
Persistent Organic Pollutant Levels in Maternal and Cord Blood Plasma and Breast Milk: Results from the Rio Birth Cohort Pilot Study of Environmental Exposure and Childhood Development (PIPA Study)
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
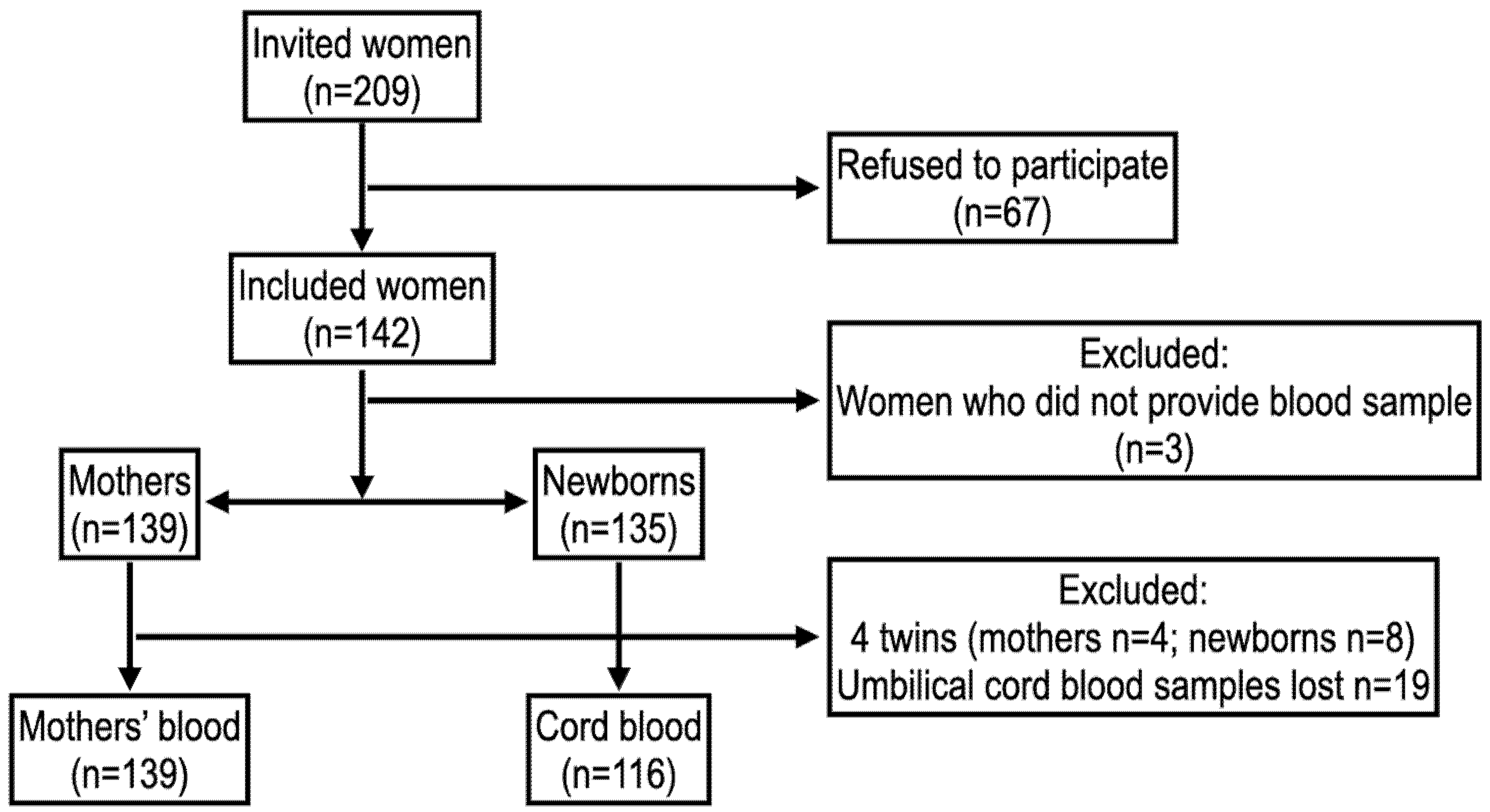
2.1. Participants and Enrollment
2.2. Sampling
2.3. Analytical Methods
2.4. Quality Assurance and Quality Control for OCP and PCB Analysis
2.5. Estimated Daily Intake and Hazard Quotient Calculations for Children
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Longnecker, M.P.; Rogan, W.J.; Lucier, G. The human health effects of ddt (dichlorodiphenyltrichloroethane) and pcbs (polychlorinated biphenyls) and an overview of organochlorines in public health. Annu. Rev. Public Health 1997, 18, 211–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, L.W.; Weber, R.; Nakano, T.; Johansson, N. PCBs risk evaluation, environmental protection, and management: 50-year research and counting for elimination by 2028. Environ. Sci. Pollut. Res. 2018, 25, 16269–16276. [Google Scholar] [CrossRef] [Green Version]
- Brazil—Ministry of the Environment. National Implementation Plan Brazil: Convention Stockholm; Ministry of the Environment: Brasília, Brazil, 2015.
