

Association between Anemia Severity and Ischemic Stroke Incidence: A Retrospective Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
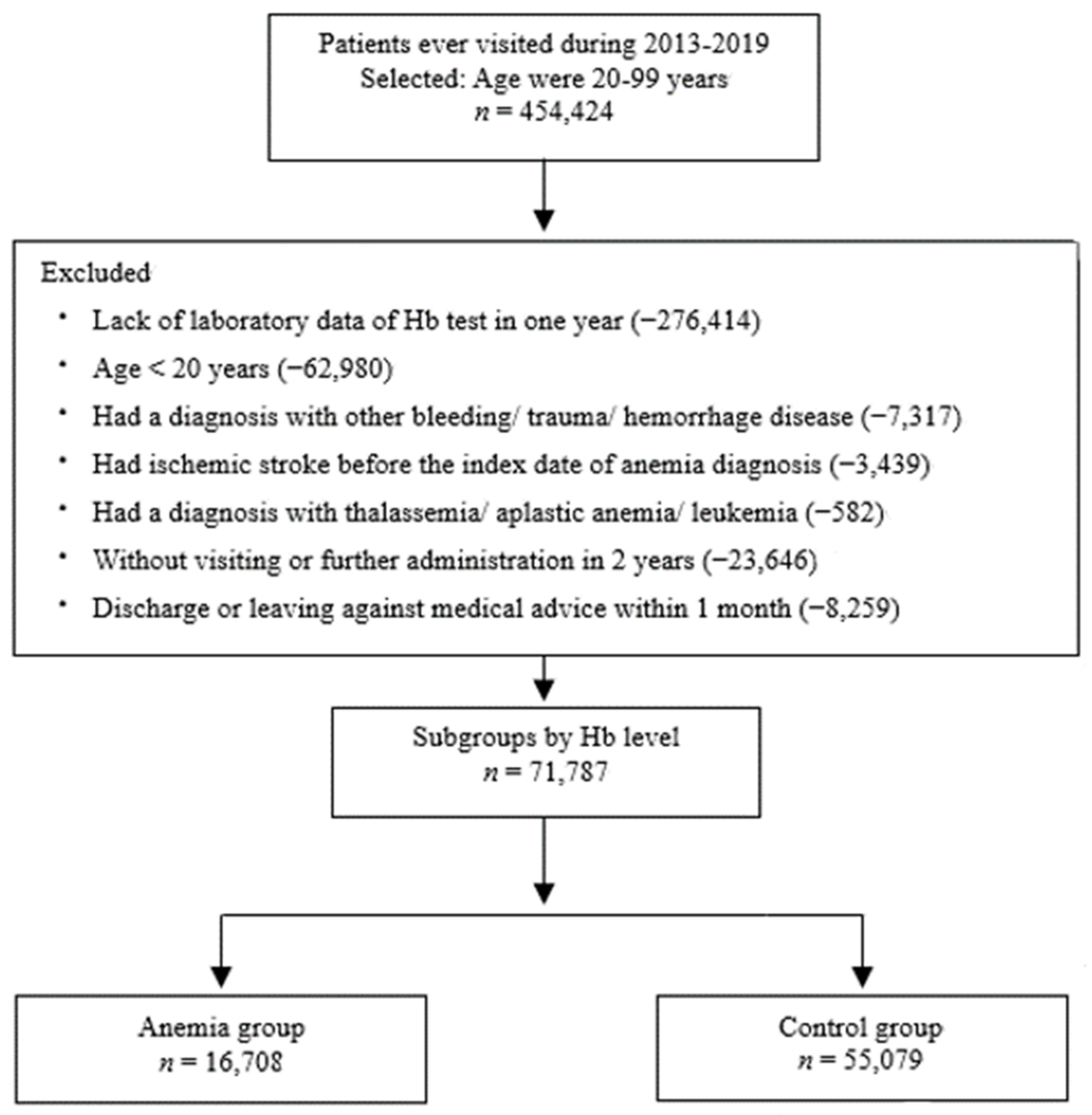
2.1. Study Cohort
2.2. Definition of Anemia and ICD Codes
2.3. Outcome and Associated Factors
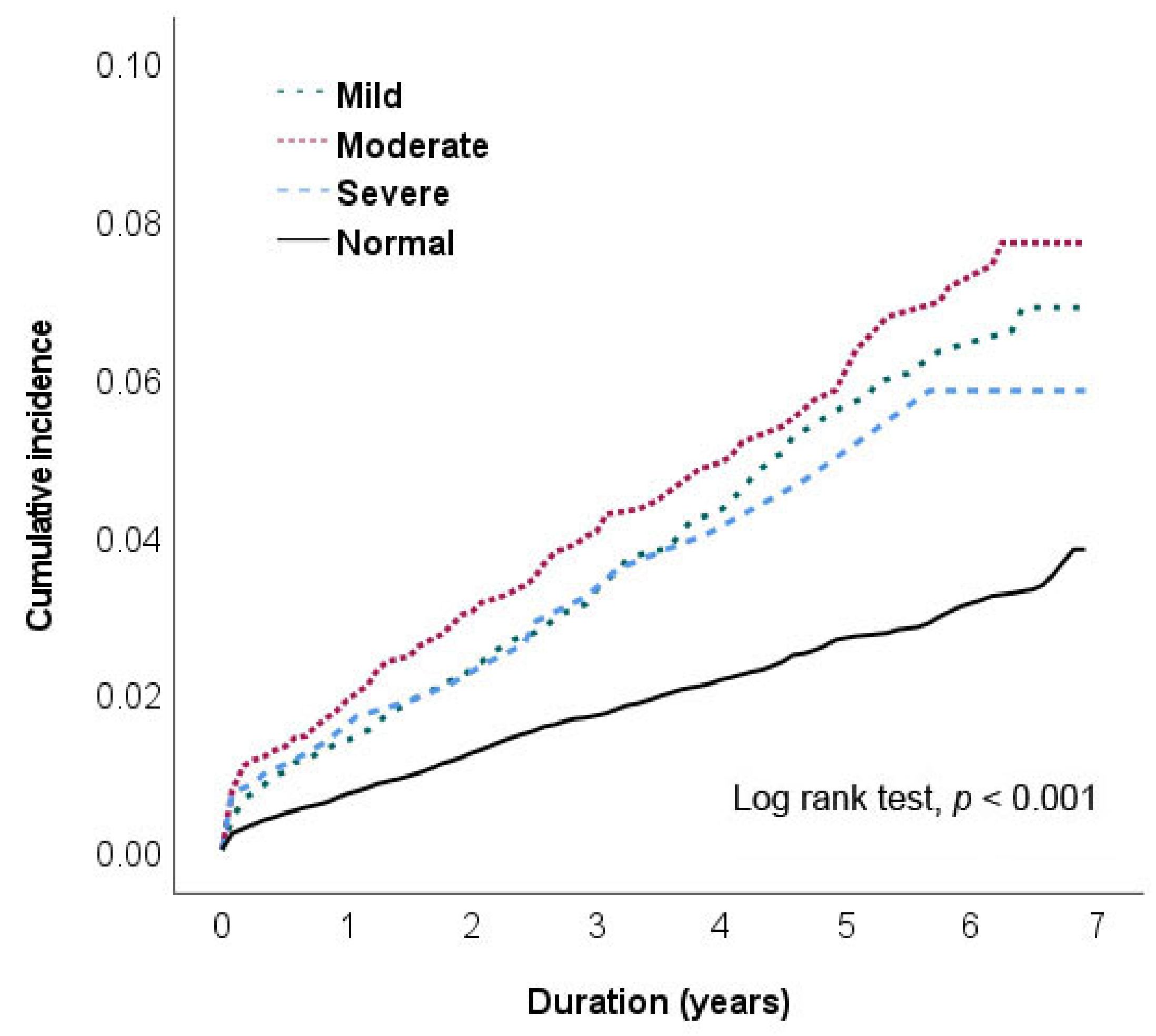
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.J.; Riley-Bennett, F.; Russell, L.; Lee, C.; Sturt, R.; Walker, M.; Sackley, C. Nominal group technique to establish the core components of home-based rehabilitation for survivors of stroke with severe disability. BMJ Open 2021, 11, e052593. [Google Scholar] [CrossRef]
- Gottesman, R.F.; Seshadri, S. Risk Factors, Lifestyle Behaviors, and Vascular Brain Health. Stroke 2022, 53, 394–403. [Google Scholar] [CrossRef]
- Guzik, A.; Bushnell, C. Stroke epidemiology and risk factor management. Continuum Lifelong Learn. Neurol. 2017, 23, 15–39. [Google Scholar] [CrossRef] [PubMed]
