. J. Womens Health 2018, 27, 965–973. [Google Scholar] [CrossRef]
- Sun, F.; Norman, I.J.; While, A.E. Physical Activity in Older People: A Systematic Review. BMC Public Health 2013, 13, 449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Socci, M.; Santini, S.; Dury, S.; Perek-Białas, J.; D’Amen, B.; Principi, A. Physical Activity during the Retirement Transition of Men and Women: A Qualitative Longitudinal Study. BioMed Res. Int. 2021, 2021, 2720885. [Google Scholar] [CrossRef] [PubMed]
- Lipton, R.B.; Bigal, M.E.; Diamond, M.; Freitag, F.; Reed, M.L.; Stewart, W.F.; on behalf of the AMPP Advisory Group. Migraine Prevalence, Disease Burden, and the Need for Preventive Therapy. Neurology 2007, 68, 343–349. [Google Scholar] [CrossRef] [Green Version]
- Lisicki, M.; Figuerola, M.L.; Bonamico, L.; Lew, D.; Goicochea, M.T.; on behalf of the Headache Group of the Argentinian Neurological Society The Prevalence of Migraine in Argentina. The prevalence of migraine in Argentina: A Reappraisal. Cephalalgia 2021, 41, 821–826. [Google Scholar] [CrossRef] [PubMed]
- Krøll, L.S.; Hammarlund, C.S.; Linde, M.; Gard, G.; Jensen, R.H. The Effects of Aerobic Exercise for Persons with Migraine and Co-Existing Tension-Type Headache and Neck Pain. A Randomized, Controlled, Clinical Trial. Cephalalgia 2018, 38, 1805–1816. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D.; Holland, S.; Freitag, F.; Dodick, D.W.; Argoff, C.; Ashman, E. Evidence-Based Guideline Update: Pharmacologic Treatment for Episodic Migraine Prevention in Adults: Table 1: Report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology 2012, 78, 1337–1345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hien, H.; González, A. Migraine Headache Prophylaxis. Am. Fam. Physician 2019, 99, 17. [Google Scholar]