- Delgado, I.F.; Barretto, H.H.; Kussumi, T.A.; Alleluia, I.B.; Baggio, C.D.A.; Paumgartten, F.J.R. Serum levels of organochlorine pesticides and polychlorinated biphenyls among inhabitants of Greater Metropolitan Rio de Janeiro, Brazil. Cad. Saúde Pública 2002, 18, 519–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricking, M.; Schwarzbauer, J. DDT isomers and metabolites in the environment: An overview. Environ. Chem. Lett. 2012, 10, 317–323. [Google Scholar] [CrossRef]
- Ferreira, V.B.; Estrella, L.F.; Alves, M.G.R.; Gallistl, C.; Vetter, W.; Silva, T.T.C.; Malm, O.; Torres, J.P.M.; Finco, F.D.B.A. Residues of legacy organochlorine pesticides and DDT metabolites in highly consumed fish from the polluted Guanabara Bay, Brazil: Distribution and assessment of human health risk. J. Environ. Sci. Health Part B 2020, 55, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Guida, Y.; de Carvalho, G.O.; Capella, R.; Pozo, K.; Lino, A.S.; Azeredo, A.; Carvalho, D.F.P.; Braga, A.L.F.; Torres, J.P.M.; Meire, R.O. Atmospheric Occurrence of Organochlorine Pesticides and Inhalation Cancer Risk in Urban Areas at Southeast Brazil. Environ. Pollut. 2021, 271, 116359. [Google Scholar] [CrossRef]
- Ródio, G.R.; Rosset, I.G.; Brandalize, A.P.C. Pesticides exposure and consequences to human health. Res. Soc. Dev. 2021, 10, e43010817526. [Google Scholar] [CrossRef]
- Bhatt, R.V. Environmental influence on reproductive health. Int. J. Gynecol. Obstet. 2000, 70, 69–75. [Google Scholar] [CrossRef]
- Makri, A.; Goveia, M.; Balbus, J.; Parkin, R. Children’s susceptibility to chemicals: A review by developmental stage. J. Toxicol. Environ. Health Part B 2004, 7, 417–435. [Google Scholar] [CrossRef]
- Woodruff, T.J.; Zota, A.; Schwartz, J.M. Environmental Chemicals in Pregnant Women in the United States: NHANES 2003–2004. Environ. Health Perspect. 2011, 119, 878–885. [Google Scholar] [CrossRef]
- Covaci, A.; Jorens, P.; Jacquemyn, Y.; Schepens, P. Distribution of PCBs and organochlorine pesticides in umbilical cord and maternal serum. Sci. Total Environ. 2002, 298, 45–53. [Google Scholar] [CrossRef]
- Heck, M.; dos Santos, J.S.; Junior, S.B.; Costabeber, I.; Emanuelli, T. Estimation of children exposure to organochlorine compounds through milk in Rio Grande do Sul, Brazil. Food Chem. 2007, 102, 288–294. [Google Scholar] [CrossRef]
- Sagiv, S.K.; Tolbert, P.E.; Altshul, L.M.; Korrick, S.A. Organochlorine Exposures During Pregnancy and Infant Size at Birth. Epidemiology 2007, 18, 120–129. [Google Scholar] [CrossRef] [PubMed]
- Eskenazi, B.; Marks, A.R.; Bradman, A.; Fenster, L.; Johnson, C.; Barr, D.B.; Jewell, N.P. In Utero Exposure to Dichlorodiphenyltrichloroethane (DDT) and Dichlorodiphenyldichloroethylene (DDE) and Neurodevelopment Among Young Mexican American Children. Pediatrics 2006, 118, 233–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirillo, P.M.; La Merrill, M.A.; Krigbaum, N.Y.; Cohn, B.A. Grandmaternal Perinatal Serum DDT in Relation to Granddaughter Early Menarche and Adult Obesity: Three Generations in the Child Health and Development Studies Cohort. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1480–1488. [Google Scholar] [CrossRef]
- Asmus, C.I.R.F.; Barbosa, A.P.; Meyer, A.; Damasceno, N.; Rosa, A.C.S.; Medronho, R.; Da Cunha, A.J.L.A.; Moreira, J.C.; Fernandes, T.V.R.D.B.; Martins, M.; et al. Rio Birth Cohort Study on Environmental Exposure and Childhood Development—PIPA Project. Ann. Glob. Health 2020, 86, 59. [Google Scholar] [CrossRef] [PubMed]
- Sarcinelli, P.N.; Pereira, A.C.S.; Mesquita, S.A.; Oliveira-Silva, J.J.; Meyer, A.; Menezes, M.A.; Alves, S.R.; Mattos, R.C.; Moreira, J.C.; Wolff, M. Dietary and reproductive determinants of plasma organochlorine levels in pregnant women in Rio de Janeiro. Environ. Res. 2003, 91, 143–150. [Google Scholar] [CrossRef]
- Environmental Protection Agency (EPA). Method 8081B Organochlorine Pesticides by Gas Chromatography; Revision; Environmental Protection Agency: Washington, DC, USA, 2007.
