
“I’m Hooked on e-cycling, I Can Finally Be Active Again”: Perceptions of e-cycling as a Physical Activity Intervention during Breast Cancer Treatment

Abstract
:1. Introduction
1.1. Breast Cancer and Physical Activity
1.2. Participation Rates and Barriers to Physical Activity
1.3. The Emergence of E-Bikes
1.4. Aims and Research Questions
- What are the perceived barriers and facilitators to e-bike usage during breast cancer treatment?
- When, during cancer treatment, is perceived to be optimum for introducing e-cycling?
- Does the implementation of an e-bike taster session elicit changes in perceptions of e-cycling during breast cancer treatment?
2. Materials and Methods
2.1. Study Design and Protocol
2.2. Researcher Characteristics
2.3. Participant Recruitment
2.3.1. Inclusion and Exclusion Criteria
2.3.2. Sampling
2.4. Interview Questions
2.5. Taster Session
2.6. Ethical Approval
2.7. Data Analysis
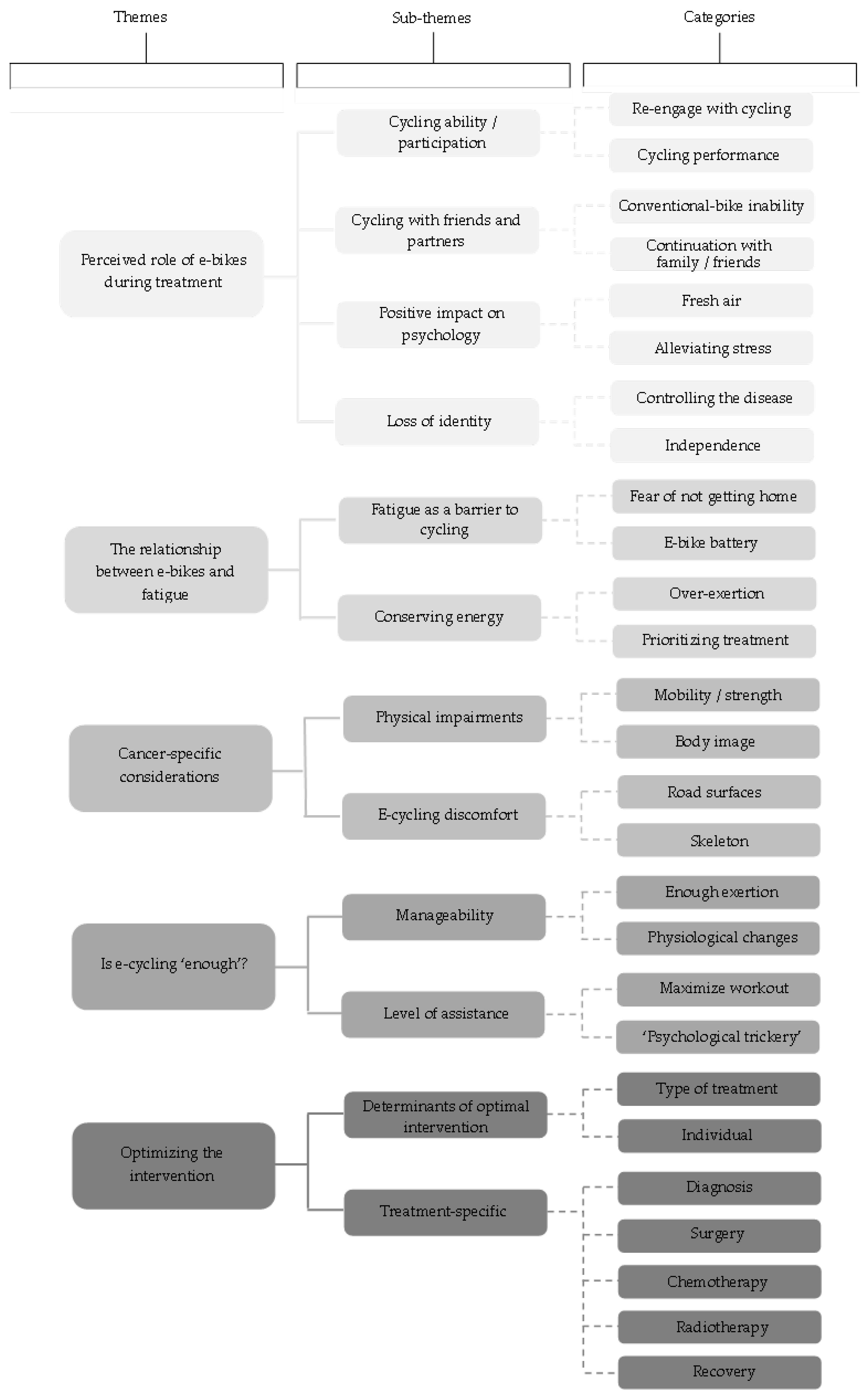
3. Results
3.1. Theme 1: Perceived Role of E-Bikes during Treatment
3.1.1. Cycling Ability/Participation
P.20: “I liked cycling, but it was hard work. Yeah. And, and now, now that I’m diagnosed and I’m on medication, I don’t think I could do it. I’m just exhausted after physical activity.”(Pre-taster, 96 months since diagnosis (SD), multiple cancer diagnoses, undergoing treatment)
P.16: “I don’t use my push bike very much at all. I was reluctant to get on it I think for a long time because I hadn’t got the energy levels to do that. So yes, I think an e-bike definitely would help, knowing that you know I’ve got the power behind me.”(Post-taster, 15 months SD, undergoing treatment)
P.2: “It makes it more do-able, you’d be able to go further distances and hills wouldn’t put you off. So you didn’t, you wouldn’t have to be as fit to cycle with them.”(Post-taster, 49 months SD, undergoing treatment)
P.5: “Then we went up on a hill and of course she told me that I can use a higher program to help, then it was just like same like I was going on a straight, you know, it was like cheating almost, feeling that I’m cheating because that’s not the reality.”(Post-taster, 9 months SD, undergoing hormone treatment)
3.1.2. Cycling with Friends and Partners
P.14: “My partner, and my daughters would go out riding bikes. But I, I wouldn’t go I couldn’t go because I, you know, I just hold them up, I couldn’t keep up with them.”(No-taster session as owned e-bike, 16 months SD, undergoing chemotherapy)
P.20: “There’s lots of people that are using e-bikes to like, so that they can carry on cycling with their partner because their partner is so much fitter and faster than them.”(Pre-taster, 96 months SD, multiple cancers, undergoing treatment)
3.1.3. Positive Impact on Psychology
P.6: “It’s just a wonderful feeling on an e-bike, the freedom the bike gives you, the wind in your hair and going through the countryside is just glorious, and just be able to continue to do that I think is really really important.”(No taster as owned e-bike, 32 months SD, undergoing hormone treatment)
P.15: “I was very stressed to begin with, not quite knowing where it was all going. And, yeah, to me exercise is a way of releasing stress very definitely, and I think e-cycling is perfect in that way, even more than walking for me.”(Pre-taster, 17 months SD, undergoing hormone treatment)