- Bang, O.Y.; Ovbiagele, B.; Kim, J.S. Nontraditional risk factors for ischemic stroke: An update. Stroke 2015, 46, 3571–3578. [Google Scholar] [CrossRef] [PubMed]
- Kaiafa, G.; Savopoulos, C.; Kanellos, I.; Mylonas, K.S.; Tsikalakis, G.; Tegos, T.; Kakaletsis, N.; Hatzitolios, A.I. Anemia and stroke: Where do we stand? Acta Neurol. Scand. 2017, 135, 596–602. [Google Scholar] [CrossRef]
- Kassebaum, N.J.; Jasrasaria, R.; Naghavi, M.; Wulf, S.K.; Johns, N.; Lozano, R.; Regan, M.; Weatherall, D.; Chou, D.P.; Eisele, T.P.; et al. A systematic analysis of global anemia burden from 1990 to 2010. Blood 2014, 123, 615–624. [Google Scholar] [CrossRef]
- Safiri, S.; Kolahi, A.A.; Noori, M.; Nejadghaderi, S.A.; Karamzad, N.; Bragazzi, N.L.; Sullman, M.J.M.; Abdollahi, M.; Collins, G.S.; Kaufman, J.S.; et al. Burden of anemia and its underlying causes in 204 countries and territories, 1990-2019: Results from the Global Burden of Disease Study 2019. J. Hematol. Oncol. 2021, 14, 185. [Google Scholar] [CrossRef]
- Heo, J.; Youk, T.M.; Seo, K.D. Anemia is a risk factor for the development of ischemic stroke and post-stroke mortality. J. Clin. Med. 2021, 10, 2556. [Google Scholar] [CrossRef]
- Kaiafa, G.; Kanellos, I.; Savopoulos, C.; Kakaletsis, N.; Giannakoulas, G.; Hatzitolios, A.I. Is anemia a new cardiovascular risk factor? Int. J. Cardiol. 2015, 186, 117–124. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline from the American heart association/American stroke association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef] [PubMed]
- WHO. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity. 2011. Available online: https://apps.who.int/iris/bitstream/handle/10665/85839/WHO_NMH_NHD_MNM_11.1_eng.pdf?ua=1 (accessed on 16 February 2023).
