
A Multi-Pollutant and Meteorological Analysis of Cardiorespiratory Mortality among the Elderly in São Paulo, Brazil—An Artificial Neural Networks Approach



Abstract
:1. Introduction
2. Materials and Methods
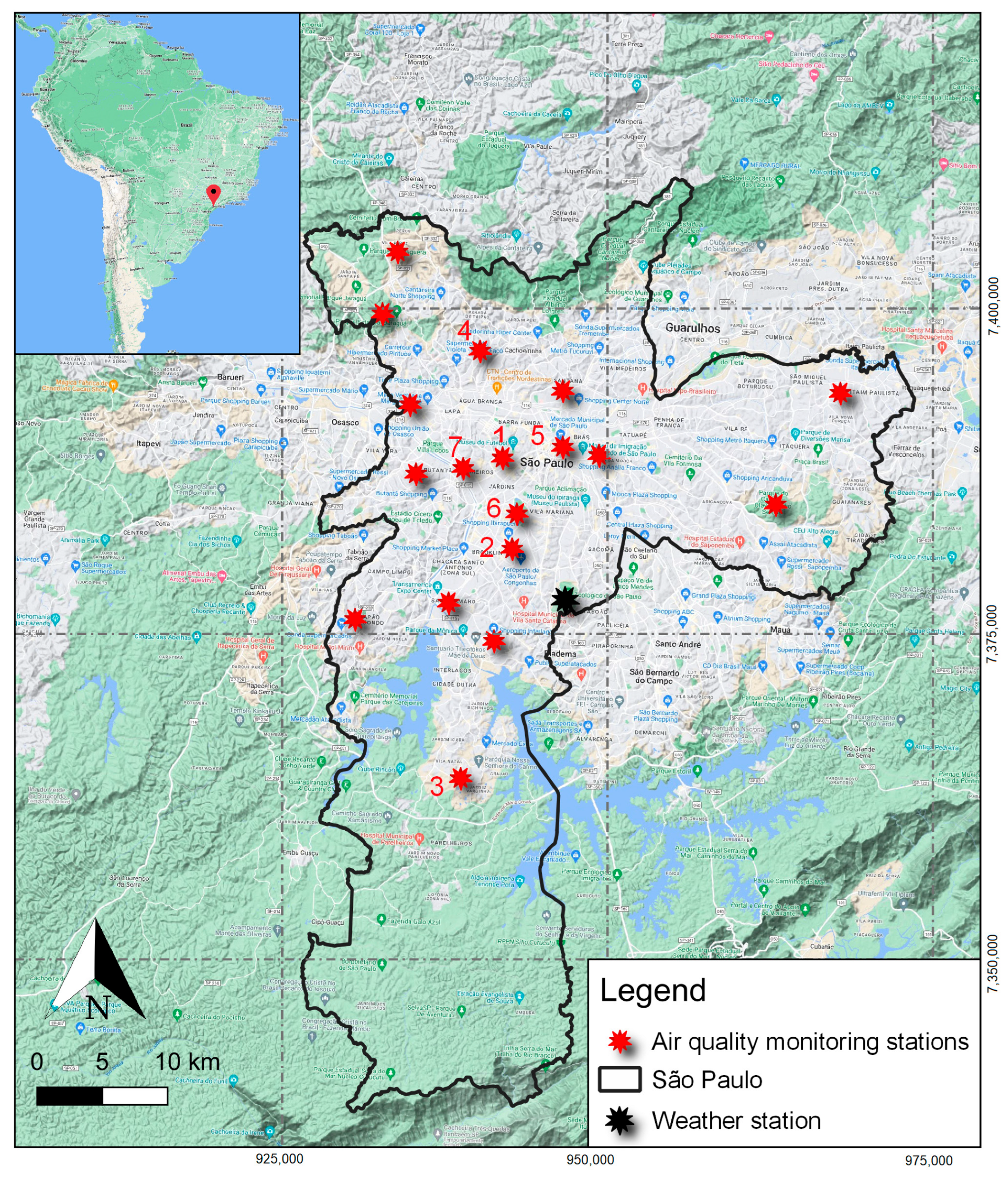
2.1. Study Area, Data Sources, and Processing
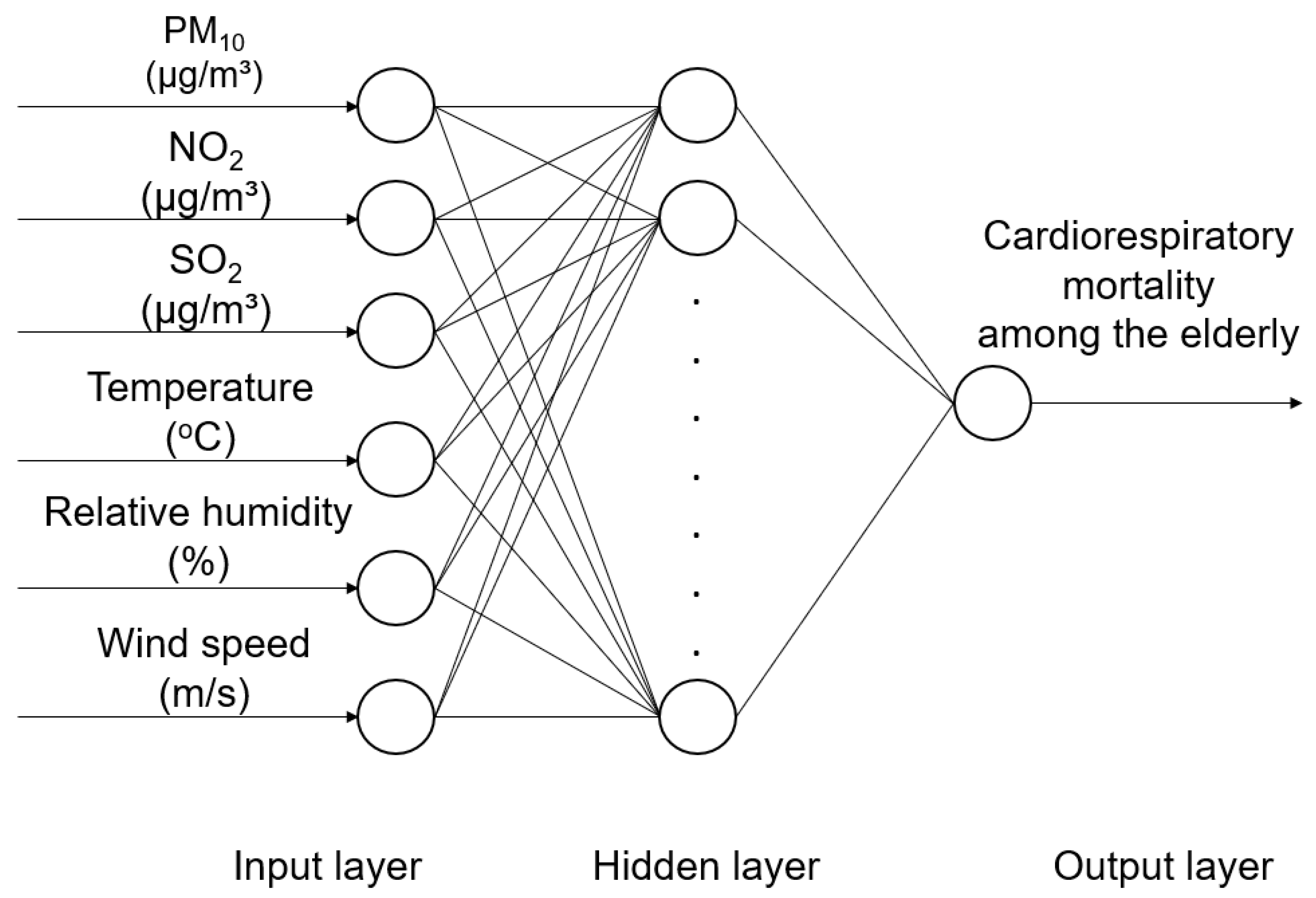
2.2. Artificial Neural Network
2.3. Generalized Linear Model
3. Results
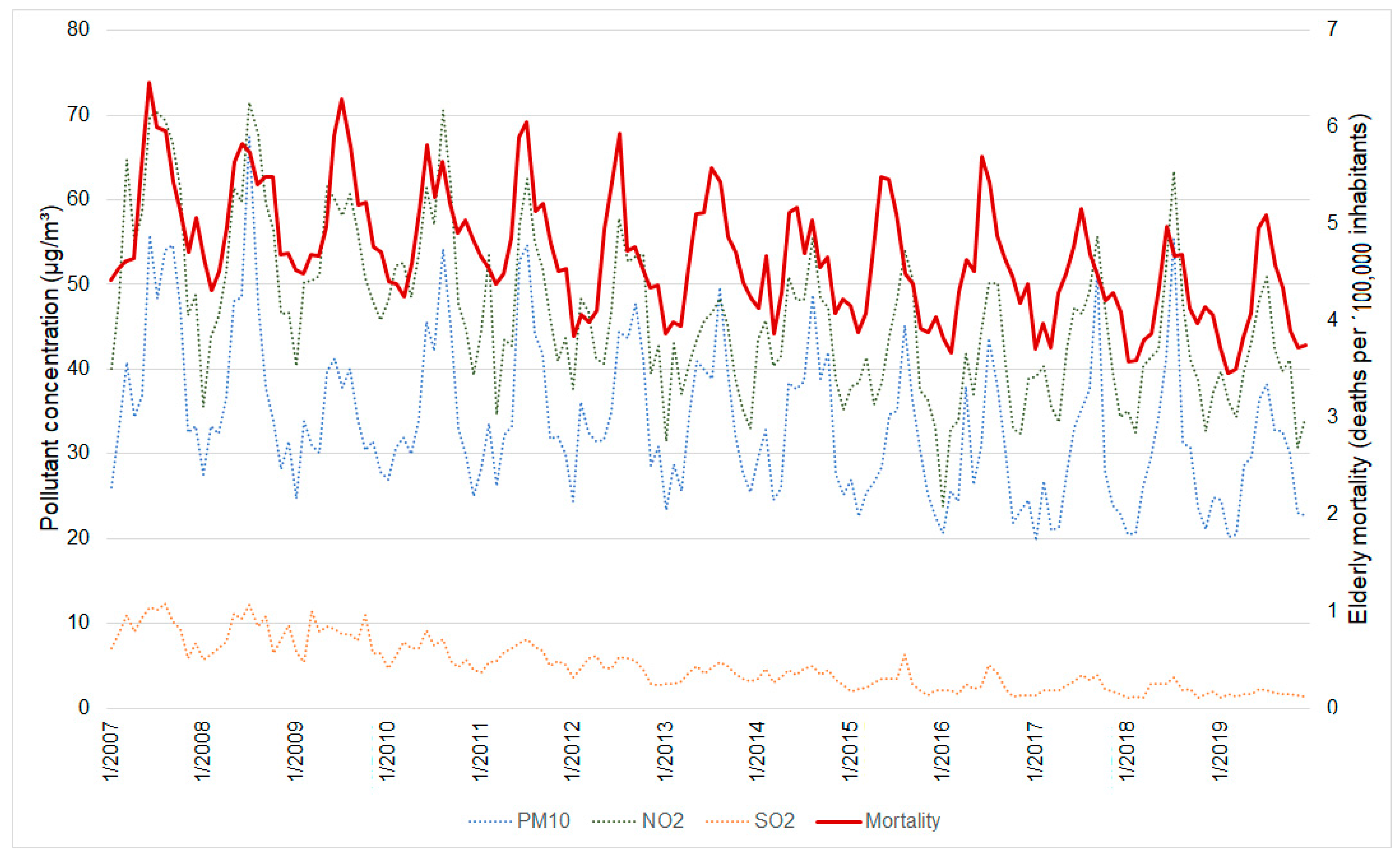
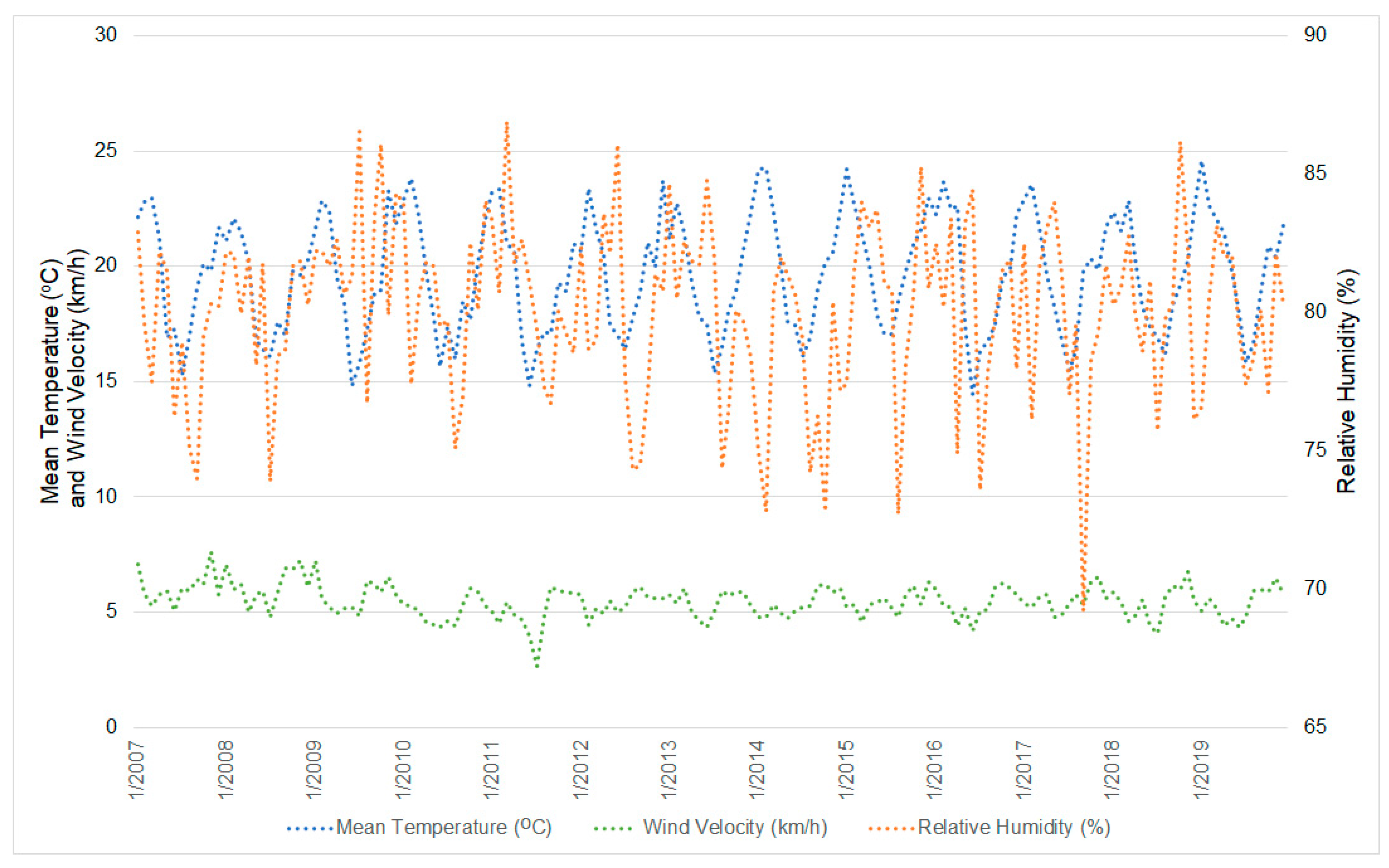
3.1. Descriptive Statistics
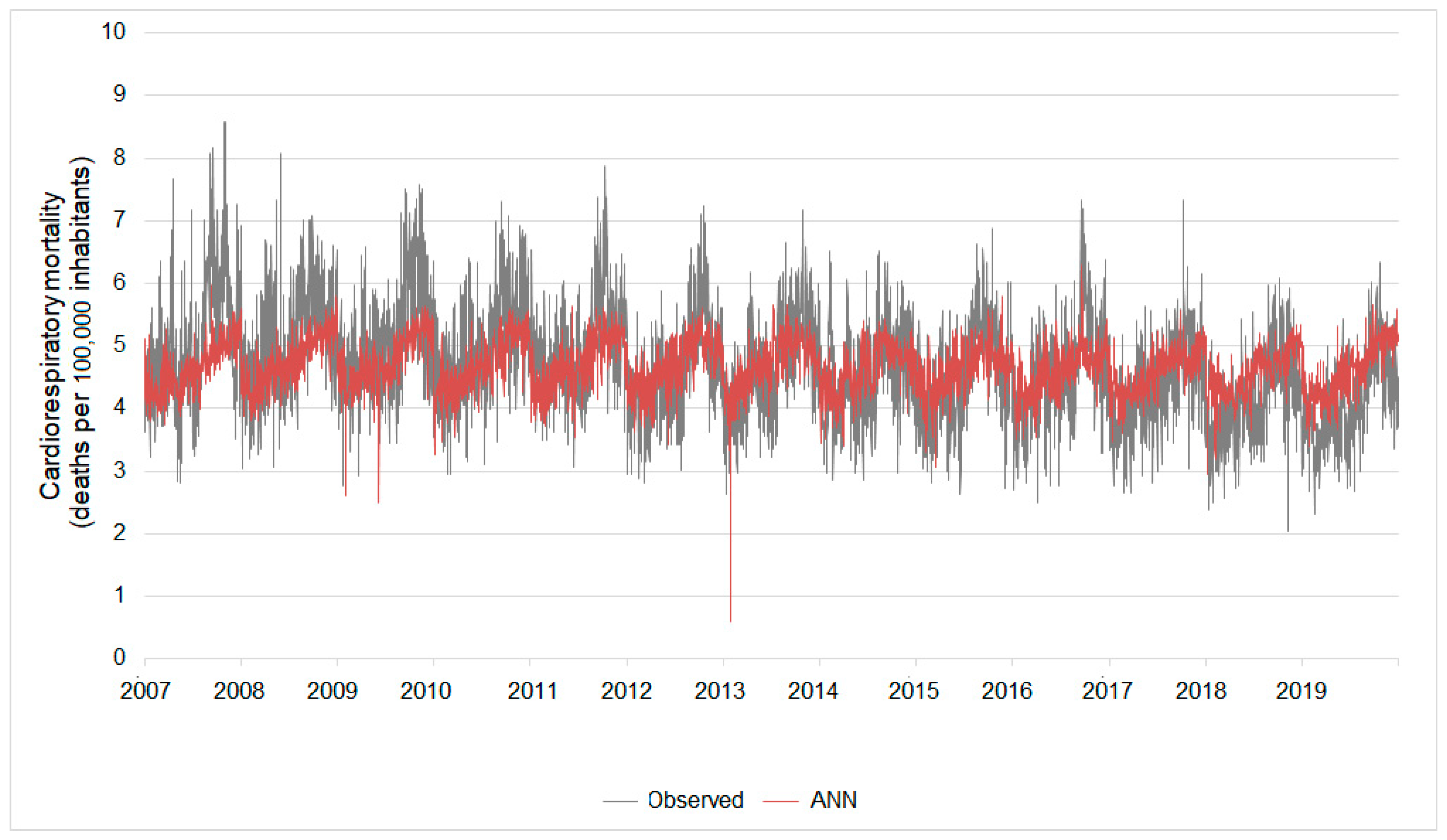
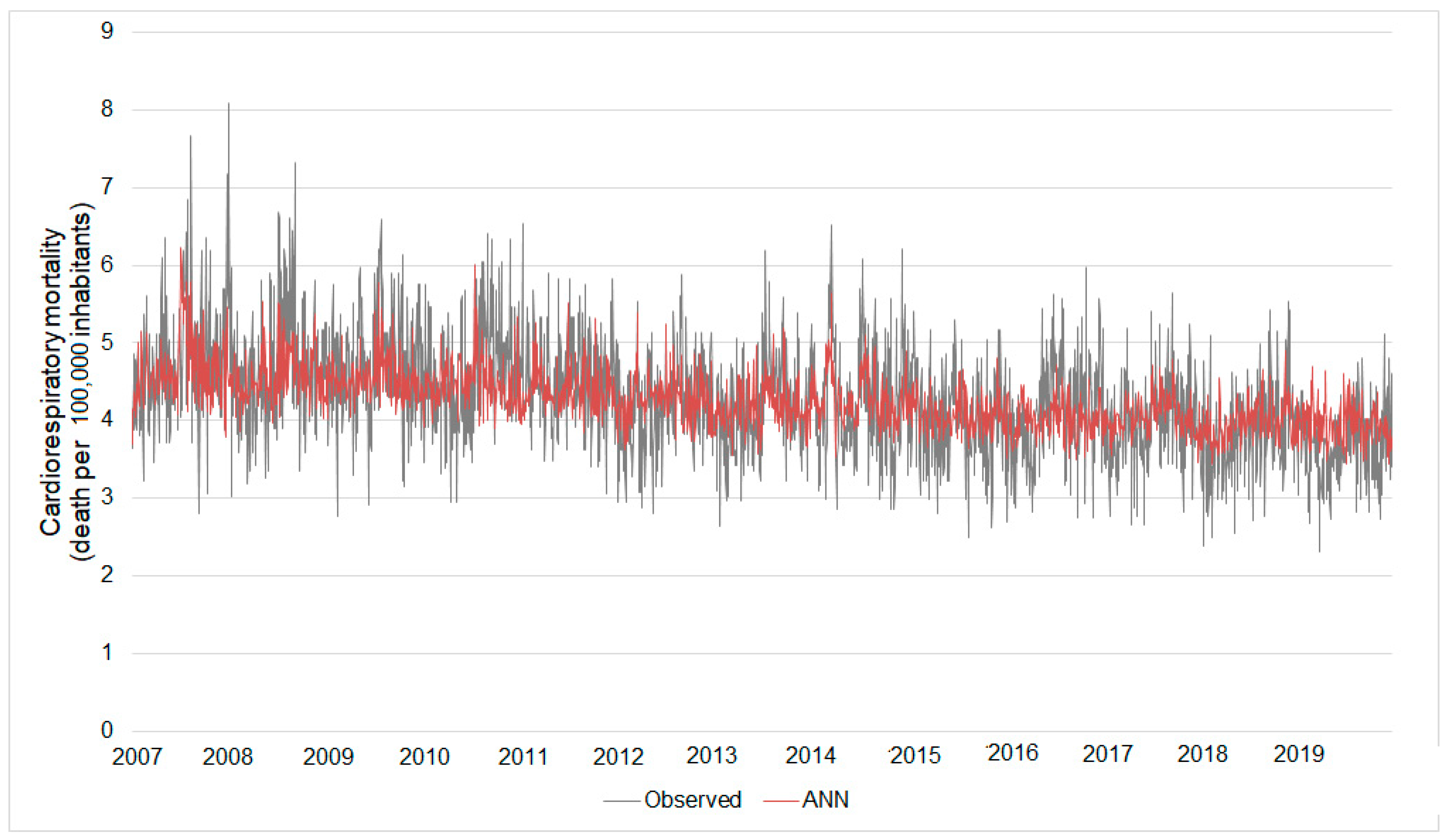
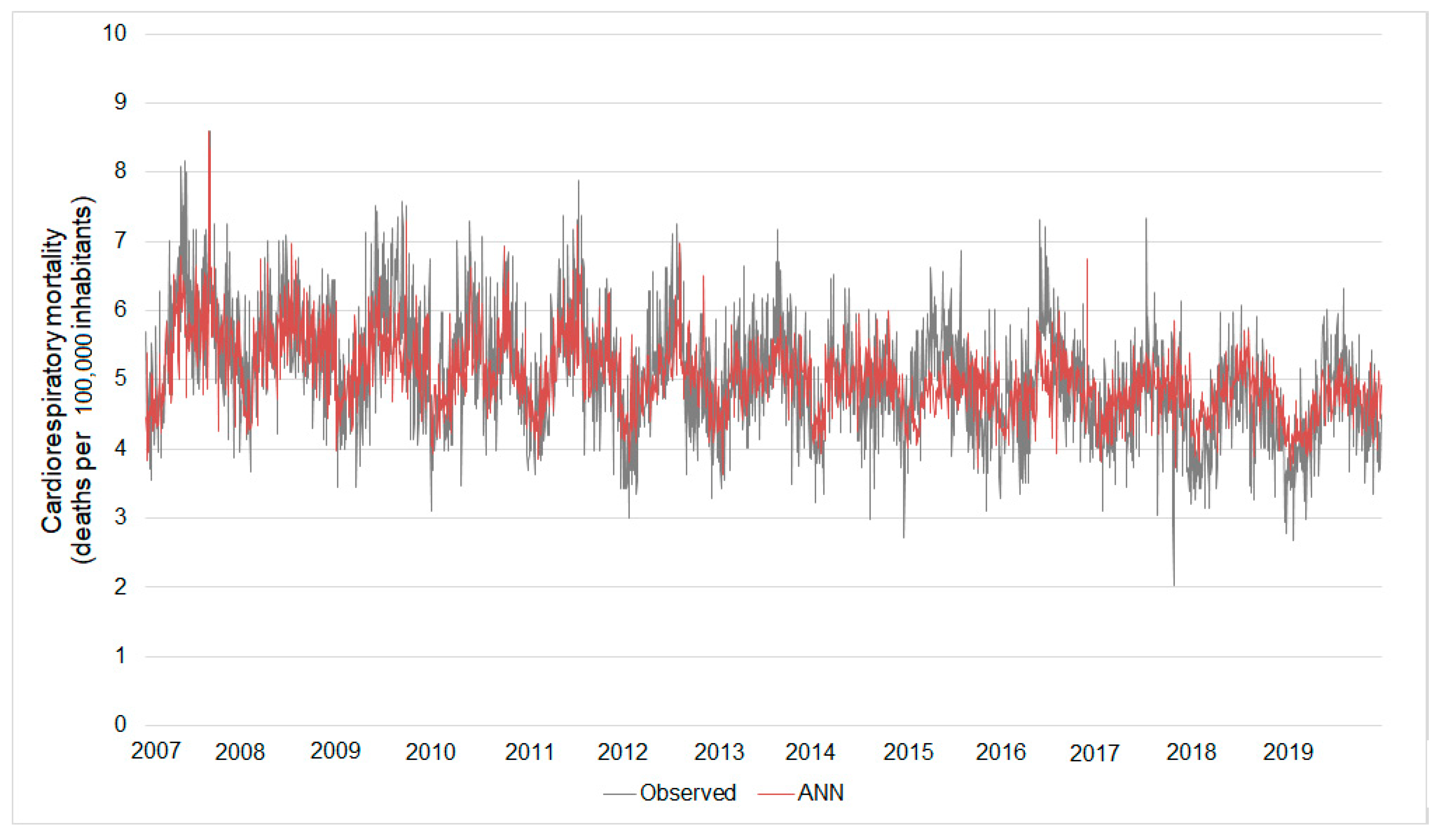
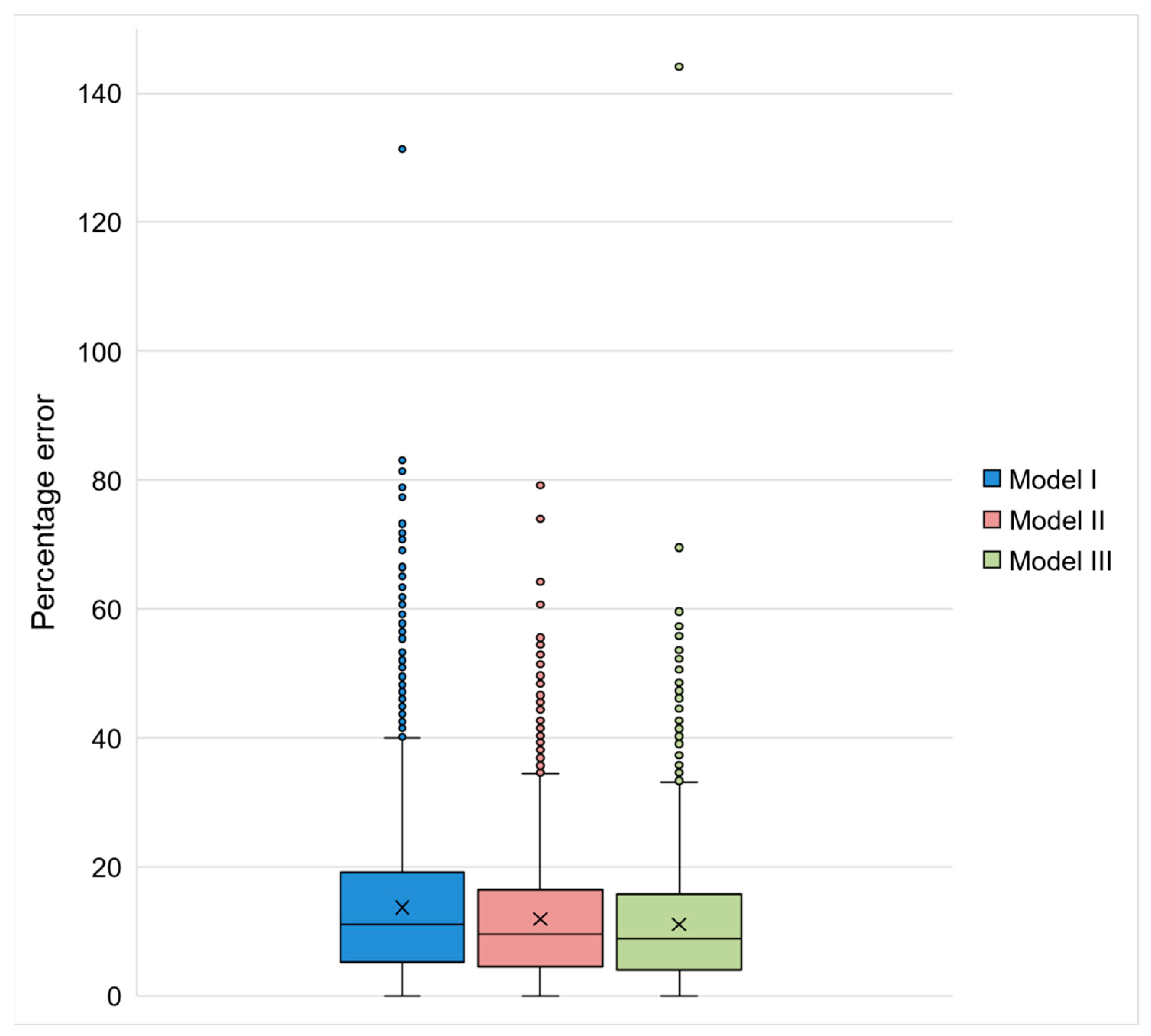
3.2. Artificial Neural Networks
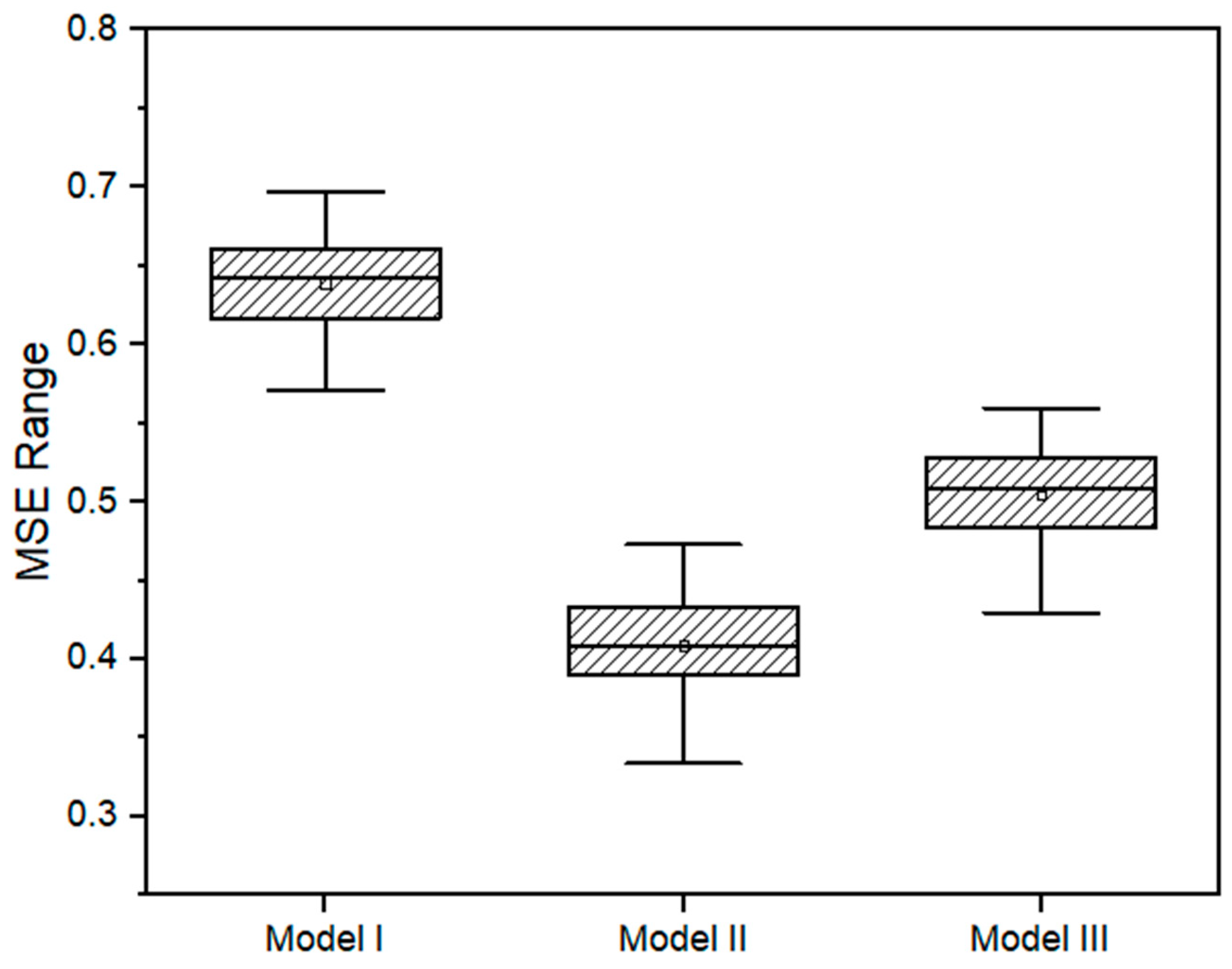
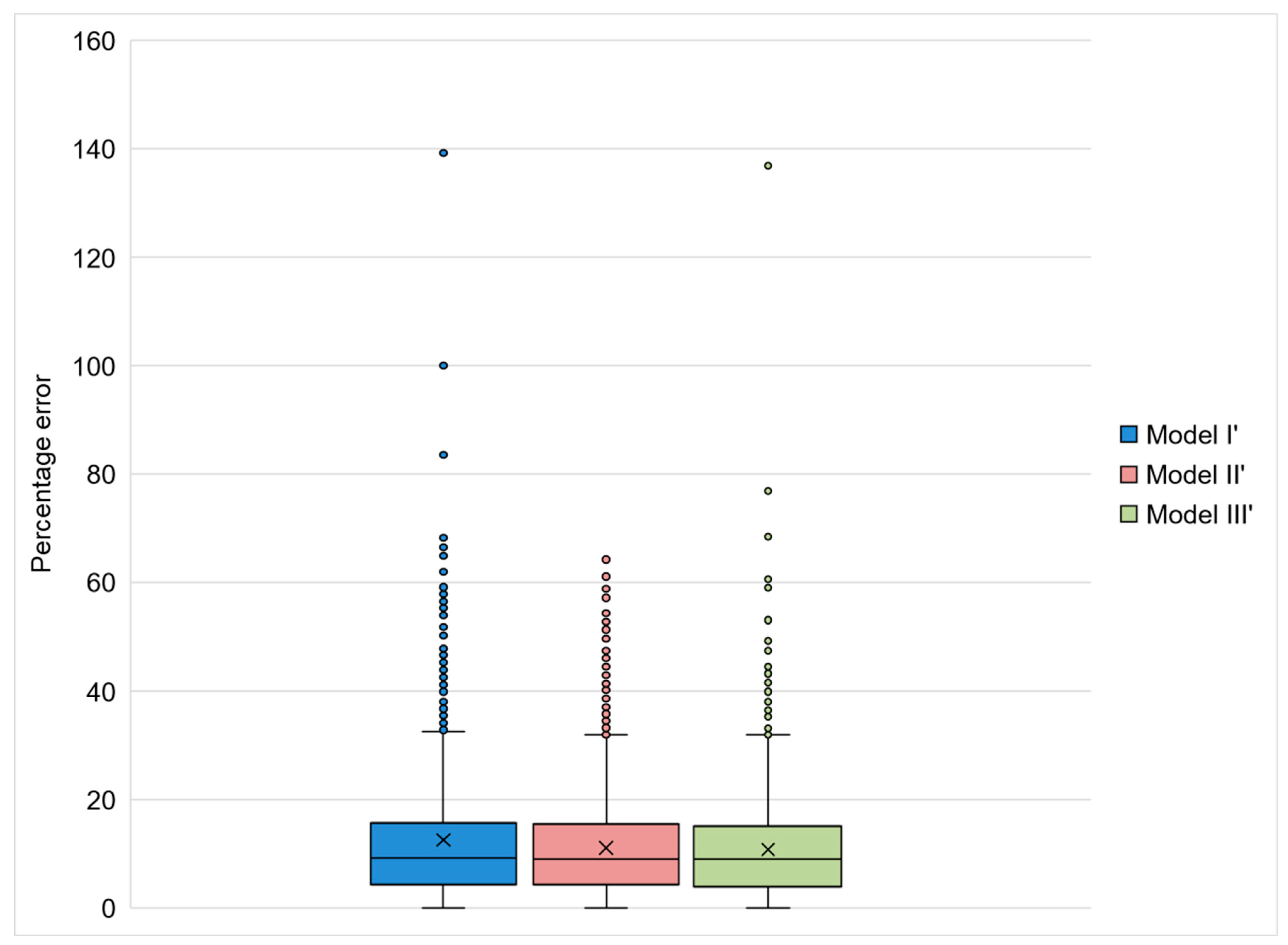
3.3. ANN Validation by the Comparison with GLM Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Ambient Air Pollution. Available online: https://www.who.int/teams/environment-climate-change-and-health/air-quality-and-health/ambient-air-pollution (accessed on 1 August 2021).
- GBD 2019 Risk Factors Collaborators. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- Burnett, R.; Chen, H.; Fann, N.; Hubbell, B.; Pope, C.A.; Frostad, J.; Lim, S.S.; Kan, H.; Walker, K.D.; Thurston, G.D.; et al. Global Estimates of Mortality Associated with Long- Term Exposure to Outdoor Fine Particulate Matter. Proc. Natl. Acad. Sci. USA 2018, 115, 9592–9597. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Z.; Zhu, D. Exposure to Outdoor Air Pollution and Its Human Health Outcomes: A Scoping Review. PLoS ONE 2019, 14, e0216550. [Google Scholar] [CrossRef]
- Requia, W.J.; Adams, M.D.; Arain, A.; Papatheodorou, S.; Koutrakis, P.; Mahmoud, M. Global Association of Air Pollution and Cardiorespiratory Diseases: A Systematic Review, Meta-Analysis, and Investigation of Modifier Variables. Am. J. Public Health 2018, 108, S123–S130. [Google Scholar] [CrossRef] [PubMed]
- Newell, K.; Kartsonaki, C.; Lam, K.B.H.; Kurmi, O.P. Cardiorespiratory Health Effects of Particulate Ambient Air Pollution Exposure in Low-Income and Middle-Income Countries: A Systematic Review and Meta-Analysis. Lancet Planet. Health 2017, 1, e360–e367. [Google Scholar] [CrossRef] [Green Version]
- Krall, J.R.; Chang, H.H.; Waller, L.A.; Mulholland, J.A.; Winquist, A.; Talbott, E.O.; Rager, J.R.; Tolbert, P.E.; Sarnat, S.E. A Multicity Study of Air Pollution and Cardiorespiratory Emergency Department Visits: Comparing Approaches for Combining Estimates across Cities. Environ. Int. 2018, 120, 312–320. [Google Scholar] [CrossRef]