P.5: “I guess, because it’s a kind of stress for me that I’m afraid of the traffic. And it was a stress for me to even just, you know, we mostly used the bike road but there were other bikers, there were there were other pedestrians.”(Post-taster, 9 months SD, undergoing hormone treatment)
3.1.4. Loss of Identity
P.16: “Having the e-bike gives you that security but allows you to have the exercise as well, and and the independence, because otherwise you’re relying on someone else drive you or you have to try and park the car.”(Post-taster, 15 months SD, undergoing treatment)
P.21: “I can’t drive so, I could use the e-bike for exercise and also if I ever wanted to sort of get to a shop or something and you know use it for that, that kind of thing.”(Post-taster, 56 months SD, undergoing chemotherapy)
3.2. Theme 2: The Relationship between E-Bikes and Fatigue
3.2.1. Fatigue as a Barrier to Cycling
P.20: “I was surprised. I just didn’t feel exhausted. I think I was expecting it to take more out of me.”(Post-taster, 96 months SD, multiple cancer diagnoses, undergoing treatment)
P.10: “If I cycled an hour there then that’s also an hour back. But with an e-bike, I feel like you just, you’ve that extra assistance so less worry about getting back, so then you just go a little bit further, I think. I’d be encouraged to go to places that you wouldn’t on a push bike.”(Pre-taster, 17 months SD, undergoing treatment)
P.8: “If you went on a route that is, like, I’m only choosing this route because I’ve got an electric bike so I know I can make it and then the bike breaks and then you’re like, oh what now.”(Post-taster, 17 months SD, undergoing hormone treatment)
3.2.2. Conserving Energy
P.15: “You have to be very careful not to overdo it, because it’s quite exciting to get on an e-bike, you know, and you think oh I’ll have a go, but it’s easy to do too much and suffer from it.”(Post-taster, 17 months SD, undergoing hormone treatment)
P.14: “If I lacked energy, I wouldn’t use an e-bike, I would be trying to conserve my energy for areas where I would need that energy.”(No-taster session as owned e-bike, 16 months SD, undergoing chemotherapy)
3.3. Theme 3: Cancer-Specific Considerations
3.3.1. Physical Impairments
P.9: “I thought maybe, you know, the slight weakness I have in my right arm because of the removal of the lymph node might have affected it, but that wasn’t a problem.”(Post-taster session, 8 months SD, finishing treatment)
P.19: “I don’t think I had the strength in my hand or my arm to hold on and maintain a rigid arm. That was quite difficult.”(Post-taster, 92 months SD, multiple occurrences, undergoing treatment)
3.3.2. E-Cycling Discomfort
P.17: “It wasn’t the exercise as much as the sort of the slight pummeling you get by going on the road on a small thing. So I guess that’s what would stop me using them at points when I was having chemo.”(Post-taster, 3 months SD, undergoing radiotherapy)
P.20: “I think it’s something you’d, if you’re gonna recommend it you to people with stage 4 you’d have to take it on board, you’d have to find out more about their physical condition and assess if it’s suitable for them, I think.”(Post-taster, 96 months SD, multiple cancers, undergoing treatment)
P.18: “I tend to sort of like stand up on the pedals if I know there’s a bump coming or try and avoid it, or whatever. But it’s no more of an issue than it is with an ordinary bike.”(No taster as owned e-bike, 233 months SD, multiple cancers, undergoing hormone treatment)
