
Is Hospital Hospice Service Associated with Efficient Healthcare Utilization in Deceased Lung Cancer Patients? Hospital Charges at Their End of Life

Abstract
:1. Introduction
2. Materials and Methods
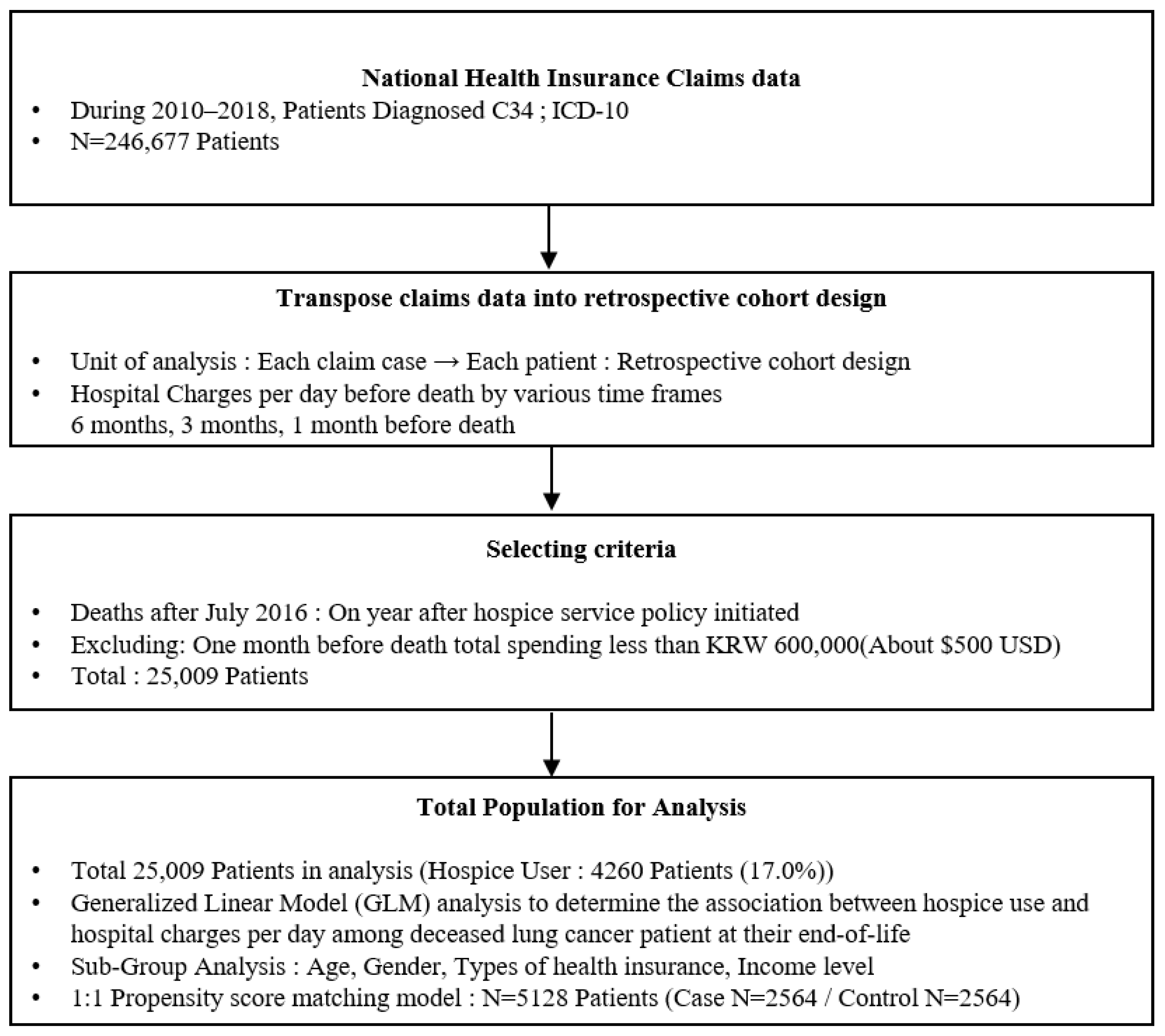
2.1. Study Population
2.2. Variables
2.3. Statistical Analyses
3. Results
3.1. Patient Sample and Characteristics
3.2. Association between Hospice Service and Efficient Healthcare Utilization
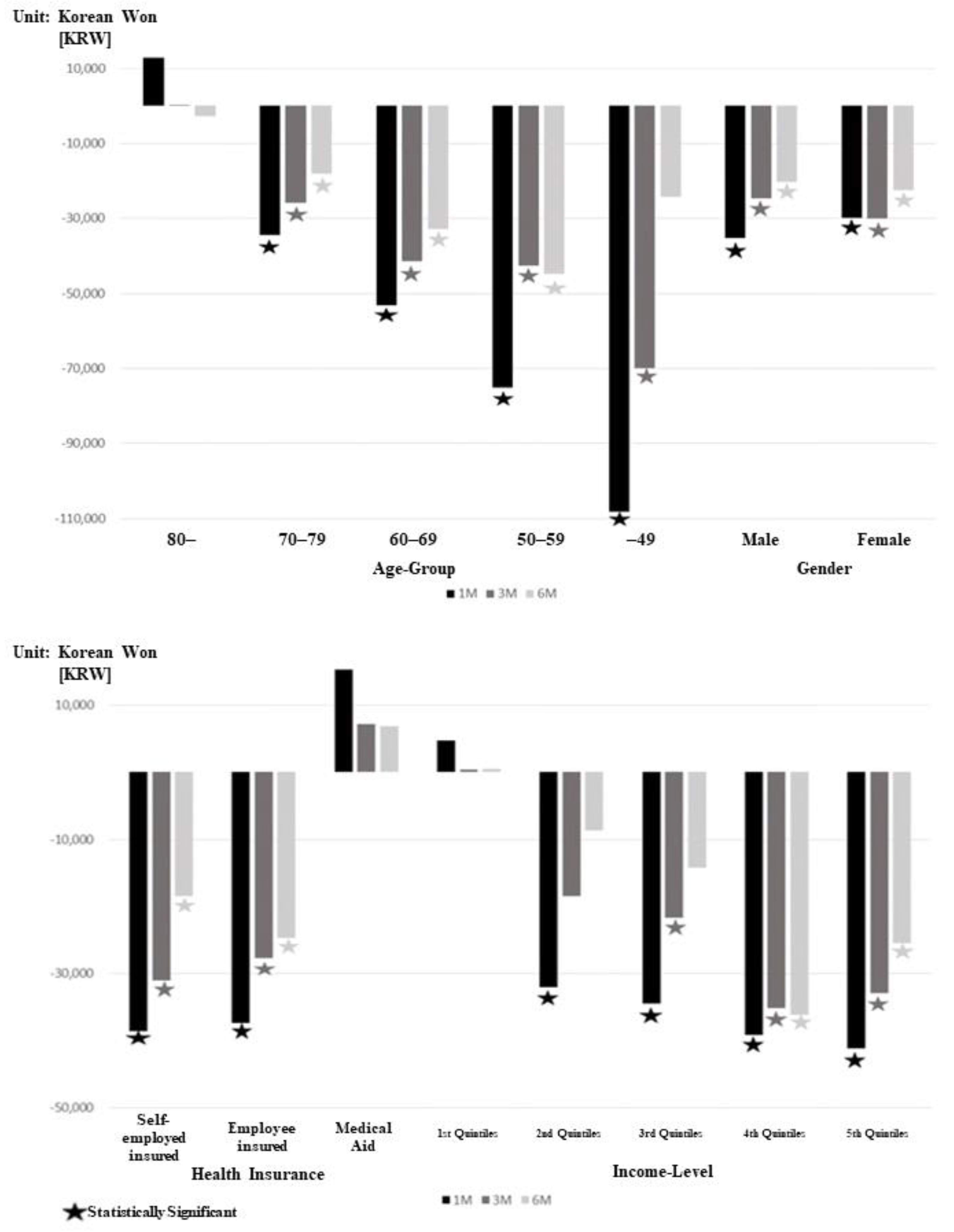
3.3. Subgroup Analysis and Propensity Score Matching Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Burden of Disease Cancer Collaboration; Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [PubMed]
- Statistics Korea. Cause of Death Statistics in Korea; Statistics Korea: Daejeon, Republic of Korea, 2018. [Google Scholar]
- Park, J.H.; Lee, K.S.; Choi, K.S. Burden of cancer in Korea during 2000–2020. Cancer Epidemiol. 2013, 37, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Meropol, N.J.; Schulman, K.A. Cost of cancer care: Issues and implications. J. Clin. Oncol. 2007, 25, 180–186. [Google Scholar] [CrossRef]
- Sullivan, R.; Peppercorn, J.; Sikora, K.; Zalcberg, J.; Meropol, N.J.; Amir, E.; Khayat, D.; Boyle, P.; Autier, P.; Tannock, I.F.; et al. Delivering affordable cancer care in high-income countries. Lancet Oncol. 2011, 12, 933–980. [Google Scholar] [CrossRef]
- DiMasi, J.A.; Hansen, R.W.; Grabowski, H.G. The price of innovation: New estimates of drug development costs. J. Health Econ. 2003, 22, 151–185. [Google Scholar] [CrossRef] [Green Version]
- McCall, N. Utilization and costs of Medicare services by beneficiaries in their last year of life. Med. Care 1984, 22, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Lubitz, J.D.; Riley, G.F. Trends in Medicare payments in the last year of life. N. Engl. J. Med. 1993, 328, 1092–1096. [Google Scholar] [CrossRef]
- Brown, M.L.; Riley, G.F.; Schussler, N.; Etzioni, R. Estimating health care costs related to cancer treatment from SEER-Medicare data. Med. Care 2002, 40, IV-104-17. [Google Scholar] [CrossRef]
- Yabroff, K.R.; Lamont, E.B.; Mariotto, A.; Warren, J.L.; Topor, M.; Meekins, A.; Brown, M.L. Cost of care for elderly cancer patients in the United States. J. Natl. Cancer Inst. 2008, 100, 630–641. [Google Scholar] [CrossRef] [Green Version]
- Gardiner, C.; Brereton, L.; Frey, R.; Wilkinson-Meyers, L.; Gott, M. Exploring the financial impact of caring for family members receiving palliative and end-of-life care: A systematic review of the literature. Palliat. Med. 2014, 28, 375–390. [Google Scholar] [CrossRef]
