5hmC Level Predicts Biochemical Failure Following Radical Prostatectomy in Prostate Cancer Patients with ERG Negative Tumors

 , and
, and
Abstract
:1. Introduction
2. Results
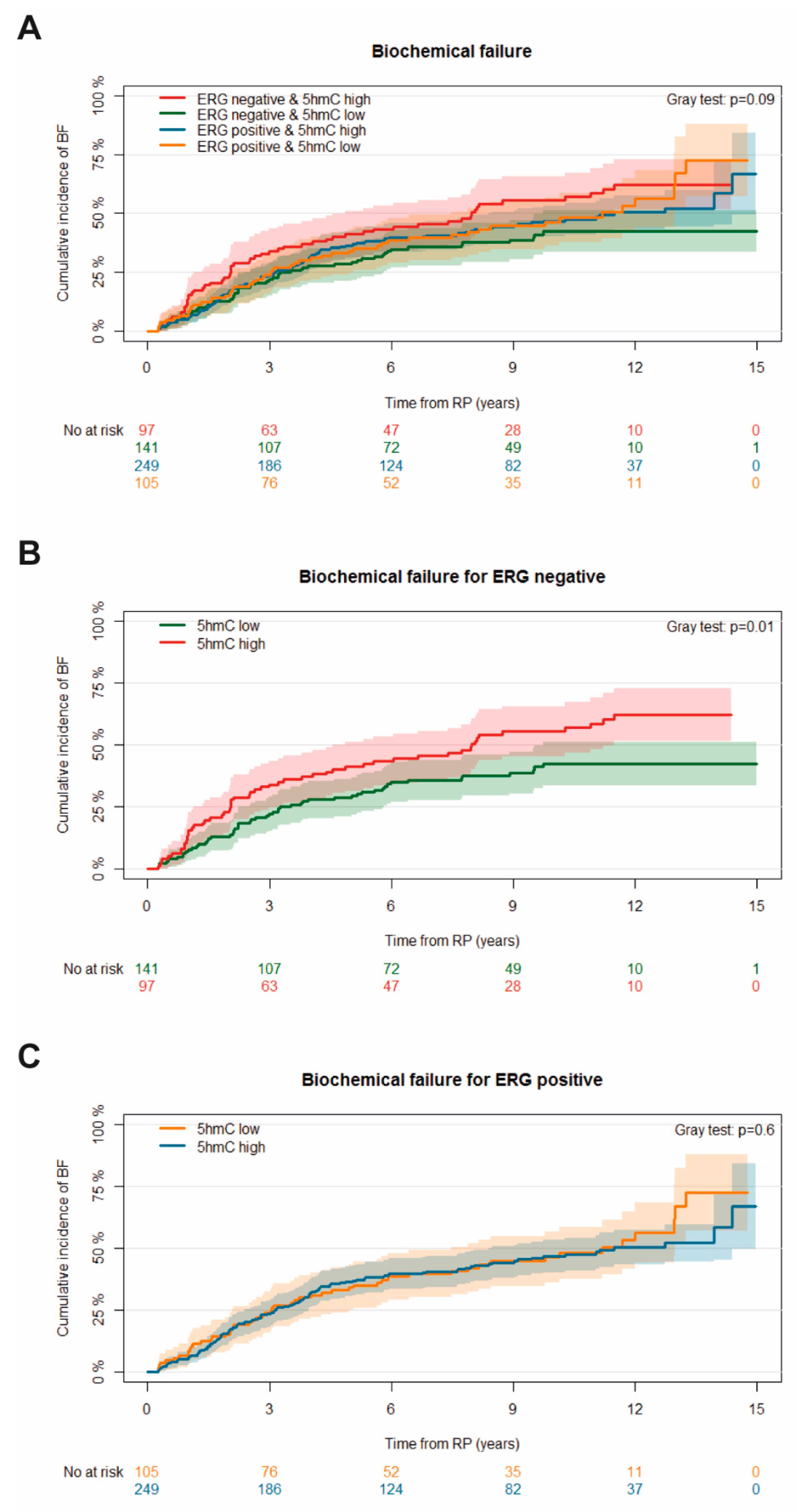
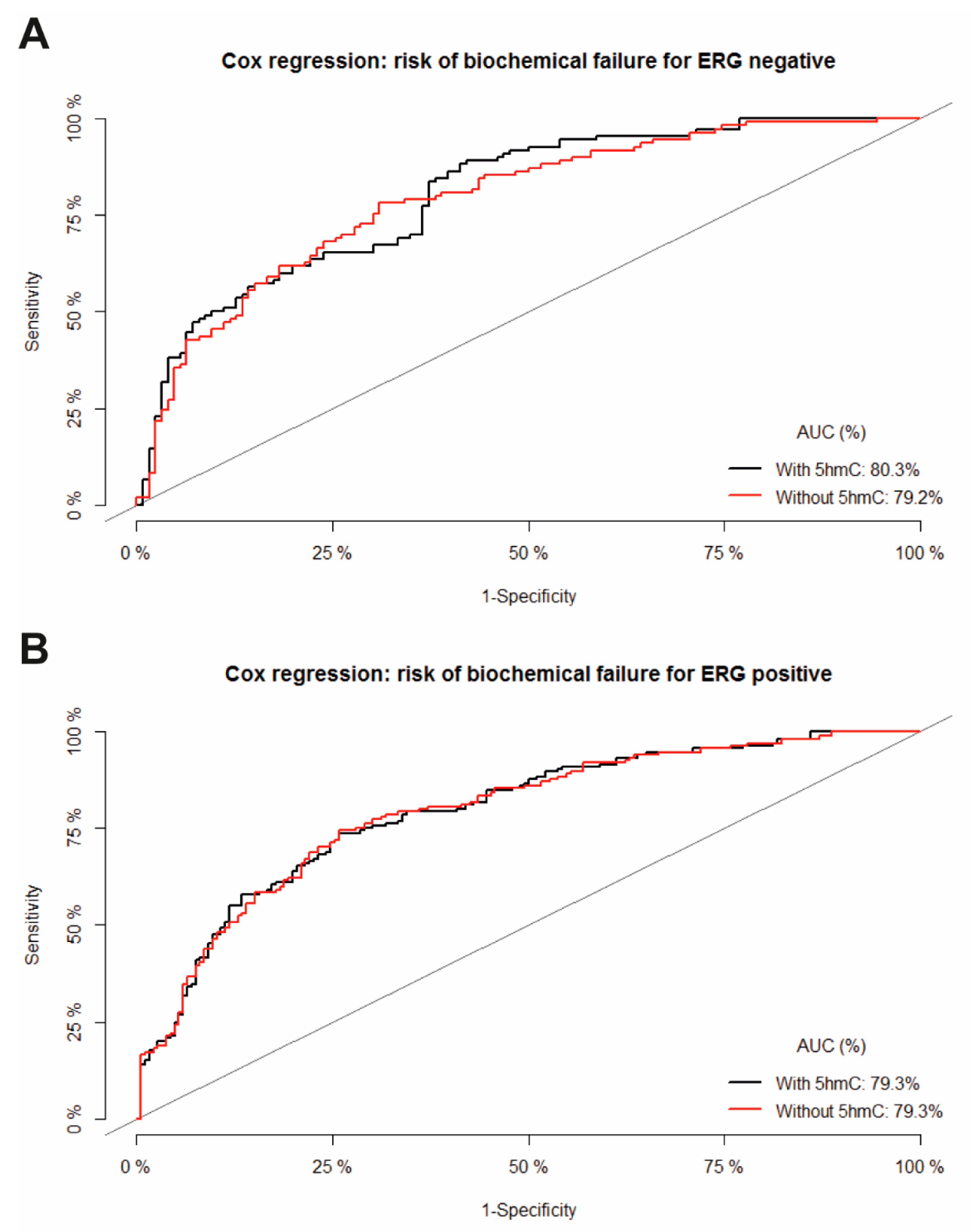
Biochemical Failure
3. Discussion
4. Materials and Methods
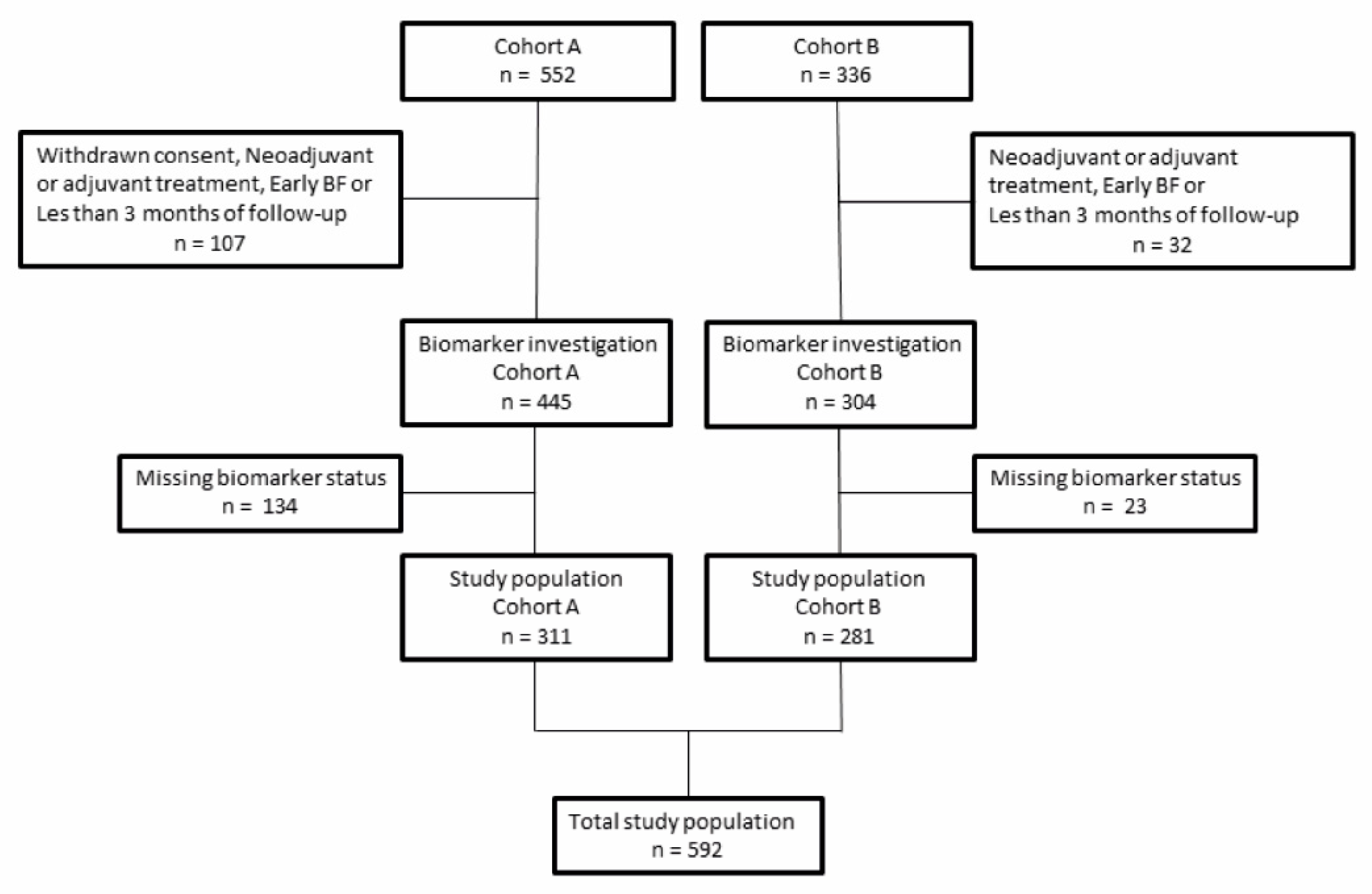
4.1. Patient Cohort
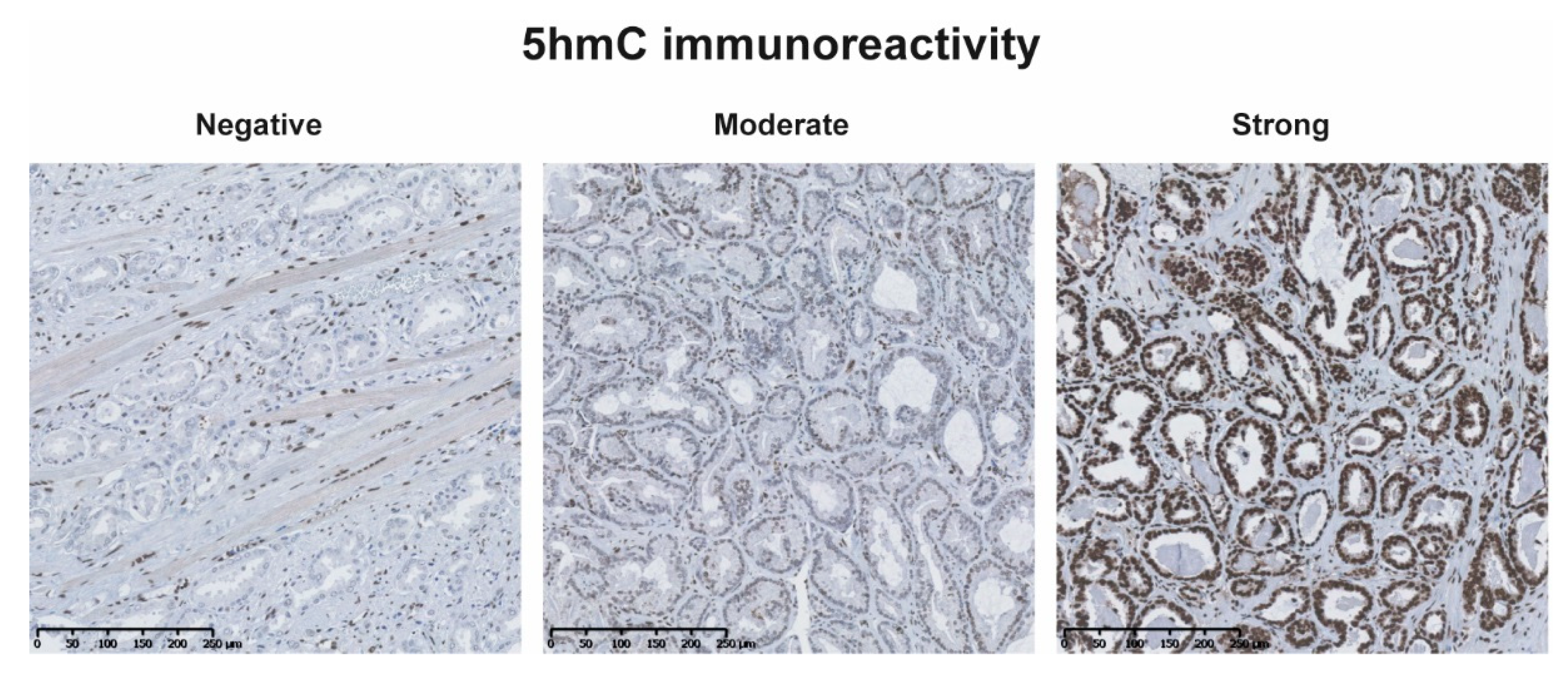
4.2. Immunohistochemistry
4.3. Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cooperberg, M.R.; Hilton, J.F.; Carroll, P.R. The CAPRA-S Score: A Straightforward Tool for Improved Prediction of Outcomes after Radical Prostatectomy. Cancer 2011, 117, 5039–5046. [Google Scholar] [CrossRef] [PubMed]
- Cooperberg, M.R.; Pasta, D.J.; Elkin, E.P.; Litwin, M.S.; Latini, D.M.; Du Chane, J.; Carroll, P.R. The University of California, San Francisco Cancer of the Prostate Risk Assessment Score: A Straightforward and Reliable Preoperative Predictor of Disease Recurrence after Radical Prostatectomy. J. Urol. 2005, 173, 1938–1942. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical Outcome After Radical Prostatectomy, External Beam Radiation Therapy, or Interstitial Radiation Therapy for Clinically Localized Prostate Cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Klotz, L.; Vesprini, D.; Sethukavalan, P.; Jethava, V.; Zhang, L.; Jain, S.; Yamamoto, T.; Mamedov, A.; Loblaw, A. Long-Term Follow-up of a Large Active Surveillance Cohort of Patients with Prostate Cancer. J. Clin. Oncol. 2015, 33, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Tosoian, J.J.; Mamawala, M.; Epstein, J.I.; Landis, P.; Wolf, S.; Trock, B.J.; Carter, H.B. Intermediate and Longer-Term Outcomes From a Prospective Active-Surveillance Program for Favorable-Risk Prostate Cancer. J. Clin. Oncol. 2015, 33, 3379–3385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiffmann, J.; Wenzel, P.; Salomon, G.; Budäus, L.; Schlomm, T.; Minner, S.; Wittmer, C.; Kraft, S.; Krech, T.; Steurer, S.; et al. Heterogeneity in D’Amico Classification-Based Low-Risk Prostate Cancer: Differences in Upgrading and Upstaging According to Active Surveillance Eligibility. Urol. Oncol. 2015, 33, 329.e13–329.e19. [Google Scholar] [CrossRef] [PubMed]