- Lemmens, J.; De Pauw, J.; Van Soom, T.; Michiels, S.; Versijpt, J.; van Breda, E.; Castien, R.; De Hertogh, W. The Effect of Aerobic Exercise on the Number of Migraine Days, Duration and Pain Intensity in Migraine: A Systematic Literature Review and Meta-Analysis. J. Headache Pain 2019, 20, 16. [Google Scholar] [CrossRef]
- Hanssen, H.; Minghetti, A.; Magon, S.; Rossmeissl, A.; Rasenack, M.; Papadopoulou, A.; Klenk, C.; Faude, O.; Zahner, L.; Sprenger, T.; et al. Effects of Different Endurance Exercise Modalities on Migraine Days and Cerebrovascular Health in Episodic Migraineurs: A Randomized Controlled Trial. Scand. J. Med. Sci. Sports 2018, 28, 1103–1112. [Google Scholar] [CrossRef]
- Yang, Y.; Ligthart, L.; Terwindt, G.M.; Boomsma, D.I.; Rodriguez-Acevedo, A.J.; Nyholt, D.R. Genetic Epidemiology of Migraine and Depression. Cephalalgia 2016, 36, 679–691. [Google Scholar] [CrossRef]
- Müller, B.; Gaul, C.; Glass, Ä.; Reis, O.; Jürgens, T.P.; Kropp, P.; Ruscheweyh, R.; Straube, A.; Brähler, E.; Förderreuther, S.; et al. Physical Activity Is Associated with Less Analgesic Use in Women Reporting Headache—A Cross-Sectional Study of the German Migraine and Headache Society (DMKG). Pain Ther. 2022, 11, 545–560. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Sánchez, S.; Fernández-de-las-Peñas, C.; Jiménez-García, R.; Hernández-Barrera, V.; Alonso-Blanco, C.; Palacios-Ceña, D.; Carrasco-Garrido, P. Prevalence of Migraine Headaches in the Romany Population in Spain: Sociodemographic Factors, Lifestyle and Co-Morbidity. J. Transcult. Nurs. 2013, 24, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Hernández-Barrera, V.; Carrasco-Garrido, P.; Alonso-Blanco, C.; Palacios-Ceña, D.; Jiménez-Sánchez, S.; Jiménez-García, R. Population-Based Study of Migraine in Spanish Adults: Relation to Socio-Demographic Factors, Lifestyle and Co-Morbidity with Other Conditions. J. Headache Pain 2010, 11, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Lera López, F.; Garrués Irisarri, M.; Ollo López, A.; Sánchez Iriso, E.; Cabasés Hita, J.M.; Sánchez Santos, J.M. Actividad Física y Salud Autopercibida En Personas Mayores de 50 Años. Rev. Int. Med. Cienc. Act. Física Deporte 2017, 17, 559–571. [Google Scholar]