- Beccaro, M.; Costantini, M.; Giorgi Rossi, P.; Miccinesi, G.; Grimaldi, M.; Bruzzi, P.; ISDOC Study Group. Actual and preferred place of death of cancer patients. Results from the Italian survey of the dying of cancer (ISDOC). J. Epidemiol. Community Health 2006, 60, 412–416. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Atlas of Palliative Care at the End of Life; Worldwide Palliative Care Alliance: London, UK, 2014. [Google Scholar]
- Rome, R.B.; Luminais, H.H.; Bourgeois, D.A.; Blais, C.M. The role of palliative care at the end of life. Ochsner. J. 2011, 11, 348–352. [Google Scholar] [PubMed]
- Park, B.K.; Park, Y.M.; Kim, Y.S.; Hong, S.J.; Park, S.C.; Kim, Y.N.; Yook, T.M.; Bae, S.J. Analysis of the Use and Effect of Inpatient Hospice in Terminal Cancer Patients after Applying Health Insurance, Research Report 2018-20-028; National Health Insurance Ilsan Hospital: Gyeonggi-do, Republic of Korea, 2019. [Google Scholar]
- Health Insurance Review and Assessment Service. Application of Palliative Care Health Insurance—Medical Care Benefit Cost and Practical Guidance; Health Insurance Review and Assessment Service: Wonju, Republic of Korea, 2015. [Google Scholar]
- National Cancer Center of Korea. Status of Hospice Palliative Care 2016; National Cancer Center of Korea: Goyang, Republic of Korea, 2018. [Google Scholar]
- National Cancer Center of Korea. Status of Hospice Palliative Care 2017; National Cancer Center of Korea: Goyang, Republic of Korea, 2019. [Google Scholar]
- Taylor, D.H., Jr. The effect of hospice on Medicare and informal care costs: The U.S. Experience. J. Pain Symptom Manag. 2009, 38, 110–114. [Google Scholar] [CrossRef] [PubMed]
- Higginson, I.J.; Finlay, I.; Goodwin, D.M.; Cook, A.M.; Hood, K.; Edwards, A.G.K.; Douglas, H.-R.; Norman, C.E. Do hospital-based palliative teams improve care for patients or families at the end of life? J. Pain Symptom Manag. 2002, 23, 96–106. [Google Scholar] [CrossRef]
- Zhang, B.; Wright, A.A.; Huskamp, H.A.; Nilsson, M.E.; Maciejewski, M.L.; Earle, C.C.; Block, S.D.; Maciejewski, P.K.; Prigerson, H.G. Health care costs in the last week of life: Associations with end-of-life conversations. Arch. Intern. Med. 2009, 169, 480–488. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.J.; Han, K.T.; Kim, T.H.; Park, E.C. Does hospital need more hospice beds? Hospital charges and length of stays by lung cancer inpatients at their end of life: A retrospective cohort design of 2002–2012. Palliat. Med. 2015, 29, 808–816. [Google Scholar] [CrossRef]