- Seposo, X.; Ueda, K.; Sugata, S.; Yoshino, A.; Takami, A. Short-Term Effects of Air Pollution on Daily Single- and Co-Morbidity Cardiorespiratory Outpatient Visits. Sci. Total Environ. 2020, 729, 138934. [Google Scholar] [CrossRef] [PubMed]
- Landrigan, P.J. Air Pollution and Health. Lancet Public Health 2017, 2, e4–e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makri, A.; Stilianakis, N.I. Vulnerability to Air Pollution Health Effects. Int. J. Hyg. Environ. Health 2008, 211, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Bentayeb, M.; Simoni, M.; Baiz, N.; Norback, D.; Baldacci, S.; Maio, S.; Viegi, G.; Annesi-Maesano, I. Adverse Respiratory Effects of Outdoor Air Pollution in the Elderly. Int. J. Tuberc. Lung Dis. 2012, 16, 1149–1161. [Google Scholar] [CrossRef] [PubMed]
- Simoni, M.; Baldacci, S.; Maio, S.; Cerrai, S.; Sarno, G.; Viegi, G. Adverse Effects of Outdoor Pollution in the Elderly. J. Thorac. Dis. 2015, 7, 34–45. [Google Scholar] [CrossRef] [PubMed]
- Koken, P.J.M.; Piver, W.T.; Ye, F.; Elixhauser, A.; Olsen, L.M.; Portier, C.J. Temperature, Air Pollution, and Hospitalization for Cardiovascular Diseases among Elderly People in Denver. Environ. Health Perspect. 2003, 111, 1312–1317. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.E.; Lim, Y.H.; Kim, H. Temperature Modifies the Association between Particulate Air Pollution and Mortality: A Multi-City Study in South Korea. Sci. Total Environ. 2015, 524–525, 376–383. [Google Scholar] [CrossRef]