3.4. Theme 4: Is E-Cycling ‘Enough’?
3.4.1. Manageability
P.20: “The fact that we we went on this this bike ride we got back, and I just didn’t feel exhausted. I think I was expecting it to take it more out of me.”(Post-taster, 96 months SD, multiple cancers, undergoing treatment)
P.19: “I think it was more than I expected because you still feel as though you’re cycling. You don’t feel as though everything’s doing the hard work for you. You feel that you’re having exercise, but just having that extra push when you needed it.”(Post-taster, 92 months SD, multiple occurrences, undergoing treatment)
P.21: “But I was still puffed out when we got to the top, I had to have a little breather. You know I had the full support on I did still need a bit of a breather.”(Post-taster, 56 months SD, undergoing chemotherapy)
3.4.2. Level of Assistance
P.15: “So because I’m feeling fairly fit at the moment, I only had it on the eco level. So, yeah, even though it’s an e-bike, you can choose your level so that’s why it would be quite good because you could sort of tailor it to different people and how that person feels at the time”(Post-taster, 17 months SD, undergoing hormone treatment)
P.7: “Once I finally got used to motor I turned it right down, because I wanted it to be part of my daily exercise.”(Post-taster, 97 months SD, undergoing hormone treatment)
P.13: “It could have a psychological effect because you know you wouldn’t maybe go out on a normal bike, because of how you’re feeling yet you’d go out on an e-bike and end up actually doing the same amount of effort.”(Post-taster, 90 months SD, no current treatment)
3.5. Theme 5: Optimizing the Intervention
P.1: “In general, whether you’d be able to do it with cancer treatments is individual because everyone is so different and everyone’s regime is different.”(Post-taster, 41 months SD, no current treatment)
3.5.1. Diagnosis
P.20: “It’s not when you’re first diagnosed, because it was just like you couldn’t even think something new.”(Post-taster, 96 months SD, multiple cancers, undergoing treatment)
P.7: “The reasons they need it before is so that they can use it to improve their fitness, because the more fit you are before your surgery, the quicker recovery when you come out for chemotherapy.”(Post-taster, 97 months SD, undergoing hormone treatment)
3.5.2. Surgery
P.9: “I guess it depends what surgery you have. If you’ve just had a lumpectomy, you probably could get onto a bike relatively soon.”(Pre-taster session, 8 months since diagnosis, finishing treatment)
P.6: “It would have been the mindfulness of distracting me from all those dark thoughts and all that gloom and you feel like you haven’t got the future. So anything that takes you away from that.”(No taster as owned e-bike, 32 months SD, undergoing hormone treatment)
3.5.3. Chemotherapy
P.13: “Week one, I wouldn’t be able to go for it. But then on week two and three, I was feeling perfectly well, or getting to the stage where I had enough energy to go for it.”(Post-taster, 90 months SD, no current treatment)
P.15: “I think chemo affects the brain too and they have that they say, you know that you have brain fog or kind of things and the dizziness and and all kinds of things which is probably not the very ideal time to go on a bike.”(Pre-taster, 17 months SD, undergoing hormone treatment)
3.5.4. Radiotherapy
P.17: “So, the tiredness wasn’t from the radiotherapy, it was more from the driving to the appointment, you know going to and from the appointment every day.”(Pre-taster, 3 months SD, undergoing radiotherapy)
P.13: “You get radiotherapy burns. Would I have cycled with them? I don’t know, maybe.”(Pre-taster, 90 months SD, no current treatment)
3.5.5. Recovery
P.20: “That sort of rehabilitation, that rebuilding yourself because after being poisoned and, you know, cut open and radiated, you know it’s a lot for your body to go through.”(Post-taster, 96 months SD, multiple cancers, undergoing treatment)
4. Discussion
4.1. The Impact of Taster Sessions
4.2. The Role of E-Bikes during Breast Cancer Treatment
4.2.1. Physical Benefits
4.2.2. Psychological Benefits
4.3. Barriers and Facilitators to E-Cycling
4.3.1. Fatigue
4.3.2. Accessibility
4.3.3. Social Interaction
4.4. Cancer Treatment Considerations
4.5. Strengths and Limitations
4.6. Implications for Practice and Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- NHS. Cancer. Available online: https://www.nhs.uk/conditions/cancer/ (accessed on 25 March 2022).
