1. Introduction
Self-paced work in hot conditions results in diminished productivity [
1], which is partly attributable to behavioral thermoregulation, a self-preservation process where pace slows in response to the perception of heat stress [
2]. Decreased productivity during heat stress can also be impacted by hyperthermia, dehydration, fatigue, and cardiovascular strain [
3,
4,
5]. Understanding heat stress limitations on worker productivity is important because preserving productivity for economic reasons may be at odds with occupational health and safety regulations [
6].
The magnitude of cardiovascular strain workers experience under heat stress can be represented as cardiovascular drift, a well-established phenomenon that occurs during continuous, submaximal, steady-state exercise, and is characterized by a progressive increase in heart rate (HR) and decrease in stroke volume (SV) over time. The drift in HR and SV is often concomitant to a decrease in work capacity, indexed as maximal oxygen uptake (
O
2max) [
4]. Heat stress and hyperthermia amplify cardiovascular drift and accompanying decrements in
O
2max in as little as 45 min during exercise [
4,
7]. As cardiovascular drift progresses and
O
2max decreases during steady-state exercise, the relative intensity of exercise for a given absolute workload represents a greater percentage of
O
2max, and therefore results in greater physiological and perceptual strain.
The National Institute for Occupational Safety and Health (NIOSH) outlines acceptable work standards for hot conditions [
8]. They recommend an intensity of continuous work to be no more than 30% to 40%
O
2max without the presence of environmental heat stress [
8]. While performing at maximal capacity may not be required for many occupations, progressive reductions in
O
2max—and consequently increases in %
O
2max—that accompany cardiovascular drift could result in submaximal work intensities that exceed this recommended range, which may also negatively impact worker productivity and safety.
One heat stress mitigation strategy recommended by NIOSH is the incorporation of work-to-rest ratios. However, their efficacy with regards to blunting cardiovascular drift and concomitant reductions in
O
2max has not been investigated. Most prior studies that examined cardiovascular drift and subsequent effects on
O
2max utilized continuous work protocols [
4,
7,
9,
10], and those that incorporated rest did not measure
O
2max [
11] or utilized a prolonged 90 min rest period prior to the maximal exercise test [
12].
The minimum work:rest ratio recommended by NIOSH is 45:15 min [
8] and there is evidence that 15 min of rest is not adequate for preventing increases in thermal and cardiovascular strain [
13]; if elevated body temperature persists, then some amount of ‘accumulated’ cardiovascular drift would be expected over consecutive work:rest cycles, which could result in reduced
O
2max. Without an understanding of the extent to which work capacity is reduced, optimizing work:rest ratios designed to mitigate physiological strain during work under heat stress is an improbable task. The purpose of this study was to test the hypothesis that during moderate-intensity work utilizing the recommend 45:15 min work:rest ratio, cardiovascular drift will accumulate over time. Furthermore, it was hypothesized that the magnitude of accumulated cardiovascular drift would be proportional to decrements in
O
2max.
2. Materials and Methods
A repeated measures crossover research design was utilized. Participants completed three sessions on different days, each separated by at least 48 h and not more than 1 week. The initial visit was for measurement of O2max and familiarization. The remaining two experimental trials were counterbalanced, and the treatment orders were randomly assigned. For one experimental trial, participants performed simulated work at a moderate intensity for 120 min as two 45 min:15 min work:rest cycles. On a different day, participants performed simulated work for 15 min, immediately followed by measurement of O2max. The purpose of the separate 15 and 120 min trials was so that O2max could be assessed before and after cardiovascular drift occurred since O2max could not be assessed twice within the same 120 min trial. Other than duration, all aspects of the 15 and 120 min trials were identical.