- Huo, J.; Hong, Y.R.; Turner, K.; Bian, J.; Grewal, R.; Wilkie, D.J. Utilization pattern and service settings of palliative care for patients with metastatic non-small cell lung cancer. Cancer 2019, 125, 4481–4489. [Google Scholar] [CrossRef]
- Hwang, J.; Shen, J.; Kim, S.J.; Chun, S.Y.; Kioka, M.; Sheraz, F.; Kim, P.; Byun, D.; Yoo, J.W. Ten-Year Trends of Utilization of Palliative Care Services and Life-Sustaining Treatments and Hospital Costs Associated With Patients With Terminally Ill Lung Cancer in the United States From 2005 to 2014. Am. J. Hosp. Palliat. Care 2019, 36, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Triplett, D.P.; LeBrett, W.G.; Bryant, A.K.; Bruggeman, A.R.; Matsuno, R.K.; Hwang, L.; Boero, I.J.; Roeland, E.J.; Yeung, H.N.; Murphy, J.D. Effect of Palliative Care on Aggressiveness of End-of-Life Care Among Patients With Advanced Cancer. J. Oncol. Pract. 2017, 13, e760–e769. [Google Scholar] [CrossRef]
- Mor, V.; Wagner, T.H.; Levy, C.; Ersek, M.; Miller, S.C.; Gidwani-Marszowski, R.; Joyce, N.; Faricy-Anderson, K.; Corneau, E.A.; Lorenz, K.; et al. Association of Expanded VA Hospice Care With Aggressive Care and Cost for Veterans With Advanced Lung Cancer. JAMA Oncol. 2019, 5, 810–816. [Google Scholar] [CrossRef]
- Ho, T.H.; Barbera, L.; Saskin, R.; Lu, H.; Neville, B.A.; Earle, C.C. Trends in the aggressiveness of end-of-life cancer care in the universal health care system of Ontario, Canada. J. Clin. Oncol. 2011, 29, 1587–1591. [Google Scholar] [CrossRef] [Green Version]
- Langton, J.M.; Blanch, B.; Drew, A.K.; Haas, M.; Ingham, J.M.; Pearson, S.A. Retrospective studies of end-of-life resource utilization and costs in cancer care using health administrative data: A systematic review. Palliat. Med. 2014, 28, 1167–1196. [Google Scholar] [CrossRef]
- Obermeyer, Z.; Makar, M.; Abujaber, S.; Dominici, F.; Block, S.; Cutler, D.M. Association between the Medicare hospice benefit and health care utilization and costs for patients with poor-prognosis cancer. JAMA 2014, 312, 1888–1896. [Google Scholar] [CrossRef]