- Hsieh, M.T.; Hsieh, C.Y.; Tsai, T.T.; Wang, Y.C.; Sung, S.F. Performance of ICD-10-CM diagnosis codes for identifying acute ischemic stroke in a national health insurance claims database. Clin. Epidemiol. 2020, 12, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Yao, C.Y.; Chien, J.H.; Chuang, H.Y.; Ho, T.F. Associated factors with acute transfusion reaction from hospital online reporting events: A retrospective cohort study. J. Patient Saf. 2020, 16, e303–e309. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.L.; Hung, S.H.; Ling, W.; Lin, H.C.; Li, H.C.; Chung, S.D. Association between ischemic stroke and iron-deficiency anemia: A population-based study. PLoS ONE 2013, 8, e82952. [Google Scholar] [CrossRef] [Green Version]
- Sui, Y.; Hong, C.T.; Chien, L.N.; Liu, H.Y.; Chiou, H.Y.; Hsieh, Y.C. Association between anemia and stroke in females: Anationwide, population-based cohort study in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 7440. [Google Scholar] [CrossRef]
- Lin, Y.-Y.; Huang, C.-S. Aging in Taiwan: Building a society for active aging and aging in place. Gerontologist 2015, 56, 176–183. [Google Scholar] [CrossRef] [Green Version]
- Halawi, R.; Moukhadder, H.; Taher, A. Anemia in the elderly: A consequence of aging? Expert Rev. Hematol. 2017, 10, 327–335. [Google Scholar] [CrossRef]
- Goodnough, L.T.; Schrier, S.L. Evaluation and management of anemia in the elderly. Am. J. Hematol. 2014, 89, 88–96. [Google Scholar] [CrossRef] [Green Version]
- Chueh, H.W.; Jung, H.L.; Shim, Y.J.; Choi, H.S.; Han, J.Y. High anemia prevalence in Korean older adults, an advent healthcare problem: 2007–2016 KNHANES. BMC Geriatr. 2020, 20, 509. [Google Scholar] [CrossRef]
- Kılıçgedik, A.; Dündar, C.; Tigen, M.K. Anemia in heart failure. Anadolu Kardiyol. Derg. 2012, 12, 65–70. [Google Scholar]
- Hong, C.H.; Falvey, C.; Harris, T.B.; Simonsick, E.M.; Satterfield, S.; Ferrucci, L.; Metti, A.L.; Patel, K.V.; Yaffe, K. Anemia and risk of dementia in older adults: Findings from the Health ABC study. Neurology 2013, 81, 528–533. [Google Scholar] [CrossRef] [Green Version]
- Ruan, Y.; Guo, Y.; Kowal, P.; Lu, Y.; Liu, C.; Sun, S.; Huang, Z.; Zheng, Y.; Wang, W.; Li, G.; et al. Association between anemia and frailty in 13,175 community-dwelling adults aged 50 years and older in China. BMC Geriatr. 2019, 19, 327. [Google Scholar] [CrossRef] [Green Version]
- Culleton, B.F.; Manns, B.J.; Zhang, J.; Tonelli, M.; Klarenbach, S.; Hemmelgarn, B.R. Impact of anemia on hospitalization and mortality in older adults. Blood 2006, 107, 3841–3846. [Google Scholar] [CrossRef] [Green Version]
- Michalak, S.S.; Rupa-Matysek, J.; Gil, L. Comorbidities, repeated hospitalizations, and age ≥ 80 years as indicators of anemia development in the older population. Ann. Hematol. 2018, 97, 1337–1347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, X.; Hu, H.; Farooqi, I.; Simpkins, J.W. Blood substitution therapy rescues the brain of mice from ischemic damage. Nat. Commun. 2020, 11, 4078. [Google Scholar] [CrossRef] [PubMed]
