
Predictors of Youth Accessibility for a Mobile Phone-Based Life Skills Training Program for Addiction Prevention

Abstract
:1. Introduction
2. Methods
2.1. Participants, Setting, and Procedure
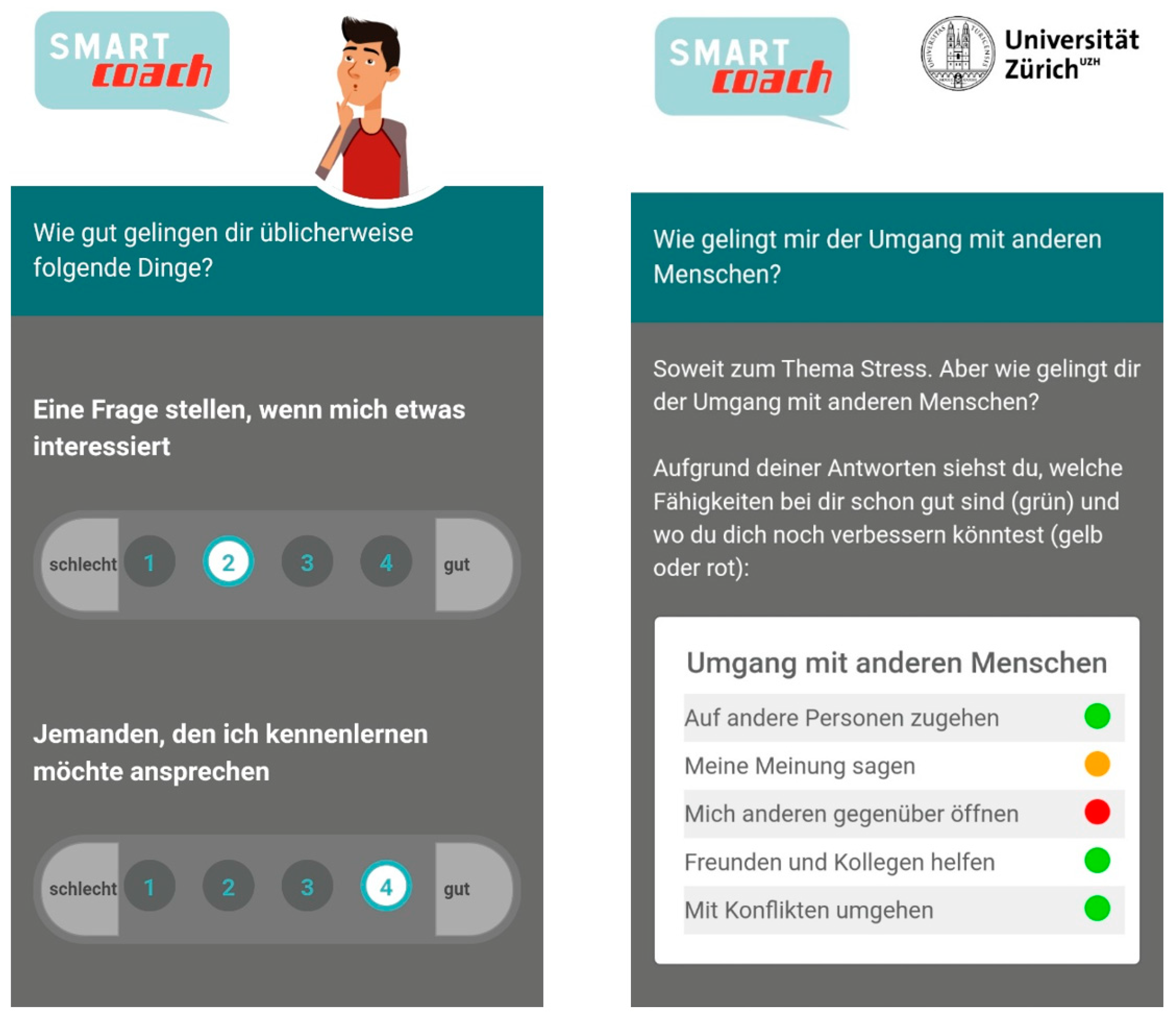
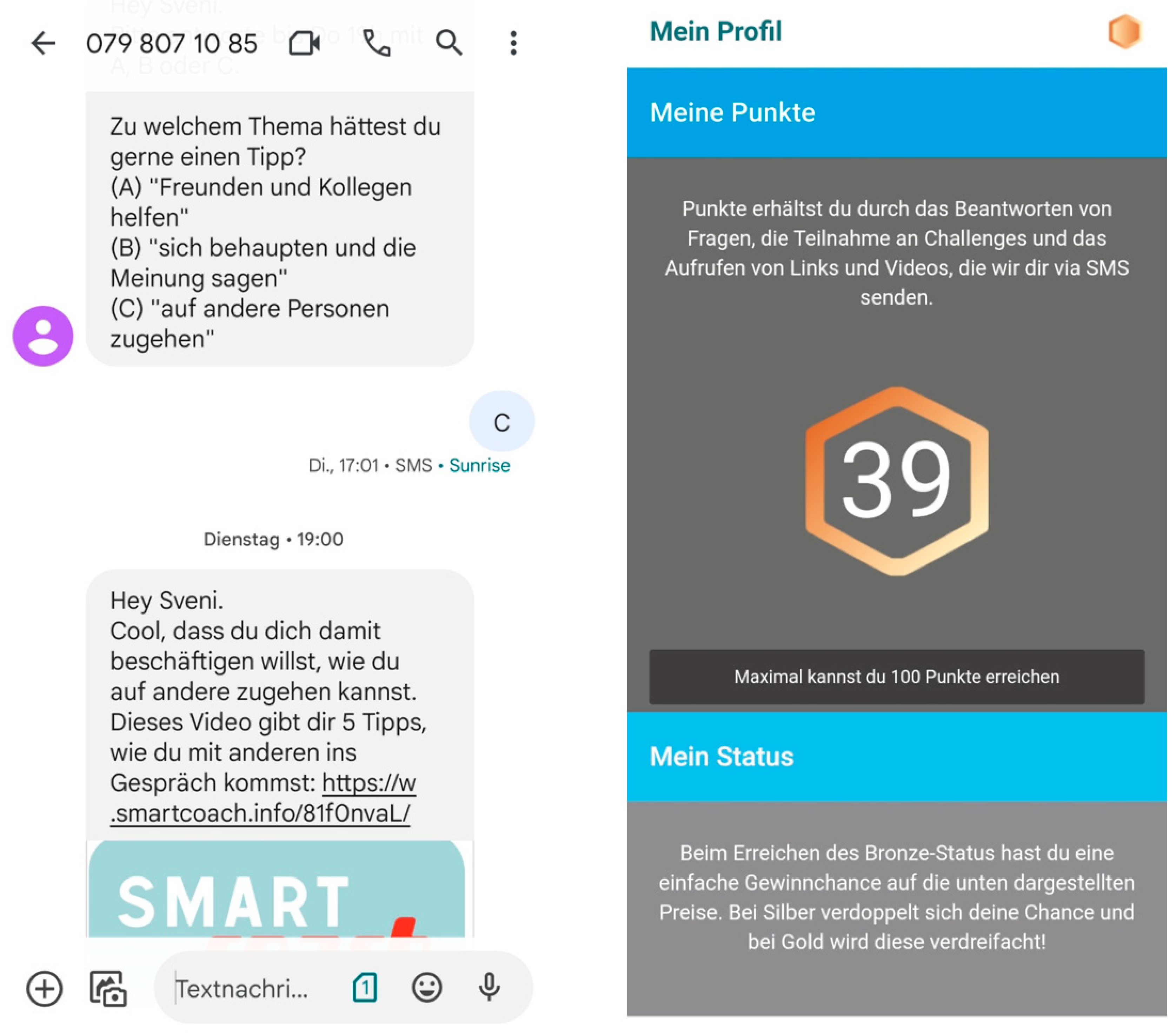
2.2. Intervention Program
2.3. Assessments and Outcomes
2.4. Statistical Analysis
3. Results
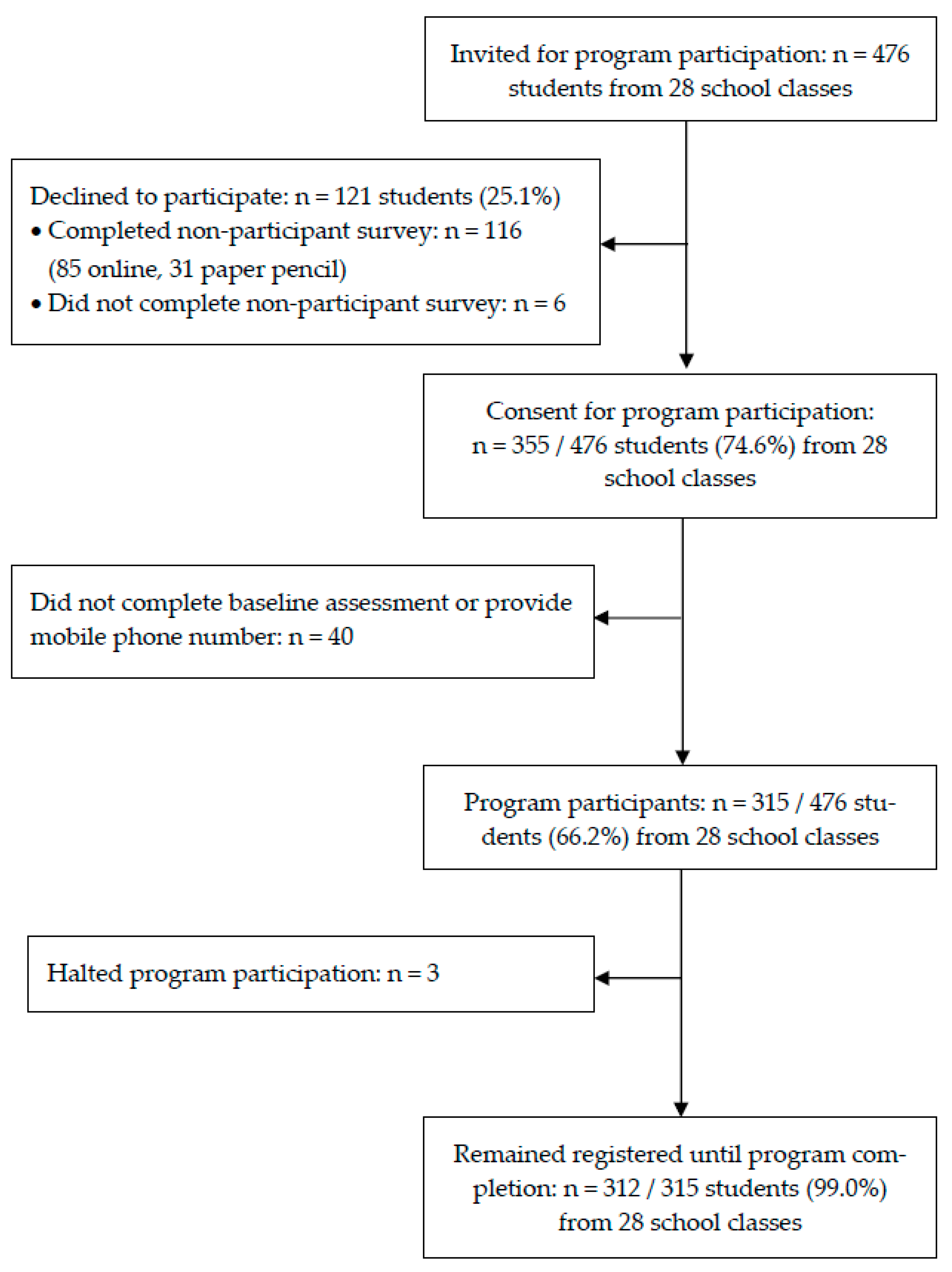
3.1. Program Participants
3.2. Predictors of Program Participation
3.3. Reasons for Not Participating in the Program
3.4. Predictors of Program Use
4. Discussion
4.1. Principal Results
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elgar, F.J.; Pfortner, T.K.; Moor, I.; De Clercq, B.; Stevens, G.W.; Currie, C. Socioeconomic inequalities in adolescent health 2002–2010: A time-series analysis of 34 countries participating in the Health Behaviour in School-aged Children study. Lancet 2015, 385, 2088–2095. [Google Scholar] [CrossRef] [Green Version]
- Hammond, M.A.; Khurana, A.; Stormshak, E.A. Adolescent measures of family socioeconomic status: Reliability, validity, and effects on substance use behaviors in adolescence and young adulthood. Prev. Med. Rep. 2021, 21, 101317. [Google Scholar] [CrossRef] [PubMed]
- Macintyre, A.K.; Torrens, C.; Campbell, P.; Maxwell, M.; Pollock, A.; Biggs, H.; Woodhouse, A.; Williams, J.M.; McLean, J. Socioeconomic inequalities and the equity impact of population-level interventions for adolescent health: An overview of systematic reviews. Public Health 2020, 180, 154–162. [Google Scholar] [CrossRef]
- Brown, T.; Platt, S.; Amos, A. Equity impact of interventions and policies to reduce smoking in youth: Systematic review. Tob. Control. 2014, 23, e98. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Klesges, L.M.; Dzewaltowski, D.A.; Estabrooks, P.A.; Vogt, T.M. Evaluating the impact of health promotion programs: Using the RE-AIM framework to form summary measures for decision making involving complex issues. Health Educ. Res. 2006, 21, 688–694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thyrian, J.R.; John, U. Population