
Impact of Antenatal Care on Perinatal Outcomes in New South Wales, Australia: A Decade-Long Regional Perspective

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
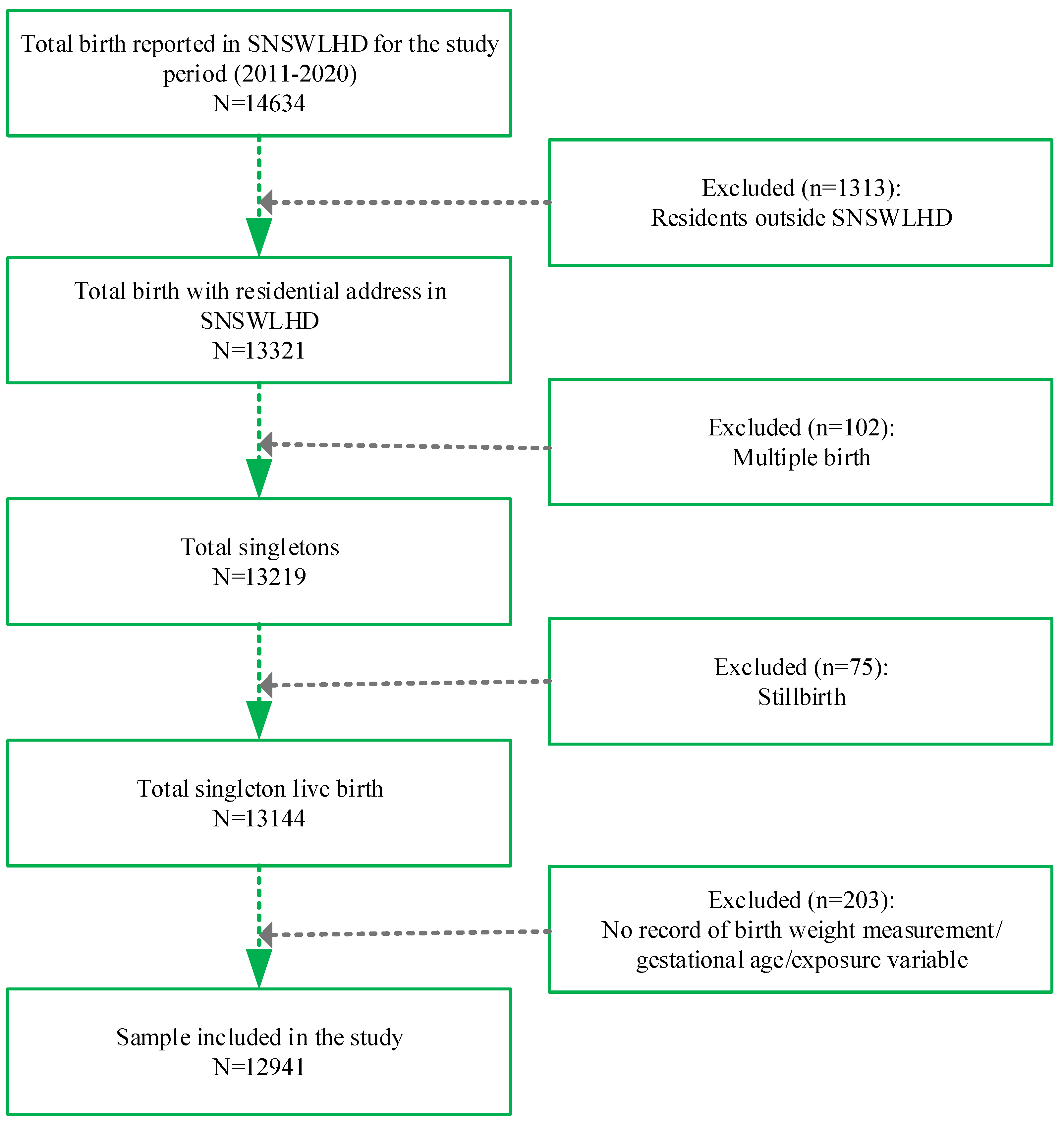
2.1. Data Source and Sample Composition
2.2. Study Outcomes
2.3. Exposure Variables
2.4. Confounders
2.5. Statistical Analysis
2.6. Ethical Consideration
3. Results
3.1. Characteristics of Study Sample
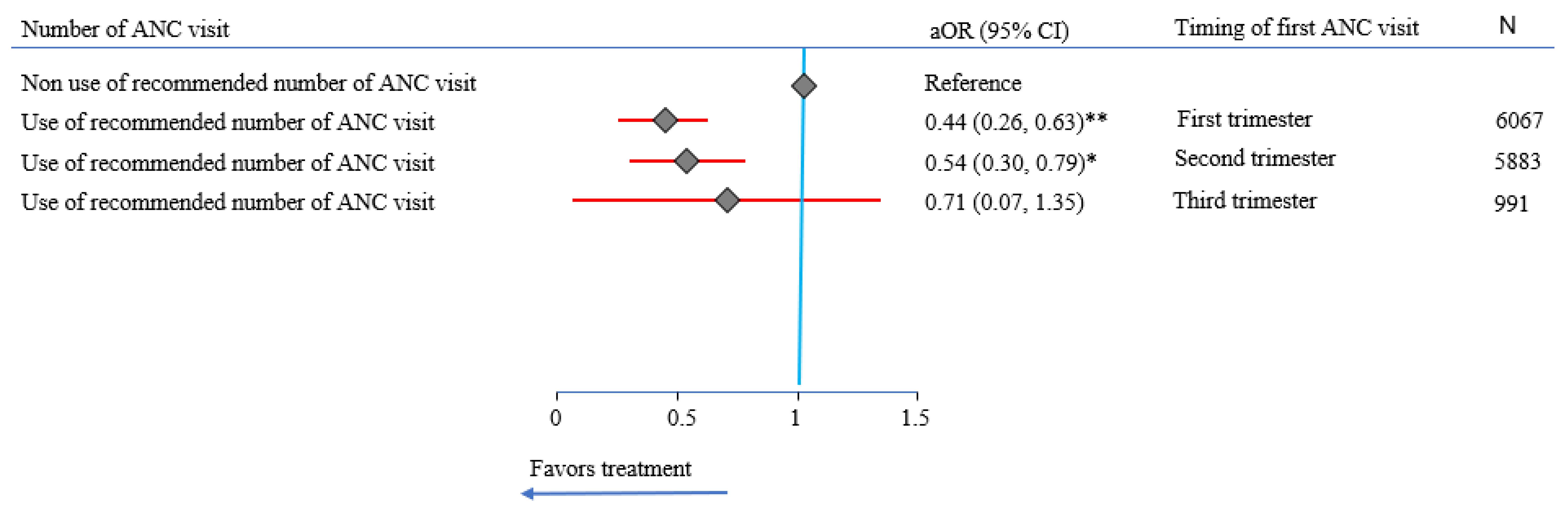
3.2. Impact of Number and Timing of ANC on LBW
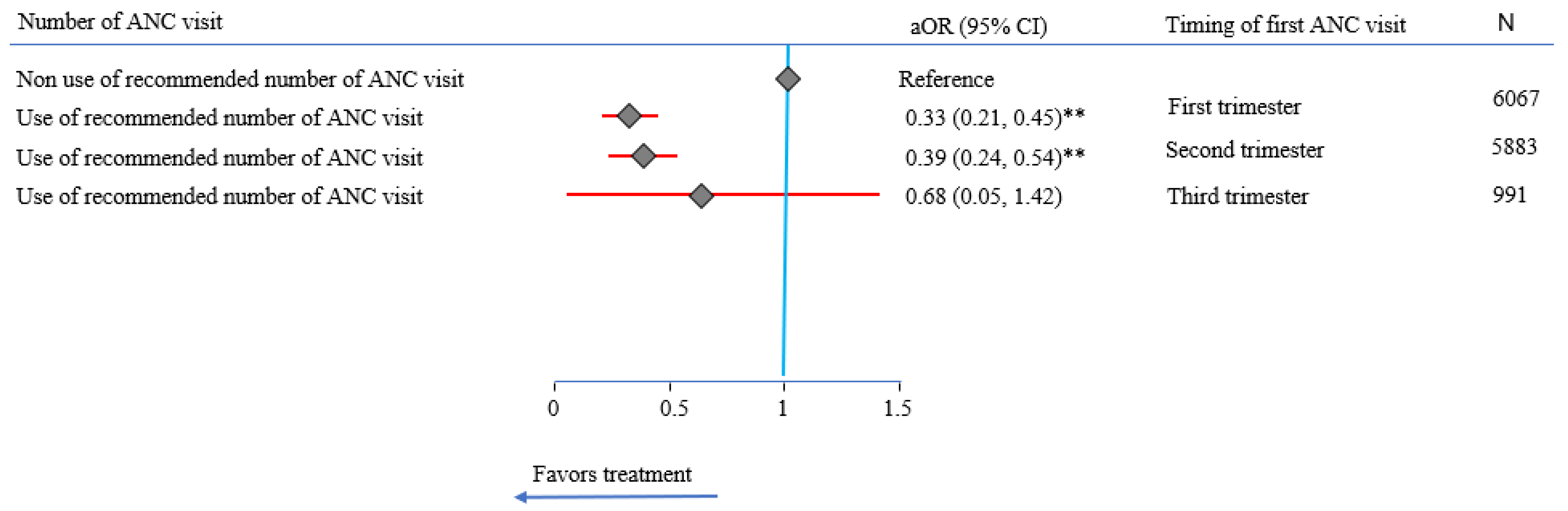
3.3. Impact of Number and Timing of ANC on Preterm Birth
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Frey, H.A.; Klebanoff, M.A. The epidemiology, etiology, and costs of preterm birth. Fetal Neonatal Med. 2016, 21, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Mathewson, K.J.; Chow, C.H.; Dobson, K.G.; Pope, E.I.; Schmidt, L.A.; Van Lieshout, R.J. Mental health of extremely low birth weight survivors: A systematic review and meta-analysis. Psychol. Bull. 2017, 143, 347. [Google Scholar] [CrossRef] [PubMed]