- Petry, N.; Olofin, I.; Hurrell, R.F.; Boy, E.; Wirth, J.P.; Moursi, M.; Donahue Angel, M.; Rohner, F. The proportion of anemia associated with iron deficiency in low, medium, and high human development index countries: A systematic analysis of national surveys. Nutrients 2016, 8, 693. [Google Scholar] [CrossRef] [PubMed]
- Makipour, S.; Kanapuru, B.; Ershler, W.B. Unexplained anemia in the elderly. Semin. Hematol. 2008, 45, 250–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, D.L. Anemia in the elderly. Am. Fam. Physician 2000, 62, 1565–1572. [Google Scholar]
- Stauder, R.; Valent, P.; Theurl, I. Anemia at older age: Etiologies, clinical implications, and management. Blood 2018, 131, 505–514. [Google Scholar] [CrossRef] [Green Version]
- Ghoshal, S. Freedman BI. Mechanisms of Stroke in Patients with Chronic Kidney Disease. Am. J. Nephrol. 2019, 50, 229–239. [Google Scholar] [CrossRef]
- Poznyak, A.V.; Sadykhov, N.K.; Kartuesov, A.G.; Borisov, E.E.; Sukhorukov, V.N.; Orekhov, A.N. Atherosclerosis specific features in chronic kidney disease (CKD). Biomedicines 2022, 10, 2094. [Google Scholar] [CrossRef] [PubMed]
- Morita, S.; Malik, A.H.; Kuno, T.; Ando, T.; Kaul, R.; Yandrapalli, S.; Briasoulis, A. Analysis of outcome of 6-month readmissions after percutaneous left atrial appendage occlusion. Heart 2022, 108, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Sim, Y.E.; Wee, H.E.; Ang, A.L.; Ranjakunalan, N.; Ong, B.C.; Abdullah, H.R. Prevalence of preoperative anemia, abnormal mean corpuscular volume and red cell distribution width among surgical patients in Singapore, and their influence on one year mortality. PLoS ONE 2017, 12, e0182543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, H.J.; Koo, J.W.; Roh, S.K.; Kim, Y.K.; Suh, J.S.; Moon, J.H.; Sohn, S.K.; Baek, D.W. COVID-19 transmission and blood transfusion: A case report. J. Infect. Public Health 2020, 13, 1678–1679. [Google Scholar] [CrossRef] [PubMed]
- Yin, Z.; Yu, B.; Liu, W.; Lan, K. Blood transfusion and mortality in myocardial infarction: An updated meta-analysis. Oncotarget 2017, 8, 102254–102262. [Google Scholar] [CrossRef] [Green Version]
- Parnianfard, N.; Sadat Ebrahimi, S.R.; Hoseini, P. Hyperlipidemia as a stroke risk factor: Study of patients from northwest of Iran from 2008 to 2013. Atherosclerosis 2020, 315, e196. [Google Scholar] [CrossRef]
- Stewart, S.; Hart, C.L.; Hole, D.J.; McMurray, J.J. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am. J. Med. 2002, 113, 359–364. [Google Scholar] [CrossRef]
- Raghunath, S.; Pfeifer, J.M.; Ulloa-Cerna, A.E.; Nemani, A.; Carbonati, T.; Jing, L.; van Maanen, D.P.; Hartzel, D.N.; Ruhl, J.A.; Lagerman, B.F.; et al. Deep neural networks can predict new-onset atrial fibrillation from the 12-lead ECG and help identify those at risk of atrial fibrillation-related stroke. Circulation 2021, 143, 1287–1298. [Google Scholar] [CrossRef]
- Tu, S.J.; Hanna-Rivero, N.; Elliott, A.D.; Clarke, N.; Huang, S.; Pitman, B.M.; Gallagher, C.; Linz, D.; Mahajan, R.; Lau, D.H.; et al. Associations of anemia with stroke, bleeding, and mortality in atrial fibrillation: A systematic review and meta-analysis. J. Cardiovasc. Electrophysiol. 2021, 32, 686–694. [Google Scholar] [CrossRef]
