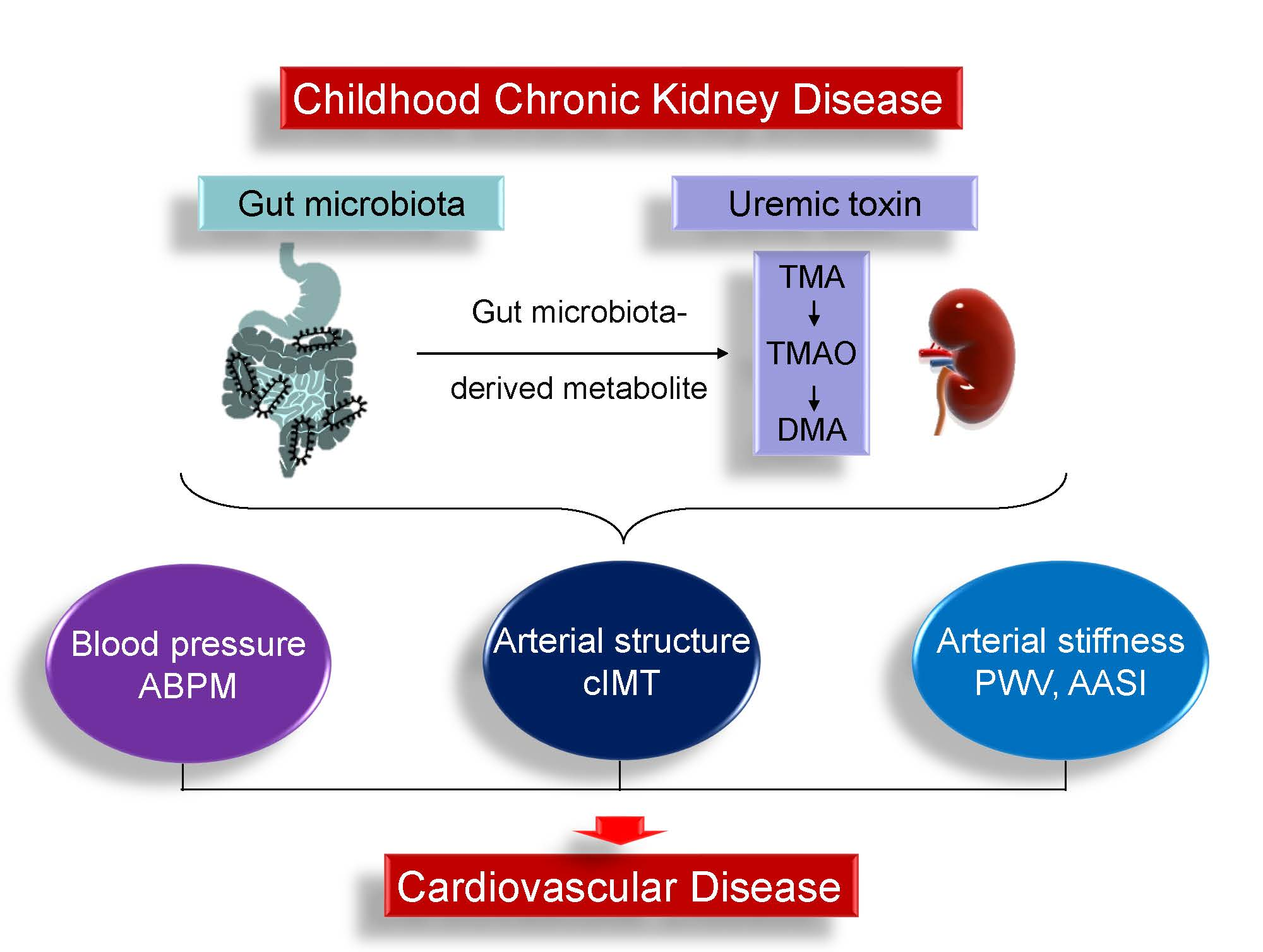
Gut Microbiota-Dependent Trimethylamine N-Oxide Pathway Associated with Cardiovascular Risk in Children with Early-Stage Chronic Kidney Disease

 ,
, 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Biochemical Analysis
2.3. Office BP and 24-Hour ABPM
2.4. Carotid Ultrasonography
2.5. Liquid Chromatography–Mass Spectrometry (LC–MS) Analysis
2.6. Analysis of Gut-Microbiota Composition
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mitsnefes, M.M. Cardiovascular disease in children with chronic kidney disease. J. Am. Soc. Nephrol. 2012, 23, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Urbina, E.M.; Williams, R.V.; Alpert, B.S.; Collins, R.T.; Daniels, S.R.; Hayman, L.; Jacobson, M.; Mahoney, L.; Mietus-Snyder, M.; Rocchini, A.; et al. American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee of the Council on Cardiovascular Disease in the Young. American Heart Association Atherosclerosis, Hypertension, and Obesity in Youth Committee of the Council on Cardiovascular Disease in the Young. Noninvasive assessment of subclinical atherosclerosis in children and adolescents: Recommendations for standard assessment for clinical research: A scientific statement from the American Heart Association. Hypertension 2009, 54, 919–950. [Google Scholar] [PubMed]
- Kuo, H.C.; Hsu, C.N.; Huang, C.F.; Lo, M.H.; Chien, S.J.; Tain, Y.L. Urinary arginine methylation index associated with ambulatory blood pressure abnormalities in children with chronic kidney disease. J. Am. Soc. Hypertens. 2012, 6, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Mitsnefes, M.; Flynn, J.; Cohn, S.; Samuels, J.; Blydt-Hansen, T.; Saland, J.; Kimball, T.; Furth, S.; Warady, B.; CKiD Study Group. Masked hypertension associates with left ventricular hypertrophy in children with CKD. J. Am. Soc. Nephrol. 2010, 21, 137–144. [Google Scholar] [CrossRef] [PubMed]
- Brady, T.M.; Schneider, M.F.; Flynn, J.T.; Cox, C.; Samuels, J.; Saland, J.; White, C.T.; Furth, S.; Warady, B.A.; Mitsnefes, M. Carotid intima-media thickness in children with CKD: Results from the CKiD study. Clin. J. Am. Soc. Nephrol. 2012, 7, 1930–1937. [Google Scholar] [CrossRef] [PubMed]