- St. John, J.; Powell, K.; Conley-Lacomb, M.K.; Chinni, S.R. TMPRSS2-ERG Fusion Gene Expression in Prostate Tumor Cells and Its Clinical and Biological Significance in Prostate Cancer Progression. J. Cancer Sci. Ther. 2012, 4, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.P.; Barros-Silva, J.D.; Ersvaer, E.; Kildal, W.; Hveem, T.S.; Pradhan, M.; Vieira, J.; Teixeira, M.R.; Danielsen, H.E. Prostate Cancer Prognosis Defined by the Combined Analysis of 8q, PTEN and ERG. Transl. Oncol. 2016, 9, 575–582. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Llodrà, S.; Juanpere, N.; de Muga, S.; Lorenzo, M.; Gil, J.; Font-Tello, A.; Agell, L.; Albero-González, R.; Segalés, L.; Merino, J.; et al. ERG Overexpression plus SLC45A3 (Prostein) and PTEN Expression Loss: Strong Association of the Triple Hit Phenotype with an Aggressive Pathway of Prostate Cancer Progression. Oncotarget 2017, 8, 74106–74118. [Google Scholar] [CrossRef] [PubMed]
- Hägglöf, C.; Hammarsten, P.; Strömvall, K.; Egevad, L.; Josefsson, A.; Stattin, P.; Granfors, T.; Bergh, A. TMPRSS2-ERG Expression Predicts Prostate Cancer Survival and Associates with Stromal Biomarkers. PLoS ONE 2014, 9, e86824. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Kelly, T.K.; Jones, P.A. Epigenetics in Cancer. Carcinogenesis 2010, 31, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Shi, X.; Guo, L.; Li, Y.; Luo, M.; He, J.; Chen, Z.; Shi, X.; Guo, L.; Li, Y.; et al. Decreased 5-Hydroxymethylcytosine Levels Correlate with Cancer Progression and Poor Survival: A Systematic Review and Meta-Analysis. Oncotarget 2015, 8, 1944–1952. [Google Scholar] [CrossRef] [PubMed]
- Branco, M.R.; Ficz, G.; Reik, W. Uncovering the Role of 5-Hydroxymethylcytosine in the Epigenome. Nat. Rev. Genet. 2011, 13, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Kamdar, S.N.; Ho, L.T.; Kron, K.J.; Isserlin, R.; Van Der Kwast, T.; Zlotta, A.R.; Fleshner, N.E.; Bader, G.; Bapat, B. Dynamic Interplay between Locus-Specific DNA Methylation and Hydroxymethylation Regulates Distinct Biological Pathways in Prostate Carcinogenesis. Clin. Epigenet. 2016, 8, 32. [Google Scholar] [CrossRef] [PubMed]