- Krishnasivam, D.; Trentino, K.M.; Burrows, S.; Farmer, S.L.; Picardo, S.; Leahy, M.F.; Halder, A.; Chamberlain, J.; Swain, S.; Muthucumarana, K.; et al. Anemia in hospitalized patients: An overlooked risk in medical care. Transfusion 2018, 58, 2522–2528. [Google Scholar] [CrossRef]
- Lucca, U.; Tettamanti, M.; Mosconi, P.; Apolone, G.; Gandini, F.; Nobili, A.; Tallone, M.V.; Detoma, P.; Giacomin, A.; Clerico, M.; et al. Association of mild anemia with cognitive, functional, mood and quality of life outcomes in the elderly: The “Health and Anemia” study. PLoS ONE 2008, 3, e1920. [Google Scholar] [CrossRef] [PubMed]
- Yotsueda, R.; Tanaka, S.; Taniguchi, M.; Fujisaki, K.; Torisu, K.; Masutani, K.; Hirakata, H.; Kitazono, T.; Tsuruya, K. Hemoglobin concentration and the risk of hemorrhagic and ischemic stroke in patients undergoing hemodialysis: The Q-cohort study. Nephrol. Dial. Transplant. 2018, 33, 856–864. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic n = 71,787 | Normal n = 55,079 (76.73%) | All Anemia n = 16,708 (23.27%) | p | Mild Anemia | Moderate Anemia | Severe Anemia | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n = 9065 (53.99%) | n = 6532 (39.27%) | n = 1111 (6.75%) | |||||||||
| Hb (g/dL) | 14.2 ± 1.3 | 10.7 ± 1.6 | <0.001 | 11.8 ± 0.5 | 9.9 ± 0.8 | 6.7 ± 1.1 | |||||
| Gender | |||||||||||
| Male | 26,184 | 47.54% | 6185 | 37.02% | 3933 | 43.39% | 1880 | 28.78% | 372 | 33.48% | |
| Female | 28,895 | 52.46% | 10, 523 | 62.98% | 5132 | 56.61% | 4652 | 71.22% | 739 | 66.52% | |
| Age (years) | 50.6 ± 16.3 | 59.1 ± 18.5 | <0.001 | 58.9 ± 18.5 | 59.7 ± 18.6 | 57.9 ± 17.5 | |||||
| 20–30 | 7298 | 13.25% | 1123 | 6.72% | <0.001 | 704 | 8.1% | 705 | 7.78% | 369 | 5.65% |
| 31–40 | 9139 | 16.59% | 1961 | 11.74% | 1069 | 12.3% | 1077 | 11.88% | 756 | 11.57% | |
| 41–50 | 10,423 | 18.92% | 2883 | 17.26% | 1287 | 14.9% | 1316 | 14.52% | 1275 | 19.52% | |
| 51–60 | 12,475 | 22.65% | 2586 | 15.48% | 1451 | 16.8% | 1489 | 16.43% | 919 | 14.07% | |
| 61–70 | 9168 | 16.65% | 2754 | 16.48% | 1512 | 17.5% | 1610 | 17.76% | 999 | 15.29% | |
| 71–80 | 4732 | 8.59% | 2990 | 17.90% | 1536 | 17.7% | 1671 | 18.43% | 1147 | 17.56% | |
| 81 above | 1844 | 3.35% | 2411 | 14.43% | 1100 | 12.7% | 1197 | 13.20% | 1067 | 16.33% | |
| Comorbidities | |||||||||||
| Hypertension | 6497 | 11.80% | 3408 | 20.40% | <0.001 | 1797 | 19.82% | 1400 | 21.43% | 211 | 18.99% |
| Diabetes | 3713 | 6.74% | 2467 | 14.77% | <0.001 | 1254 | 13.83% | 1067 | 16.33% | 146 | 13.14% |
| Chronic kidney disease | 496 | 0.90% | 1015 | 6.07% | <0.001 | 300 | 3.31% | 580 | 8.88% | 135 | 12.15% |
| Chronic heart failure disease | 500 | 0.91% | 446 | 2.67% | <0.001 | 206 | 2.27% | 208 | 3.18% | 32 | 2.88% |
| Chronic obstructive pulmonary disease | 1159 | 2.10% | 495 | 2.96% | <0.001 | 293 | 3.23% | 179 | 2.74% | 23 | 2.07% |
| Hyperlipidemia | 2177 | 3.95% | 643 | 3.85% | 0.544 | 395 | 4.36% | 222 | 3.40% | 26 | 2.34% |