- Lin, I.C.; Hsu, C.N.; Lo, M.H.; Chien, S.J.; Tain, Y.L. Low urinary citrulline/arginine ratio associated with blood pressure abnormalities and arterial stiffness in childhood chronic kidney disease. J. Am. Soc. Hypertens. 2016, 10, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Taal, M.W. Arterial stiffness in chronic kidney disease: An update. Curr. Opin. Nephrol. Hypertens. 2014, 23, 169–173. [Google Scholar] [CrossRef] [PubMed]
- Ohishi, M.; Tatara, Y.; Ito, N.; Takeya, Y.; Onishi, M.; Maekawa, Y.; Kato, N.; Kamide, K.; Rakugi, H. The combination of chronic kidney disease and increased arterial stiffness is a predictor for stroke and cardiovascular disease in hypertensive patients. Hypertens. Res. 2011, 34, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Jovanovich, A.; Isakova, T.; Stubbs, J. Microbiome and Cardiovascular Disease in CKD. Clin. J. Am. Soc. Nephrol. 2018, 13, 1598–1604. [Google Scholar] [CrossRef] [PubMed]
- Meijers, B.; Jouret, F.; Evenepoel, P. Linking gut microbiota to cardiovascular disease and hypertension: Lessons from chronic kidney disease. Pharmacol. Res. 2018, 133, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.; Kitai, T.; Hazen, S.L. Gut Microbiota in Cardiovascular Health and Disease. Circ. Res. 2017, 120, 1183–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, T.; Santisteban, M.M.; Rodriguez, V.; Li, E.; Ahmari, N.; Carvajal, J.M.; Zadeh, M.; Gong, M.; Qi, Y.; Zubcevic, J.; et al. Gut dysbiosis is linked to hypertension. Hypertension 2015, 65, 1331–1340. [Google Scholar] [CrossRef] [PubMed]
- Velasquez, M.T.; Ramezani, A.; Manal, A.; Raj, D.S. Trimethylamine N-Oxide: The Good, the Bad and the Unknown. Toxins (Basel). 2016, 8, E326. [Google Scholar] [CrossRef] [PubMed]
- Schiattarella, G.G.; Sannino, A.; Toscano, E.; Giugliano, G.; Gargiulo, G.; Franzone, A.; Trimarco, B.; Esposito, G.; Perrino, C. Gut microbe-generated metabolite trimethylamine-N-oxide as cardiovascular risk biomarker: A systematic review and dose-response meta-analysis. Eur. Heart J. 2017, 38, 2948–2956. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.; Wang, Z.; Kennedy, D.J.; Wu, Y.; Buffa, J.A.; Agatisa-Boyle, B.; Li, X.S.; Levison, B.S.; Hazen, S.L. Gut microbiota-dependent trimethylamine N-oxide (TMAO) pathway contributes to both development of renal insufficiency and mortality risk in chronic kidney disease. Circ. Res. 2015, 116, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Dumas, M.E.; Kinross, J.; Nicholson, J.K. Metabolic phenotyping and systems biology approaches to understanding metabolic syndrome and fatty liver disease. Gastroenterology 2014, 146, 46–62. [Google Scholar] [CrossRef] [PubMed]
- Stubbs, J.R.; House, J.A.; Ocque, A.J.; Zhang, S.; Johnson, C.; Kimber, C.; Schmidt, K.; Gupta, A.; Wetmore, J.B.; Nolin, T.D.; et al. Serum Trimethylamine-N-Oxide is Elevated in CKD and Correlates with Coronary Atherosclerosis Burden. J. Am. Soc. Nephrol. 2016, 27, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. Suppl. 2013, 3, 1–150. [Google Scholar]
- Schwartz, G.J.; Muñoz, A.; Schneider, M.F.; Mak, R.H.; Kaskel, F.; Warady, B.A.; Furth, S.L. New equations to estimate GFR in children with CKD. J. Am. Soc. Nephrol. 2009, 20, 629–637. [Google Scholar] [CrossRef] [PubMed]
- Renkema, K.Y.; Winyard, P.J.; Skovorodkin, I.N.; Levtchenko, E.; Hindryckx, A.; Jeanpierre, C.; Weber, S.; Salomon, R.; Antignac, C.; Vainio, S.; et al. Novel perspectives for investigating congenital anomalies of the kidney and urinary tract (CAKUT). Nephrol. Dial. Transplant. 2011, 26, 3843–3851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wuhl, E.; Witte, K.; Soergelm, M.; Mehls, O.; Schaefer, F. German Working Group on Pediatric Hypertension. Distribution of 24-h ambulatory blood pressure in children: Normalized reference values and role of body dimensions. J. Hypertens. 2002, 20, 1995–2007. [Google Scholar] [CrossRef] [PubMed]
- Kollias, A.; Stergiou, G.S.; Dolan, E.; O’Brien, E. Ambulatory arterial stiffness index: A systematic review and meta-analysis. Atherosclerosis 2012, 224, 291–301. [Google Scholar] [CrossRef] [PubMed]
- DiRienzo, D.B. Effect of probiotics on biomarkers of cardiovascular disease: Implications for heart-healthy diets. Nutr. Rev. 2014, 72, 18–29. [Google Scholar] [CrossRef] [PubMed]