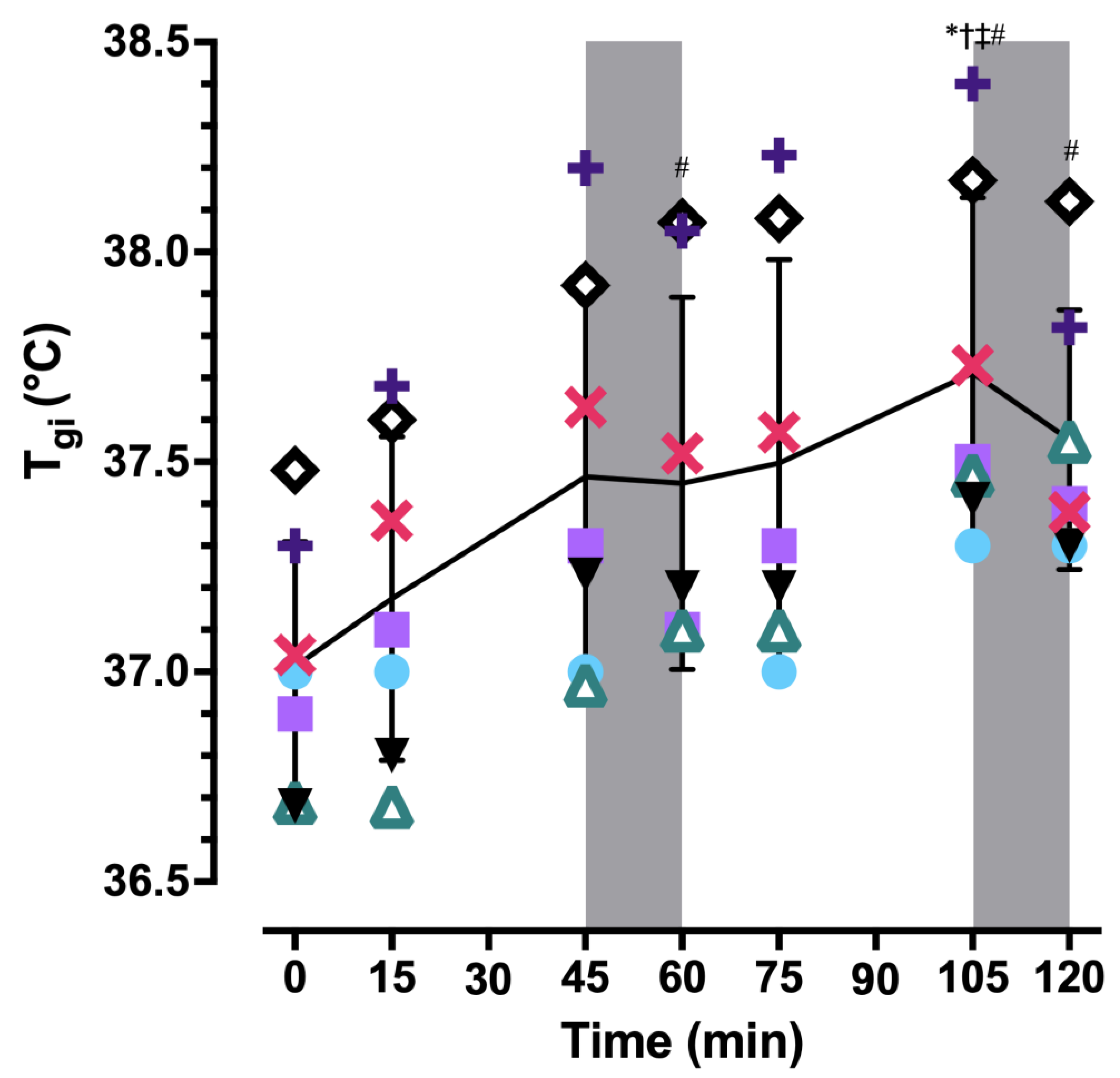
All sessions occurred in a climate-controlled environmental chamber at approximately the same time of day for each participant to control for circadian variation in core temperature, measured as gastrointestinal temperature (T
gi). Each female participant completed all experimental visits within a single phase of the menstrual cycle to control for fluctuations in baseline core body temperature; the menstrual cycle phase was not expected to influence study outcomes [
14]. Resting T
gi was used to confirm self-reported menstrual cycle phase. Environmental conditions were established using indoor wet-bulb globe temperature (WBGT
in) [
15], and confirmed by a Kestrel 4400 Heat Stress Meter (Kestrel Meters, Boothwyn, PA). The initial visit occurred in temperate conditions [22 °C, 40% relative humidity (RH), WBGT
in = 17 °C], whereas remaining visits occurred under heat stress (34 °C, 55% RH, WBGT
in = 29 °C). The hot environmental conditions were chosen using data from the National Weather Service for the Southeastern United States intended to mimic the WBGT workers in this region experience during summer [
16]. Air flow generated by the environmental chamber accounted for the NIOSH assumption of ‘perceptible air movement’ [
8]. The 45:15 min work:rest ratio was determined from the NIOSH Recommended Alert Limits and the adjusted ambient temperature for the test environment [
8]. The assigned workload aimed to elicit 201–300 kcal·h
−1 (metabolic rate [
Ṁ] = 234–349 W), which is defined as moderate intensity by the American Conference of Governmental Industrial Hygienists (ACGIH) and NIOSH [
8,
17]. Workload was evaluated as a time-weighted average, and to achieve moderate intensity work, participants performed arm curls, treadmill walking, and rest; arm curls were included in the protocol to vary the metabolic demand during simulated work [
18]. Arm curls were completed while standing, using a total weight of 4.5 kg (2.25 kg in each hand) at a rate of 20 curls per min in time with a metronome. Treadmill walking was prescribed to achieve
O
2 = 1.0–1.1 L·min
−1 at 4.0 km·h
−1, and the grade was adjusted accordingly.
An a priori power analysis revealed eight participants were needed to observe a meaningful effect of cardiovascular drift on
O
2max, based on means, SDs, and an effect size from a prior study [
4] using G*Power 3.1.9.4 [
19]. To account for the individual characteristic assumptions of the NIOSH heat stress guidelines, participant inclusion criteria were healthy men and women who were “physically fit, well rested, fully hydrated, [and] under age 40” [