| Atrial fibrillation | 270 | 0.49% | 169 | 1.01% | <0.001 | 86 | 0.95% | 73 | 1.12% | 10 | 0.90% |
| Treatment | |||||||||||
| Blood transfusion | 1795 | 3.26% | 3273 | 19.59% | <0.001 | 1017 | 11.22% | 1577 | 24.14% | 679 | 61.12% |
| Iron therapy | 72 | 0.13% | 662 | 3.96% | <0.001 | 67 | 0.74% | 388 | 5.94% | 207 | 18.63% |
| Folic acid supplement | 344 | 0.62% | 469 | 2.81% | <0.001 | 135 | 1.49% | 226 | 3.46% | 108 | 9.72% |
| Vitamin B12 supplement | 68 | 0.12% | 94 | 0.56% | <0.001 | 37 | 0.41% | 38 | 0.58% | 19 | 1.71% |
| Severity of Anemia | WHO Criteria (Hb, g/dL) | Study Cohort n = 71,787 | Stroke Events n = 1191 | Death Events n = 1969 | Average Follow Up | ||||
|---|---|---|---|---|---|---|---|---|---|
| Male | Female | n | % | n | % | n | % | Years | |
| Normal | >13.0 | >12.0 | 55,079 | ― | 744 | 1.35 | 740 | 1.34 | 2.32 ± 2.04 |
| Anemia | 16,708 | 447 | 2.68 | 1229 | 7.63 | ||||
| Mild | 11.0–12.9 | 11.0–11.9 | 9065 | 54.25 | 229 | 2.53 | 496 | 5.47 | 2.09 ± 1.95 |
| Moderate | 8.0–10.9 | 8.0–10.9 | 6532 | 39.09 | 193 | 2.95 | 599 | 9.17 | 1.98 ± 1.95 |
| Severe | <8.0 | <8.0 | 1111 | 6.65 | 25 | 2.25 | 134 | 12.06 | 1.95 ± 1.94 |
| Predictors | HR (95% CI) | |||
|---|---|---|---|---|
| Univariate | p | Adjusted | p | |
| Severity of anemia | ||||
| Normal | ― | ― | ||
| Mild | 1.96 (1.69–2.27) | <0.001 | 0.98 (0.84–1.15) | 0.795 |
| Moderate | 2.31 (1.97–2.71) | <0.001 | 1.20 (1.02–1.43) | 0.032 |
| Severe | 1.73 (1.16–2.58) | 0.007 | 0.99 (0.66–1.48) | 0.943 |
| Gender (male) | 1.66 (1.48–1.87) | <0.001 | 1.64 (1.46–1.85) | <0.001 |
| Age (years) | 1.07 (1.07–1.08) | <0.001 | 1.07 (1.065–1.074) | <0.001 |
| Comorbidity | ||||
| Hypertension | 3.11 (2.76–3.50) | <0.001 | 1.26 (1.10–1.45) | 0.001 |
| Diabetes mellitus | 2.86 (2.50–3.28) | <0.001 | 1.48 (1.27–1.71) | <0.001 |
| Chronic kidney disease | 2.65 (2.10–3.35) | <0.001 | 1.02 (0.80–1.31) | 0.869 |
| Chronic heart failure disease | 3.18 (2.41–4.19) | <0.001 | 1.00 (0.74–1.35) | 0.988 |
| Chronic obstructive pulmonary disease | 1.88 (144–2.46) | <0.001 | 0.76 (0.58–1.00) | 0.053 |
| Hyperlipidemia | 1.89 (1.54–2.31) | <0.001 | 1.13 (0.91–1.39) | 0.280 |
| Atrial fibrillation | 5.50 (3.98–7.59) | <0.001 | 1.84 (1.31–2.60) | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-F.; Ho, T.-F.; Kuo, Y.-H.; Chien, J.-H. Association between Anemia Severity and Ischemic Stroke Incidence: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2023, 20, 3849. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20053849
Chen H-F, Ho T-F, Kuo Y-H, Chien J-H. Association between Anemia Severity and Ischemic Stroke Incidence: A Retrospective Cohort Study. International Journal of Environmental Research and Public Health. 2023; 20(5):3849. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20053849
Chicago/Turabian StyleChen, Hui-Fen, Tsing-Fen Ho, Yu-Hung Kuo, and Ju-Huei Chien. 2023. "Association between Anemia Severity and Ischemic Stroke Incidence: A Retrospective Cohort Study" International Journal of Environmental Research and Public Health 20, no. 5: 3849. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20053849