- Strand, S.H.; Hoyer, S.; Lynnerup, A.-S.; Haldrup, C.; Storebjerg, T.M.; Borre, M.; Orntoft, T.F.; Sorensen, K.D. High Levels of 5-Hydroxymethylcytosine (5hmC) Is an Adverse Predictor of Biochemical Recurrence after Prostatectomy in ERG-Negative Prostate Cancer. Clin. Epigenet. 2015, 7, 111. [Google Scholar] [CrossRef] [PubMed]
- Storebjerg, T.M.; Strand, S.H.; Høyer, S.; Lynnerup, A.-S.; Borre, M.; Ørntoft, T.F.; Sørensen, K.D. Dysregulation and Prognostic Potential of 5-Methylcytosine (5mC), 5-Hydroxymethylcytosine (5hmC), 5-Formylcytosine (5fC), and 5-Carboxylcytosine (5caC) Levels in Prostate Cancer. Clin. Epigenet. 2018, 10, 105. [Google Scholar] [CrossRef] [PubMed]
- Røder, M.A.; Berg, K.D.; Gruschy, L.; Brasso, K.; Iversen, P. First Danish Single-Institution Experience with Radical Prostatectomy: Biochemical Outcome in 1200 Consecutive Patients. Prostate Cancer 2011, 2011, 236357. [Google Scholar] [CrossRef] [PubMed]
- Røder, M.A.; Brasso, K.; Christensen, I.J.; Johansen, J.; Langkilde, N.C.; Hvarness, H.; Carlsson, S.; Jakobsen, H.; Borre, M.; Iversen, P. Survival after Radical Prostatectomy for Clinically Localised Prostate Cancer: A Population-Based Study. BJU Int. 2014, 113, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Barbieri, C.E.; Tomlins, S.A. Reprint of: The Prostate Cancer Genome: Perspectives and Potential. Urol. Oncol. Semin. Orig. Investig. 2015, 33, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Dobosy, J.R.; Roberts, J.L.W.; Fu, V.X.; Jarrard, D.F. The Expanding Role of Epigenetics in the Development, Diagnosis and Treatment of Prostate Cancer and Benign Prostatic Hyperplasia. J. Urol. 2007, 177, 822–831. [Google Scholar] [CrossRef] [PubMed]
- Chiam, K.; Ricciardelli, C.; Bianco-Miotto, T. Epigenetic Biomarkers in Prostate Cancer: Current and Future Uses. Cancer Lett. 2014, 342, 248–256. [Google Scholar] [CrossRef] [PubMed]
