
Impact of the Empathic Understanding of People and Type D Personality as the Correlates of Social Skills of Primary Health Care Nurses: A Cross-Sectional Study
 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
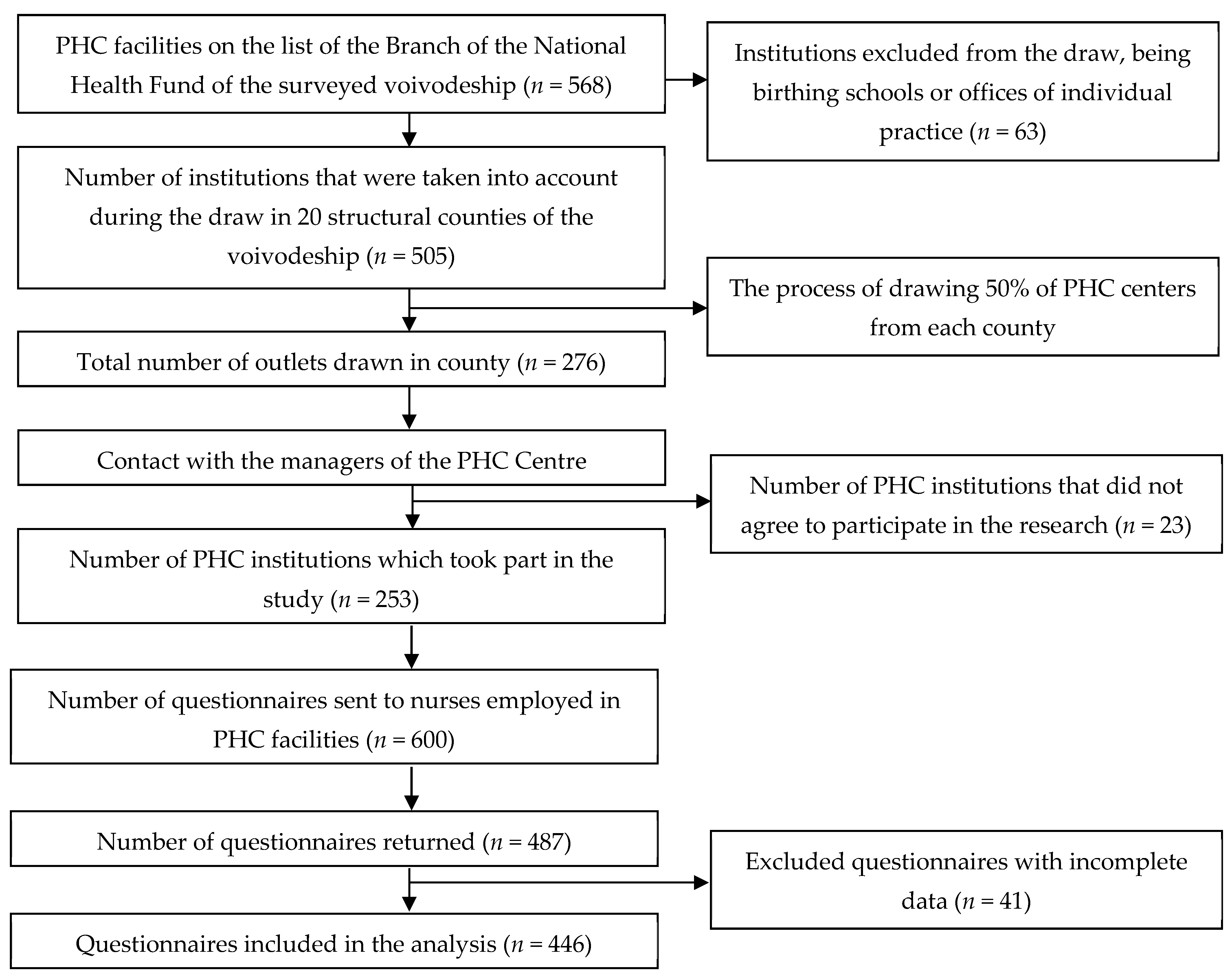
2.1. Study Design
2.2. Ethics Approval
2.3. Questionnaires
2.3.1. Assessment of Social Skills
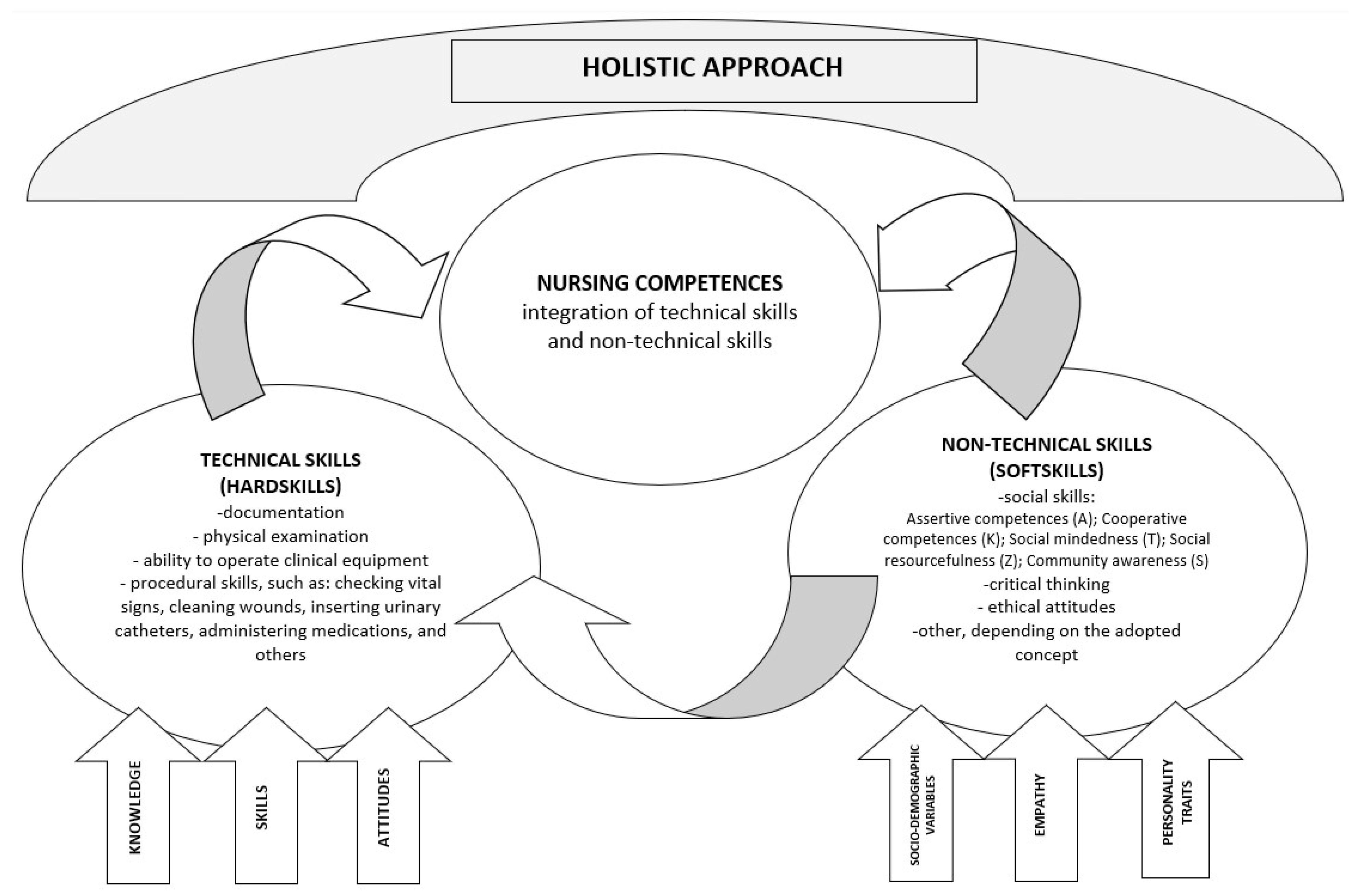
- Assertive competences subscale (A—14 items)—this assesses each respondent’s ability to influence other people and the ability to refuse or object. The score in the subscale ranged from 14 to 56 points.
- Cooperative competences subscale (K—16 items)—this assesses the skills of establishing cooperation and resolving interpersonal conflicts. The score in the subscale ranged from 16 to 64 points.
- Social mindedness subscale (T—11 items) assesses the ability to establish and maintain social relationships. The score in the subscale ranged from 11 to 44 points.