- Chiang, J.K.; Kao, Y.H.; Lai, N.S. The Impact of Hospice Care on Survival and Healthcare Costs for Patients with Lung Cancer: A National Longitudinal Population-Based Study in Taiwan. PLoS ONE 2015, 10, e0138773. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Earle, C.C.; Landrum, M.B.; Souza, J.M.; Neville, B.A.; Weeks, J.C.; Ayanian, J.Z. Aggressiveness of cancer care near the end of life: Is it a quality-of-care issue? J. Clin. Oncol. 2008, 26, 3860–3866. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.P.; Wu, C.Y.; Hwang, I.H.; Kao, C.H.; Hung, Y.P.; Hwang, S.J.; Li, C.-P. How different is the care of terminal pancreatic cancer patients in inpatient palliative care units and acute hospital wards? A nationwide population-based study. BMC Palliat. Care 2016, 15, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Merchant, S.J.; Brogly, S.B.; Goldie, C.; Booth, C.M.; Nanji, S.; Patel, S.V.; Lajkosz, K.; Baxter, N.N. Palliative Care is Associated with Reduced Aggressive End-of-Life Care in Patients with Gastrointestinal Cancer. Ann. Surg. Oncol. 2018, 25, 1478–1487. [Google Scholar] [CrossRef] [PubMed]
- Davies, E.; Higginson, I.J.; World Health Organization. Better Palliative Care for Older People; Regional Office for Europe: Copenhagen, Denmark; World Health Organization: Genève, Switzerland, 2004. [Google Scholar]
- Mohammed, A.A.; Al-Zahrani, O.; Salem, R.A.; Elsayed, F.M. Aggressive Care at the End of Life; Where Are We? Indian J. Palliat. Care 2019, 25, 539–543. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Total | Hospice Service | p-Value | |||
|---|---|---|---|---|---|---|
| Non-User | User | |||||
| Total (N, %) | 25,009 | 20,749 (83.0) | 4260 (17.0) | |||
| Age Group (N, %) | ||||||
| 80- | 6285 (25.1) | 5204 (82.8) | 1081 (17.2) | <0.01 | ||
| 70–79 | 9184 (36.7) | 7657 (83.4) | 1527 (16.6) | |||
| 60–69 | 6195 (24.8) | 5181 (83.6) | 1014 (16.4) | |||
| 50–59 | 2616 (10.5) | 2132 (81.5) | 484 (18.5) | |||
| −49 | 729 (2.9) | 575 (78.9) | 154 (21.1) | |||
| Gender (N, %) | ||||||
| Male | 18,917 (75.6) | 15,803 (83.5) | 3114 (16.5) | <0.01 | ||
| Female | 6080 (24.4) | 4936 (81.2) | 1144 (18.8) | |||
| Health Insurance (N, %) | ||||||
| Self-employed insured | 7300 (29.2) | 6092 (83.5) | 1208 (16.5) | <0.01 | ||
| Employee insured | 15,481 (61.9) | 12,725 (82.2) | 2756 (17.8) | |||
| Medical Aid | 2216 (8.9) | 1922 (86.7) | 294 (13.3) | |||
| Income Level (N, %) | ||||||
| 1st Quintile | 2603 (10.4) | 2245 (86.2) | 358 (13.8) | <0.01 | ||
| 2nd Quintile | 4363 (17.4) | 3625 (83.1) | 738 (16.9) | |||
| 3rd Quintile | 4170 (16.7) | 3472 (83.3) | 698 (16.7) | |||
| 4th Quintile | 5400 (21.6) | 4489 (83.1) | 911 (16.9) | |||
| 5th Quintile | 8473 (33.9) | 6918 (81.6) | 1555 (18.4) | |||