- INMETRO. Orientação sobre Validação de Métodos Analíticos. Documento de caráter orientativo, Pub. L. No. DOQ-CGCRE-008 Revisão; National Institute of Metrology Standardization and Industrial Quality: Rio de Janeiro, Brazil, 2020.
- Mekonen, S.; Ambelu, A.; Wondafrash, M.; Kolsteren, P.; Spanoghe, P. Exposure of infants to organochlorine pesticides from breast milk consumption in southwestern Ethiopia. Sci. Rep. 2021, 11, 22053. [Google Scholar] [CrossRef]
- Azeredo, A.; Torres, J.P.; Fonseca, M.D.F.; Britto, J.L.; Bastos, W.R.; e Silva, C.E.A.; Cavalcanti, G.; Meire, R.O.; Sarcinelli, P.N.; Claudio, L.; et al. DDT and its metabolites in breast milk from the Madeira River basin in the Amazon, Brazil. Chemosphere 2008, 73, S246–S251. [Google Scholar] [CrossRef] [Green Version]
- Souza, R.C.; Portella, R.B.; Almeida, P.V.N.B.; Pinto, C.O.; Gubert, P.; Da Silva, J.D.S.; Nakamura, T.C.; Rego, E.L.D. Human milk contamination by nine organochlorine pesticide residues (OCPs). J. Environ. Sci. Health Part B 2020, 55, 530–538. [Google Scholar] [CrossRef] [PubMed]
- IRIS—Integrated Risk Information System. p,p’-Dichlorodiphenyltrichloroethane (DDT) (CASRN 50-29-3); EPA—U.S. Environmental Protection Agency, National Center for Environmental Assessment: Washington, DC, USA, 1987.
- Zhou, P.; Wu, Y.; Yin, S.; Li, J.; Zhao, Y.; Zhang, L.; Chen, H.; Liu, Y.; Yang, X.; Li, X. National survey of the levels of persistent organochlorine pesticides in the breast milk of mothers in China. Environ. Pollut. 2011, 159, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.; Wang, D.; Ni, R.; Lin, Y.; Feng, C.; Xu, Q.; Jia, X.; Wang, G.; Zhou, Z. Organochlorine pesticides and their metabolites in human breast milk from Shanghai, China. Environ. Sci. Pollut. Res. 2015, 22, 9293–9306. [Google Scholar] [CrossRef]
- Kuang, L.; Hou, Y.; Huang, F.; Hong, H.; Sun, H.; Deng, W.; Lin, H. Pesticide residues in breast milk and the associated risk assessment: A review focused on China. Sci. Total Environ. 2020, 727, 138412. [Google Scholar] [CrossRef]
- Junqué, E.; Garcia, S.; Martínez, M.; Rovira, J.; Schuhmacher, M.; Grimalt, J.O. Changes of organochlorine compound concentrations in maternal serum during pregnancy and comparison to serum cord blood composition. Environ. Res. 2020, 182, 108994. [Google Scholar] [CrossRef]
- Cohn, B.A.; Cirillo, P.M.; Christianson, R.E. Prenatal DDT Exposure and Testicular Cancer: A Nested Case-Control Study. Arch. Environ. Occup. Health 2010, 65, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Bastos, A.M.X.; De Souza, M.D.C.B.; Filho, G.L.D.A.; Krauss, T.M.; Pavesi, T.; Silva, L.E. Organochlorine compound levels in fertile and infertile women from Rio de Janeiro, Brazil. Arq. Bras. Endocrinol. Metabol. 2013, 57, 346–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bravo, N.; Grimalt, J.O.; Chashchin, M.; Chashchin, V.P.; Odland, J. Drivers of maternal accumulation of organohalogen pollutants in Arctic areas (Chukotka, Russia) and 4,4′-DDT effects on the newborns. Environ. Int. 2019, 124, 541–552. [Google Scholar] [CrossRef]
- Bravo, N.; Hansen, S.; Økland, I.; Garí, M.; Álvarez, M.V.; Matiocevich, S.; Odland, J.; Grimalt, J.O. Influence of maternal and sociodemographic characteristics on the accumulation of organohalogen compounds in Argentinian women. The EMASAR study. Environ. Res. 2017, 158, 759–767. [Google Scholar] [CrossRef]
- Lopes, B.; Arrebola, J.; Serafim, A.; Company, R.; Rosa, J.; Olea, N. Polychlorinated biphenyls (PCBs) and p,p′-dichlorodiphenyldichloroethylene (DDE) concentrations in maternal and umbilical cord serum in a human cohort from South Portugal. Chemosphere 2014, 114, 291–302. [Google Scholar] [CrossRef]
- Walker, J.B.; Seddon, L.; McMullen, E.; Houseman, J.; Tofflemire, K.; Corriveau, A.; Weber, J.-P.; Mills, C.; Smith, S.; Van Oostdam, J. Organochlorine levels in maternal and umbilical cord blood plasma in Arctic Canada. Sci. Total Environ. 2003, 302, 27–52. [Google Scholar] [CrossRef]
- ATSDR: Toxicological Profile for Hexachlorocyclohexanes; United States of America Department of Health and Human Services, Public Health Service, Agency for Toxic Substances and Disease Registry: Washington, DC, USA, 2005.