- Hao, X.; Luo, H.; Krawczyk, M.; Wei, W.; Wang, W.; Wang, J.; Flagg, K.; Hou, J.; Zhang, H.; Yi, S.; et al. DNA Methylation Markers for Diagnosis and Prognosis of Common Cancers. Proc. Natl. Acad. Sci. USA 2017, 114, 7414–7419. [Google Scholar] [CrossRef] [PubMed]
- Haldrup, C.; Mundbjerg, K.; Vestergaard, E.M.; Lamy, P.; Wild, P.; Schulz, W.A.; Arsov, C.; Visakorpi, T.; Borre, M.; Høyer, S.; et al. DNA Methylation Signatures for Prediction of Biochemical Recurrence after Radical Prostatectomy of Clinically Localized Prostate Cancer. J. Clin. Oncol. 2013, 31, 3250–3258. [Google Scholar] [CrossRef] [PubMed]
- Brothman, A.R.; Swanson, G.; Maxwell, T.M.; Cui, J.; Murphy, K.J.; Herrick, J.; Speights, V.O.; Isaac, J.; Rohr, L.R. Global Hypomethylation Is Common in Prostate Cancer Cells: A Quantitative Predictor for Clinical Outcome? Cancer Genet. Cytogenet. 2005, 156, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Haffner, M.C.; Chaux, A.; Meeker, A.K.; Esopi, D.M.; Gerber, J.; Pellakuru, L.G.; Toubaji, A.; Argani, P.; Iacobuzio-Donahue, C.; Nelson, W.G.; et al. Global 5-Hydroxymethylcytosine Content Is Significantly Reduced in Tissue Stem/Progenitor Cell Compartments and in Human Cancers. Oncotarget 2011, 2, 627–637. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Liu, Y.; Bai, F.; Zhang, J.-Y.; Ma, S.-H.; Liu, J.; Xu, Z.-D.; Zhu, H.-G.; Ling, Z.-Q.; Ye, D.; et al. Tumor Development Is Associated with Decrease of TET Gene Expression and 5-Methylcytosine Hydroxylation. Oncogene 2013, 32, 663–669. [Google Scholar] [CrossRef] [PubMed]
- Smeets, E.; Lynch, A.G.; Prekovic, S.; Van den Broeck, T.; Moris, L.; Helsen, C.; Joniau, S.; Claessens, F.; Massie, C.E. The Role of TET-Mediated DNA Hydroxymethylation in Prostate Cancer. Mol. Cell. Endocrinol. 2018, 462, 41–55. [Google Scholar] [CrossRef] [PubMed]
- Kroeze, L.I.; Aslanyan, M.G.; van Rooij, A.; Koorenhof-Scheele, T.N.; Massop, M.; Carell, T.; Boezeman, J.B.; Marie, J.-P.; Halkes, C.J.M.; de Witte, T.; et al. Characterization of Acute Myeloid Leukemia Based on Levels of Global Hydroxymethylation. Blood 2014, 124, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Tsai, K.-W.; Li, G.-C.; Chen, C.-H.; Yeh, M.-H.; Huang, J.-S.; Tseng, H.-H.; Fu, T.-Y.; Liou, H.-H.; Pan, H.-W.; Huang, S.-F.; et al. Reduction of Global 5-Hydroxymethylcytosine Is a Poor Prognostic Factor in Breast Cancer Patients, Especially for an ER/PR-Negative Subtype. Breast Cancer Res. Treat. 2015, 153, 219–234. [Google Scholar] [CrossRef] [PubMed]