- Korvenranta, E.; Lehtonen, L.; Rautava, L.; Häkkinen, U.; Andersson, S.; Gissler, M.; Hallman, M.; Leipälä, J.; Peltola, M.; Tammela, O. Impact of very preterm birth on health care costs at five years of age. Pediatrics 2010, 125, e1109–e1114. [Google Scholar] [CrossRef] [PubMed]
- Achana, F.; Johnson, S.; Ni, Y.; Marlow, N.; Wolke, D.; Khan, K.; Petrou, S. Economic costs and health utility values associated with extremely preterm birth: Evidence from the EPICure2 cohort study. Paediatr. Perinat. 2022, 36, 696–705. [Google Scholar] [CrossRef]
- Henderson, J.; Carson, C.; Redshaw, M. Impact of preterm birth on maternal well-being and women’s perceptions of their baby: A population-based survey. BMJ Open 2016, 6, e012676. [Google Scholar] [CrossRef] [Green Version]
- Treyvaud, K.; Lee, K.J.; Doyle, L.W.; Anderson, P.J. Very preterm birth influences parental mental health and family outcomes seven years after birth. J. Pediatr. 2014, 164, 515–521. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.J.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Australian Burden of Disease Study: Impact and Causes of Illness and Death in Australia 2015; Australian Burden of Disease Series; Australian Institute of Health and Welfare: Canberra, Australia, 2019.
- Pregnancy Care Guidelines. Available online: https://www.health.gov.au/resources/pregnancy-care-guidelines (accessed on 1 March 2022).
- Foundations for Enhanced Maternity Data Collection and Reporting in Australia: National Maternity Data Development Project Stage 1. Available online: https://www.aihw.gov.au/getmedia/fd74001a-17f6-4676-926a-d64fde23c554/16915.pdf.aspx?inline=true (accessed on 2 August 2022).
- Maternal Deaths in Australia. Available online: https://www.aihw.gov.au/getmedia/64189da2-a826-4d42-ad23-1c36a50ac4ff/Maternal-deaths-in-Australia.pdf.aspx?inline=true (accessed on 9 December 2021).
- Australia’s Mothers and Babies. Available online: https://www.aihw.gov.au/reports/mothers-babies/australias-mothers-babies-data-visualisations/contents/summary (accessed on 1 March 2022).
- The First 2000 Days Framework. Available online: https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/PD2019_008.pdf (accessed on 7 April 2022).
- Birth—Birth Weight, Code N: Identifying and Definitional Attributes. Available online: https://meteor.aihw.gov.au/content/459938 (accessed on 13 July 2022).