- World Health Organization. Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 25 March 2022).
- Cancer Research UK. Breast Cancer Incidence (Invasive) Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/breast-cancer/incidence-invasive#ref (accessed on 26 March 2022).
- Hortobagyi, G.N.; de la Garza Salazar, J.; Pritchard, K.; Amadori, D.; Haidinger, R.; Hudis, C.A.; Khaled, H.; Liu, M.C.; Martin, M.; Namer, M.; et al. The global breast cancer burden: Variations in epidemiology and survival. Clin. Breast Cancer 2005, 6, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Momenimovahed, Z.; Salehiniya, H. Epidemiological characteristics of and risk factors for breast cancer in the world. Breast Cancer Targets Ther. 2019, 11, 151–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, A.M.; Weber, B.L. Genetic and hormonal risk factors in breast cancer. J. Natl. Cancer Inst. 2000, 92, 1126–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.S.; Zhao, Z.; Yang, Z.N.; Xu, F.; Lu, H.J.; Zhu, Z.Y.; Shi, W.; Jiang, J.; Yao, P.P.; Zhu, H.P. Risk factors and preventions of breast cancer. Int. J. Biol. Sci. 2017, 13, 1387–1397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parsekar, K.; Howard Wilsher, S.; Sweeting, A.; Patel, A.; Fordham, R. Societal costs of chemotherapy in the UK: An incidence-based cost-of-illness model for early breast cancer. BMJ Open 2021, 11, e039412. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Cardinal, B.J.; Winters-Stone, K.; Smit, E.; Loprinzi, C.L. Physical activity and the risk of breast cancer recurrence: A literature review. Oncol. Nurs. Forum 2012, 39, 269–274. [Google Scholar] [CrossRef] [Green Version]
- Spei, M.E.; Samoli, E.; Bravi, F.; La Vecchia, C.; Bamia, C.; Benetou, V. Physical activity in breast cancer survivors: A systematic review and meta-analysis on overall and breast cancer survival. Breast 2019, 44, 144–152. [Google Scholar] [CrossRef]
- Department of Health & Social Care. UK Chief Medical Officers’ Physical Activity Guidelines. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832868/uk-chief-medical-officers-physical-activity-guidelines.pdf (accessed on 27 March 2022).
- Cannioto, R.A.; Hutson, A.; Dighe, S.; McCann, W.; McCann, S.E.; Zirpoli, G.R.; Barlow, W.; Kelly, K.M.; DeNysschen, C.A.; Hershman, D.L.; et al. Physical activity before, during, and after chemotherapy for high-risk breast cancer: Relationships with survival. J. Natl. Cancer Inst. 2021, 113, 54–63. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Cardinal, B.J. Effects of physical activity on common side effects of breast cancer treatment. Breast Cancer 2012, 19, 4–10. [Google Scholar] [CrossRef]
- Gurgel AR, B.; Mingroni-Netto, P.; Farah, J.C.; de Brito CM, M.; Levin, A.S.; Brum, P.C. Determinants of health and physical activity levels among breast cancer survivors during the COVID-19 pandemic: A cross-sectional study. Front. Physiol. 2021, 12, 624169. [Google Scholar] [CrossRef]
- Pinto, B.M.; Trunzo, J.J.; Reiss, P.; Shiu, S.Y. Exercise participation after diagnosis of breast cancer: Trends and effects on mood and quality of life. Psycho-Oncology 2002, 11, 389–400. [Google Scholar] [CrossRef]
- Wurz, A.; St-Aubin, A.; Brunet, J. Breast cancer survivors’ barriers and motives for participating in a group-based physical activity program offered in the community. Support. Cancer Ther. 2015, 23, 2407–2416. [Google Scholar] [CrossRef] [Green Version]
- Beasley, J.M.; Kwan, M.L.; Chen, W.Y.; Weltzien, E.K.; Kroenke, C.H.; Lu, W.; Nechuta, S.J.; Cadmus-Bertram, L.; Patterson, R.E.; Sternfeld, B.; et al. Meeting the physical activity guidelines and survival after breast cancer: Findings from the after breast cancer pooling project. Breast Cancer Res. Treat. 2012, 131, 637–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mason, C.; Alfano, C.M.; Smith, A.W.; Wang, C.Y.; Neuhouser, M.L.; Duggan, C.; Bernstein, L.; Baumgartner, K.B.; Baumgartner, R.N.; Ballard-Barbash, R.; et al. Long-term physical activity trends in breast cancer survivors. Cancer Epidemiol. Biomark. Prev. 2013, 22, 1153–1161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunet, J.; Taran, S.; Burke, S.; Sabiston, C.M. A qualitative exploration of barriers and motivators to physical activity participation in women treated for breast cancer. Disabil. Rehabil. 2013, 35, 2038–2045. [Google Scholar] [CrossRef] [PubMed]