impact—Definition, calculation and its use in prevention science in the example of tobacco smoking reduction. Health Policy 2007, 82, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Schmid, H.; Rösch, C.; Süsstrunk, S.; Haug, S. Teilnahmebereitschaft von Jugendlichen an einem Rauchstoppprogramm über das Mobiltelefon [Willingness of adolescents to participate in a smokingcessation program using a mobile phone]. Präv Gesundheitsf 2015, 10, 62–67. [Google Scholar] [CrossRef]
- Thrul, J.; Stemmler, M.; Goecke, M.; Bühler, A. Are you in or out? Recruitment of adolescent smokers into a behavioral smoking cessation intervention. Addict. Behav. 2015, 45, 150–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haug, S.; Paz Castro, R.; Schaub, M.P. Erreichbarkeit Jugendlicher für ein Internet- und SMS-Programm zum Thema Alkohol [Accessibility of Adolescents for an Internet- and Text Message-Based Program Concerning Alcohol Abuse]. Sucht-Z. Wiss. Prax. 2015, 61, 357–365. [Google Scholar] [CrossRef] [Green Version]
- Haug, S.; Paz Castro, R. Erreichbarkeit Jugendlicher für ein mobiltelefonbasiertes Programm zur Suchtprävention durch die Förderung von Lebenskompetenzen [Accessibility of adolescents for a mobile phone-based life-skills training program for addiction prevention]. Sucht-Z. Wiss. Prax. 2018, 64, 129–139. [Google Scholar] [CrossRef]
- Thornton, L.; Brown, H.M.; Osman, B.; Stewart, C.; Whife, J.; Champion, K.E.; Gardner, L.A.; McBride, N.; Allsop, S.; Spring, B.; et al. Factors associated with adolescents’ engagement with a healthy lifestyles app. Procedia Comput. Sci. 2022, 206, 56–67. [Google Scholar] [CrossRef]
- Jakob, R.; Harperink, S.; Rudolf, A.M.; Fleisch, E.; Haug, S.; Mair, J.L.; Salamanca-Sanabria, A.; Kowatsch, T. Factors Influencing Adherence to mHealth Apps for Prevention or Management of Noncommunicable Diseases: Systematic Review. J. Med. Internet Res. 2022, 24, e35371. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, S.; Jerrott, S.; Clark, S.; Campbell, L.A.; Murphy, A.; Wozney, L. Text Message Interventions in Adolescent Mental Health and Addiction Services: Scoping Review. JMIR Ment. Health 2021, 8, e16508. [Google Scholar] [CrossRef] [PubMed]