- Saldanha, G.; Joshi, K.; Lawes, K.; Bamford, M.; Moosa, F.; Teo, K.W.; Pringle, J.H. 5-Hydroxymethylcytosine Is an Independent Predictor of Survival in Malignant Melanoma. Mod. Pathol. 2017, 30, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Liao, Y.; Gu, J.; Wu, Y.; Long, X.; Ge, D.I.; Xu, J.; Ding, J. Low Level of 5-Hydroxymethylcytosine Predicts Poor Prognosis in Non-Small Cell Lung Cancer. Oncol. Lett. 2016, 11, 3753–3760. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.; Zhang, J.; Guo, Z.; Ma, Q.; Xu, Z.; Zhou, Y.; Xu, Z.; Li, Z.; Liu, Y.; Ye, X.; et al. Loss of 5-Hydroxymethylcytosine Is Linked to Gene Body Hypermethylation in Kidney Cancer. Cell Res. 2016, 26, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.-Y.; Han, C.-S.; Li, P.-L.; Zhang, X.-C. 5-Hydroxymethylcytosine Expression Is Associated with Poor Survival in Cervical Squamous Cell Carcinoma. Jpn. J. Clin. Oncol. 2016, 46, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.D.; Vainer, B.; Thomsen, F.B.; Røder, M.A.; Gerds, T.A.; Toft, B.G.; Brasso, K.; Iversen, P. ERG Protein Expression in Diagnostic Specimens Is Associated with Increased Risk of Progression during Active Surveillance for Prostate Cancer. Eur. Urol. 2014, 66, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, A.; Graff, R.E.; Bauer, S.R.; Pitt, M.J.; Lis, R.T.; Stack, E.C.; Martin, N.E.; Kunz, L.; Penney, K.L.; Ligon, A.H.; et al. The TMPRSS2:ERG Rearrangement, ERG Expression, and Prostate Cancer Outcomes: A Cohort Study and Meta-Analysis. Cancer Epidemiol. Biomark. Prev. 2012, 21, 1497–1509. [Google Scholar] [CrossRef] [PubMed]
- Huber, F.; Montani, M.; Sulser, T.; Jaggi, R.; Wild, P.; Moch, H.; Gevensleben, H.; Schmid, M.; Wyder, S.; Kristiansen, G. Comprehensive Validation of Published Immunohistochemical Prognostic Biomarkers of Prostate Cancer—What Has Gone Wrong? A Blueprint for the Way Forward in Biomarker Studies. Br. J. Cancer 2014, 112, 140–148. [Google Scholar] [CrossRef] [PubMed]