- Lepeule, J.; Litonjua, A.A.; Gasparrini, A.; Koutrakis, P.; Sparrow, D.; Vokonas, P.S.; Schwartz, J. Lung Function Association with Outdoor Temperature and Relative Humidity and Its Interaction with Air Pollution in the Elderly. Environ. Res. 2018, 165, 110–117. [Google Scholar] [CrossRef]
- Schwartz, J. Short Term Fluctuations in Air Pollution and Hospital Admissions of the Elderly for Respiratory Disease. Thorax 1995, 50, 531–538. [Google Scholar] [CrossRef] [Green Version]
- Medina-Ramón, M.; Zanobetti, A.; Schwartz, J. The Effect of Ozone and PM10 on Hospital Admissions for Pneumonia and Chronic Obstructive Pulmonary Disease: A National Multicity Study. Am. J. Epidemiol. 2006, 163, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Larrieu, S.; Lefranc, A.; Gault, G.; Chatignoux, E.; Couvy, F.; Jouves, B.; Filleul, L. Are the Short-Term Effects of Air Pollution Restricted to Cardiorespiratory Diseases? Am. J. Epidemiol. 2009, 169, 1201–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, M.; Zeka, A.; Schwartz, J. Association between PM2.5 and All-Cause and Specific-Cause Mortality in 27 US Communities. J. Expo. Sci. Environ. Epidemiol. 