- Garrido, S.; Millington, C.; Cheers, D.; Boydell, K.; Schubert, E.; Meade, T.; Nguyen, Q.V. What Works and What Doesn’t Work? A Systematic Review of Digital Mental Health Interventions for Depression and Anxiety in Young People. Front. Psychiatry 2019, 10, 759. [Google Scholar] [CrossRef]
- Kazemi, D.M.; Borsari, B.; Levine, M.J.; Li, S.; Lamberson, K.A.; Matta, L.A. A Systematic Review of the mHealth Interventions to Prevent Alcohol and Substance Abuse. J. Health Commun. 2017, 22, 413–432. [Google Scholar] [CrossRef] [Green Version]
- Calear, A.L.; Christensen, H.; Mackinnon, A.; Griffiths, K.M. Adherence to the MoodGYM program: Outcomes and predictors for an adolescent school-based population. J. Affect. Disord. 2013, 147, 338–344. [Google Scholar] [CrossRef]
- Paz Castro, R.; Haug, S.; Filler, A.; Kowatsch, T.; Schaub, M.P. Engagement within a Mobile Phone-Based Smoking Cessation Intervention for Adolescents and its Association with Participant Characteristics and Outcomes. J. Med. Internet Res. 2017, 19, e356. [Google Scholar] [CrossRef]
- Haug, S.; Paz Castro, R.; Wenger, A.; Schaub, M.P. A mobile phone–based life-skills training program for substance use prevention among adolescents: Cluster-randomized controlled trial. J. Med. Internet Res. Mhealth Uhealth 2021, 9, e26951. [Google Scholar] [CrossRef]
- Haug, S.; Paz Castro, R.; Wenger, A.; Schaub, M.P. Efficacy of a mobile phone-based life-skills training program for substance use prevention among adolescents: Study protocol of a cluster-randomised controlled trial. BMC Public Health 2018, 18, 1102. [Google Scholar] [CrossRef]
- Paz Castro, R.; Haug, S.; Wenger, A.; Schaub, M.P. Longer-Term Efficacy of a Digital Life-Skills Training for Substance Use Prevention. Am. J. Prev. Med. 2022, 63, 944–953. [Google Scholar] [CrossRef]