- Kirkegaard, T.; Edwards, J.; Tovey, S.; McGlynn, L.M.; Krishna, S.N.; Mukherjee, R.; Tam, L.; Munro, A.F.; Dunne, B.; Bartlett, J.M.S. Observer Variation in Immunohistochemical Analysis of Protein Expression, Time for a Change? Histopathology 2006, 48, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Allsbrook, W.C.; Amin, M.B.; Egevad, L.L.; ISUP Grading Committee. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef] [PubMed]
- Svensson, M.A.; Perner, S.; Ohlson, A.-L.; Day, J.R.; Groskopf, J.; Kirsten, R.; Sollie, T.; Helenius, G.; Andersson, S.-O.; Demichelis, F.; et al. A Comparative Study of ERG Status Assessment on DNA, MRNA, and Protein Levels Using Unique Samples from a Swedish Biopsy Cohort. Appl. Immunohistochem. Mol. Morphol. 2014, 22, 136–141. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Tomlins, S.A.; Mudaliar, K.M.; Chiu, Y.-L.; Esgueva, R.; Mehra, R.; Suleman, K.; Varambally, S.; Brenner, J.C.; Macdonald, T.; et al. Antibody-Based Detection of ERG Rearrangement–Positive Prostate Cancer 1,2. Neoplasia 2010, 12, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.D.; Brasso, K.; Thomsen, F.B.; Røder, M.A.; Holten-Rossing, H.; Toft, B.G.; Iversen, P.; Vainer, B. ERG Protein Expression over Time: From Diagnostic Biopsies to Radical Prostatectomy Specimens in Clinically Localised Prostate Cancer. J. Clin. Pathol. 2015, 68, 788–794. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, G.; Røder, M.A.; Berg, K.D.; Elversang, J.; Iglesias-Gato, D.; Moreira, J.; Toft, B.G.; Brasso, K. Predictive Value of Combined Analysis of Pro-NPY and ERG in Localized Prostate Cancer. APMIS 2018, 126, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M.; Smith, T.L. A Note on Quantifying Follow-up in Studies of Failure Time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]
- Gray, R.J. A Class of K-Sample Tests for Comparing the Cumulative Incidence of a Competing Risk. Ann. Stat. 1988, 16, 1141–1154. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristic of the Study Cohort | Study Population n = 592 | 5hmC Low n = 246 | 5hmC High n = 346 | p-Value |