| Diagnosed year (N, %) | ||||||
| 2014 | 1445 (5.8) | 1122 (77.6) | 323 (22.4) | <0.01 | ||
| 2015 | 2886 (11.5) | 2278 (78.9) | 608 (21.1) | |||
| 2016 | 7411 (29.6) | 6087 (82.1) | 1324 (17.9) | |||
| 2017 | 8405 (33.6) | 7057 (84.0) | 1348 (16.0) | |||
| 2018 | 4862 (19.4) | 4205 (86.5) | 657 (13.5) | |||
| Survival Time (day) (Mean, SD) | 323 | 311 (326) | 382 (350) | <0.01 | ||
| Hospital charges per day (1 M before death) (Mean, SD) | 290,973 | 297,333 (312,473) | 260,017 (122,071) | <0.01 | ||
| Hospital charges per day (3 M before death) (Mean, SD) | 268,738 | 274,031 (262,168) | 242,977 (156,739) | <0.01 | ||
| Hospital charges per day (6 M before death) (Mean, SD) | 267,626 | 272,055 (244,318) | 246,068 (158,531) | <0.01 | ||
| Variables | One Month Before Death Spending (KRW) | p-Value | Three Months Before Death Spending (KRW) | p-Value | Six Month Before Death Spending (KRW) | p-Value |
|---|---|---|---|---|---|---|
| Hospice Service | ||||||
| Non-User | ref | ref | ref | |||
| User | −33,806 | <0.01 | −25,948 | <0.01 | −20,620 | <0.01 |
| Age Group | ||||||
| 80- | ref | ref | ref | |||
| 70–79 | 50,833 | <0.01 | 41,150 | <0.01 | 43,586 | <0.01 |
| 60–69 | 83,805 | <0.01 | 72,689 | <0.01 | 76,135 | <0.01 |
| 50–59 | 113,926 | <0.01 | 104,677 | <0.01 | 109,322 | <0.01 |
| −49 | 148,995 | <0.01 | 128,106 | <0.01 | 132,039 | <0.01 |
| Gender | ||||||
| Male | ref | ref | ref | |||
| Female | 10,094 | 0.02 | 9959 | 0.01 | 8216 | 0.02 |
| Health Insurance | ||||||
| Self-employed insured | 38,082 | 0.02 | 40,289 | <0.01 | 33,487 | 0.01 |
| Employee insured | 41,559 | 0.01 | 37,818 | 0.01 | 34,009 | 0.01 |
| Medical aid | ref | ref | ref | |||
| Income Level | ||||||
| 1st Quintile | ref | ref | ref | |||
| 2nd Quintile | −9626 | 0.53 | −14,088 | 0.28 | −10,186 | 0.41 |
| 3rd Quintile | −8151 | 0.60 | −11,812 | 0.37 | −8129 | 0.51 |
| 4th Quintile | −6513 | 0.67 | −12,804 | 0.33 | −7013 | 0.57 |
| 5th Quintile | −1951 | 0.90 | −9788 | 0.45 | −5114 | 0.67 |
| Diagnosed year | ||||||
| 2014 | ref | ref | ref | |||
| 2015 | 3935 | 0.69 | −8729 | 0.30 | −126 | 0.99 |
| 2016 | 11,145 | 0.31 | −3397 | 0.72 | 3761 | 0.67 |
| 2017 | 43,760 | <0.01 | 36,911 | <0.01 | 46,396 | <0.01 |
| 2018 | 82,069 | <0.01 | 71,921 | <0.01 | 77,092 | <0.01 |
| Survival Time (days) | −7.8 | 0.40 | −24.3 | <0.01 | −28.7 | <0.01 |
| Variables | One Month Before Death Spending (KRW) | p-Value | Three Month Before Death Spending (KRW) | p-Value | Six Month Before Death Spending (KRW) | p-Value |