- Preterm Birth. Available online: https://www.who.int/news-room/fact-sheets/detail/preterm-birth (accessed on 8 January 2022).
- Coutinho, P.R.; Cecatti, J.G.; Surita, F.G.; Souza, J.P.d.; Morais, S.S.d. Factors associated with low birth weight in a historical series of deliveries in Campinas, Brazil. Rev. Assoc. Med. Bras. 2009, 55, 692–699. [Google Scholar] [CrossRef] [Green Version]
- Wagura, P.; Wasunna, A.; Laving, A.; Wamalwa, D.; Ng’ang’a, P. Prevalence and factors associated with preterm birth at kenyatta national hospital. BMC Pregnancy Childbirth 2018, 18, 107. [Google Scholar] [CrossRef]
- Hidalgo-Lopezosa, P.; Jiménez-Ruz, A.; Carmona-Torres, J.; Hidalgo-Maestre, M.; Rodríguez-Borrego, M.; López-Soto, P. Sociodemographic factors associated with preterm birth and low birth weight: A cross-sectional study. Women Birth 2019, 32, e538–e543. [Google Scholar] [CrossRef]
- Taha, Z.; Ali Hassan, A.; Wikkeling-Scott, L.; Papandreou, D. Factors associated with preterm birth and low birth weight in Abu Dhabi, the United Arab Emirates. Int. J. Environ. Res. Public Health 2020, 17, 1382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Socio-Economic Indexes for Areas. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/allprimarymainfeatures/8C5F5BB699A0921CCA258259000BA619?opendocument (accessed on 5 September 2022).
- Victora, C.G.; Huttly, S.R.; Fuchs, S.C.; Olinto, M. The role of conceptual frameworks in epidemiological analysis: A hierarchical approach. Int. J. Epidemiol. 1997, 26, 224–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewandowska, M. Maternal obesity and risk of low birth weight, fetal growth restriction, and macrosomia: Multiple analyses. Nutrients 2021, 13, 1213. [Google Scholar] [CrossRef] [PubMed]
- Derakhshan, A.; Peeters, R.P.; Taylor, P.N.; Bliddal, S.; Carty, D.M.; Meems, M.; Vaidya, B.; Chen, L.; Knight, B.A.; Ghafoor, F. Association of maternal thyroid function with birthweight: A systematic review and individual-participant data meta-analysis. Lancet Diabetes Endocrinol. 2020, 8, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Raynes-Greenow, C. Gaps and challenges underpinning the first analysis of global coverage of early antenatal care. Lancet Glob. Health 2017, 5, e949–e950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Branco da Fonseca, C.R.; Strufaldi, M.W.L.; de Carvalho, L.R.; Puccini, R.F. Adequacy of antenatal care and its relationship with low birth weight in Botucatu, São Paulo, Brazil: A case-control study. BMC Pregnancy Childbirth 2014, 14, 255. [Google Scholar] [CrossRef] [Green Version]
- Zhou, H.; Wang, A.; Huang, X.; Guo, S.; Yang, Y.; Martin, K.; Tian, X.; Josephs-Spaulding, J.; Ma, C.; Scherpbier, R.W. Quality antenatal care protects against low birth weight in 42 poor counties of Western China. PLoS ONE 2019, 14, e0210393. [Google Scholar] [CrossRef] [Green Version]
- Beeckman, K.; Louckx, F.; Downe, S.; Putman, K. The relationship between antenatal care and preterm birth: The importance of content of care. Eur. J. Public Health 2013, 23, 366–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seear, K.H.; Spry, E.P.; Carlin, E.; Atkinson, D.N.; Marley, J.V. Aboriginal women’s experiences of strengths and challenges of antenatal care in the Kimberley: A qualitative study. Women Birth 2021, 34, 570–577. [Google Scholar] [CrossRef]
- Trinh, L.T.T.; Rubin, G. Late entry to antenatal care in New South Wales, Australia. Reprod. Health 2006, 3, 8. [Google Scholar] [CrossRef]
- Brown, A.E.; Middleton, P.F.; Fereday, J.A.; Pincombe, J.I. Cultural safety and midwifery care for Aboriginal women–A phenomenological study. Women Birth 2016, 29, 196–202. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.; Glover, K.; Weetra, D.; Ah Kit, J.; Stuart-Butler, D.; Leane, C.; Turner, M.; Gartland, D.; Yelland, J. Improving access to antenatal care for Aboriginal women in South Australia: Evidence from a population-based study. Birth 2016, 43, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Gatwiri, K.; Rotumah, D.; Rix, E. BlackLivesMatter in healthcare: Racism and implications for health inequity among Aboriginal and Torres Strait Islander Peoples in Australia. Int. J. Environ. Res. Public Health 2021, 18, 4399. [Google Scholar] [CrossRef] [PubMed]
- National Aboriginal and Torres Strait Islander Health Workforce Strategic Framework (2016–2023). Available online: https://www.health.gov.au/sites/default/files/documents/2020/12/national-aboriginal-and-torres-strait-islander-health-workforce-strategic-framework-2016-2023.pdf (accessed on 21 May 2022).