- Paz Castro, R.; Haug, S.; Debelak, R.; Kowatsch, T.; Jakob, R.; Schaub, M.P. Engagement with a mobile phone-based life-skills intervention for adolescents and its association with participant characteristics and outcomes: Tree-based analysis. J. Med. Internet Res. 2022, 24, e28638. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef] [PubMed]
- McAlister, A.L.; Perry, C.L.; Parcel, G.S. How Individuals, Environments, and Health Behaviour Interact: Social Cognitive Theory. In Health Behavior and Health Education: Theory, Research, and Practice; Glanz, K., Rimer, B.K., Viswanath, K., Eds.; Jossey-Bass: San Francisco, CA, USA, 2008. [Google Scholar]
- Botvin, G.J.; Griffin, C. Life skills training: Preventing substance misuse by enhancing individual and social competence. In Theory-Based Approaches to Substance Misuse and Abuse Prevention in School; Weichold, K., Giannotta, F., Eds.; Jossey-Bass: San Francisco, CA, USA, 2014; pp. 57–66. [Google Scholar]
- O’Neill, J.; Tabish, H.; Welch, V.; Petticrew, M.; Pottie, K.; Clarke, M.; Evans, T.; Pardo Pardo, J.; Waters, E.; White, H.; et al. Applying an equity lens to interventions: Using PROGRESS ensures consideration of socially stratifying factors to illuminate inequities in health. J. Clin. Epidemiol. 2014, 67, 56–64. [Google Scholar] [CrossRef]
- Sorensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; Consortium Health Literacy Project, E. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bollweg, T.M.; Okan, O.; Fretian, A.M.; Broder, J.; Domanska, O.M.; Jordan, S.; Bruland, D.; Pinheiro, P.; Bauer, U. Adapting the European Health Literacy Survey Questionnaire for Fourth-Grade Students in Germany: Validation and Psychometric Analysis. Health Lit. Res. Pract. 2020, 4, e144–e159. [Google Scholar] [CrossRef] [PubMed]
- Hanewinkel, R.; Hansen, J.; Neumann, C.; Petersen, F.L. Kinder- und Jugendgesundheit in Schulen: Erhebung Schuljahr 2020/21 [Child and Adolescent Health in Schools: Survey School Year 2020/21]; Institut für Therapie- und Gesundheitsforschung IFT-Nord: Kiel, Germany, 2021. [Google Scholar]