- Asmus, C.I.R.F.; Alonzo, H.G.A.; Palácios, M.; da Silva, A.P.; Filhote, M.I.D.F.; Buosi, D.; Câmara, V.D.M. Assessment of human health risk from organochlorine pesticide residues in Cidade dos Meninos, Duque de Caxias, Rio de Janeiro, Brazil. Cad. Saude Publica 2008, 24, 755–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieira, E.D.; Torres, J.P.; Malm, O. DDT Environmental Persistence from Its Use in a Vector Control Program: A Case Study. Environ. Res. 2001, 86, 174–182. [Google Scholar] [CrossRef]
- Mohr, S.; dos Santos, J.S.; Schwanz, T.G.; Wagner, R.; Mozzaquatro, J.O.; Lorenzoni, A.S.; Costabeber, I.H. Polychlorinated biphenyls in umbilical cord serum of newborns from Rio Grande do Sul state, Brazil. Clin. Chim. Acta 2015, 451, 323–328. [Google Scholar] [CrossRef] [PubMed]
- ATSDR: Addendum to the Toxicological Profile for Polychlorinated Biphenyls; United States of America Department of Health and Human Services, Public Health Service, Agency for Toxic Substances and Disease Registry: Washington, DC, USA, 2011.
- La Merrill, M.A.; Johnson, C.L.; Smith, M.T.; Kandula, N.R.; Macherone, A.; Pennell, K.D.; Kanaya, A.M. Exposure to persistent organic pollutants (POPs) and their relationship to hepatic fat and insulin insensitivity among Asian Indian immigrants in the United States. Environ. Sci. Technol. 2019, 53, 13906–13918. [Google Scholar] [CrossRef]
- Valvi, D.; Mendez, M.A.; Martinez, D.; Grimalt, J.; Torrent, M.; Sunyer, J.; Vrijheid, M. Prenatal Concentrations of Polychlorinated Biphenyls, DDE, and DDT and Overweight in Children: A Prospective Birth Cohort Study. Environ. Health Perspect. 2012, 120, 451–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warner, M.; Rauch, S.; Coker, E.S.; Harley, K.; Kogut, K.; Sjödin, A.; Eskenazi, B. Obesity in relation to serum persistent organic pollutant concentrations in CHAMACOS women. Environ. Epidemiol. 2018, 2, e032. [Google Scholar] [CrossRef]
- Gladen, B.C.; Klebanoff, M.A.; Hediger, M.L.; Katz, S.H.; Barr, D.B.; Davis, M.D.; Longnecker, M. Prenatal DDT Exposure in Relation to Anthropometric and Pubertal Measures in Adolescent Males. Environ. Health Perspect. 2004, 112, 1761–1767. [Google Scholar] [CrossRef] [Green Version]
- Cupul-Uicab, L.A.; Klebanoff, M.A.; Brock, J.W.; Longnecker, M.P. Prenatal Exposure to Persistent Organochlorines and Childhood Obesity in the U.S. Collaborative Perinatal Project. Environ. Health Perspect. 2013, 121, 1103–1109. [Google Scholar] [CrossRef]
- LaKind, J.S.; Berlin, C.M.; Sjödin, A.; Turner, W.; Wang, R.Y.; Needham, L.L.; Paul, I.M.; Stokes, J.L.; Naiman, D.Q.; Patterson, D.G. Do Human Milk Concentrations of Persistent Organic Chemicals Really Decline During Lactation? Chemical Concentrations During Lactation and Milk/Serum Partitioning. Environ. Health Perspect. 2009, 117, 1625–1631. [Google Scholar] [CrossRef] [Green Version]
- Yu, Z.; Palkovicova, L.; Drobna, B.; Petrik, J.; Kocan, A.; Trnovec, T.; Hertz-Picciotto, I. Comparison of organochlorine compound concentrations in colostrum and mature milk. Chemosphere 2007, 66, 1012–1018. [Google Scholar] [CrossRef]
- Veyhe, A.S.; Hofoss, D.; Hansen, S.; Thomassen, Y.; Sandanger, T.M.; Odland, J.; Nieboer, E. The Northern Norway Mother-and-Child Contaminant Cohort (MISA) Study: PCA analyses of environmental contaminants in maternal sera and dietary intake in early pregnancy. Int. J. Hyg. Environ. Health 2015, 218, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.-L.; Yan, C.-H.; Yu, X.-D.; Tian, Y.; Zhao, L.; Liu, J.-X.; Shen, X.-M. Relationship between serum concentrations of polychlorinated biphenyls and organochlorine pesticides and dietary habits of pregnant women in Shanghai. Sci. Total Environ. 2011, 409, 2997–3002. [Google Scholar] [CrossRef] [PubMed]
- Brazil—Brazilian Institute of Statistics and Geography. Family Budget Survey 2017–2018; Brazilian Institute of Statistics and Geography: Rio de Janeiro, Brazil, 2019; ISBN 978-85-240-4505-9. Available online: https://biblioteca.ibge.gov.br/index.php/bibliotecacatalogo?view=detalhes&id=2101749 (accessed on 2 November 2022).