- Di, H.-K.; Gan, Y.; Lu, K.; Wang, C.; Zhu, Y.; Meng, X.; Xia, W.-Q.; Xu, M.-Z.; Feng, J.; Tian, Q.-F. Maternal smoking status during pregnancy and low birth weight in offspring: Systematic review and meta-analysis of 55 cohort studies published from 1986 to 2020. World J. Pediatr 2022, 18, 176–185. [Google Scholar] [CrossRef] [PubMed]
- Ratnasiri, A.W.; Gordon, L.; Dieckmann, R.A.; Lee, H.C.; Parry, S.S.; Arief, V.N.; DeLacy, I.H.; Lakshminrusimha, S.; DiLibero, R.J.; Basford, K.E. Smoking during pregnancy and adverse birth and maternal outcomes in California, 2007 to 2016. Am. J. Perinatol. 2020, 37, 1364–1376. [Google Scholar] [CrossRef]
- Hackshaw, A.; Rodeck, C.; Boniface, S. Maternal smoking in pregnancy and birth defects: A systematic review based on 173 687 malformed cases and 11.7 million controls. Hum. Reprod. Update 2011, 17, 589–604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabra, S.; Gratacós, E.; Roig, M.D.G. Smoking-induced changes in the maternal immune, endocrine, and metabolic pathways and their impact on fetal growth: A topical review. Fetal. Diagn. Ther. 2017, 41, 241–250. [Google Scholar] [CrossRef]
- Farrant, B.M.; White, S.W.; Shepherd, C.C. Trends and predictors of extreme preterm birth: Western Australian population-based cohort study. PLoS ONE 2019, 14, e0214445. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Study Factors | Study Sample | Low Birthweight | Preterm Birth | ||
|---|---|---|---|---|---|
| Community-level and socioeconomic factors | N (% ϕ) | n | % (95% CI) | n | % (95% CI) |
| Hospital of birth | |||||
| Cooma Health Service | 1469 (11.4) | 36 | 2.5 (1.8, 3.4) | 34 | 2.3 (1.7, 3.2) |
| Goulburn Base Hospital | 2819 (21.8) | 95 | 3.4 (2.8, 4.1) | 113 | 4.0 (3.3, 4.8) |
| Moruya District Hospital | 2750 (21.3) | 87 | 3.2 (2.6, 3.9) | 91 | 3.3 (2.7, 4.0) |
| Queanbeyan Health Service | 3569 (27.6) | 61 | 1.7 (1.3, 2.2) | 67 | 1.9 (1.5, 2.4) |
| South East Regional Hospital | 2334 (18.0) | 59 | 2.5 (2.0, 3.2) | 63 | 2.7 (2.1, 3.4) |
| IRSAD quintile (N = 12,927) | |||||
| First (most advantaged) | 1571 (12.1) | 18 | 1.1 (0.7, 1.8) | 24 | 1.5 (1.0, 2.3) |
| Second | 854 (6.6) | 16 | 1.9 (1.2, 3.0) | 21 | 2.5 (1.6, 3.7) |
| Third | 2462 (19.0) | 47 | 1.9 (1.2, 3.0) | 49 | 2.0 (1.5, 2.6) |
| Fourth | 4956 (38.3) | 138 | 2.8 (2.4, 3.3) | 142 | 2.9 (2.4, 3.4) |
| Fifth (most disadvantaged) | 3084 (23.8) | 119 | 3.9 (3.2, 4.6) | 132 | 4.3 (3.6, 5.1) |
| Maternal and newborn factors | |||||
| Maternal age | |||||
| 20–34 years | 10,243 (79.2) | 255 | 2.5 (2.2, 2.8) | 275 | 2.7 (2.4, 3.0) |
| <20 years | 570 (4.4) | 31 | 5.4 (3.9, 7.6) | 32 | 5.6 (4.0, 7.8) |
| 35+ years | 2128 (16.4) | 52 | 2.4 (1.9, 3.2) | 61 | 2.9 (2.2, 3.7) |