- Goodman, E.; Adler, N.E.; Kawachi, I.; Frazier, A.L.; Huang, B.; Colditz, G.A. Adolescents’ perceptions of social status: Development and evaluation of a new indicator. Pediatrics 2001, 108, e31. [Google Scholar] [CrossRef] [Green Version]
- Goodman, E.; Huang, B.; Schafer-Kalkhoff, T.; Adler, N.E. Perceived socioeconomic status: A new type of identity that influences adolescents’ self-rated health. J. Adolesc. Health 2007, 41, 479–487. [Google Scholar] [CrossRef] [Green Version]
- Lampert, T.; Hoebel, J.; Kuntz, B.; Müters, S.; Kroll, L.E. Messung des sozioökonomischen Status und des subjektiven sozialen Status in KiGGS Welle 2 [Measurement of socio-economic status and subjective social status in KiGGS Wave 2]. J. Health Monit. 2018, 3, 114–133. [Google Scholar]
- Jacobs Foundation. Juvenir Studie 4.0. Zuviel Stress—Zuviel Druck! Wie Schweizer Jugendliche Mit Stress und Leistungsdruck Umgehen [Too Much Stress—Too Much Pressure! How Swiss Adolescents Cope with Stress and Pressure]; Jacobs Foundation: Basel, Switzerland, 2015. [Google Scholar]
- Coroiu, A.; Meyer, A.; Gomez-Garibello, C.A.; Brahler, E.; Hessel, A.; Korner, A. Brief Form of the Interpersonal Competence Questionnaire (ICQ-15) Development and Preliminary Validation with a German Population Sample. Eur. J. Psychol. Assess. 2015, 31, 272–279. [Google Scholar] [CrossRef]
- Bush, K.; Kivlahan, D.R.; McDonell, M.B.; Fihn, S.D.; Bradley, K.A. The AUDIT alcohol consumption questions (AUDIT-C): An effective brief screening test for problem drinking. Ambulatory care quality improvement project (ACQUIP). Alcohol use disorders identification test. Arch. Intern. Med. 1998, 158, 1789–1795. [Google Scholar] [CrossRef] [Green Version]
- Rumpf, H.J.; Wohlert, T.; Freyer-Adam, J.; Grothues, J.; Bischof, G. Screening questionnaires for problem drinking in adolescents: Performance of AUDIT, AUDIT-C, CRAFFT and POSIT. Eur. Addict. Res. 2013, 19, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Marmet, S.; Archimi, A.; Windlin, B.; Delgrande Jordan, M. Substanzkonsum bei Schülerinnen und Schülern