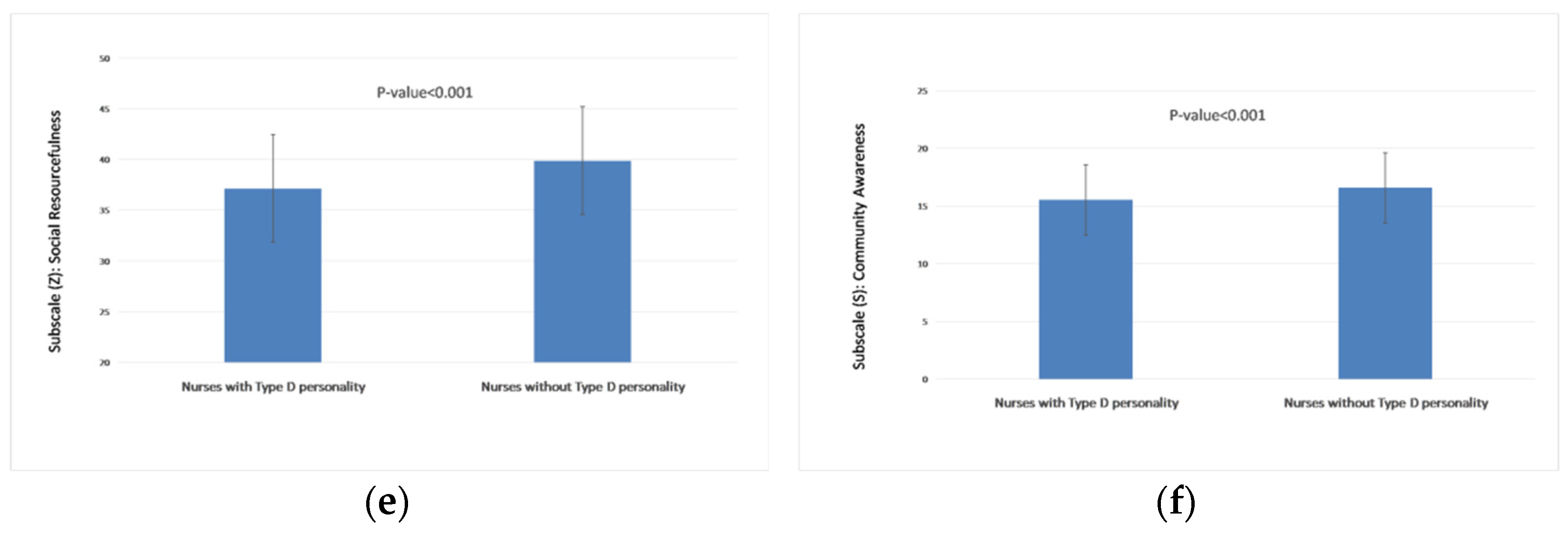
- Social resourcefulness subscale (Z—13 items)—this assesses the ability to enforce one’s rights and privileges and influence others in achieving one’s goals. The score in the subscale ranged from 13 to 52 points.
- Subscale community awareness (S—6 items)—this assesses the ability to initiate and implement social goals, as well as engage others in these goals. The score ranged from 6 to 24 points.
2.3.2. Empathy Level Assessment
2.3.3. Severity of Type D Personality Traits
2.3.4. Sociodemographic Variables
2.4. Statistical Analyses
3. Results
3.1. Characteristics of Participants
3.2. Distribution of Analysed Characteristics According to PROKOS, KRE and DS-14
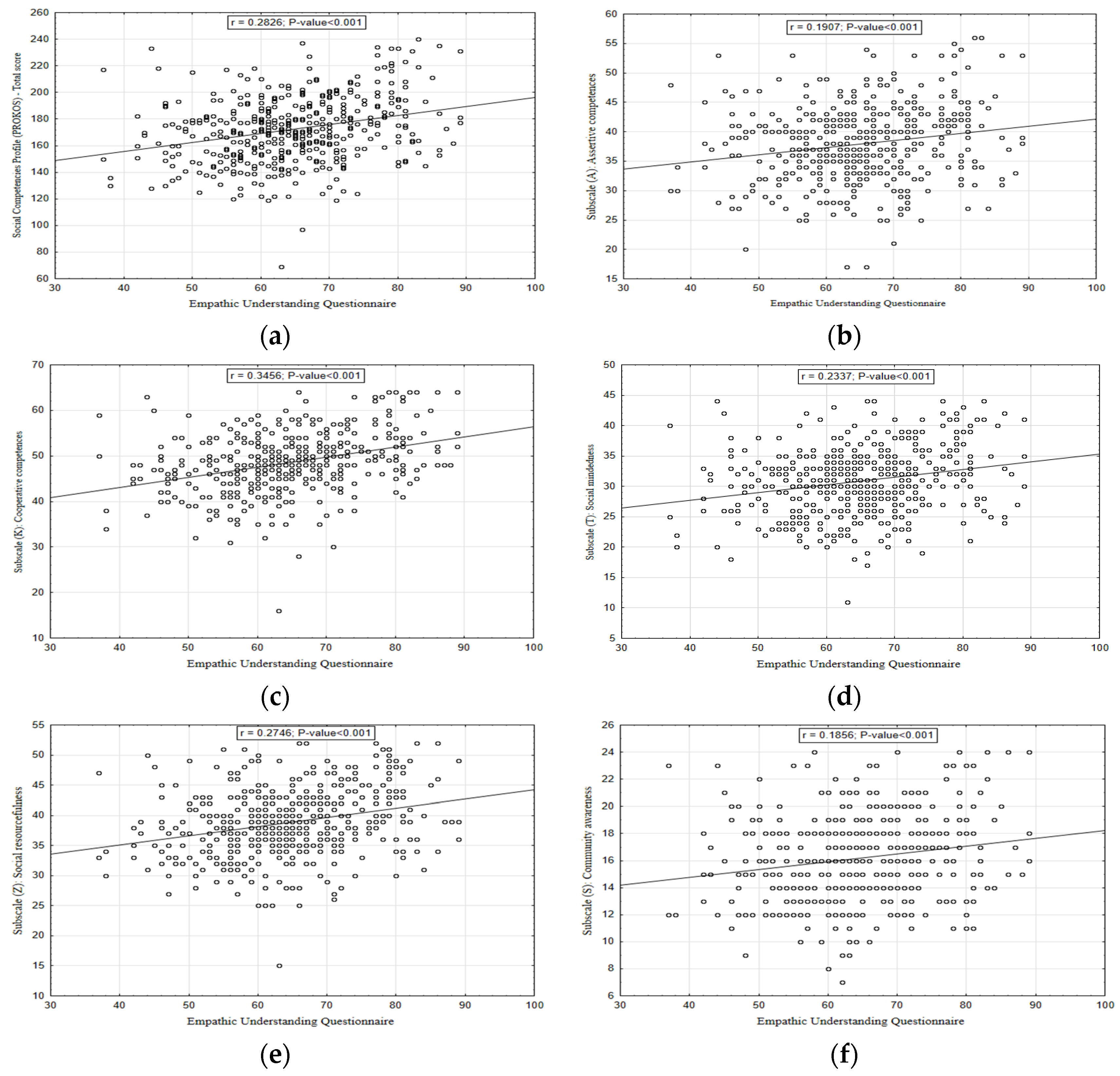
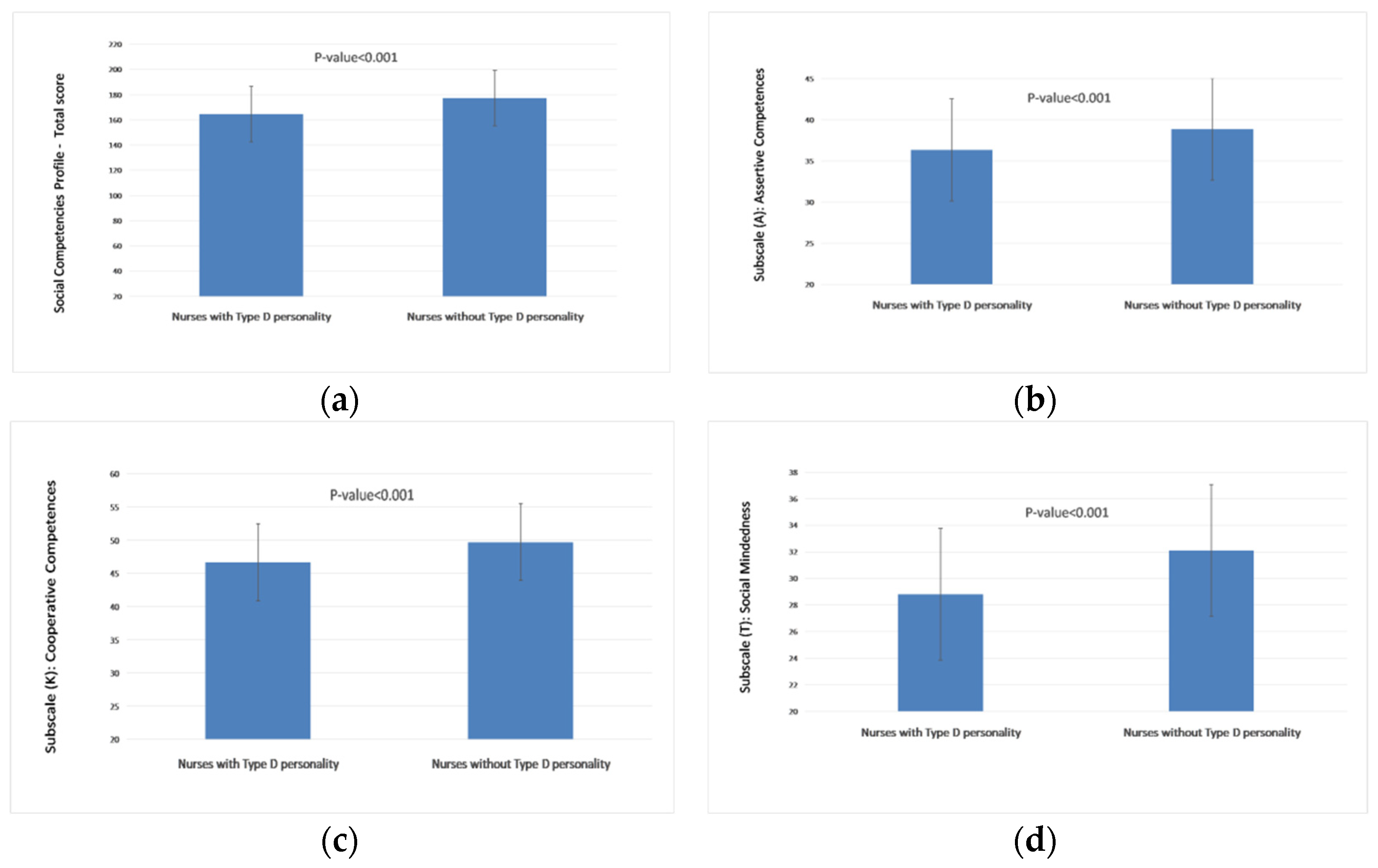
3.3. Relationship between Empathic Understanding Questionnaire, Type D Personality and Social Competences
3.4. Multivariable Analysis between Empathic Understanding Questionnaire, Type D Personality and Social Competences
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Competences for Nurses Working in Primary Health Care. 2020. Available online: https://www.euro.who.int/en/health-topics/Health-systems/nursing-and-midwifery/publications/2020/competencies-for-nurses-working-in-primary-health-care-2020 (accessed on 15 September 2022).