- Bélair, M.-A.; Kohen, D.E.; Kingsbury, M.; Colman, I. Relationship between Leisure Time Physical Activity, Sedentary Behaviour and Symptoms of Depression and Anxiety: Evidence from a Population-Based Sample of Canadian Adolescents. BMJ Open 2018, 8, e021119. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Men n = 8188 | Women n = 8941 | Total n = 17,139 | X2 | df | p-Value Mann–Whitney U Test | |||
|---|---|---|---|---|---|---|---|---|---|
| Age | |||||||||
| Median (IQR) | 47 | (21) | 47 | (21) | 47 | (21) | - | - | 0.506 |
| Mean (SD) | 46.8 | (13.2) | 46.9 | (13.3) | 46.8 | (13.3) | - | - | - |
| Migraine | n | % | n | % | n | % | X2 | df | p-value Chi-square test |
| Yes | 532 | 6.5 | 1440 | 16.1 * | 1972 | 11.5 | 388.4 | 1 | <0.001 |
| No | 7666 | 93.5 | 7501 | 83.9 * | 15,167 | 88.5 | |||
| PAL | |||||||||
| Inactive | 1155 | 14.1 | 1326 | 14.8 | 2481 | 14.5 | 373.4 | 3 | <0.001 |
| Walker | 3335 | 40.7 | 4565 | 51.1 * | 7900 | 46.1 | |||
| Active | 2350 | 28.7 | 2338 | 26.1 * | 4688 | 27.4 | |||
| Very active | 1358 | 16.6 | 712 | 8.0 * | 2070 | 12.1 | |||
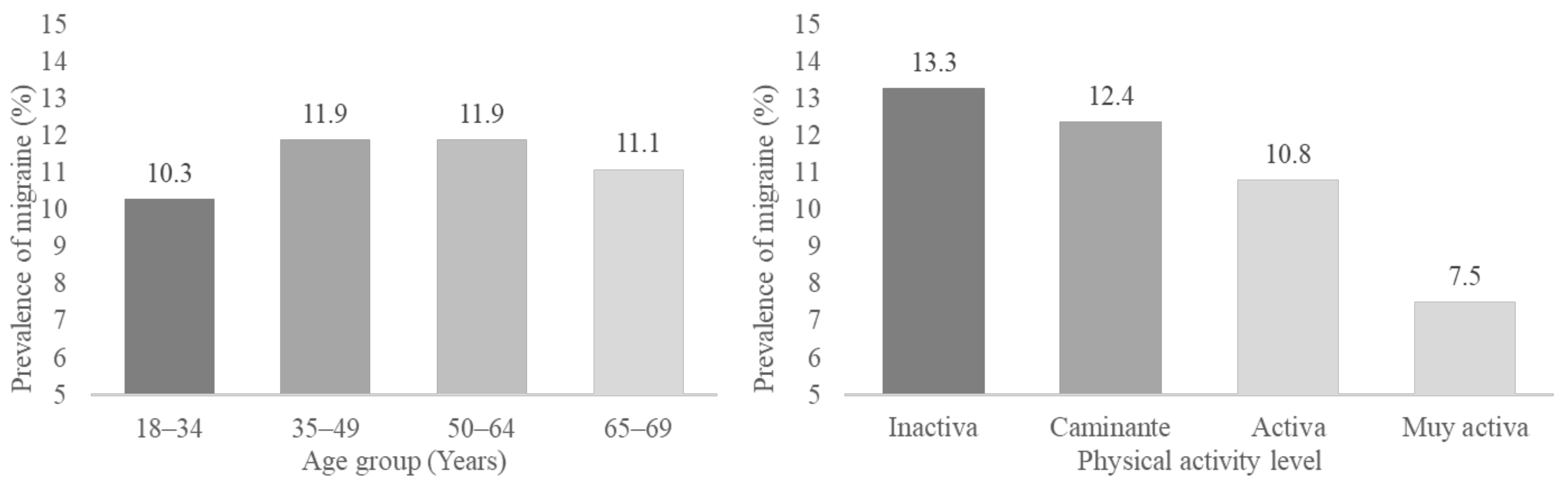
| Migraine | 18–34 Years | 35–49 Years | 50–64 Years | 65–69 Years | Total | X2 | df | p | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes n (%) | 341 a | (10.3) | 734 a | (11.9) | 707 a | (11.9) | 190 a | (11.1) | 1972 | (11.5) | 6.3 | 3 | 0.098 |
| No n (%) | 2956 a | (89.7) | 5443 | (88.1) | 5247 a | (88.1) | 1521 | (88.9) | 15,167 | (88.5) | |||
| Migraine | Inactive | Walker | Active | Very active | Total | ||||||||
| Yes n (%) | 331 a | (13.3) | 981 a | (12.4) | 504 b | (10.8) | 156 c | (7.5) | 1972 | (11.5) | 49.3 | 3 | <0.001 |