- Sant’Ana, L.S.; Vassilieff, I.; Jokl, L. Levels of organochlorine insecticides in milk of mothers from urban and rural areas of botucatu, SP, Brazil. Bull. Environ. Contam. Toxicol. 1989, 42, 911–918. [Google Scholar] [CrossRef]
- Matuo, Y.K.; Lopes, J.N.C.; Casanova, I.C.; Matuo, T. Organochlorine pesticide residues in human milk in the Ribeirão Preto region, state of São Paulo, Brazil. Arch. Environ. Contam. Toxicol. 1992, 22, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wu, X.; Lei, B.; Jing, Y.; Jiang, Z.; Zhang, X.; Fang, X.; Yu, Y. Transplacental transfer characteristics of organochlorine pesticides in paired maternal and cord sera, and placentas and possible influencing factors. Environ. Pollut. 2018, 233, 446–454. [Google Scholar] [CrossRef] [PubMed]
- Yin, S.; Zhang, J.; Guo, F.; Zhao, L.; Poma, G.; Covaci, A.; Liu, W. Transplacental transfer of organochlorine pesticides: Concentration ratio and chiral properties. Environ. Int. 2019, 130, 104939. [Google Scholar] [CrossRef]
- Bedi, J.S.; Gill, J.P.S.; Aulakh, R.S.; Kaur, P.; Sharma, A.; Pooni, P.A. Pesticide residues in human breast milk: Risk assessment for infants from Punjab, India. Sci. Total Environ. 2013, 463–464, 720–726. [Google Scholar] [CrossRef]
- Czaja, K.; Ludwicki, J.K.; Góralcyk, K.; Strucinski, P. Effect of age and number of deliveries on mean concentration of organochlorine compounds in human breast milk in Poland. Bull. Environ. Contam. Toxicol. 1997, 59, 407–413. [Google Scholar] [CrossRef]
- Çoc, I.; Bilgili, A.; Özdemir, M.; Özbek, H.; Bilgili, N.; Burgaz, S. Organochlorine pesticide residues in human breast milk from agricultural regions of Turkey, 1996–1996. Bull. Environ. Contam. Toxicol. 1997, 59, 577–582. [Google Scholar] [CrossRef]
- Rogan, W.J.; Gladen, B.C.; McKinney, J.D.; Carrera, N.; Hardy, P.; Thullen, J.; Tingelstad, J.; Tully, M. Polychlorinated biphenyls (PCBs) and dichlorodiphenyl dichloroethene in human milk: Effects on growth, morbity, and duration of lactation. Am. J. Public Health 1987, 77, 1294–1297. [Google Scholar] [CrossRef]
- Bates, M.N.; Hannah, D.J.; Buckland, S.J.; Taucher, J.A.; van Maanen, T. Chlorinated organic contaminants in breast milk of New Zealand women. Environ. Health Perspect. 1994, 102, 211–217. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| N | % | |
|---|---|---|
| Mothers’ | ||
| age (years) | ||
| 16–19 | 12 | 9.0 |
| 20–39 | 110 | 82.7 |
| ≥40 | 11 | 8.3 |
| Ethnicity | ||
| White | 34 | 26.4 |
| Non-white | 95 | 73.6 |
| Income * | ||
| ≤1733.33 | 36 | 31.3 |
| 1733.34–3000.00 | 52 | 45.2 |
| >3000.00 | 27 | 23.5 |
| Schooling | ||
| High school or less | 100 | 76.3 |
| Higher education | 31 | 23.7 |
| Body Mass Index | ||
| <25 | 55 | 47.0 |
| 25–29.9 | 39 | 33.3 |
| ≥30 | 23 | 19.7 |
| Alcohol consumption | ||
| Yes | 61 | 46.6 |
| No | 70 | 53.4 |
| Smoking | ||
| Never | 103 | 79.8 |
| Before pregnancy | 14 | 10.9 |
| During pregnancy | 12 | 9.3 |
| Passive smoking | ||
| Yes | 62 | 48.4 |
| No | 66 | 51.6 |
| Newborn sex | ||
| Male | 62 | 54.9 |