in der Schweiz im Jahr 2014 und Trend seit 1986—Resultate der Studie “Health Behaviour in School-aged Children” (HBSC) [Substance Use among Students in Switzerland in 2014 and Trend Since 1986—Results of the Study “Health Behaviour in School-Aged Children” (HBSC); Sucht Schweiz: Lausanne, Switzerland, 2015. [Google Scholar]
- Bates, D.; Machler, M.; Bolker, B.M.; Walker, S.C. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Haug, S.; Boumparis, N.; Wenger, A.; Paz Castro, R.; Schaub, M.P. Mobile App-Based Coaching for Alcohol Prevention among Adolescents: Pre-Post Study on the Acceptance and Effectiveness of the Program “MobileCoach Alcohol”. Int. J. Environ. Res. Public Health 2023, 20, 3263. [Google Scholar] [CrossRef]
- Achilles, M.R.; Anderson, M.; Li, S.H.; Subotic-Kerry, M.; Parker, B.; O’Dea, B. Adherence to e-mental health among youth: Considerations for intervention development and research design. Digit. Health 2020, 6, 2055207620926064. [Google Scholar] [CrossRef]
- Perski, O.; Blandford, A.; West, R.; Michie, S. Conceptualising engagement with digital behaviour change interventions: A systematic review using principles from critical interpretive synthesis. Transl. Behav. Med. 2017, 7, 254–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Level/Characteristic | Variable Category | Percentage of Program Participants (n = 470) | Mean Number of Interactions with Program (n = 315) |
|---|---|---|---|
| Individual | |||
| Sex | Male | 61.4 (223) | 13.6 (137) |
| Female | 72.1 (247) | 17.7 (178) | |
| Age in years | 14 | 60.8 (125) | 14.9 (76) |
| 15 | 61.3 (181) | 17.2 (111) | |
| 16 and older | 78.0 (164) | 15.4 (128) | |
| Socioeconomic status | Low | 68.9 (132 a) | 15.7 (91) |
| Medium | 68.6 (226) | 16.0 (155) | |
| High | 62.7 (110) | 15.8 (69) | |
| Health literacy | Low | 66.7 (147) | 16.7 (98) |
| Medium | 69.4 (144) | 15.5 (100) | |
| High | 65.4 179) | 15.6 (117) | |
| Migration background | No | 72.2 (176) | 19.1 (127) |
| Yes | 63.9 (294) | 13.8 (188) | |