- Chou, H.H.; Lin, C.Y.; Chiou, Y.H.; Tain, Y.L.; Wang, Y.F.; Wang, H.H.; Chiou, Y.Y. Clinical characteristics and prevalence of complications of chronic kidney disease in children: The Taiwan Pediatric Renal Collaborative study. Pediatr. Nephrol. 2016, 31, 1113–1120. [Google Scholar] [CrossRef] [PubMed]
- Feig, D.I.; Kang, D.H.; Nakagawa, T.; Mazzali, M.; Johnson, R.J. Uric acid and hypertension. Curr. Hypertens. Rep. 2006, 8, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama, H.; Shiina, K.; Vlachopoulos, C.; Iwasaki, Y.; Matsumoto, C.; Kimura, K.; Fujii, M.; Chikamori, T.; Yamashina, A. Involvement of Arterial Stiffness and Inflammation in Hyperuricemia-Related Development of Hypertension. Hypertension 2018, 72, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.K.; Chen, C.C.; Liu, P.Y.; Panyod, S.; Liao, B.Y.; Chen, P.C.; Kao, H.L.; Kuo, H.C.; Kuo, C.H.; Chiu, T.H.T.; et al. Identification of TMAO-producer phenotype and host-diet-gut dysbiosis by carnitine challenge test in human and germ-free mice. Gut 2018. pii: Gutjnl-2018-317155. [Google Scholar] [CrossRef] [PubMed]
- Kelly, T.N.; Bazzano, L.A.; Ajami, N.J.; He, H.; Zhao, J.; Petrosino, J.F.; Correa, A.; He, J. Gut microbiome associates with lifetime cardiovascular disease risk profile among Bogalusa Heart Study participants. Circ. Res. 2016, 119, 956–964. [Google Scholar] [CrossRef] [PubMed]
- Cani, P.D.; de Vos, W.M. Next-Generation Beneficial Microbes: The Case of Akkermansia muciniphila. Front. Microbiol. 2017, 8, 1765. [Google Scholar] [CrossRef] [PubMed]
- Wühl, E.; van Stralen, K.J.; Verrina, E.; Bjerre, A.; Wanner, C.; Heaf, J.G.; Zurriaga, O.; Hoitsma, A.; Niaudet, P.; Palsson, R.; et al. Timing and outcome of renal replacement therapy in patients with congenital malformations of the kidney and urinary tract. Clin. J. Am. Soc. Nephrol. 2013, 8, 67–74. [Google Scholar]
- Tsai, T.C.; Chen, Y.C.; Lo, C.W.; Wang, W.S.; Lo, S.S.; Tang, G.J.; Thien, P.F. Incidence and renal survival of ESRD in the young Taiwanese population. Clin. J. Am. Soc. Nephrol. 2014, 9, 302–309. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| CKD Stage | G1 | G2–G3 |
| N = 60 | N = 26 | |
| Gender: M:F | 35:25 | 19:7 |
| Underlying disease: CAKUT: non-CAKUT | 33:27 | 22:4 * |
| Age, years | 9.5 (5.2–13) | 13.7 (7.9–16.2) * |