2007, 17, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Brunekreef, B.; Hoek, G.; Schouten, L.; Bausch-Goldbohm, S.; Fischer, P.; Armstrong, B.G.; Hughes, E.; Jerrett, M.; Beelen, R.; van den Brandt, P.A. Effects of Long-Term Exposure to Traffic-Related Air Pollution on Respiratory and Cardiovascular Mortality in the Netherlands: The NLCS-AIR Study. Res. Rep. (Health Eff. Inst.) 2009, 139, 5–71. [Google Scholar]
- Dong, G.H.; Zhang, P.; Sun, B.; Zhang, L.; Chen, X.; Ma, N.; Yu, F.; Guo, H.; Huang, H.; Lee, Y.L.; et al. Long-Term Exposure to Ambient Air Pollution and Respiratory Disease Mortality in Shenyang, China: A 12-Year Population-Based Retrospective Cohort Study. Respiration 2012, 84, 360–368. [Google Scholar] [CrossRef]
- Dominski, F.H.; Lorenzetti Branco, J.H.; Buonanno, G.; Stabile, L.; Gameiro da Silva, M.; Andrade, A. Effects of Air Pollution on Health: A Mapping Review of Systematic Reviews and Meta-Analyses. Environ. Res. 2021, 201, 111487. [Google Scholar] [CrossRef]
- Yap, J.; Ng, Y.; Yeo, K.K.; Sahlén, A.; Lam, C.S.P.; Lee, V.; Ma, S. Particulate Air Pollution on Cardiovascular Mortality in the Tropics: Impact on the Elderly. Environ. Health A Glob. Access Sci. Source 2019, 18, 34. [Google Scholar] [CrossRef] [Green Version]
- IBGE. Panorama São Paulo. Available online: https://cidades.ibge.gov.br/brasil/sp/sao-paulo/panorama (accessed on 20 October 2022).