- Larsson, I.L.; Jönsson, C.; Olsson, A.C.; Gard, G.; Johansson, K. Women’s experience of physical activity following breast cancer treatment. Scand. J. Caring Sci. 2008, 22, 422–429. [Google Scholar] [CrossRef] [PubMed]
- Blackburn, N.E.; Mc Veigh, J.G.; Mc Caughan, E.; Wilson, I.M. The musculoskeletal consequences of breast reconstruction using the latissimus dorsi muscle for women following mastectomy for breast cancer: A critical review. Eur. J. Cancer Care 2018, 27, e12664. [Google Scholar] [CrossRef] [PubMed]
- Steindorf, K.; Schmidt, M.E.; Klassen, O.; Ulrich, C.M.; Oelmann, J.; Habermann, N.; Beckhove, P.; Owen, R.; Debus, J.; Wiskemann, J.; et al. Randomized, controlled trial of resistance training in breast cancer patients receiving adjuvant radiotherapy: Results on cancer-related fatigue and quality of life. Ann. Oncol. 2014, 25, 2237–2243. [Google Scholar] [CrossRef]
- Wilson, D.J. Exercise for the patient after breast cancer surgery. Semin. Oncol. Nurs. 2017, 33, 98–105. [Google Scholar] [CrossRef]
- Rogers, L.Q.; Markwell, S.J.; Verhulst, S.; McAuley, E.; Courneya, K.S. Rural breast cancer survivors: Exercise preferences and their determinants. Psycho-Oncology 2009, 18, 412–421. [Google Scholar] [CrossRef]
- Smith-Turchyn, J.; Richardson, J.; Tozer, R.; McNeely, M.; Thabane, L. Physical activity and breast cancer: A qualitative study on the barriers to and facilitators of exercise promotion from the perspective of health care professionals. Physiother. Can. 2016, 68, 383–390. [Google Scholar] [CrossRef] [Green Version]
- Van Waart, H.; Stuiver, M.M.; Van Harten, W.H.; Geleijn, E.; Kieffer, J.M.; Buffart, L.M.; De Maaker-Berkhof, M.; Boven, E.; Schrama, J.; Geenen, M.M.; et al. Effect of low-intensity physical activity and moderate- to high-intensity physical exercise during adjuvant chemotherapy on physical fitness, fatigue, and chemotherapy completion rates: Results of the PACES randomized clinical trial. Clin. Oncol. 2015, 33, 1918–1927. [Google Scholar] [CrossRef] [Green Version]
- Emery, C.A. Injury prevention in paediatric sport-related injuries: A scientific approach. Br. J. Sport. Med. 2009, 44, 64–69. [Google Scholar] [CrossRef] [Green Version]
- Cheville, A.L.; Tchou, J. Barriers to rehabilitation following surgery for primary breast cancer. J. Surg. Oncol. 2007, 95, 409–418. [Google Scholar] [CrossRef]
- Bourne, J.E.; Sauchelli, S.; Perry, R.; Page, A.; Leary, S.; England, C. Health benefits of electrically-assisted cycling: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 116. [Google Scholar] [CrossRef]
- Fishman, E.; Cherry, C. E-bikes in the mainstream: Reviewing a decade of research. Trans. Rev. 2016, 36, 72–91. [Google Scholar] [CrossRef]
- de Geus, B.; Kempenaers, F.; Lataire, P.; Meeusen, R. Influence of electrically assisted cycling on physiological parameters in untrained subjects. Eur. J. Sport Sci. 2013, 13, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Castro, A.; Gaupp-Berghausen, M.; Dons, E.; Standaert, A.; Laeremans, M.; Clark, A.; Anaya-Boig, E.; Cole-Hunter, T.; Avila-Palencia, I.; Rojas-Rueda, D.; et al. Physical activity of electric bicycle users compared to conventional bicycle users and non-cyclists: Insights based on health and transport data from an online survey in seven European cities. Transp. Res. Interdiscip. Perspect. 2019, 1, 100017. [Google Scholar] [CrossRef]
- Jones, T.; Harms, L.; Heinen, E. Motives, perceptions and experiences of electric bicycle owners and implications for health, wellbeing and mobility. J. Transp. Geogr. 2016, 53, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Sundfør, T.M.; Svendsen, M.; Tonstad, S. Effect of intermittent versus continuous energy restriction on weight loss, maintenance and cardiometabolic risk: A randomized 1-year trial. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 698–706. [Google Scholar] [CrossRef] [Green Version]