| Body height, percentile | 50 (25–75) | 25 (15–75) |
| Body weight, percentile | 50 (15–85) | 25 (15–78) |
| Systolic blood pressure, mmHg | 106 (99–115) | 119 (108–127) * |
| Diastolic blood pressure, mmHg | 68 (61–77) | 70 (63–79) |
| Body mass index, kg·m−2 | 17 (15.6–20.8) | 17.3 (15.7–23.5) |
| Hypertension (by office blood pressure) | 18 (30%) | 11 (42%) |
| Blood urea nitrogen, mg/dL | 11 (10–13) | 17 (13–20) * |
| Creatinine, mg/dL | 0.48 (0.39–0.53) | 0.89 (0.65–1.18) * |
| eGFR, mL·min−1·1.73 m−2 | 113 (103–129) | 79 (54–85) * |
| Urine total protein-to-creatinine ratio, mg/g | 64 (38–262) | 57 (35–213) |
| Hemoglobin, g/dL | 13.4 (12.8–14.1) | 14 (12.5–15.4) |
| Total cholesterol, mg/dL | 163 (142–197) | 171 (147–182) |
| LDL, mg/dL | 90 (68–111) | 88 (77–100) |
| Triglyceride, mg/dL | 67 (52–101) | 70 (52–103) |
| Glucose, mg/dL | 86 (82–91) | 89 (85–93) |
| Uric acid, mg/dL | 4.8 (3.9–5.7) | 6.6 (5.9–7.6) * |
| Sodium, mEq/L | 141 (140–142) | 141 (140–142) |
| Potassium, mEq/L | 4.4 (4.2–4.6) | 4.4 (4.2–4.6) |
| Calcium, mg/dL | 9.6 (9.2–9.9) | 9.8 (9.5–10) |
| Phosphate, mg/dL | 4.9 (4.7–5.3) | 4.8 (4.1–5.1) |
| CKD Stage | G1 | G2–G3 |
| 24 h ABPM | N = 35 | N = 19 |
| Abnormal ABPM profile (with any of the following abnormalities) Average 24 h BP > 95th percentile Average daytime BP > 95th percentile Average nighttime > 95th percentile BP load ≥ 25% Nocturnal decrease of BP < 10% | 20 (57%) 3 (9%) 3 (9%) 7 (20%) 14 (40%) 14 (40%) | 15 (79%) 3 (16%) 4 (21%) 6 (32%) 14 (74%) * 8 (42%) |
| Cardiovascular assessment | ||
| cIMT, mm | 0.4 (0.3–0.4) | 0.3 (0.3–0.4) |
| PWV, m/s | 3.8 (3.4–4.2) | 4.1 (3.7–4.9) * |
| AASI | 0.36 (0.24–0.44) | 0.38 (0.32–0.41) |
| CKD Stage | G1 | G2–G3 |
| N = 60 | N = 26 | |
| Urine level, ng/mg Cr | ||
| DMA | 234 (160–300) | 177 (137–228) * |
| TMA | 8 (5.5–14.8) | 6.9 (3.8–11.2) |
| TMAO | 344 (200–853) | 209 (155–412) * |
| Abundance of Genus | cIMT | PWV | AASI | DMA | TMA | TMAO | ||||||
| r | p | r | p | r | p | r | p | r | p | r | p | |
| Bacteroides | −0.007 | 0.956 | 0.086 | 0.518 | −0.052 | 0.709 | 0.072 | 0.508 | −0.001 | 0.991 | 0.024 | 0.827 |
| Blautia | −0.139 | 0.293 | 0.055 | 0.68 | 0.011 | 0.939 | 0.107 | 0.325 | −0.05 | 0.646 | 0.307 | 0.004 * |