| Maternal Aboriginal status (N = 12,907) | |||||
| Non-Aboriginal | 12,077 (93.3) | 286 | 2.4 (2.1, 2.7) | 327 | 2.7 (2.4, 3.0) |
| Aboriginal | 830 (6.4) | 52 | 6.3 (4.8, 8.1) | 41 | 4.9 (3.7, 6.6) |
| Maternal hypertension | |||||
| No | 12,451 (96.2) | 325 | 2.6 (2.3, 2.9) | 362 | 2.9 (2.6, 3.2) |
| Yes | 490 (3.8) | 13 | 2.7 (1.5, 4.5) | 6 | 1.2 (0.6, 2.7) |
| Maternal diabetes | |||||
| No | 12,128 (93.7) | 322 | 2.7 (2.4, 3.0) | 339 | 2.8 (2.5, 3.1) |
| Yes | 813 (6.3) | 16 | 2.0 (1.2, 3.2) | 29 | 3.6 (2.5, 5.1) |
| Tobacco smoking (N = 12,909) | |||||
| No | 10,644 (82.3) | 170 | 1.6 (1.4, 1.9) | 248 | 2.3 (2.1, 2.6) |
| Yes | 2265 (17.5) | 163 | 7.2 (6.2, 8.3) | 115 | 5.1 (4.2, 6.1) |
| Newborn Aboriginal status (N = 12,692) | |||||
| Non-Aboriginal | 11,572 (89.4) | 264 | 2.3 (2.0, 2.6) | 311 | 2.7 (2.4, 3.0) |
| Aboriginal | 1120 (8.7) | 69 | 6.2 (4.9, 7.7) | 51 | 4.6 (3.5, 5.9) |
| Apgar score (N = 12,847) | |||||
| ≥7 Apgar | 12,663 (97.9) | 303 | 2.4 (2.1, 2.7) | 332 | 2.6 (2.4, 2.9) |
| <7 Apgar | 184 (1.4) | 26 | 14.1 (9.8, 19.9) | 28 | 15.2 (10.7, 21.2) |
| Newborn sex (N = 12,940) | |||||
| Male | 6661 (51.5) | 144 | 2.2 (1.8, 2.5) | 193 | 2.9 (2.5, 3.3) |
| Female | 6279 (48.5) | 194 | 3.1 (2.7, 3.5) | 175 | 2.8 (2.4, 3.2) |
| Mode of birth | |||||
| Vaginal | 9488 (73.3) | 241 | 2.5 (2.2, 2.9) | 258 | 2.7 (2.4, 3.1) |
| Caesarean | 3453 (26.7) | 97 | 2.8 (2.3, 3.4) | 110 | 3.2 (2.6, 3.8) |
| Exposure variables | |||||
| Timing of first ANC visit | |||||
| First trimester | 6067 (46.9) | 145 | 2.4 (2.0, 2.8) | 165 | 2.7 (2.3, 3.2) |
| Second trimester | 5883 (45.5) | 160 | 2.7 (2.3, 3.2) | 174 | 3.0 (2.6, 3.4) |
| Third trimester | 991 (7.7) | 33 | 3.3 (2.4, 4.6) | 29 | 2.9 (2.0, 4.2) |
| Recommended number of ANC visits | |||||
| Yes | 10,902 (84.2) | 208 | 1.9 (1.7, 2.2) | 221 | 2.0 (1.8, 2.3) |
| No | 2039 (15.8) | 130 | 6.4 (5.4, 7.5) | 147 | 7.2 (6.2, 8.4) |
| Total | 12,941 (100) | 338 | 2.6 (2.4, 2.9) | 368 | 2.8 (2.6, 3.1) |
| Confounding Variables | uOR (95% CI) | p-Value | aOR (95% CI) | p-Value |
|---|---|---|---|---|
| Year of birth (2011–2020) | 0.97 (0.93, 1.00) | 0.083 | ||
| Hospital of birth | ||||
| Cooma Health Service | Reference | |||
| Goulburn Base Hospital | 1.39 (0.94, 2.05) | 0.100 | ||
| Moruya District Hospital | 1.30 (0.88, 1.93) | 0.190 | ||
| Queanbeyan Health Service | 0.69 (0.46, 1.05) | 0.080 | ||
| South East Regional Hospital | 1.03 (0.68, 1.57) | 0.880 | ||
| IRSAD quintile (N = 12,927) | ||||
| First (most advantaged) | Reference | Reference | ||
| Second | 1.65 (0.84, 3.25) | 0.150 | 1.60 (0.76, 3.38) | 0.216 |
| Third | 1.68 (0.97, 2.90) | 0.060 | 1.42 (0.77, 2.64) | 0.261 |