- Dons, E.; Rojas-Rueda, D.; Anaya-Boig, E.; Avila-Palencia, I.; Brand, C.; Cole-Hunter, T.; de Nazelle, A.; Eriksson, U.; Gaupp-Berghausen, M.; Gerike, R.; et al. Transport mode choice and body mass index: Cross-sectional and longitudinal evidence from a European-wide study. Environ. Int. 2018, 119, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Sperlich, B.; Zinner, C.; Hebert-Losier, K.; Born, D.P.; Holmberg, H.C. Biomechanical, cardiorespiratory, metabolic and perceived responses to electrically assisted cycling. Eur. J. Appl. Physiol. 2012, 112, 4015–4025. [Google Scholar] [CrossRef] [PubMed]
- Adeoye-Olatunde, O.A.; Olenik, N.L. Research and scholarly methods: Semi-structured interviews. J. Am. Coll. Clin. Pharm. 2021, 4, 1358–1367. [Google Scholar] [CrossRef]
- Redig, A.J.; McAllister, S.S. Breast cancer as a systemic disease: A view of metastasis. J. Intern. Med. 2013, 274, 112–126. [Google Scholar] [CrossRef] [Green Version]
- Guest, G.; Namey, E.; Chen, M. A simple method to assess and report thematic saturation in qualitative research. PLoS ONE 2020, 15, e0232076. [Google Scholar] [CrossRef] [PubMed]
- Price, B. Laddered questions and qualitative data research interviews. J. Adv. Nurs. 2002, 37, 273–281. [Google Scholar] [CrossRef]
- Majid MA, A.; Othman, M.; Mohamad, S.F.; Lim SA, H.; Yusof, A. Piloting for Interviews in Qualitative Research: Operationalization and Lessons Learnt. Int. J. Acad. Res. Bus. Soc. Sci. 2017, 7, 1073–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psycol. 2006, 4, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Guba, E.G. Criteria for assessing the trustworthiness of naturalistic inquiries. Educ. Commun. Technol. J. 1981, 29, 75–91. [Google Scholar] [CrossRef]
- Saballe, C.; Le, H.; Dirin, A. Experience changes the perception and feelings: A case study on mvr application in educational context. Edulearn Proc. 2018, 1, 10204–10213. [Google Scholar] [CrossRef]
- Rey-Barth, S.; Pinsault, N.; Terrisse, H.; Eychenne, C.; Rolland, C.; Foote, A.; Guyot, C.; Bosson, J.L. A program centered on smart electrically assisted bicycle outings for rehabilitation after breast cancer: A pilot study. Med. Eng. Phys. 2022, 100, 103758. [Google Scholar] [CrossRef] [PubMed]
- Popovich, N.; Gordon, E.; Shao, Z.; Xing, Y.; Wang, Y.; Handy, S. Experiences of electric bicycle users in the Sacramento, California Area. Travel Behav. Soc. 2014, 1, 37–44. [Google Scholar] [CrossRef]
- Johnson, M.; Rose, G. Extending life on the bike: Electric bike use by older Australians. J. Transp. Health 2015, 2, 276–283. [Google Scholar] [CrossRef]
- Leger, S.J.; Dean, J.L.; Edge, S.; Casello, J.M. “If I had a regular bicycle, I wouldn’t be out riding anymore”: Perspectives on the potential of e-bikes to support active living and independent mobility among older adults in Waterloo, Canada. Transp. Res. A Policy Pract. 2019, 123, 240–254. [Google Scholar] [CrossRef]
- Marincek, D.; Rérat, P. From conventional to electrically-assisted cycling. A biographical approach to the adoption of the e-bike. Int. J. Sustain. Transp. 2021, 15, 768–777. [Google Scholar] [CrossRef]
- Dill, J.; Rose, G. Electric bikes and transportation policy. Transp. Res. Rec. 2012, 2314, 1–6. [Google Scholar] [CrossRef]
- Fernández-Heredia, Á.; Monzón, A.; Jara-Díaz, S. Understanding cyclists’ perceptions, keys for a successful bicycle promotion. Transp. Res. A Policy Pract. 2014, 63, 1–11. [Google Scholar] [CrossRef]
- Melia, S.; Bartle, C. Who uses e-bikes in the UK and why? Int. J. Sustain. Transp. 2022, 16, 965–977. [Google Scholar] [CrossRef]
- Browall, M.; Mijwel, S.; Rundqvist, H.; Wengström, Y. Physical activity during and after adjuvant treatment for breast cancer: An integrative review of women’s experiences. Integr. Cancer Ther. 2018, 17, 16–30. [Google Scholar] [CrossRef] [Green Version]