|---|---|---|---|---|
| Age at baseline, years, median (IQR) | 63.2 (59.5–67.0) | 64.1 (60.3–67.7) | 62.5 (59.0–66.6) | 0.003 * |
| PSA, µg/L, median (IQR) | 10.6 (7.1–16.0) | 10.9 (7.2–16.1) | 10.6 (7.1–16.0) | 0.7 * |
| Clinical T-stage | 0.03 ** | |||
| cT1 | 161 (27.2%) | 53 (21.5%) | 108 (31.3%) | |
| cT2 | 423 (71.6%) | 190 (77.2%) | 233 (67.5%) | |
| cT3 | 7 (1.2%) | 3 (1.2%) | 4 (1.2%) | |
| Missing | 1 | 0 | 1 | |
| Biopsy Gleason score | 0.05 ** | |||
| ≤6 | 361 (69.4%) | 133 (63.6%) | 228 (73.3%) | |
| 7 | 125 (24.0%) | 58 (27.8%) | 67 (21.5%) | |
| 8–10 | 34 (6.5%) | 18 (8.6%) | 16 (5.1%) | |
| Missing | 72 | 37 | 35 | |
| Pathological T-stage | 0.5 ** | |||
| pT2 | 392 (66.3%) | 167 (67.9%) | 225 (65.2%) | |
| pT3-4 | 199 (33.7%) | 79 (32.1%) | 120 (34.8%) | |
| Missing | 1 | 0 | 1 | |
| Radical prostatectomy Gleason score | 0.001 ** | |||
| ≤6 | 202 (34.1%) | 64 (26.0%) | 138 (39.9%) | |
| 7 | 316 (53.4%) | 141 (57.3%) | 175 (50.6%) | |
| 8–10 | 74 (12.5%) | 41 (16.7%) | 33 (9.5%) | |
| Margin status | 0.8 ** | |||
| R− | 329 (56.0%) | 135 (55.3%) | 194 (56.6%) | |
| R+ | 258 (44.0%) | 109 (44.7%) | 149 (43.4%) | |
| Missing | 5 | 2 | 3 | |
| ERG | <0.0001 ** | |||
| Negative | 238 (40.2%) | 141 (57.3%) | 97 (28.0%) | |
| Positive | 354 (59.8%) | 105 (42.7%) | 249 (72.0%) |
| A: For patients with ERG negative tumors | ||||
| For Patients with ERG Negative Tumors | Univariate analysis | Multivariate analysis | ||
| HR (95% CI) | p-value | HR (95% CI) | p-value | |
| 5hmC | ||||
| Low | REF | REF | ||
| High | 1.6 (1.1–2.4) | 0.01 | 1.8 (1.2–2.7) | 0.003 |
| Age at RP | ||||
| For 5-yr difference | 1.0 (0.9–1.2) | 0.7 | 1.0 (0.9–1.2) | 0.8 |
| PSA | ||||
| For 2-fold difference | 1.7 (1.4–2.2) | <0.0001 | 1.4 (1.1–1.8) | 0.002 |
| Pathological T-stage | ||||
| pT2 | REF | REF | ||
| pT3-4 | 3.1 (2.1–4.5) | <0.0001 | 1.9 (1.2–2.8) | 0.004 |
| RP Gleason score | ||||
| ≤6 | REF | REF | ||
| 7 | 2.5 (1.4–4.5) | 0.003 | 2.2 (1.2–4.0) | 0.01 |
| 8–10 | 5.4 (2.8–10.2) | <0.0001 | 4.6 (2.3–9.0) | <0.0001 |