| Origin from a non-German-speaking country | No Yes | 69.4 (209 b) 65.2 (256) | 19.0 (145 c) 13.2 (167) |
| At-risk alcohol use | No | 15.9 (254) | |
| Yes | 15.7 (61) | ||
| Nicotine/Tobacco smoking | No | 16.1 (232) | |
| Yes | 15.2 (83) | ||
| Cannabisuse | No | 16.5 (277) | |
| Yes | 11.3 (38) | ||
| Perceived stress | Low | 12.0 (56) | |
| Medium | 18.6 (106) | ||
| High | 15.4 (153) | ||
| Social skills | Low | 17.6 (88) | |
| Medium | 14.1 (97) | ||
| High | 16.1 (130) | ||
| School class | |||
| Educational level | Secondary | 58.9 (316) | 14.8 (186) |
| Upper secondary | 83.8 (154) | 17.5 (129) | |
| Time of recruitment | 8 to 9 a.m. | 63.0 (165) | 15.6 (104) |
| 10 to 12 a.m. | 70.6 (228) | 15.4 (161) | |
| 1 to 3 p.m. | 64.9 (77) | 18.3 (50) | |
| Duration of workshop | Up to 20 min | 54.3 (151) | 15.3 (82) |
| 21–50 min | 64.4 (132) | 14.3 (85) | |
| Over 50 min | 79.1 (187) | 17.1 (148) | |
| Number of students present | 10 to 15 | 60.3 (136) | 13.0 (82) |
| 16 to 19 | 72.4 (181) | 17.9 (131) | |
| 20 and more | 66.7 (153) | 15.7 (102) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haug, S.; Boumparis, N.; Wenger, A.; Schaub, M.P.; Kiselev, N. Predictors of Youth Accessibility for a Mobile Phone-Based Life Skills Training Program for Addiction Prevention. Int. J. Environ. Res. Public Health 2023, 20, 6379. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20146379
Haug S, Boumparis N, Wenger A, Schaub MP, Kiselev N. Predictors of Youth Accessibility for a Mobile Phone-Based Life Skills Training Program for Addiction Prevention. International Journal of Environmental Research and Public Health. 2023; 20(14):6379. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20146379
Chicago/Turabian StyleHaug, Severin, Nikolaos Boumparis, Andreas Wenger, Michael Patrick Schaub, and Nikolai Kiselev. 2023. "Predictors of Youth Accessibility for a Mobile Phone-Based Life Skills Training Program for Addiction Prevention" International Journal of Environmental Research and Public Health 20, no. 14: 6379. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20146379