8]. NIOSH does not define ‘physically fit’; this criterion was considered met if participants self-reported meeting the public health recommendation of ≥150 min of moderate-intensity physical activity per week or the equivalent [
20]. Additional exclusion criteria included a history of metabolic, renal, or cardiovascular disease, gastrointestinal issues that contraindicate the use of an ingestible thermistor, or contraindications to exercise in the heat. Participants were instructed to arrive for all trials hydrated, rested, and having refrained from eating 2 h prior to the trial, as well as having avoided the use of alcohol, tobacco, and caffeine 24 h prior to testing.
Initial Visit. Written informed consent was obtained prior to participation. Hydration status was assessed via urine specific gravity (USG), with USG ≤ 1.020 considered adequately hydrated [
21]. Percent body fat was estimated using the sum of skinfolds at three sites [
22]. Height was measured using a stadiometer (model no. 213 1821009, Seca, Chino, CA, USA) and body mass was measured using a digital scale (BWB-800, Tanita Corporation, Tokyo, Japan) while the participant was wearing shorts, socks, sports bra (females), and tank top. Next, participants donned trousers (50% polyester, 50% cotton) and a long-sleeved buttoned shirt (65% polyester, 35% cotton), and were instrumented with a HR monitor around their chest (H10, Polar USA, Bethpage, NY, USA). Finally, participants were familiarized with the questions and scales for rating of perceived exertion (RPE) and rating of thermal sensation (RTS) [
23,
24].
A graded exercise test (GXT) was administered on a treadmill to measure
O
2max (TrueOne 2400, Parvo Medics, Salt Lake City, UT, USA). Participants ran at a constant self-selected speed and an initial grade of 2.5%. The grade increased every 2 min by 2.5% until volitional exhaustion. RPE and HR were recorded 15 s before the end of each stage and at maximal exertion. Three minutes after the end of the test, a 2 mL blood sample was drawn from a superficial forearm vein or obtained via fingerstick to assess blood lactate (YSI 2300 STAT PLUS, YSI Inc., Yellow Springs, OH, USA; Lactate Plus Meter, Nova Biomedical, Waltham, MA, USA). After the GXT, participants rested for 20 min before completing a ~2 min
O
2max plateau verification protocol during which they ran to volitional exhaustion [
25]. The workload for the verification was determined by the last stage of the GXT: if it lasted <1 min, verification occurred at the same workload, but if it was ≥1 min, it occurred at the next stage (+2.5% grade). Lastly, the exercise intensity to be used during the experimental trials was verified and participants were familiarized with the CO
2-rebreathing technique used to non-invasively determine cardiac output during exercise [
26].