- Abe, K.C.; Miraglia, S.G.E.K. Health Impact Assessment of Air Pollution in São Paulo, Brazil. Int. J. Environ. Res. Public Health 2016, 13, 694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministério da Infraestrutura Frota de Veículos. 2021. Available online: https://www.gov.br/infraestrutura/pt-br/assuntos/transito/conteudo-Senatran/frota-de-veiculos-2021 (accessed on 20 October 2022).
- SEADE PIB SP. Available online: https://www.seade.gov.br/produtos2/ (accessed on 10 April 2021).
- Saldiva, P.H.N.; Lichtenfels, A.J.; Paiva, P.S.O.; Barone, I.A.; Martins, M.A.; Massad, E.; Pereira, J.C.R.; Xavier, V.P.; Singer, J.M.; Böhm, G.M. Association between Air Pollution and Mortality Due to Respiratory Diseases in Children in São Paulo, Brasil. Environ. Res. 1994, 65, 218–225. [Google Scholar] [CrossRef]
- Saldiva, P.H.N.; Pope III, C.A.; Schwartz, J.; Dockery, D.W.; Lichtenfels, A.J.; Salge, J.M.; Barone, I.A.; Bohm, G.M. Air Pollution and Mortality in Elderly People: A Time-Series Study in Sao Paulo, Brazil. Arch. Environ. Health Int. J. 1995, 50, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Pereira, L.A.A.; Loomis, D.; de Conceição, G.M.S.; Braga, A.L.F.; Arcas, R.M.; Kishi, H.S.; Singer, J.M.; Böhm, G.M.; Saldiva, P.H.N. Association between Air Pollution and Intrauterine Mortality in Sao Paulo, Brazil. Environ. Health Perspect. 1998, 106, 325–329. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.A.; Martins, M.A.; Farhat, S.C.; Pope III, C.A.; de Conceição, G.M.S.; Anastácio, V.M.; Hatanaka, M.; Andrade, W.C.; Hamaue, W.R.; Böhm, G.M.; et al. Air Pollution and Respiratory Illness of Children in São Paulo, Brazil. Paediatr. Perinat. Epidemiol. 1999, 13, 475–488. [Google Scholar] [CrossRef]
- Bravo, M.A.; Son, J.; De Freitas, C.U.; Gouveia, N.; Bell, M.L. Air Pollution and Mortality in São Paulo, Brazil: Effects of Multiple Pollutants and Analysis of Susceptible Populations. J. Expo. Sci. Environ. Epidemiol. 2016, 26, 150–161. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.C.; Dos Santos, G.M.S.; de Coêlho, M.S.Z.S.; Miraglia, S.G.E.K. PM 10 Exposure and Cardiorespiratory Mortality—Estimating the Effects and Economic Losses in São Paulo, Brazil. Aerosol Air Qual. Res. 2018, 18, 3127–3133. [Google Scholar] [CrossRef] [Green Version]
- Santana, J.C.C.; Miranda, A.C.; Yamamura, C.L.K.; da Silva Filho, S.C.; Tambourgi, E.B.; Ho, L.L.; Berssaneti, F.T. Effects of Air Pollution on Human Health and Costs: Current Situation in São Paulo, Brazil. Sustainability 2020, 12, 4875. [Google Scholar] [CrossRef]
- Costa, A.F.; Hoek, G.; Brunekreef, B.; de Leon, A.C.M.P. Air Pollution and Deaths among Elderly Residents of São Paulo, Brazil: An Analysis of Mortality Displacement. Environ. Health Perspect. 2017, 125, 349–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, T.M.; Forti, M.C.; de Freitas, C.U.; Nascimento, F.P.; Junger, W.L.; Gouveia, N. Effects of Particulate Matter and Its Chemical Constituents on Elderly Hospital Admissions Due to Circulatory and Respiratory Diseases. Int. J. Environ. Res. Public Health 2016, 13, 947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martins, M.C.H.; Fatigati, F.L.; Véspoli, T.C.; Martins, L.C.; Pereira, L.A.; Martins, M.A.; Saldiva, P.H.N.; Braga, A.L.F. Influence of Socioeconomic Conditions on Air Pollution Adverse Health Effects in Elderly People: An Analysis of Six Regions in São Paulo, Brazil. J. Epidemiol. Community Health 2004, 58, 41–46. [Google Scholar] [CrossRef]
- Dominici, F.; Peng, R.D.; Barr, C.D.; Bell, M.L. Protecting Human Health from Air Pollution: Shifting from a Single-Pollutant to a Multipollutant Approach. Epidemiology 2010, 21, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gold, D.R.; Damokosh, A.I.; Pope, C.A.; Dockery, D.W.; McDonnell, W.F.; Serrano, P.; Retama, A.; Castillejos, M. Particulate and Ozone Pollutant Effects on the Respiratory Function of Children in Southwest Mexico City. Epidemiology 1999, 10, 470. [Google Scholar] [CrossRef] [Green Version]
- Davalos, A.D.; Luben, T.J.; Herring, A.H.; Sacks, J.D. Current Approaches Used in Epidemiologic Studies to Examine Short-Term Multipollutant Air Pollution Exposures. Ann. Epidemiol. 2016, 27, 145–153.e1. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Liu, W.; Wang, X.; Ye, Z.; Tan, Q.; Qiu, W.; Nie, X.; Li, M.; Wang, B.; Chen, W. A Review of Practical Statistical Methods Used in Epidemiological Studies to Estimate the Health Effects of Multi-Pollutant Mixture. Environ. Pollut. 2022, 306, 119356. [Google Scholar] [CrossRef]
- Rodríguez-Villamizar, L.A.; Rojas-Roa, N.Y.; Blanco-Becerra, L.C.; Herrera-Galindo, V.M.; Fernández-Niño, J.A. Short-Term Effects of Air Pollution on Respiratory and Circulatory Morbidity in Colombia 2011–2014: A Multi-City, Time-Series Analysis. Int. J. Environ. Res. Public Health 2018, 15, 1610. [Google Scholar] [CrossRef] [Green Version]
- Jiang, Y.; Chen, J.; Wu, C.; Lin, X.; Zhou, Q.; Ji, S.; Yang, S.; Zhang, X.; Liu, B. Temporal Cross-Correlations between Air Pollutants and Outpatient Visits for Respiratory and Circulatory System Diseases in Fuzhou, China. BMC Public Health 2020, 20, 1131. [Google Scholar] [CrossRef]
- Zhang, J.; Liu, Y.; Cui, L.L.; Liu, S.Q.; Yin, X.X.; Li, H.C. Ambient Air Pollution, Smog Episodes and Mortality in Jinan, China. Sci. Rep. 2017, 7, 11209. [Google Scholar] [CrossRef] [Green Version]
- Shin, H.H.; Owen, J.; Maquiling, A.; Parajuli, R.P.; Smith-Doiron, M. Circulatory Health Risks from Additive Multi-Pollutant Models: Short-Term Exposure to Three Common Air Pollutants in Canada. Environ. Sci. Pollut. Res. 2023, 30, 15740–15755. [Google Scholar] [CrossRef] [PubMed]
- Haykin, S. Redes Neurais Princípios e Prática, 2nd ed.; Grupo, A., Ed.; Pearson Education: Porto Alegre, Brazil, 2001. [Google Scholar]
- Bellinger, C.; Mohomed Jabbar, M.S.; Zaïane, O.; Osornio-Vargas, A. A Systematic Review of Data Mining and Machine Learning for Air Pollution Epidemiology. BMC Public Health 2017, 17, 907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabaneros, S.M.; Calautit, J.K.; Hughes, B.R. A Review of Artificial Neural Network Models for Ambient Air Pollution Prediction. Environ. Model. Softw. 2019, 119, 285–304. [Google Scholar] [CrossRef]
- Araujo, L.N.; Belotti, J.T.; Alves, T.A.; de Tadano, Y.S.; Siqueira, H. Ensemble Method Based on Artificial Neural Networks to Estimate Air Pollution Health Risks. Environ. Model. Softw. 2020, 123, 104567. [Google Scholar] [CrossRef]
- Miranda, A.C.; Santana, J.C.C.; Yamamura, C.L.K.; Rosa, J.M.; Tambourgi, E.B.; Ho, L.L.; Berssaneti, F.T. Application of Neural Network to Simulate the Behavior of Hospitalizations and Their Costs under the Effects of Various Polluting Gases in the City of São Paulo. Air Qual. Atmos. Health 2021, 14, 2091–2099. [Google Scholar] [CrossRef]
- CETESB. Qualidade Do Ar No Estado de São Paulo 2019; CETESB: São Paulo, Brazil, 2020.