| Female | 51 | 45.1 |
| Birth weight (g) | ||
| <2500 | 8 | 7.0 |
| ≥2500 | 107 | 93.0 |
| Size for gestational age | ||
| Small for gestational age | 8 | 7.8 |
| Appropriate for gestational age | 84 | 81.5 |
| Large for gestational age | 11 | 10.7 |
| Gestational age (weeks) | ||
| <37 | 10 | 9.8 |
| ≥37 | 92 | 90.2 |
| Apgar 5th min | ||
| ≤8 | 22 | 19.5 |
| >8 | 91 | 80.5 |
| LOD * ng/mL | Samples > LOD N (%) | GM ** (95%CI) | Min | 25% | 50% | 75% | Max | |
|---|---|---|---|---|---|---|---|---|
| Mothers’ blood | ||||||||
| 4,4′-DDE | 0.045 | 30 (22.22) | 0.131 (0.089–0.193) | 0.050 | 0.069 | 0.087 | 0.198 | 3.196 |
| ∑DDT | - | 33 (24.44) | 0.136 (0.090–0.204) | 0.030 | 0.067 | 0.085 | 0.215 | 3.249 |
| β-HCH | 0.02 | 12 (8.89) | 0.121 (0.105–0.140) | 0.090 | 0.102 | 0.119 | 0.144 | 0.179 |
| γ-HCH | 0.07 | 10 (7.41) | 0.175 (0.150–0.205) | 0.136 | 0.145 | 0.171 | 0.216 | 0.251 |
| ∑HCH | - | 13 (9.63) | 0.230 (0.173–0.306) | 0.090 | 0.154 | 0.248 | 0.328 | 0.430 |
| ∑PCB a | - | 11 (8.15) | 0.110 (0.081–0.149) | 0.064 | 0.068 | 0.097 | 0.160 | 0.255 |
| ∑OCPs a | - | 41 (30.37) | 0.187 (0.135–0.259) | 0.030 | 0.080 | 0.171 | 0.308 | 3.249 |
| ∑POPs | - | 46 (34.07) | 0.190 (0.141–0.255) | 0.084 | 0.169 | 0.305 | 3.249 | |
| Umbilical cord blood | ||||||||
| 2,4′-DDT | 0.02 | 8 (6.90) | 0.133 (0.083–0.215) | 0.065 | 0.082 | 0.183 | 0.206 | 0.254 |
| 4,4′-DDD | 0.03 | 9 (7.76) | 0.066 (0.037–0.118) | 0.030 | 0.030 | 0.071 | 0.122 | 0.226 |
| 4,4′-DDE | 0.05 | 18 (15.52) | 0.150 (0.086–0.264) | 0.052 | 0.065 | 0.110 | 0.266 | 5.440 |
| 4,4′-DDT | 0.05 | 12 (10.34) | 0.099 (0.059–0.168) | 0.050 | 0.053 | 0.071 | 0.187 | 0.477 |
| ∑DDT | - | 33 (28.45) | 0.151 (0.100–0.227) | 0.030 | 0.064 | 0.100 | 0.334 | 6.231 |
| β-HCH | 0.02 | 13 (11.21) | 0.071 (0.047–0.105) | 0.023 | 0.038 | 0.093 | 0.119 | 0.169 |
| γ-HCH | 0.07 | 6 (5.17) | 0.157 (0.139–0.178) | 0.138 | 0.140 | 0.157 | 0.177 | 0.178 |
| ∑HCH | - | 15 (12.93) | 0.136 (0.082–0.226) | 0.023 | 0.073 | 0.178 | 0.289 | 0.442 |
| PCB 153 | 0.02 | 6 (5.17) | 0.076 (0.038–0.149) | 0.021 | 0.043 | 0.080 | 0.155 | 0.204 |
| ∑PCB b | - | 11 (9.48) | 0.225 (0.118–0.430) | 0.050 | 0.106 | 0.193 | 0.457 | 1.150 |
| ∑OCPs b | - | 40 (34.48) | 0.177 (0.124–0.252) | 0.050 | 0.074 | 0.251 | 0.558 | 6.220 |
| ∑POP | - | 41 (35.34) | 0.192 (0.130–0.284) | 0.050 | 0.074 | 0.247 | 0.734 | 6.270 |
| N; GM * (95%CI) | ||||
|---|---|---|---|---|
| ∑DDT | ∑HCH | ∑OCP | ∑POP | |
| Mothers | ||||
| Age | ||||
| 16–19 | 2; 0.07 (0.02–0.25) | 1; 0.27 (-) | 4; 0.18 (0.04–0.70) | 4; 0.18 (0.04–0.78) |
| 20–39 | 22; 0.16 (0.10–0.25) | 9; 0.21 (0.14–0.31) | 29; 0.18 (0.12–0.26) | 34; 0.18 (0.13–0.25) |
| ≥40 | 9; 0.19 (0.06–0.61) | 2; 0.12 (0.13–1.14) | 8; 0.23 (0.07–0.69) | 8; 0.23 (0.08–0.69) |
| Ethnicity | ||||
| White | 13; 0.11 (0.07–0.20) | 5; 0.29 (0.22–0.39) | 15; 0.19 (0.12–0.30) | 16; 0.19 (0.13–0.29) |
| Non-white | 19; 0.15 (0.08–0.29) | 8; 0.20 (0.13–0.31) | 25; 0.19 (0.12–0.31) | 29; 0.19 (0.12–0.29) |
| Income | ||||