| Faecalibacterium | −0.234 | 0.074 | 0.014 | 0.916 | −0.066 | 0.635 | 0.047 | 0.665 | −0.079 | 0.468 | 0.072 | 0.508 |
| Bifidobacterium | −0.01 | 0.94 | −0.013 | 0.919 | 0.044 | 0.752 | 0.227 | 0.036 * | −0.025 | 0.817 | 0.36 | 0.001 * |
| Oscillospira | 0.186 | 0.159 | 0.029 | 0.829 | 0.264 | 0.054 | −0.038 | 0.725 | 0.111 | 0.311 | −0.031 | 0.776 |
| Parabacteroides | 0.112 | 0.4 | 0.052 | 0.693 | −0.003 | 0.981 | 0.053 | 0.625 | −0.144 | 0.185 | 0.03 | 0.785 |
| Clostridium | −0.011 | 0.936 | 0.196 | 0.137 | 0.044 | 0.75 | −0.065 | 0.554 | −0.038 | 0.728 | 0.13 | 0.232 |
| Ruminococcus | 0.227 | 0.084 | 0.107 | 0.418 | 0.266 | 0.052 | 0.002 | 0.985 | 0.034 | 0.757 | 0.094 | 0.388 |
| Akkermansia | 0.018 | 0.89 | 0.076 | 0.565 | 0.007 | 0.959 | −0.097 | 0.372 | −0.023 | 0.832 | −0.071 | 0.519 |
| Collinsella | −0.75 | 0.573 | 0.239 | 0.068 | 0.081 | 0.559 | 0.112 | 0.307 | −0.128 | 0.24 | 0.254 | 0.018 * |
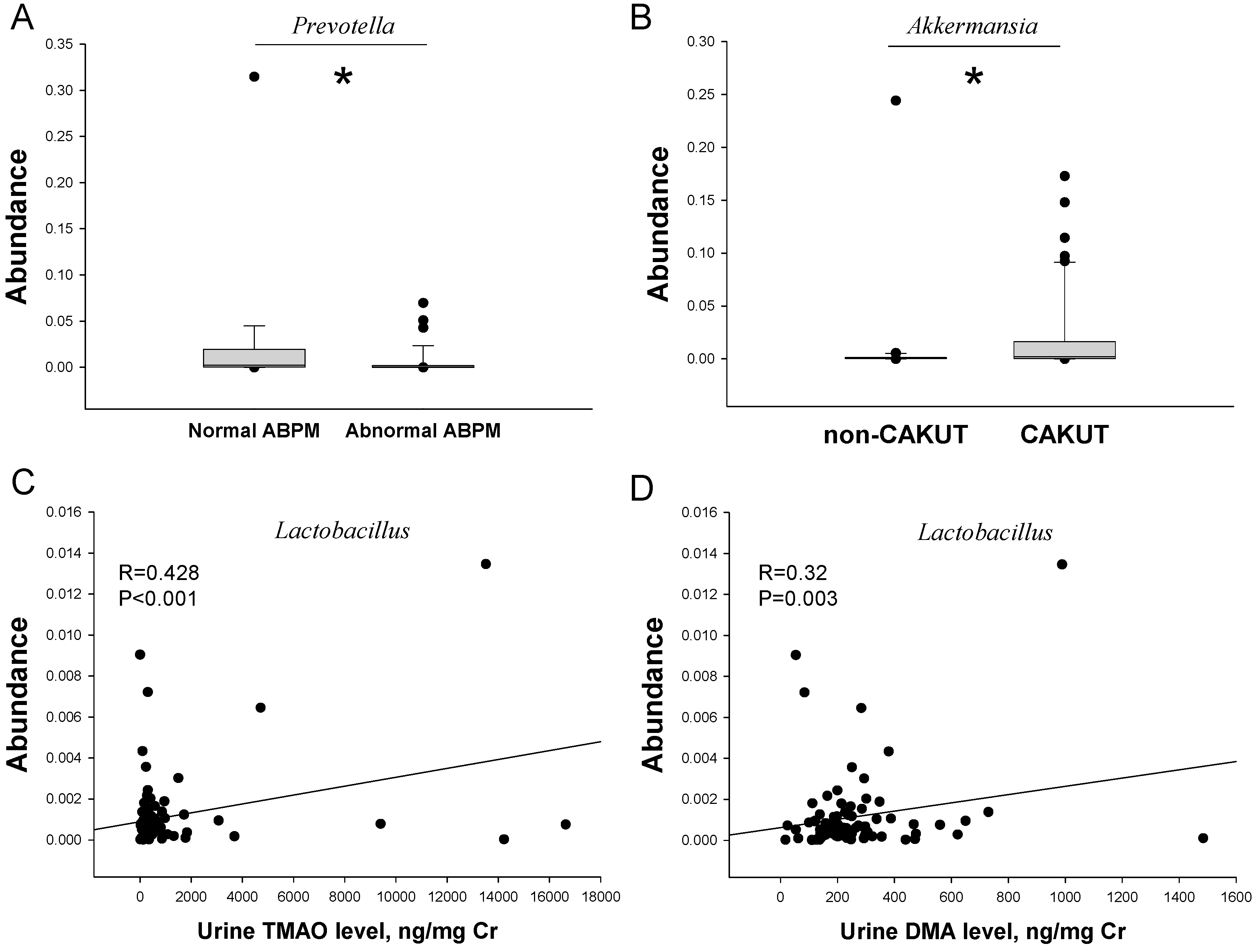
| Lactobacillus | −0.284 | 0.029 * | 0.066 | 0.622 | −0.151 | 0.274 | 0.32 | 0.003 * | 0.145 | 0.181 | 0.428 | <0.001 * |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, C.-N.; Lu, P.-C.; Lo, M.-H.; Lin, I.-C.; Chang-Chien, G.-P.; Lin, S.; Tain, Y.-L. Gut Microbiota-Dependent Trimethylamine N-Oxide Pathway Associated with Cardiovascular Risk in Children with Early-Stage Chronic Kidney Disease. Int. J. Mol. Sci. 2018, 19, 3699. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19123699
Hsu C-N, Lu P-C, Lo M-H, Lin I-C, Chang-Chien G-P, Lin S, Tain Y-L. Gut Microbiota-Dependent Trimethylamine N-Oxide Pathway Associated with Cardiovascular Risk in Children with Early-Stage Chronic Kidney Disease. International Journal of Molecular Sciences. 2018; 19(12):3699. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19123699
Chicago/Turabian StyleHsu, Chien-Ning, Pei-Chen Lu, Mao-Hung Lo, I-Chun Lin, Guo-Ping Chang-Chien, Sufan Lin, and You-Lin Tain. 2018. "Gut Microbiota-Dependent Trimethylamine N-Oxide Pathway Associated with Cardiovascular Risk in Children with Early-Stage Chronic Kidney Disease" International Journal of Molecular Sciences 19, no. 12: 3699. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms19123699