Experimental Trials. An ingestible thermometer pill (eCelsius Performance, BodyCap Medical, Hérouville-Saint-Clair, France), for the measurement of T
gi, was provided for ingestion 5 h prior to arrival—6 h prior to the start of exercise—to ensure passage into the gastrointestinal tract and to avoid artifact by water consumption [
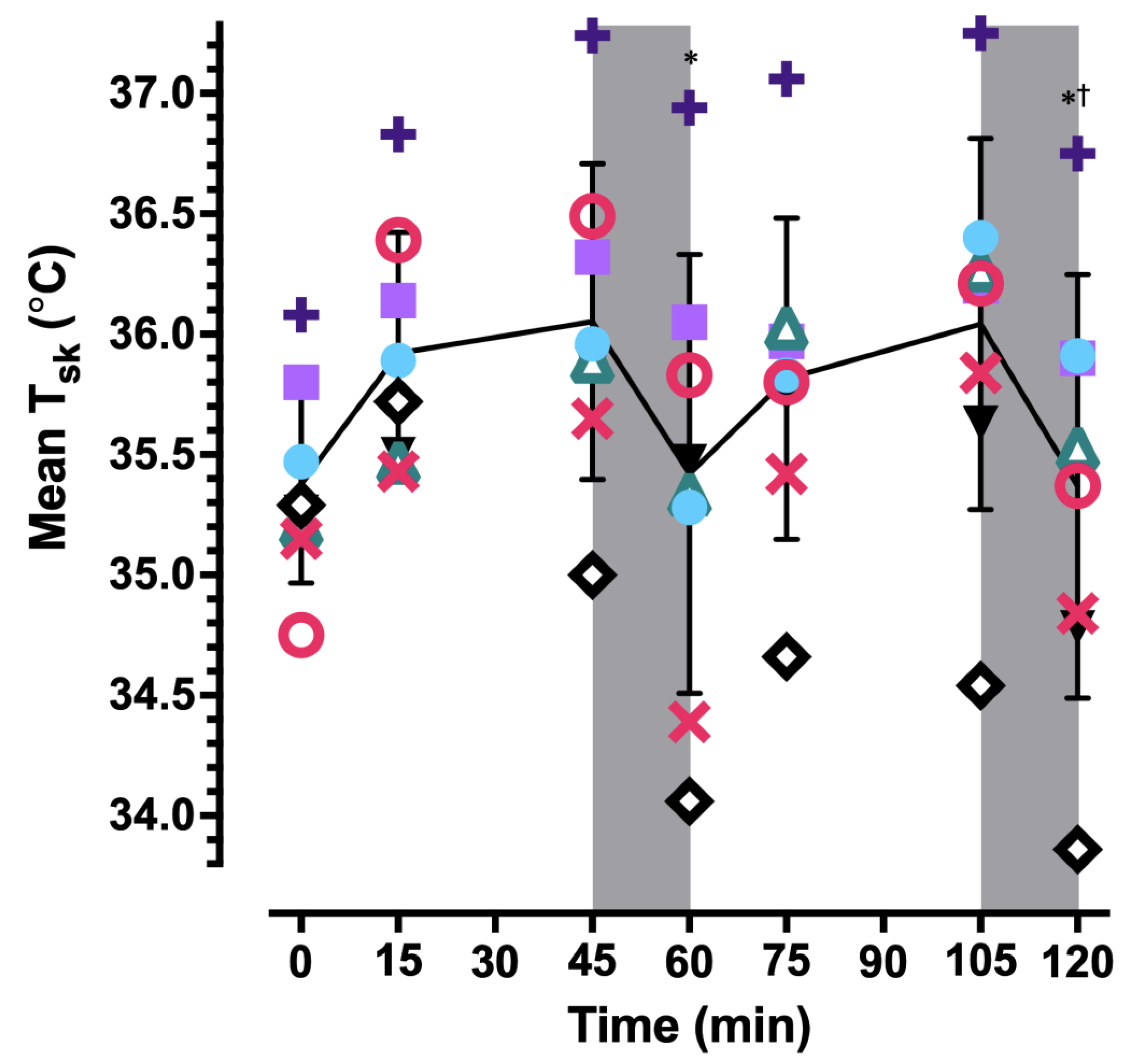
27]. USG and nude body mass were assessed before exercise began, and participants again donned the same trousers and a long-sleeved shirt. Skin temperature was measured at four sites using wireless data loggers (iButton model no. DS1921H, Embedded Data Systems, Lawrenceburg, KY). Mean skin temperature (
sk) was calculated as
sk = 0.3(
T1 +
T2) + 0.2(
T3 +
T4), where
T1,
T2,
T3, and
T4 correspond to skin temperature of the chest, lateral deltoid, quadriceps, and gastrocnemius, respectively [
28]. T
gi and
sk were used to calculate weighted mean body temperature (
b) as
b = 0.8(T
gi) + 0.2(
sk) [
29].