| No n (%) | 2150 a | (86.7) | 6919 a | (87.6) | 4184 b | (89.2) | 1914 c | (92.5) | 15,167 | (88.5) | |||
| Variables | Men n = 532 | Women n = 1440 | Total n = 1972 | X2 | df | p-Value Mann–Whitney U Test | |||
|---|---|---|---|---|---|---|---|---|---|
| Age | |||||||||
| Median (IQR) | 48.5 | (19) | 47 | (19) | 48 | (20) | - | - | 0.470 |
| Mean (SD) | 47.6 | (12.7) | 47.2 | (12.6) | 47.3 | (12.6) | - | - | - |
| Depression | n | % | n | % | n | % | X2 | df | p-value Chi-square test |
| Yes | 122 | 22.9 | 383 | 26.7 | 505 | 25.6 | 2.8 | 1 | 0.093 |
| No | 410 | 77.1 | 1054 | 73.3 | 1464 | 74.4 | |||
| Anxiety | |||||||||
| Yes | 110 | 20.7 | 387 | 26.9 * | 497 | 25.2 | 8.0 | 1 | 0.005 |
| No | 387 | 26.9 | 1050 | 73.1 * | 1969 | 74.8 | |||
| Analgesics | |||||||||
| Yes | 298 | 56.0 | 964 | 66.9 * | 1262 | 64.0 | 20.1 | 1 | <0.001 |
| No | 234 | 44.0 | 476 | 33.1 * | 710 | 36.0 | |||
| Self-perceived health | |||||||||
| Negative | 94 | 17.7 | 220 | 15.3 | 314 | 15.9 | 3.9 | 2 | 0.142 |
| Fair | 165 | 31.0 | 510 | 35.4 | 675 | 34.2 | |||
| Positive | 273 | 51.3 | 710 | 49.3 | 983 | 49.8 | |||
| PAL | |||||||||
| Inactive | 83 | 15.6 | 248 | 17.2 | 331 | 16.8 | 31.7 | 3 | <0.001 |
| Walker | 247 | 46.4 | 734 | 51.0 | 981 | 49.7 | |||
| Active | 130 | 24.4 | 374 | 26.0 | 504 | 25.6 | |||
| Very active | 72 | 13.5 | 84 | 5.8 * | 156 | 7.9 | |||
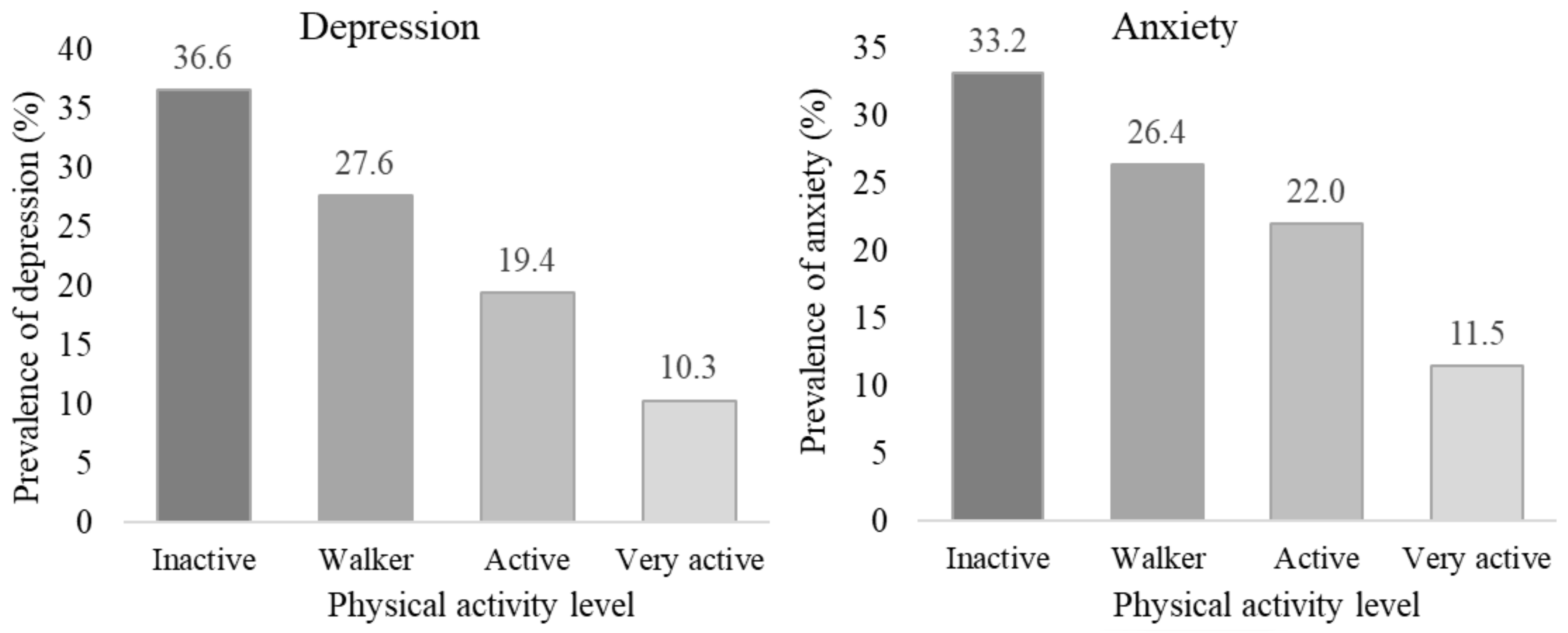
| Depression | Inactive | Walker | Active | Very Active | Total | X2 | df | p | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yes n (%) | 121 a | 36.6 | 270 b | 27.6 | 98 c | 19.4 | 16 d | 10.3 | 505 | 25.6 | 52.2 | 3 | <0.001 |
| No n (%) | 210 a | 63.4 | 708 b | 72.4 | 406 c | 80.6 | 140 d | 89.7 | 1464 | 74.4 | |||
| Anxiety | |||||||||||||
| Yes n (%) | 110 a | 33.2 | 258 ab | 26.4 | 111 b | 22.0 | 18 c | 11.5 | 497 | 25.2 | 30.2 | 3 | <0.001 |