| Margin status | ||||
| R− | REF | REF | ||
| R+ | 2.1 (1.5–3.1) | <0.0001 | 1.5 (1.0–2.3) | 0.04 |
| B: For patients with ERG positive tumors | ||||
| For Patients with ERG Positive Tumors | Univariate analysis | Multivariate analysis | ||
| HR (95% CI) | P-value | HR (95% CI) | P-value | |
| 5hmC | ||||
| Low | REF | REF | ||
| High | 0.9 (0.7–1.3) | 0.6 | 1.0 (0.7–1.4) | 0.9 |
| Age at RP | ||||
| For 5-yr difference | 1.1 (0.9–1.3) | 0.3 | 0.9 (0.8–1.1) | 0.5 |
| PSA | ||||
| For 2-fold difference | 1.7 (1.4–2.1) | <0.0001 | 1.4 (1.2–1.7) | 0.0002 |
| Pathological T-stage | ||||
| pT2 | REF | REF | ||
| pT3-4 | 3.0 (2.2–4.1) | <0.0001 | 1.9 (1.3–2.7) | 0.0003 |
| RP Gleason score | ||||
| ≤6 | REF | REF | ||
| 7 | 2.9 (2.0–4.2) | <0.0001 | 2.0 (1.4–3.0) | 0.0004 |
| 8–10 | 5.7 (3.3–9.7) | <0.0001 | 3.6 (2.0–6.4) | <0.0001 |
| Margin status | ||||
| R− | REF | REF | ||
| R+ | 2.4 (1.7–3.3) | <0.0001 | 1.6 (1.1–2.2) | 0.007 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kristensen, G.; Strand, S.H.; Røder, M.A.; Berg, K.D.; Toft, B.G.; Høyer, S.; Borre, M.; Sørensen, K.D.; Brasso, K. 5hmC Level Predicts Biochemical Failure Following Radical Prostatectomy in Prostate Cancer Patients with ERG Negative Tumors. Int. J. Mol. Sci. 2019, 20, 1025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20051025
Kristensen G, Strand SH, Røder MA, Berg KD, Toft BG, Høyer S, Borre M, Sørensen KD, Brasso K. 5hmC Level Predicts Biochemical Failure Following Radical Prostatectomy in Prostate Cancer Patients with ERG Negative Tumors. International Journal of Molecular Sciences. 2019; 20(5):1025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20051025
Chicago/Turabian StyleKristensen, Gitte, Siri H. Strand, Martin Andreas Røder, Kasper Drimer Berg, Birgitte Grønkær Toft, Søren Høyer, Michael Borre, Karina Dalsgaard Sørensen, and Klaus Brasso. 2019. "5hmC Level Predicts Biochemical Failure Following Radical Prostatectomy in Prostate Cancer Patients with ERG Negative Tumors" International Journal of Molecular Sciences 20, no. 5: 1025. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20051025