Next, two 2 mL blood samples were obtained from a superficial forearm vein for the baseline assessment of plasma osmolality, blood lactate concentration, hematocrit, and hemoglobin concentration. Whole blood was centrifuged at 3500×
g for 15 min and plasma osmolality was measured using freezing point depression (Fiske Micro-Osmometer, Model 210, Advanced Instruments, Norwood, MA, USA). Hematocrit and hemoglobin concentration were used to calculate changes in plasma volume [
30]. Participants then entered an environmental chamber maintained at a WBGT
in of 29 °C and sat quietly in a chair for 20 min to allow for equilibration to the hot environment and for preparation.
Figure 1 illustrates procedures for the 120 min protocol (120MIN). Around minute 15 and just before minute 45 of each exercise bout,
O
2, RPE, RTS, and cardiac output were measured; SV was calculated from HR and cardiac output measures. T
gi, HR, and skin temperature were recorded continuously. Participants remained in the environmental chamber, seated, for each rest break. At minute 120, participants immediately began a GXT with progressively increasing workloads in stages using the same speed and increases in grade (+2.5%) as the initial visit, running until volitional exhaustion to determine
O
2max. Three to 5 min after the GXT, a final blood sample was obtained via venipuncture to assess changes in blood lactate concentration, plasma osmolality, and plasma volume from baseline. Participants were allowed to drink cool water (~20 °C) ad libitum throughout, provided it did not impede the collection of data or completion of the protocol. Water temperature was determined as the mean temperature of 0, 60, and 120 min. Cardiovascular drift was assessed as changes in HR and SV between 15 min and 45, 75, and 105 min.
On a different day, participants completed a 15 min trial (15MIN) identical to the first 15 min of 120MIN; O2max was measured during a GXT that began at minute 15. HR, Tgi, and O2 were recorded during exercise. Like 120MIN, a blood sample was obtained ~3 min after the end of the test to assess blood lactate.
After exercise, participants were asked to towel off before measurement of nude body mass. Change in body mass was used in the calculation of whole body sweat loss, adjusted for fluid consumed, urine output, blood drawn, as well as estimated respiratory water loss and respiratory mass loss [
31]. Total water consumption was the difference in pre- and post-mass of the participant’s water bottle.
Metabolic rate (
Ṁ) during submaximal exercise was calculated from measures of
O
2 and RER [
32]. Net metabolic heat production (
Ṁ-
) was calculated as the difference between
Ṁ and external work rate (
).
Ṁ and
Ṁ-
were calculated separately for arm curls, walking, and rest, and are reported as a time-weighted average per NIOSH recommendations [
8].
Statistical analyses were performed using SPSS for Windows v.25 (IBM Corporation, Somers, NY, USA). Paired samples t-tests were used to test the significance of mean differences in O2max between 15MIN and 120MIN, as well as hematological variables pre- and post-exercise. For continuous variables such as cardiovascular, thermal, and metabolic measures, a one-way repeated measures analysis of variance (ANOVA) was conducted to compare values across time. If sphericity was violated, the Greenhouse-Geisser correction was applied. In the event of a significant omnibus test, pairwise comparisons with a Bonferroni α correction were performed. For ordinal variables (RPE; RTS), a nonparametric Friedman’s ANOVA was used. All statistical tests used an α level of 0.05.