| No n (%) | 221 a | 66.8 | 720 ab | 73.6 | 393 b | 78.0 | 138 c | 88.5 | 1472 | 74.8 | |||
| Analgesics | |||||||||||||
| Yes n (%) | 233 a | 70.4 | 651 a | 66.4 | 295 b | 58.5 | 83 b | 53.2 | 1262 | 64.0 | 20.7 | 3 | <0.001 |
| No n (%) | 98 a | 29.6 | 330 a | 33.6 | 209 b | 41.5 | 73 b | 46.8 | 710 | 36.0 | |||
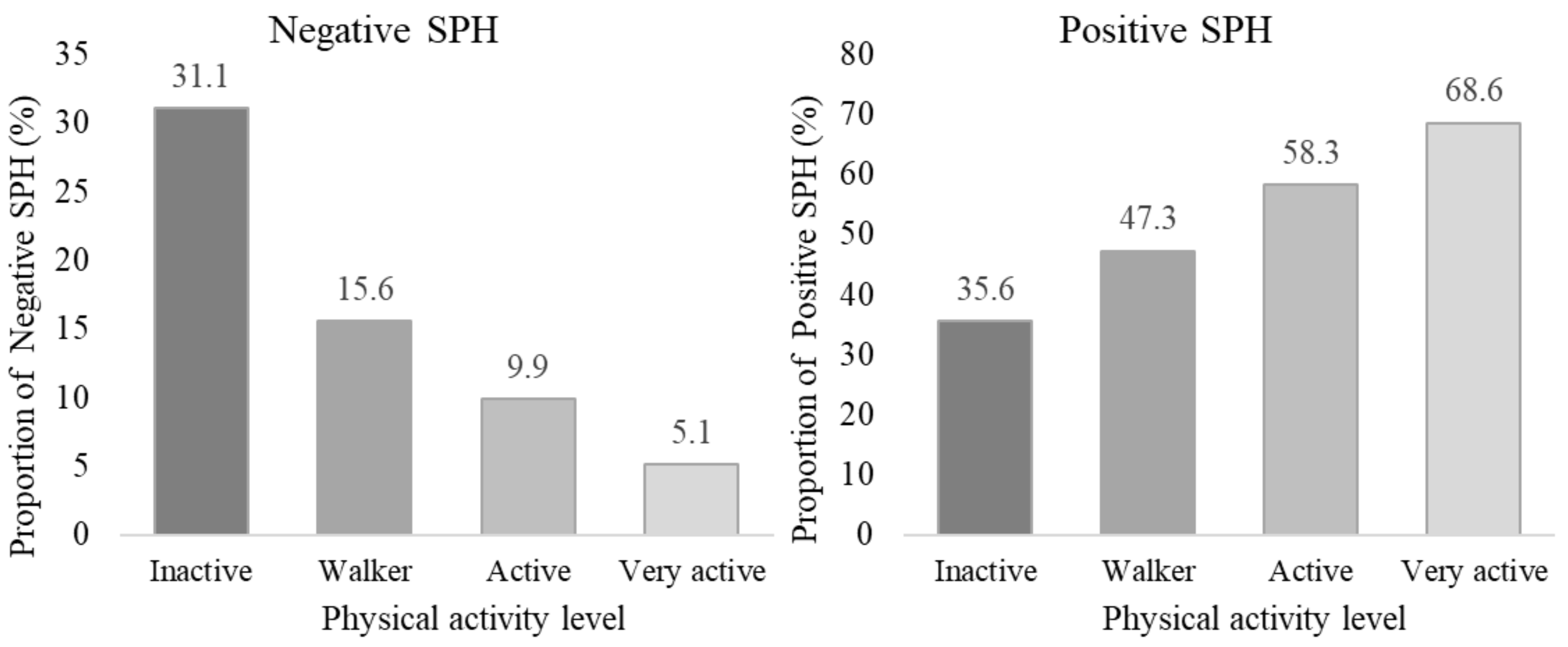
| Self-perceived health | |||||||||||||
| Negative n (%) | 103 a | 31.1 | 153 b | 15.6 | 50 c | 9.9 | 8 c | 5.1 | 314 | 15.9 | 110.1 | 6 | <0.001 |
| Fair n (%) | 110 a | 33.2 | 364 a | 37.1 | 160 a | 31.7 | 41 a | 26.3 | 675 | 34.2 | |||
| Positive n (%) | 118 a | 35.6 | 464 b | 47.3 | 294 c | 58.3 | 107 c | 68.6 | 983 | 49.8 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denche-Zamorano, Á.; Paredes-Mateos, V.; Pastor-Cisneros, R.; Carlos-Vivas, J.; Contreras-Barraza, N.; Iturra-Gonzalez, J.A.; Mendoza-Muñoz, M. Physical Activity Level, Depression, Anxiety, and Self-Perceived Health in Spanish Adults with Migraine: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 13882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192113882
Denche-Zamorano Á, Paredes-Mateos V, Pastor-Cisneros R, Carlos-Vivas J, Contreras-Barraza N, Iturra-Gonzalez JA, Mendoza-Muñoz M. Physical Activity Level, Depression, Anxiety, and Self-Perceived Health in Spanish Adults with Migraine: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(21):13882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192113882
Chicago/Turabian StyleDenche-Zamorano, Ángel, Víctor Paredes-Mateos, Raquel Pastor-Cisneros, Jorge Carlos-Vivas, Nicolás Contreras-Barraza, José A. Iturra-Gonzalez, and María Mendoza-Muñoz. 2022. "Physical Activity Level, Depression, Anxiety, and Self-Perceived Health in Spanish Adults with Migraine: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 21: 13882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192113882