- Bagnasco, A.; Catania, G.; Zanini, M.; Pozzi, F.; Aleo, G.; Watson, R.; Hayter, M.; Sasso, L. Core competencies for family and community nurses: A European e-Delphi study. Nurse Educ. Pract. 2022, 60, 103296. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Family Health Nurse: Context, Conceptual Framework and Curriculum. 2000. Available online: https://www.euro.who.int/en/health-topics/Health-systems/nursing-and-midwifery/publications/2000/the-family-health-nurse-context,-conceptual-framework-and-curriculum (accessed on 15 September 2022).
- Fukada, M. Nursing Competency: Definition, Structure and Development. Yonago Acta Med. 2018, 61, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, S.M.; Fang, S.C.; Hung, C.T.; Chen, Y.H. Psychometric evaluation of a nursing competence assessment tool among nursing students: A development and validation study. BMC Med. Educ. 2022, 22, 372. [Google Scholar] [CrossRef] [PubMed]
- Takase, M.; Teraoka, S. Development of the Holistic Nursing Competence Scale. Nurs. Health Sci. 2011, 13, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Japanese Nursing Association. Nursing Clinical Ladder, Japan Nurses Association Version: A Guidebook for Practical Use. 2. Introduction/Practical Use Edition; Japanese Nursing Association: Tokyo, Japan, 2016. [Google Scholar]
- Ewertsson, M.; Gustafsson, M.; Blomberg, K.; Holmström, I.K.; Allvin, R. Use of technical skills and medical devices among new registered nurses: A questionnaire study. Nurse Educ. Today 2015, 35, 1169–1174. [Google Scholar] [CrossRef]
- Cimatti, B. Definition, development, assessment of soft skills and their role for the quality of organizations and enterprises. Int. J. Qual. Res. 2016, 10, 97–130. Available online: http://ijqr.net/journal/v10-n1/5.pdf (accessed on 15 September 2022).
- Prodanovic, M.M. The Delicate Mechanism of Politeness as a Strong Soft Skill. IUP J. Soft Ski. 2014, 8, 7–19. Available online: https://ssrn.com/abstract=2640010 (accessed on 15 September 2022).
- Jain, S.; Anjuman, A.S.S. Facilitating the Acquisition of Soft Skills Through Training. IUP J. Soft Ski. 2013, 7, 32–39. Available online: https://ssrn.com/abstract=2346051 (accessed on 15 September 2022).