4. Discussion
The purpose of this study was to determine the extent to which cardiovascular drift ‘accumulated’ over consecutive work:rest cycles and the subsequent impact on work capacity, indexed as
O
2max. As hypothesized, the primary finding was that cardiovascular drift accumulated over multiple work bouts; however,
O
2max was unaffected. The statistically nonsignificant 2% decrease in
O
2max after two work:rest cycles in 120MIN compared to 15MIN corresponded to comparable GXT durations and final workloads in the majority of participants. The observed change in
O
2max, as well as the magnitude of all individual responses, was within the expected day-to-day variability for repeated
O
2max testing [
34].
The magnitude of cardiovascular drift observed in the current study was comparable to other studies involving prolonged exercise in the heat. Gliner et al. [
11] observed responses over 4 h of 50:10 work:rest at 35%
O
2max in the heat (35 °C, 30% RH), and found similar magnitudes of drift in HR and SV—+23% and approximately −23%, respectively—but
O
2max was not assessed at the conclusion of the protocol. Other studies observed a comparable magnitude of cardiovascular drift of 9–19% and a concomitant decrement in
O
2max [
4,
7,
9,
10,
35], but despite the similar magnitude of cardiovascular responses,
O
2max was unaffected in the current study.
Contrary to other studies demonstrating that the elevated HR associated with cardiovascular drift reflects an increased relative metabolic intensity as a result of accompanying decreases in
O
2max [
4,
10,
35], the increase in HR in the present study appeared to be dissociated from relative metabolic intensity since
O
2max was preserved at the end of two work:rest cycles. Despite this, RPE increased slightly over consecutive work bouts, which is consistent with the observed increase in HR that is associated with cardiovascular drift. However, the precise explanation for this result is elusive since we did not observe a change in relative metabolic intensity (i.e., %
O
2max). The ~0.5 °C increase in T
gi between 15 and 105 min may have contributed, as RPE has been shown to be amplified by elevated body temperature [
36,
37].
Although the relative magnitudes of drift (i.e., % change) in HR and SV in the present study were comparable to the studies cited above, the absolute values for HR and SV were lower in this study. The absolute and relative work intensities utilized in this study were lower, which resulted in a lower absolute metabolic demand and elicited HR of 110–130 beats·min
−1 during exercise, compared to 150–170 beats·min
−1 in others [
4,
7,
9,
10,
35]. This difference in working HR resulted in a greater cardiac reserve (i.e., the difference between exercise values and maximum values) in the present study. The rest period prior to measurement of
O
2max in this study also may have facilitated greater cardiac reserve considering the other cited studies did not include a rest period between submaximal exercise and measurement of
O
2max. It may be that there is a minimum threshold work intensity and accompanying cardiovascular drift involving higher absolute HR and SV, and therefore greater reductions in cardiac reserve—rather than a given magnitude of cardiovascular drift per se—that is most strongly associated with reductions in
O
2max during prolonged work in the heat.