|---|---|---|---|---|---|---|
| Hospice Service | ||||||
| Non-User | ref | ref | ref | |||
| User | −18,178 | <0.01 | −9577 | 0.04 | −4732 | 0.03 |
| Age Group | ||||||
| 80– | ref | ref | ref | |||
| 70–79 | 32,581 | <0.01 | 30,706 | <0.01 | 33,992 | <0.01 |
| 60–69 | 64,879 | <0.01 | 54,407 | <0.01 | 56,818 | <0.01 |
| 50–59 | 86,492 | <0.01 | 94,790 | <0.01 | 84,199 | <0.01 |
| −49 | 87,369 | <0.01 | 84,213 | <0.01 | 76,009 | <0.01 |
| Gender | ||||||
| Male | ref | ref | ref | |||
| Female | 22,619 | <0.01 | 19,275 | <0.01 | 13,400 | 0.04 |
| Health Insurance | ||||||
| Self-employed insured | 17,212 | 0.50 | 24,767 | 0.26 | 31,141 | 0.15 |
| Employee insured | 20,219 | 0.42 | 25,582 | 0.23 | 32,859 | 0.11 |
| Medical Aid | ref | ref | ref | |||
| Income Level | ||||||
| 1st Quintile | ref | ref | ref | |||
| 2nd Quintile | −5379 | 0.82 | −5072 | 0.80 | −11,698 | 0.56 |
| 3rd Quintile | −1198 | 0.96 | −3406 | 0.87 | −5417 | 0.79 |
| 4th Quintile | −8805 | 0.71 | −9707 | 0.63 | −17,565 | 0.38 |
| 5th Quintile | −4528 | 0.85 | −8200 | 0.68 | −14,298 | 0.47 |
| Diagnosed year | ||||||
| 2014 | ref | ref | ref | |||
| 2015 | −11,487 | 0.63 | −4007 | 0.85 | 21,118 | 0.29 |
| 2016 | 9622 | 0.70 | −665 | 0.98 | 15,805 | 0.45 |
| 2017 | 29,505 | 0.26 | 29,481 | 0.18 | 46,727 | 0.03 |
| 2018 | 63,641 | 0.02 | 57,447 | 0.01 | 74,933 | <0.01 |
| Survival Time (days) | −3.7 | 0.84 | −36.0 | 0.02 | −27.3 | 0.07 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.J.; Kim, S.J. Is Hospital Hospice Service Associated with Efficient Healthcare Utilization in Deceased Lung Cancer Patients? Hospital Charges at Their End of Life. Int. J. Environ. Res. Public Health 2022, 19, 15331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192215331
Kim DJ, Kim SJ. Is Hospital Hospice Service Associated with Efficient Healthcare Utilization in Deceased Lung Cancer Patients? Hospital Charges at Their End of Life. International Journal of Environmental Research and Public Health. 2022; 19(22):15331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192215331
Chicago/Turabian StyleKim, Dong Jun, and Sun Jung Kim. 2022. "Is Hospital Hospice Service Associated with Efficient Healthcare Utilization in Deceased Lung Cancer Patients? Hospital Charges at Their End of Life" International Journal of Environmental Research and Public Health 19, no. 22: 15331. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192215331