- Matczak, A.; Martowska, K. Social Competencies Profile PROKOS; Psychological Test Laboratory of the Polish Psychological Association: Warsaw, Poland, 2013; pp. 5–65. [Google Scholar]
- Ray, J.D.; Overman, A.S. Hard facts about soft skills. Am. J. Nurs. 2014, 114, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Little, S.G.; Swangler, J.; Akin-Little, A. Defining Social Skills. In Handbook of Social Behavior and Skills in Children; Autism and Child Psychopathology Series; Matson, J., Ed.; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar] [CrossRef]
- Argyle, M. Social skills. In Abilities and Learning Processes; Mackintosh, N.J., Colman, A.M., Eds.; Zyski S-ka Publisher: Poznan, Poland, 2002; pp. 5–30. [Google Scholar]
- Lang, N.C. The Concepts of Social Competence and Social Noncompetence. In Group Work Practice to Advance Social Competence: A Specialized Methodology for Social Work; Columbia University Press: New York, NY, USA, 2010; pp. 19–20. [Google Scholar]
- Reitz, S. Improving Social Competence via E-Learning? The Example of Human Rights Education; Peter Lang GmbH: Frankfurt, Germany, 2012; pp. 4–30. [Google Scholar]
- Jurevičienė, M.; Kaffemaniene, I.; Ruškus, J. Concept and Structural Components of Social Skills. Balt. J. Sport Health Sci. 2018, 3, 42–52. [Google Scholar] [CrossRef]
- Semrud-Clikeman, M. Social Competence in Children; Springer: Berlin, Germany, 2007; pp. 1–9. [Google Scholar] [CrossRef]
- Matczak, A. Social Competencies Questionnaire; Psychological Test Laboratory of the Polish Psychological Association: Warsaw, Poland, 2007; pp. 5–52. [Google Scholar]
- Gokel, O.; Gokmen, D. Effects of Social Skill Training Program on Social Skill of Young People. Eurasia J. Math. Sci. Technol. Educ. 2017, 13, 7365–7373. [Google Scholar] [CrossRef] [PubMed]
- Losa-Iglesias, M.E.; López López, D.; Rodriguez Vazquez, R.; Becerro de Bengoa-Vallejo, R. Relationships between social skills and self-esteem in nurses: A questionnaire study. Contemp. Nurse 2017, 53, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.J. Patient satisfaction reporting and its implications for patient care. AMA J. Ethics 2015, 7, 616–621. [Google Scholar] [CrossRef] [Green Version]
- Amoah, V.M.K.; Anokye, R.; Boakye, D.S.; Acheampong, E.; Budu-Ainooson, A.; Okyere, E.; Afriyie, J.O. A qualitative assessment of perceived barriers to effective therapeutic communication among nurses and patients. BMC Nurs. 2019, 18, 4. [Google Scholar] [CrossRef]
- Nisa, S.N.; Hussain, M.; Afzal, M.; Gilani, S.A. Quality of nurse patient therapeutic communication and overall patient satisfaction during their hospitalization stay. Int. J. Med. Sci. Public Health 2017, 6, 675–680. [Google Scholar]
- Nursing and Midwifery Council. The Code: Standards of Conduct; Performance and Ethics for Nurses; Midwives and Nurse Associates; Nursing and Midwifery Council: London, UK, 2018; Available online: https://www.nmc.org.uk/standards/code/ (accessed on 18 September 2022).
- Müller, R.; Peter, C.; Cieza, A.; Post, M.W.; Van Leeuwen, C.M.; Werner, C.S.; Geyh, S. Social skills: A resource for more social support, lower depression levels, higher quality of life, and participation in individuals with spinal cord injury? Arch. Phys. Med. Rehabil. 2015, 96, 447–455. [Google Scholar] [CrossRef] [Green Version]
- Brunero, S.; Cowan, D.; Chaniang, S.; Lamont, S. Empathy education in post-graduate nurses: An integrative review. Nurse Educ. Today 2022, 112, 105338. [Google Scholar] [CrossRef]
- Vioulac, C.; Aubree, C.; Massy, Z.A.; Untas, A. Empathy and stress in nurses working in haemodialysis: A qualitative study. J. Adv. Nurs. 2016, 72, 1075–1085. [Google Scholar] [CrossRef]
- de Kemp, R.A.; Overbeek, G.; de Wied, M.; Engels, R.C.; Scholte, R.H. Early adolescent empathy, parental support, and antisocial behavior. J. Genet. Psychol. 2007, 168, 5–18. [Google Scholar] [CrossRef]
- Sher, L. Type D personality: The heart, stress, and cortisol. QJM Int. J. Med. 2005, 98, 323–329. [Google Scholar] [CrossRef] [Green Version]
- Ogińska-Bulik, N.; Juczyński, Z.; Denollet, J. Type D personality scale DS-14. In Tools for Measuring Stress and for Coping with Stress; Juczyński, Z., Ogińska-Bulik, N., Eds.; Psychological Test Laboratory of the Polish Psychological Association: Warsaw, Poland, 2013; pp. 71–85. [Google Scholar]
- Chrzan-Rodak, A.; Ślusarska, B. Empathy and Type D personality as the correlates of level of social skills of Primary Health Carenurses. Nurs. 21st Century 2022, 21, 143–150. [Google Scholar] [CrossRef]
- National Health Fund of Poland. List of Providers PHC. 2019. Available online: https://aplikacje.nfz.gov.pl/umowy/Provider/SearchResults?Year=2019&Branch=03&ServiceType=01&Code=&Name=&City=&Nip=&Regon=&Product= (accessed on 18 September 2022).