| ≤1733.33 | 4; 0.21 (0.02–2.32) | 3; 0.24 (0.18–0.40) | 6; 0.27 (0.08–0.89) | 7; 0.25 (0.09–0.70) |
| 1733.34–3000.00 | 10; 0.11 (0.07–0.17) | 5; 0.24 (0.18–0.31) | 14; 0.17 (0.12–0.24) | 18; 0.17 (0.13–0.23) |
| >3000.00 | 13; 0.13 (0.06–0.30) | 4; 0.19 (0.07–0.52) | 14; 0.18 (0.09–0.38) | 14; 0.19 (0.09–0.39) |
| Body Mass Index | ||||
| <25 | 11; 0.13 (0.07–0.26) | 7; 0.28 (0.19–0.42) | 16; 0.18 (0.11–0.30) | 18; 0.19 (0.12–0.30) |
| 25–29.9 | 12; 0.10 (0.05–0.23) | 1; 0.28 (-) † | 12; 0.14 (0.07–0.31) | 13; 0.15 (0.07–0.29) |
| ≥30 | 8; 0.25 (0.09–0.72) | 3; 0.18 (0.02–0.68) | 10; 0.30 (0.15–0.60) | 10; 0.32 (0.16–0.64) |
| Newborns | ||||
| Sex | ||||
| Male | 16; 0.18 (0.11–0.30) | 9; 0.11 (0.05–0.23) | 21; 0.19 (0.13–0.29) | 22; 0.21 (0.13–0.33) |
| Female | 16; 0.13 (0.06–0.27) | 5; 0.17 (0.05–0.54) | 17; 0.16 (0.08–0.34) | 17; 0.18 (0.08–0.40) |
| Birth weight (g) | ||||
| <2500 | 3; 0.08 (0.05–0.13) | 1; 0.25 (0.01–0.86) | 4; 0.11 (0.04–0.27) | 4; 0.11 (0.04–0.27) |
| ≥2500 | 29; 0.17 (0.10–0.26) | 14; 0.13 (0.08–0.22) | 35; 0.19 (0.13–0.29) | 36; 0.21 (0.14–0.33) |
| Gestational age (weeks) | ||||
| <37 | 4; 0.11 (0.04–0.34) | 3; 0.17 (0.02–1.33) | 5; 0.16 (0.05–0.55) | 5; 0.17 (0.04–0.77) |
| ≥37 | 23; 0.16 (0.09–0.28) | 9; 0.08 (0.01–0.62) | 28; 0.19 (0.12–0.30) | 29; 0.20 (0.12–0.34) |
| Apgar 5th min | ||||
| ≤8 | 6; 0.53 (0.11–2.51) | 5; 0.08 (0.02–0.45) | 7; 0.56 (0.16–1.98) | 8; 0.54 (0.15–1.96) |
| >8 | 26; 0.12 (0.08–0.17) | 10; 0.17 (0.12–0.25) | 32; 0.14 (0.10–0.20) | 32; 0.15 (0.11–0.22) |
| ΣDDT Mother | ΣDDT Cord | ΣOCP Mother | ΣOCP Cord | ΣOC Mother | ΣOC Cord | ΣHCH Mother | ΣHCH Cord | DDE Mother | DDE Cord | DDE BM 1°m * | DDE BM 3°m ** | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ΣDDT Mother | ρ | 1.000 | 0.060 | 0.709 | 0.021 | 0.684 | 0.007 | 0.500 | 0.800 | 1.000 | −0.500 | 0.286 | 0.257 |
| p | 0.845 | <0.0001 | 0.940 | <0.0001 | 0.980 | 0.667 | 0.200 | 0.667 | 0.535 | 0.623 | |||
| n | 33 | 13 | 32 | 15 | 32 | 15 | 3 | 4 | 2 | 3 | 7 | 6 | |
| ΣDDT Cord | ρ | 1.000 | −0.006 | 0.913 | −0.029 | 0.911 | 0.500 | −0.543 | −0.700 | 0.500 | −0.400 | ||
| p | 0.983 | <0.0001 | 0.911 | <0.0001 | 0.667 | 0.266 | 0.188 | 0.667 | 0.600 | ||||
| n | 33 | 16 | 32 | 16 | 32 | 1 | 3 | 6 | 5 | 3 | 4 | ||
| ΣOCP Mother | ρ | 1.000 | −0.051 | 0.964 | −0.061 | −0.400 | −0.200 | −0.543 | 0.029 | 0.429 | 0.517 | ||
| p | 0.836 | <0.0001 | 0.803 | 0.600 | 0.704 | 0.266 | 0.957 | 0.337 | 0.154 | ||||
| n | 41 | 19 | 43 | 19 | 4 | 6 | 6 | 6 | 7 | 9 | |||
| ΣOCP Cord | ρ | 1.000 | −0.047 | 0.996 | −0.800 | −0.371 | −0.500 | 0.400 | −0.300 | ||||
| p | 0.847 | <0.0001 | 0.200 | 0.468 | 0.391 | 0.600 | 0.624 | ||||||
| n | 40 | 19 | 38 | 1 | 4 | 6 | 5 | 4 | 5 | ||||
| ΣOC Mother | ρ | 1.000 | −0.056 | −0.200 | 0.071 | −0.371 | 0.257 | 0.439 | 0.417 | ||||
| p | 0.819 | 0.747 | 0.879 | 0.468 | 0.623 | 0.337 | 0.265 | ||||||
| n | 46 | 19 | 5 | 7 | 6 | 6 | 7 | 9 | |||||
| ΣOC Cord | ρ | 1.00 | −0.800 | −0.393 | −0.543 | 0.400 | −0.300 | ||||||
| p | 0.200 | 0.383 | 0.266 | 0.600 | 0.624 | ||||||||