- WHO. WHO Global Air Quality Guidelines; WHO: Bonn, Germany, 2021.
- CETESB. Qualidade Do Ar No Estado de São Paulo 2020; CETESB: São Paulo, Brazil, 2021.
- Olden, J.D.; Jackson, D.A. Illuminating the “Black Box”: Understanding Variable Contributions in Artificial Neural Networks. Ecol. Modell. 2002, 154, 135–150. [Google Scholar] [CrossRef]
- McCullagh, P.; Nelder, J.A. Generalized Linear Models, 2nd ed.; Chapman and Hall: London, UK, 1989. [Google Scholar]
- de Souza Conceição, G.M.; Saldiva, P.H.N.; da Motta Singer, J. Modelos MLG e MAG Para Análise Da Associação Entre Poluição Atmosférica e Marcadores de Morbi-Mortalidade: Uma Introdução Baseada Em Dados Da Cidade de São Paulo. Rev. Bras. Epidemiol. 2001, 4, 206–219. [Google Scholar] [CrossRef] [Green Version]
- IAG—USP. Boletim Climatológico Anual Da Estação Meteorológica Do Iag/Usp; IAG—USP: São Paulo, Brazil, 2015. [Google Scholar]
- de Fatima Andrade, M.; Kumar, P.; de Freitas, E.D.; Ynoue, R.Y.; Martins, J.; Martins, L.D.; Nogueira, T.; Perez-Martinez, P.; de Miranda, R.M.; Albuquerque, T.; et al. Air Quality in the Megacity of São Paulo: Evolution over the Last 30 Years and Future Perspectives. Atmos. Environ. 2017, 159, 66–82. [Google Scholar] [CrossRef] [Green Version]
- Lencioni, S. Mudanças Na Metrópole de São Paulo (Brasil) e Transformações Industriais. Rev. Dep. Geogr. 1998, 12, 27–42. [Google Scholar] [CrossRef]
- Martins, L.C.; do Rosário Dias de Oliveira Latorre, M.; Saldiva, P.P.H.N.; Braga, A.L.F. Relação Entre Poluição Atmosférica e Atendimentos Por Infecção de Vias Aéreas Superiores No Município de São Paulo: Avaliação Do Rodízio de Veículos. Rev. Bras. Epidemiol. 2001, 4, 220–229. [Google Scholar] [CrossRef] [Green Version]
- Szwarcfiter, L.; Mendes, F.E.; La Rovere, E.L. Enhancing the Effects of the Brazilian Program to Reduce Atmospheric Pollutant Emissions from Vehicles. Transp. Res. Part D Transp. Environ. 2005, 10, 153–160. [Google Scholar] [CrossRef]
- Boldt, T.; da Silva, A.W.; de Souza Leal, C. Uma Análise Físico-Química Dos Catalisadores Automotivos: Estudo Introdutório Das Propriedades e Eficiência Catalítica. In Proceedings of the 2o Simpósio de Integração Científica e Tecnológica do Sul Catarinense, Araranguá, Brazil, 21–22 October 2003; pp. 248–260. [Google Scholar]
- do Carmo Rangel, M.; Carvalho, M.F.A. Impacto Dos Catalisadores Automotivos No Controle Da Qualidade Do Ar. Quim. Nova 2003, 26, 265–277. [Google Scholar] [CrossRef] [Green Version]
- De Carvalho, R.N.; Vicentini, P.C.; de Sá, R.A.B.; Villela, A.C.S.; Botero, S.W. A Nova Gasolina S50 E O Proconve L6. In Proceedings of the XXI Simpósio Internacional de Engenharia Automotiva; 2014; pp. 184–193. [Google Scholar] [CrossRef] [Green Version]
- Daemme, L.C.; Penteado, R.; Vicentini, P.C.; Errera, M.R. Impacto Da Redução Do Teor de Enxofre Da Gasolina S800 Para S50 Nas Emissões Da Frota Brasileira. In Proceedings of the XXVII Simpósio Internacional de Engenharia Automotiva, São Paulo, Brazil, 1 August 2019. [Google Scholar]
- Pérez-Martínez, P.J.; de Fátima Andrade, M.; de Miranda, R.M. Heavy Truck Restrictions and Air Quality Implications in São Paulo, Brazil. J. Environ. Manag. 2017, 202, 55–68. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Gouveia, N.; Salvo, A. External Effects of Diesel Trucks Circulating Inside the São Paulo Megacity. J. Eur. Econ. Assoc. 2019, 17, 947–989. [Google Scholar] [CrossRef] [Green Version]
- Sánchez-Ccoyllo, O.R.; de Andrade, M.F. The Influence of Meteorological Conditions on the Behavior of Pollutants Concentrations in São Paulo, Brazil. Environ. Pollut. 2002, 116, 257–263. [Google Scholar] [CrossRef]
- Bourotte, C.; Forti, M.C.; Taniguchi, S.; Bícego, M.C.; Lotufo, P.A. A Wintertime Study of PAHs in Fine and Coarse Aerosols in São Paulo City, Brazil. Atmos. Environ. 2005, 39, 3799–3811. [Google Scholar] [CrossRef]
- Castanho, A.D.A.; Artaxo, P. Wintertime and Summertime São Paulo Aerosol Source Apportionment Study. Atmos. Environ. 2001, 35, 4889–4902. [Google Scholar] [CrossRef]
- Martins, L.C.; Latorre, M.D.R.D.D.O.; Cardoso, M.R.A.; Gonçalves, F.L.T.; Saldiva, P.H.N.; Braga, A.L.F. Air Pollution and Emergency Room Visits Due to Pneumonia and Influenza in São Paulo, Brazil. Rev. Saude Publica 2002, 36, 88–94. [Google Scholar] [CrossRef] [Green Version]
- Francisco, P.M.S.B.; Donalisio, M.R.; Lattorre, M.D.R.D.D.O. Internações Por Doenças Respiratórias Em Idosos e a Intervenção Vacinal Contra Influenza No Estado de São Paulo Respiratory Disease Hospitalization in the Elderly in the State of São. Rev. Bras. Epidemiol. 2004, 7, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Larasati, A.; DeYong, C.; Slevitch, L. Comparing Neural Network and Ordinal Logistic Regression to Analyze Attitude Responses. Serv. Sci. 2011, 3, 304–312. [Google Scholar] [CrossRef] [Green Version]
- Shakerkhatibi, M.; Dianat, I.; Asghari Jafarabadi, M.; Azak, R.; Kousha, A. Air Pollution and Hospital Admissions for Cardiorespiratory Diseases in Iran: Artificial Neural Network versus Conditional Logistic Regression. Int. J. Environ. Sci. Technol. 2015, 12, 3433–3442. [Google Scholar] [CrossRef] [Green Version]
- Khojasteh, D.N.; Goudarzi, G.; Taghizadeh-Mehrjardi, R.; Asumadu-Sakyi, A.B.; Fehresti-Sani, M. Long-Term Effects of Outdoor Air Pollution on Mortality and Morbidity–Prediction Using Nonlinear Autoregressive and Artificial Neural Networks Models. Atmos. Pollut. Res. 2021, 12, 46–56. [Google Scholar] [CrossRef]
- Kassomenos, P.; Petrakis, M.; Sarigiannis, D.; Gotti, A.; Karakitsios, S. Identifying the Contribution of Physical and Chemical Stressors to the Daily Number of Hospital Admissions Implementing an Artificial Neural Network Model. Air Qual. Atmos. Health 2011, 4, 263–272. [Google Scholar] [CrossRef]
- Kachba, Y.R.; de Genaro Chiroli, D.M.; Belotti, J.T.; Alves, T.A.; de Souza Tadano, Y.; Siqueira, H. Influence of Vehicular Emission Variables To Morbidity and Mortality in the Largest Metropolis in South America. Sustainability 2020, 12, 2621. [Google Scholar] [CrossRef] [Green Version]