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Węgliński, A. Empathic Understanding of Other People Questionnaire—KRE-II. In Social Rehabilitation Diagnostics; Wojnarska, A., Ed.; UMCS Publisher: Lublin, Poland, 2010; pp. 67–90. [Google Scholar]
- Denollet, J. DS14: Standard Assessment of Negative Affectivity; Social Inhibition; and Type D Personality. Psychosom. Med. 2005, 67, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Maharaj, S.; Lees, T.; Lal, S. Prevalence and Risk Factors of Depression, Anxiety, and Stress in a Cohort of Australian Nurses. Int. J. Environ. Res. Public Health 2019, 16, 61. [Google Scholar] [CrossRef] [Green Version]
- Wesołowska, K.; Elovainio, M.; Gluschkoff, K.; Hietapakka, L.; Kaihlanen, A.M.; Lehtoaro, S.; Heponiemi, T. Psychosocial work environment and cross-cultural competence among native and foreign-born registered nurses. Res. Nurs. Health 2019, 42, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Marcinowicz, L.; Wojnar, D.; Terlikowski, S.J. Work activities of Primary Health Carenurses in Poland: National survey results. BMC Nurs. 2021, 20, 22. [Google Scholar] [CrossRef]
- Kirca, N.; Bademli, K. Relationship between communication skills and care behaviors of nurses. Perspect. Psychiatr. Care 2019, 55, 624–631. [Google Scholar] [CrossRef]
- Iwanow, L.; Jaworski, M.; Gotlib, J.; Panczyk, M. A Model of Factors Determining Nurses’ Attitudes towards Learning Communicative Competences. Int. J. Environ. Res. Public Health 2021, 18, 1544. [Google Scholar] [CrossRef]
- Takase, M.; Yamamoto, M.; Sato, Y. Effects of nurses’ personality traits and their environmental characteristics on their workplace learning and nursing competence. J. Nurs. Sci. 2018, 15, 167–180. [Google Scholar] [CrossRef]
- Moudatsou, M.; Stavropoulou, A.; Philalithis, A.; Koukouli, S. The Role of Empathy in Health and Social Care Professionals. Healthcare 2020, 8, 26. [Google Scholar] [CrossRef] [Green Version]
- Ruiz de Azua, S.; Ozamiz-Etxebarria, N.; Ortiz-Jauregui, M.A.; Gonzalez-Pinto, A. Communicative and Social Skills among Medical Students in Spain: A Descriptive Analysis. Int. J. Environ. Res. Public Health. 2020, 17, 1408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipp, M.J.; Riolo, C.; Riolo, M.; Farkas, J.; Liu, T.; Cisneros, G.J. Showing you care: An empathetic approach to doctor–patient communication. Semin. Orthod. 2016, 22, 88–94. [Google Scholar] [CrossRef]
- Kraft-Todd, G.T.; Reinero, D.A.; Kelley, J.M.; Heberlein, A.S.; Baer, L.; Riess, H. Empathic nonverbal behavior increases ratings of both warmth and competence in a medical context. PLoS ONE 2017, 12, e0177758. [Google Scholar] [CrossRef] [PubMed]
- Hasani, P.A.M.; Mokhtaree, M.; Fathollahi, M.S.; Farrokjzadian, J. Interpersonal communication skills and its association with personality dimensions of nurses in Rafsanjan University of Medical Sciences Iran in 2015. J. Occup. Health 2018, 7, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Gieniusz-Wojczyk, L.; Dąbek, J.; Kulik, H.; Wojczyk, S. Health-related behaviours of nurses in Poland: The role of Type D personality. J. Nurs. Manag. 2020, 28, 1725–1739. [Google Scholar] [CrossRef]
- Cho, G.J.; Kang, J. Type D personality and post-traumatic stress disorder symptoms among intensive care unit nurses: The mediating effect of resilience. PLoS ONE 2017, 12, e0175067. [Google Scholar] [CrossRef]
- Lee, J.Y.; Kim, S.Y. Mediating effects of emotional intelligence and resilience on the relationship between type D personality and caring ability in nursing students: A cross-sectional study. Nurse Educ. Today 2021, 107, 105151. [Google Scholar] [CrossRef]
- Nyklíček, I.; van Beugen, S.; Denollet, J. Effects of mindfulness-based stress reduction on distressed (type D) personality traits: A randomized controlled trial. J. Behav. Med. 2013, 36, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Bar Avrech, M.; Katz Leurer, M.; Warshawski, S.; Itzhaki, M. The role of personal resilience and personality traits of healthcare students on their attitudes towards interprofessional collaboration. Nurse Educ. Today 2018, 61, 36–42. [Google Scholar] [CrossRef]