| Fourth | 2.47 (1.51, 4.05) | <0.001 | 1.73 (0.99, 3.01) | 0.053 |
| Fifth (most disadvantaged) | 3.46 (2.10, 5.71) | <0.001 | 1.88 (1.07, 3.31) | 0.029 |
| Maternal age | ||||
| 20–34 years | Reference | |||
| <20 years | 2.25 (1.54, 3.30) | <0.001 | ||
| 35+ years | 0.98 (0.73, 1.33) | 0.900 | ||
| Maternal Aboriginal status (N = 12,907) | ||||
| Non-Aboriginal | Reference | Reference | ||
| Aboriginal | 2.76 (2.03, 3.74) | <0.001 | 1.60 (1.08, 2.37) | 0.019 |
| Maternal hypertension | ||||
| No | Reference | |||
| Yes | 1.02 (0.58, 1.78) | 0.950 | ||
| Maternal diabetes | ||||
| No | Reference | |||
| Yes | 0.74 (0.44, 1.22) | 0.240 | ||
| Tobacco smoking (N = 12,909) | ||||
| No | Reference | Reference | ||
| Yes | 4.78 (3.83, 5.95) | <0.001 | 3.67 (2.82, 4.77) | <0.001 |
| Newborn Aboriginal status (N = 12,692) | ||||
| Non-Aboriginal | Reference | |||
| Aboriginal | 2.81 (2.14, 3.69) | <0.001 | ||
| Apgar score (N = 12,847) | ||||
| ≥7 Apgar | Reference | Reference | ||
| <7 Apgar | 6.71 (4.37, 10.32) | <0.001 | 3.25 (1.86, 5.69) | <0.001 |
| Newborn sex (N = 12,940) | ||||
| Male | Reference | Reference | ||
| Female | 1.44 (1.16, 1.80) | <0.001 | 1.75 (1.36, 2.25) | <0.001 |
| Mode of birth | ||||
| Vaginal | Reference | |||
| Caesarean | 1.11 (0.87, 1.41) | 0.400 | ||
| Preterm birth | ||||
| No | Reference | Reference | ||
| Yes | 39.68 (30.81, 51.10) | 28.7 (21.4, 38.47) | <0.001 | |
| Exposure variables | ||||
| Timing of first ANC visit | ||||
| First trimester | Reference | |||
| Second trimester | 1.14 (0.91, 1.43) | 0.250 | ||
| Third trimester | 1.41 (0.96, 2.07) | 0.080 | ||
| Number of recommended ANC visits | ||||
| No | Reference | Reference | ||
| Yes | 0.29 (0.23, 0.36) | <0.001 | 0.55 (0.42, 0.73) | <0.001 |
| Confounding Variables | uOR (95% CI) | p-Value | aOR (95% CI) | p-Value |
|---|---|---|---|---|
| Year of birth (2011–2020) | 0.95 (0.92, 0.99) | 0.01 | 0.95 (0.92, 0.99) | 0.021 |
| Hospital of birth | ||||
| Cooma Health Service | Reference | |||
| Goulburn Base Hospital | 1.76 (1.19, 2.6) | <0.001 | ||
| Moruya District Hospital | 1.44 (0.97, 2.15) | 0.070 | ||
| Queanbeyan Health Service | 0.81 (0.53, 1.23) | 0.320 | ||
| South East Regional Hospital | 1.17 (0.77, 1.79) | 0.460 | ||
| IRSAD quintile (N = 12,927) | ||||
| First (most advantaged) | Reference | Reference | ||
| Second | 1.63 (0.9, 2.94) | 0.110 | 1.19 (0.62, 2.28) | 0.601 |
| Third | 1.31 (0.8, 2.14) | 0.280 | 1.03 (0.61, 1.76) | 0.905 |
| Fourth | 1.9 (1.23, 2.94) | <0.001 | 1.39 (0.87, 2.21) | 0.163 |
| Fifth (most disadvantaged) | 2.88 (1.86, 4.47) | <0.001 | 1.83 (1.14, 2.93) | 0.012 |
| Maternal age | ||||