- de Souza Tadano, Y.; Bacalhau, E.T.; Casacio, L.; Puchta, E.; Pereira, T.S.; Antonini Alves, T.; Ugaya, C.M.L.; Siqueira, H.V. Unorganized Machines to Estimate the Number of Hospital Admissions Due to Respiratory Diseases Caused by Pm10 Concentration. Atmosphere 2021, 12, 1345. [Google Scholar] [CrossRef]
- Seo, S.; Min, C.; Preston, M.; Han, S.; Choi, S.H.; Kang, S.Y.; Kim, D. Ambient PM Concentrations as a Precursor of Emergency Visits for Respiratory Complaints: Roles of Deep Learning and Multi-Point Real-Time Monitoring. Sustainability 2022, 14, 2703. [Google Scholar] [CrossRef]
- Polezer, G.; Tadano, Y.S.; Siqueira, H.V.; Godoi, A.F.L.; Yamamoto, C.I.; de André, P.A.; Pauliquevis, T.; de Andrade, M.F.; Oliveira, A.; Saldiva, P.H.N.; et al. Assessing the Impact of PM 2.5 on Respiratory Disease Using Artificial Neural Networks. Environ. Pollut. 2018, 235, 394–403. [Google Scholar] [CrossRef]
- Air, I.; Munksgaard, B. Significance of Humidity and Temperature on Skin and Upper Airway Symptoms. Indoor Air 2003, 13, 344–352. [Google Scholar]
- Nguyen, J.L.; Schwartz, J.; Dockery, D.W. The Relationship between Indoor and Outdoor Temperature, Apparent Temperature, Relative Humidity, and Absolute Humidity. Indoor Air 2014, 24, 103–112. [Google Scholar] [CrossRef] [Green Version]
- Guergova, S.; Dufour, A. Thermal Sensitivity in the Elderly: A Review. Ageing Res. Rev. 2011, 10, 80–92. [Google Scholar] [CrossRef]
- Diniz, F.R.; Gonçalves, F.L.T.; Sheridan, S. Heat Wave and Elderly Mortality: Historical Analysis and Future Projection for Metropolitan Region of Sao Paulo, Brazil. Atmosphere 2020, 11, 933. [Google Scholar] [CrossRef]
- Leirião, L.F.L.; Miraglia, S.G.E.K. Environmental and Health Impacts Due to the Violation of Brazilian Emissions Control Program Standards in Sao Paulo Metropolitan Area. Transp. Res. Part D Transp. Environ. 2019, 70, 70–76. [Google Scholar] [CrossRef]
- Leirião, L.F.L.; Debone, D.; Pauliquevis, T.; do Rosário, N.; Miraglia, S. Environmental and Public Health Effects of Vehicle Emissions in a Large Metropolis: Case Study of a Truck Driver Strike in Sao Paulo, Brazil. Atmos. Pollut. Res. 2020, 11, 24–31. [Google Scholar] [CrossRef]
- Costa, S.; Ferreira, J.; Silveira, C.; Costa, C.; Lopes, D.; Relvas, H.; Borrego, C.; Roebeling, P.; Miranda, A.I.; Paulo Teixeira, J. Integrating Health on Air Quality Assessment—Review Report on Health Risks of Two Major European Outdoor Air Pollutants: PM and NO2. J. Toxicol. Environ. Health Part B Crit. Rev. 2014, 17, 307–340. [Google Scholar] [CrossRef]
- De Veaux, R.D.; Ungar, L.H. Multicollinearity: A Tale of Two Nonparametric Regressions. In Selecting Models from Data; Cheeseman, P., Oldford, R.W., Eds.; Springer: New York, NY, USA, 1994; pp. 393–402. [Google Scholar]
- Aga, E.; Samoli, E.; Touloumi, G.; Anderson, H.R.; Cadum, E.; Forsberg, B.; Goodman, P.; Goren, A.; Kotesovec, F.; Kriz, B.; et al. Short-Term Effects of Ambient Particles on Mortality in the Elderly: Results from 28 Cities in the APHEA2 Project. Eur. Respir. J. 2003, 21 (Suppl. S40), 28–33. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Kan, H.; Chen, B.; Huang, W.; Bai, Z.; Song, G.; Pan, G. Association of Particulate Air Pollution with Daily Mortality: The China Air Pollution and Health Effects Study. Am. J. Epidemiol. 2012, 175, 1173–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filleul, L.; Tertre, A.L.; Baldi, I.; Tessier, J.F. Difference in the Relation between Daily Mortality and Air Pollution among Elderly and All-Ages Populations in Southwestern France. Environ. Res. 2004, 94, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Schwalbe, N.; Wahl, B. Artificial Intelligence and the Future of Global Health. Lancet 2020, 395, 1579–1586. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Importance (Position of Importance) (%) | |||
|---|---|---|---|
| Variable | Model I | Model II | Model III |
| PM10 concentration | 12.32 (4) | 68.34 (1) | 29.07 (1) |
| NO2 concentration | 13.22 (3) | 6.81 (3) | 27.02 (2) |
| SO2 concentration | 46.75 (1) | 3.01 (5) | 16.51 (4) |
| Temperature | 19.11 (2) | 13.10 (2) | 9.56 (5) |
| Relative humidity | 4.80 (5) | 6.10 (4) | 16.67 (3) |
| Wind speed | 3.80 (6) | 2.64 (6) | 1.17 (6) |
| Model I’ | Model II’ | Model III’ | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | 95% CI | p-Value | β | 95% CI | p-Value | β | 95% CI | p-Value | ||||
| (Intercept) | 1.626 | 1.528 | 1.724 | <0.000 | 1.168 | 1.021 | 1.315 | <0.000 | 1.583 | 1.464 | 1.703 | <0.000 |
| PM10 | 0.000 | 0.000 | 0.001 | 0.500 | 0.000 | −0.001 | 0.001 | 0.753 | 0.001 | 0.000 | 0.002 | 0.008 |
| NO2 | 0.001 | 0.000 | 0.001 | 0.014 | 0.000 | 0.000 | 0.001 | 0.543 | 0.001 | 0.000 | 0.002 | 0.036 |
| SO2 | −0.003 | −0.005 | −0.001 | 0.003 | −0.002 | −0.005 | 0.000 | 0.104 | −0.003 | −0.006 | 0.000 | 0.035 |
| Temperature | 0.001 | −0.002 | 0.003 | 0.648 | 0.011 | 0.007 | 0.015 | <0.000 | −0.008 | −0.011 | −0.005 | <0.000 |
| Relative humidity | −0.002 | −0.003 | −0.001 | <0.000 | −0.001 | −0.002 | 0.000 | 0.009 | −0.001 | −0.002 | 0.000 | 0.035 |
| Wind speed | −0.001 | −0.004 | 0.002 | 0.570 | 0.002 | −0.002 | 0.006 | 0.349 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leirião, L.; de Oliveira, M.; Martins, T.; Miraglia, S. A Multi-Pollutant and Meteorological Analysis of Cardiorespiratory Mortality among the Elderly in São Paulo, Brazil—An Artificial Neural Networks Approach. Int. J. Environ. Res. Public Health 2023, 20, 5458. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20085458
Leirião L, de Oliveira M, Martins T, Miraglia S. A Multi-Pollutant and Meteorological Analysis of Cardiorespiratory Mortality among the Elderly in São Paulo, Brazil—An Artificial Neural Networks Approach. International Journal of Environmental Research and Public Health. 2023; 20(8):5458. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20085458
Chicago/Turabian StyleLeirião, Luciana, Michelle de Oliveira, Tiago Martins, and Simone Miraglia. 2023. "A Multi-Pollutant and Meteorological Analysis of Cardiorespiratory Mortality among the Elderly in São Paulo, Brazil—An Artificial Neural Networks Approach" International Journal of Environmental Research and Public Health 20, no. 8: 5458. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20085458