| n | 40 | 1 | 4 | 7 | 6 | 4 | 5 | ||||||
| ΣHCH Mother | ρ | 1.000 | 0.500 | 0.600 | 1.000 | −0.500 | 0.500 | ||||||
| p | 0.667 | 0.285 | 0.667 | 0.667 | |||||||||
| n | 13 | 3 | 5 | 3 | 3 | 3 | |||||||
| ΣHCH Cord | ρ | 1.000 | 0.551 | −0.086 | |||||||||
| p | 0.257 | 0.872 | |||||||||||
| n | 15 | 6 | 6 | 1 | 1 | ||||||||
| DDE Mother | ρ | 1.000 | 0.484 | 0.548 | −0.042 | ||||||||
| p | 0.094 | 0.160 | 0.907 | ||||||||||
| n | 30 | 13 | 8 | 10 | |||||||||
| DDE Cord | ρ | 1.000 | 0.500 | −0.300 | |||||||||
| p | 0.667 | 0.624 | |||||||||||
| n | 18 | 3 | 5 | ||||||||||
| DDE BM 1°m * | ρ | 1.000 | 0.429 | ||||||||||
| p | 0.337 | ||||||||||||
| n | 19 | 7 | |||||||||||
| DDE BM3°m ** | ρ | 1.000 | |||||||||||
| p | |||||||||||||
| n | 22 |
| Independent Variables | Coefficient (95%CI) |
|---|---|
| Univariate models | |
| Age | 0.037 (−0.012; 0.086) |
| BMI | 0.024 (−0.044; 0.093) |
| Education (high school or more) | −0.082 (−0.989; 0.823) |
| Ethnicity (non-white) | 0.131 (−0.748; 1.010) |
| Multivariate model 1 | |
| Age | 0.027 (−0.034; 0.089) |
| BMI | 0.010 (−0.067; 0.086) |
| Multivariate model 2 | |
| Age | 0.027 (−0.037; 0.092) |
| BMI | 0.010 (−0.070; 0.090) |
| Ethnicity (non-white) | 0.183 (−0.748; 1.113) |
| Dependent Variables | Coefficient (95%CI) |
|---|---|
| Univariate models | |
| Birth weight (grams) | −11.777 (−206.718; 183.164) |
| Gestational length (weeks) | −0.943 (−3.504; 1.618) |
| Apgar score 5th min | −0.441 (−0.645; −0.237) |
| Multivariate model 1 | |
| Apgar score 5th min | −0.440 (−0.648; −0.233) |
| Multivariate model 2 | |
| Apgar score 5th min | −0.405 (−0.651; −0.160) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, A.S.E.; Moreira, J.C.; Rosa, A.C.S.; Câmara, V.M.; Azeredo, A.; Asmus, C.I.R.F.; Meyer, A. Persistent Organic Pollutant Levels in Maternal and Cord Blood Plasma and Breast Milk: Results from the Rio Birth Cohort Pilot Study of Environmental Exposure and Childhood Development (PIPA Study). Int. J. Environ. Res. Public Health 2023, 20, 778. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010778
Santos ASE, Moreira JC, Rosa ACS, Câmara VM, Azeredo A, Asmus CIRF, Meyer A. Persistent Organic Pollutant Levels in Maternal and Cord Blood Plasma and Breast Milk: Results from the Rio Birth Cohort Pilot Study of Environmental Exposure and Childhood Development (PIPA Study). International Journal of Environmental Research and Public Health. 2023; 20(1):778. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010778
Chicago/Turabian StyleSantos, Aline Souza Espindola, Josino Costa Moreira, Ana Cristina Simoes Rosa, Volney Magalhães Câmara, Antonio Azeredo, Carmen Ildes Rodrigues Froes Asmus, and Armando Meyer. 2023. "Persistent Organic Pollutant Levels in Maternal and Cord Blood Plasma and Breast Milk: Results from the Rio Birth Cohort Pilot Study of Environmental Exposure and Childhood Development (PIPA Study)" International Journal of Environmental Research and Public Health 20, no. 1: 778. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010778