- Pudkasam, S.; Feehan, J.; Talevski, J.; Vingrys, K.; Polman, R.; Chinlumprasert, N.; Stojanovska, L.; Apostolopoulos, V. Motivational strategies to improve adherence to physical activity in breast cancer survivors: A systematic review and meta-analysis. Maturitas 2021, 152, 32–47. [Google Scholar] [CrossRef]
- Byrne, H.; Caulfield, B.; De Vito, G. Effects of self-directed exercise programmes on individuals with type 2 diabetes mellitus: A systematic review evaluating their effect on HbA1c and other metabolic outcomes, physical characteristics, cardiorespiratory fitness and functional outcomes. Sports Med. 2017, 47, 717–733. [Google Scholar] [CrossRef]
- Demark-Wahnefried, W.; Hars, V.; Conaway, M.R.; Havlin, K.; Rimer, B.K.; McElveen, G.; Winer, E.P. Reduced rates of metabolism and decreased physical activity in breast cancer patients receiving adjuvant chemotherapy. Am. J. Clin. Nutr. 1997, 65, 1495–1501. [Google Scholar] [CrossRef] [Green Version]
- Kiefer, C.; Behrendt, F. Smart e-bike monitoring system: Real-time open source and open hardware GPS assistance and sensor data for electrically-assisted bicycles. IET Intell. Transp. Syst. 2016, 10, 79–88. [Google Scholar] [CrossRef] [Green Version]
- Rérat, P. The rise of the e-bike: Towards an extension of the practice of cycling? Mobilities 2021, 16, 423–439. [Google Scholar] [CrossRef]
- Jenkins, V.; Shilling, V.; Fallowfield, L.; Howell, A.; Hutton, S. Does hormone therapy for the treatment of breast cancer have a detrimental effect on memory and cognition? A pilot study. Psycho-Oncology 2004, 13, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Nocerino, R.; Colorni, A.; Lia, F.; Luè, A. E-bikes and e-scooters for smart logistics: Environmental and economic sustainability in pro-e-bike Italian pilots. Transp. Res. Proc. 2016, 14, 2362–2371. [Google Scholar] [CrossRef] [Green Version]
- MacArthur, J.; Dill, J.; Person, M. Electric bikes in North America: Results of an online survey. Transp. Res. Rec. 2014, 2468, 123–130. [Google Scholar] [CrossRef]
- Police. UK. Crime Levels Overview. Available online: https://www.police.uk/pu/your-area/avon-somerset-constabulary/bristol-airport/?tab=statistics (accessed on 15 August 2022).
- Simsekoglu, Ö.; Klöckner, C. Factors related to the intention to buy an e-bike: A survey study from Norway. Transp. Res. F Traffic Psychol. Behav. 2019, 60, 573–581. [Google Scholar] [CrossRef]
- Ahlbom, J.; Andersson, D. E-Bike Users Are Lazy… and Healthy: A Study in Consumer Behaviour on the Symbolic Values of E-Bikes, Why Some Want E-Bikes and Others Avoid Them. (Dissertation). Available online: http://urn.kb.se/resolve?urn=urn:nbn:se:hh:diva-40354</div> (accessed on 19 August 2022).
- Sander, A.P.; Wilson, J.; Izzo, N.; Mountford, S.A.; Hayes, K.W. Physical activity and exercise in survivors of breast cancer: A qualitative study. Phys. Ther. 2012, 92, 525–536. [Google Scholar] [CrossRef] [Green Version]
- Iwamitsu, Y.; Shimoda, K.; Abe, H.; Tani, T.; Okawa, M.; Buck, R. Anxiety, emotional suppression, and psychological distress before and after breast cancer diagnosis. Psychosomatics 2005, 46, 19–24. [Google Scholar] [CrossRef]
- Schumacher, J.R.; Palta, M.; Loconte, N.K.; Trentham-Dietz, A.; Witt, W.P.; Heidrich, S.M.; Smith, M.A. Characterizing the psychological distress response before and after a cancer diagnosis. J. Behav. Med. 2013, 36, 591–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schubart, J.R.; Emerich, M.; Farnan, M.; Stanley Smith, J.; Kauffman, G.L.; Kass, R.B. Screening for psychological distress in surgical breast cancer patients. Ann. Surg. Oncol. 2014, 21, 3348–3353. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-H.; Park, N.-J.; McArdle, T. Cancer-Specific Stress and Mood Disturbance: Implications for Symptom Perception, Quality of Life, and Immune Response in Women Shortly after Diagnosis of Breast Cancer. ISRN Nurs. 2012, 2012, 608039. [Google Scholar] [CrossRef] [Green Version]