Given that previous studies observed a decrease in
O
2max preceded by a similar magnitude of cardiovascular drift, why was
O
2max unaffected in the current study after 120 min? The data collected do not permit a definitive answer to this question, but preservation of SV during maximal exertion is the likely explanation. Compared to other studies [
4,
7,
9,
35], this study utilized a lower exercise intensity, longer duration, and inclusion of rest breaks. As a result,
Ṁ-
was 2–3 times greater in the other studies than the 231 W observed here. Higher
Ṁ-
caused greater increases in core temperature (even over shorter durations) that exacerbated cardiovascular strain—i.e., reduced SV—during submaximal exercise that likely persisted during maximal exercise. In contrast, despite a similar magnitude of cardiovascular drift in the current study, thermal strain was mild. This may have resulted in preservation of SV—and thereby maximal cardiac output—during maximal exercise. This notion is supported by findings from Saltin and Stenberg [
38] who observed a comparable magnitude of cardiovascular drift—increase in HR and decrease in SV of ~15% each—during prolonged, intermittent, submaximal exercise (70%
O
2max, 195 min), but only a small reduction (5%; 0.1 L·min
−1) in
O
2max after a 90 min rest period. Despite the magnitude of decrease in SV during submaximal exercise, it was restored during maximal exercise, essentially preserving
O
2max. The authors attributed the ability to achieve maximal SV, and thereby maximal cardiac output, to a reduced skin blood flow requirement during the rest prior to measurement of
O
2max [
35]. It may be that a rest period shorter than 90 min, such as the 15 min utilized in the current study, is sufficient in reducing skin blood flow requirements under conditions of relatively low exercise intensity and thermal strain. While we were unable to measure skin blood flow, the return of
sk to baseline values before the GXT to measure
O
2max is suggestive of reductions in skin blood flow during rest [
39]. Since maximal HR was achieved and because (a-
)O
2 difference would not be expected to be different under these conditions [
40], restoration of maximal SV by reductions in skin blood flow would have permitted achievement of maximal cardiac output and thereby
O
2max.
One limitation of this study is that we were not able to measure skin blood flow because of constraints regarding the instrumentation and the movement artifact associated with exercise, and so we can only speculate regarding the redistribution of blood flow to the skin. While skin temperature can be an adequate substitution for measurement of skin blood flow, participants wore a long-sleeved shirt and pants, creating a microenvironment that could have artificially elevated skin temperatures and overestimated the assumption of elevated skin blood flow; however, because skin temperature returned to baseline values during rest, we do not believe that to be the case.
Although NIOSH assumptions (age, physical fitness, health status, hydration, sleep, work intensity, environmental conditions) were accounted for in subject recruitment and study design, participants were likely not representative of the average worker, and so the extent to which these findings are applicable in the workplace is limited by the sample population. By design, participants did not have any co-morbidities, were <40 years old, and arrived at all laboratory visits prepared for peak performance: well rested, hydrated, and having refrained from recent alcohol or caffeine consumption. These ideal conditions are likely a less frequent reality, and as such generalization of these results to what workers experience warrants caution.
Even though assumptions of the ideal worker were largely met, several NIOSH recommendations were not fulfilled. Ad libitum water consumption did not meet the NIOSH-recommended rate of consumption of 0.95 L·h−1. NIOSH also recommends that work intensity does not exceed 30–40% O2max. O2 for two participants exceeded the upper end of this recommended range (>40% O2max), while three participants’ relative workloads remained below 30% O2max and three participants’ relative workloads were between 30–40% O2max, although mean O2 remained within the prescribed range for all participants throughout the entirety of the protocol. In addition, two participants exceeded the NIOSH recommendation for core body temperature during work (≥38.0 °C) during the protocol.
Because of time constraints related to study execution, data were collected between October and January, and the NIOSH assumption that workers are heat acclimatized was left unmet/unconfirmed. However, this should have a limited impact, if any, on the findings. Two trials conducted in the heat would not likely have induced any degree of acclimation, and counterbalanced treatment orders should have eliminated any systematic acclimation effect on results if there had been one. Heat acclimation alters physiological set points: for a given submaximal exercise intensity, HR, core body temperature, skin temperature, and perceived exertion are lower, while sweat rate is higher, due to changes in the homeostatic mechanisms through which they function [
41]. So, while absolute values might have been different if participants had been heat acclimated, the nature of the responses between 15 and 120 min should not have been affected.
Future research should expand upon the relationship between cardiovascular drift and O2max at varying work intensities, environmental conditions, clothing requirements, work:rest ratios, and over longer durations. The next steps should include direct assessment of changes in skin blood flow to better understand the extent to which blood flow demand impacts cardiac reserve and O2max. Additionally, the exploration of cardiovascular drift in a sample population that is more representative of the actual working population is recommended, since it is unknown whether co-morbid conditions impact the relationship between cardiovascular drift and O2max.







{kind=link}
{kind=link}
{kind=link}
{kind=link}