| 20–34 years | Reference | |||
| <20 years | 2.16 (1.48, 3.14) | <0.001 | ||
| 35+ years | 1.07 (0.81, 1.42) | 0.640 | ||
| Maternal Aboriginal status (N = 12,907) | ||||
| Non-Aboriginal | Reference | |||
| Aboriginal | 1.87 (1.34, 2.6) | <0.001 | ||
| Maternal hypertension | ||||
| No | Reference | |||
| Yes | 0.41 (0.18, 0.93) | 0.030 | ||
| Maternal diabetes | ||||
| No | Reference | Reference | ||
| Yes | 1.29 (0.87, 1.89) | 0.200 | 1.68 (1.08, 2.59) | 0.02 |
| Tobacco smoking (N = 12,909) | ||||
| No | Reference | |||
| Yes | 2.24 (1.79, 2.81) | <0.001 | ||
| Newborn Aboriginal status (N = 12,692) | ||||
| Non-Aboriginal | Reference | |||
| Aboriginal | 1.73 (1.28, 2.34) | <0.001 | ||
| Apgar score (N = 12,847) | ||||
| ≥7 Apgar | Reference | Reference | ||
| <7 Apgar | 6.67 (4.39, 10.11) | <0.001 | 3.38 (1.99, 5.74) | <0.001 |
| Newborn sex (N = 12,940) | ||||
| Male | Reference | |||
| Female | 0.96 (0.78, 1.18) | 0.710 | ||
| Mode of birth | ||||
| Vaginal | Reference | |||
| Caesarean | 1.18 (0.94, 1.48) | 0.160 | ||
| Low birth weight | ||||
| No | Reference | Reference | ||
| Yes | 39.68 (30.81, 51.1) | <0.001 | 28.04 (21.28, 36.94) | <0.001 |
| Exposure variables | ||||
| Timing of first ANC visit | ||||
| First trimester | Reference | |||
| Second trimester | 1.09 (0.88, 1.35) | 0.430 | ||
| Third trimester | 1.08 (0.72, 1.61) | 0.710 | ||
| Number of recommended ANC visits | ||||
| No | Reference | Reference | ||
| Yes | 0.27 (0.21, 0.33) | <0.001 | 0.38 (0.30, 0.49) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ghimire, P.R.; Buck, G.; Jackson, J.; Woolley, E.; Bowman, R.; Fox, L.; Gallagher, S.; Sorrell, M.; Dubois, L. Impact of Antenatal Care on Perinatal Outcomes in New South Wales, Australia: A Decade-Long Regional Perspective. Int. J. Environ. Res. Public Health 2023, 20, 977. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20020977
Ghimire PR, Buck G, Jackson J, Woolley E, Bowman R, Fox L, Gallagher S, Sorrell M, Dubois L. Impact of Antenatal Care on Perinatal Outcomes in New South Wales, Australia: A Decade-Long Regional Perspective. International Journal of Environmental Research and Public Health. 2023; 20(2):977. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20020977
Chicago/Turabian StyleGhimire, Pramesh Raj, Gretchen Buck, Jackie Jackson, Emma Woolley, Rebekah Bowman, Louise Fox, Shirlena Gallagher, Malindey Sorrell, and Lorraine Dubois. 2023. "Impact of Antenatal Care on Perinatal Outcomes in New South Wales, Australia: A Decade-Long Regional Perspective" International Journal of Environmental Research and Public Health 20, no. 2: 977. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20020977