- Irwin, M.L.; Smith, A.W.; McTiernan, A.; Ballard-Barbash, R.; Cronin, K.; Gilliland, F.D.; Baumgartner, R.N.; Baumgartner, K.B.; Bernstein, L. Influence of pre- and postdiagnosis physical activity on mortality in breast cancer survivors: The health, eating, activity, and lifestyle study. J. Clin. Oncol. 2008, 26, 3958–3964. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, A.A.; Bonsignore, A.; Bland, K.A.; McKenzie, D.C.; Gelmon, K.A.; Van Patten, C.L.; Campbell, K.L. Exercise prescription and adherence for breast cancer: One size does not FITT All. Med. Sci. Sports. Exerc. 2018, 50, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Birt, L.; Scott, S.; Cavers, D.; Campbell, C.; Walter, F. Member checking: A tool to enhance trustworthiness or merely a nod to validation? Qual. Health Res. 2016, 26, 1802–1811. [Google Scholar] [CrossRef] [Green Version]
- Taze, S.S.; Kanan, N. Experiences of women after breast cancer surgery. Florence Nightingale J. Nurs. 2020, 28, 174–183. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variable | N (%) |
|---|---|
| Age, years, mean (SD) | 57.88 (10.8) |
| Sex | |
| Female | 24 (100) |
| Male | 0 (0.0) |
| Ethnicity | |
| White | 22 (91.6) |
| Mixed | 2 (8.3) |
| Asian/Asian British | 0 (0.0) |
| Black/African/Caribbean/Black British | 0 (0.0) |
| Other | 0 (0.0) |
| Education | |
| Less than secondary school | 0 (0.0) |
| Secondary school or equivalent | 8 (33.3) |
| Bachelor’s degree | 9 (37.5) |
| Master’s degree | 5 (20.8) |
| Doctorate | 1 (4.2) |
| Other | 1 (4.2) |
| Employment status | |
| Full-time (35 h or more per week) | 4 (16.7) |
| Part-time | 6 (25.0) |
| Self-employed | 2 (8.3) |
| Unemployed | 2 (8.3) |
| Retired | 8 (33.4) |
| Sick leave | 2 (8.3) |
| Student | 0 (0.0) |
| Marital status | |
| Married | 17 (70.9) |
| Divorced | 2 (8.3) |
| Widowed | 2 (8.3) |
| Unmarried | 3 (12.5) |
| Current treatment status | |
| Ongoing | 20 (83.3) |
| Ended | 4 (16.7) |
| Months since diagnosis, mean (SD) | 40.4 (35.5) |
| Treatment type (combined across treatment window) | |
| Surgery (mastectomy/lumpectomy) | 21 (87.5) |
| Chemotherapy | 14 (58.3) |
| Radiotherapy | 15 (62.5) |
| Hormone therapy | 16 (66.7) |
| Other treatment | 3 (12.5) |
| E-bike ownership | |
| Yes | 4 (16.7) |
| No | 20 (83.3) |
| Pre-Taster Session | Post-Taster Session (Additional) | |
|---|---|---|
| Barriers | Appearance Battery life Energy/fatigue Expensive to buy Difficult to store safely Weight-heavy to pedal and maneuver | E-bike maintenance Theft Difficult to transport Remembering to charge Impact from road |
| Facilitators | Weather Someone to cycle with Cycling history Fitness | Cycle paths Knowledge of cycle routes Sufficient training Purposeful e-cycling groups Cycling ability |
| Benefits | Enhances mood Assistance makes cycling easier Environmentally friendly Independence Able to keep up with partner Prolong cycling duration Tackle hills Less fitness required | Enjoyment (more than conventional-bike) Replace car when commuting Holds space on road Safer than conventional-bike Conserve energy compared to conventional-bike Time savings |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Way, K.M.; Bourne, J.E.; Armstrong, M.E.G. “I’m Hooked on e-cycling, I Can Finally Be Active Again”: Perceptions of e-cycling as a Physical Activity Intervention during Breast Cancer Treatment. Int. J. Environ. Res. Public Health 2023, 20, 5197. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20065197
Way KM, Bourne JE, Armstrong MEG. “I’m Hooked on e-cycling, I Can Finally Be Active Again”: Perceptions of e-cycling as a Physical Activity Intervention during Breast Cancer Treatment. International Journal of Environmental Research and Public Health. 2023; 20(6):5197. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20065197
Chicago/Turabian StyleWay, Kirsty Mollie, Jessica Elizabeth Bourne, and Miranda Elaine Glynis Armstrong. 2023. "“I’m Hooked on e-cycling, I Can Finally Be Active Again”: Perceptions of e-cycling as a Physical Activity Intervention during Breast Cancer Treatment" International Journal of Environmental Research and Public Health 20, no. 6: 5197. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20065197