- Heydari, A.; Kareshki, H.; Armat, M.R. Is Nurses’ Professional Competence Related to Their Personality and Emotional Intelligence? A Cross-Sectional Study. J. Caring Sci. 2016, 5, 121–132. [Google Scholar] [CrossRef]
- Hullman, G.A.; Planisek, A.; McNally, J.S.; Rubin, R.B. Competence, Personality, and Self-Efficacy: Relationships in an Undergraduate Interpersonal Course. Atl. J. Commun. 2010, 18, 36–49. [Google Scholar] [CrossRef]
- Mroczek, B.; Kotwas, A.; Karpeta-Pawlak, I.E.; Wolinska, W.; Rudnicki, J.; Bikowska, M.; Kurpas, D. Relationships between the level of social competence and work-related behaviors in a group of physicians, nurses, and paramedics. Int. J. Psychother. Pract. Res. 2017, 1, 15–29. [Google Scholar] [CrossRef]
- Brown, R.A.; Crookes, P.A. What are the ‘necessary’ skills for a newly graduating RN? Results of an Australian survey. BMC Nurs. 2016, 15, 23. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scales | Results |
|---|---|
| Social Competences Profile (PROKOS)—Total score b | 172.27 ± 24.52 |
| High a | 58 (13.00) |
| Average a | 291 (65.25) |
| Low a | 97 (21.75) |
| Subscale (A): Assertive competences—Total score b | 37.88 ± 6.44 |
| High a | 61 (13.68) |
| Average a | 290 (65.02) |
| Low a | 95 (21.30) |
| Subscale (K): Cooperative competences—Total score b | 48.56 ± 6.56 |
| High a | 41 (9.19) |
| Average a | 306 (68.61) |
| Low a | 99 (22.20) |
| Subscale (T): Social mindedness—Total score b | 30.82 ± 5.57 |
| High a | 55 (12.33) |
| Average a | 306 (68.61) |
| Low a | 85 (19.06) |
| Subscale (Z): Social resourcefulness—Total score b | 38.84 ± 5.64 |
| High a | 58 (13.01) |
| Average a | 295 (66.14) |
| Low a | 93 (20.85) |
| Subscale (S): Community awareness—Total score b | 16.17 ± 3.15 |
| High a | 93 (20.85) |
| Average a | 322 (72.20) |
| Low a | 31 (6.95) |
| Empathic Understanding Questionnaire (KRE) b | 64.63 ± 10.16 |
| Type D personality (DS-14)—Total score b | 20.24 ± 10.96 |
| Negative Affectivity (NA) b | 11.28 ± 6.5 |
| Social Inhibition (SI) b | 8.96 ± 5.38 |
| Nurses with Type D personality a | 172 (39) |
| Social Competences Profile (PROKOS) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Total Score | Subscale A | Subscale K | Subscale T | Subscale Z | Subscale S | ||||||
| b (SE) | p | b (SE) | p | b (SE) | p | b (SE) | p | b (SE) | p | b (SE) | p |
| Empathy level assessment: | |||||||||||
| 0.76 (0.11) | <0.001 | 0.14 (0.03) | <0.001 | 0.24 (0.03) | <0.001 | 0.14 (0.03) | <0.001 | 0.17 (0.03) | <0.001 | 0.07 (0.01) | <0.001 |
| R2 | 15% | 10% | 20% | 11% | 13% | 11% | |||||
| Type D personality (reference category: No): | |||||||||||
| −11.86 (2.28) | <0.001 | −2.98 (0.61) | <0.001 | −2.88 (0.61) | <0.001 | −3.14 (0.52) | <0.001 | −2.58 (0.53) | <0.001 | −0.96 (0.3) | 0.001 |
| R2 | 11% | 8% | 10% | 11% | 9% | 9% | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chrzan-Rodak, A.; Nowicki, G.J.; Schneider-Matyka, D.; Grochans, E.; Ślusarska, B. Impact of the Empathic Understanding of People and Type D Personality as the Correlates of Social Skills of Primary Health Care Nurses: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 201. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010201
Chrzan-Rodak A, Nowicki GJ, Schneider-Matyka D, Grochans E, Ślusarska B. Impact of the Empathic Understanding of People and Type D Personality as the Correlates of Social Skills of Primary Health Care Nurses: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(1):201. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010201
Chicago/Turabian StyleChrzan-Rodak, Agnieszka, Grzegorz Józef Nowicki, Daria Schneider-Matyka, Elżbieta Grochans, and Barbara Ślusarska. 2023. "Impact of the Empathic Understanding of People and Type D Personality as the Correlates of Social Skills of Primary Health Care Nurses: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 1: 201. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010201