Proteomic Biomarkers of Retinal Inflammation in Diabetic Retinopathy

1
Department of Cellular Biology and Anatomy, Augusta University, Augusta, GA 30912, USA
2
Medical College of Georgia, Augusta University, Augusta, GA 30912, USA
3
Center for Biotechnology and Genomic Medicine, Augusta University, Augusta, GA 30912, USA
4
Department of Population Health Sciences, Augusta University, Augusta, GA 30912, USA
5
Culver Vision Discovery Institute, Augusta University, Augusta, GA 30912, USA
6
Department of Ophthalmology, Augusta University, Augusta, GA 30912, USA
*
Author to whom correspondence should be addressed.
Int. J. Mol. Sci. 2019, 20(19), 4755; https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20194755
Submission received: 30 August 2019
/
Revised: 23 September 2019
/
Accepted: 24 September 2019
/
Published: 25 September 2019
(This article belongs to the Special Issue Retinal Degeneration: From Pathophysiology to Therapeutic Approaches)
Abstract
:Diabetic retinopathy (DR), a sight-threatening neurovasculopathy, is the leading cause of irreversible blindness in the developed world. DR arises as the result of prolonged hyperglycemia and is characterized by leaky retinal vasculature, retinal ischemia, retinal inflammation, angiogenesis, and neovascularization. The number of DR patients is growing with an increase in the elderly population, and therapeutic approaches are limited, therefore, new therapies to prevent retinal injury and enhance repair are a critical unmet need. Besides vascular endothelial growth factor (VEGF)-induced vascular proliferation, several other mechanisms are important in the pathogenesis of diabetic retinopathy, including vascular inflammation. Thus, combining anti-VEGF therapy with other new therapies targeting these pathophysiological pathways of DR may further optimize treatment outcomes. Technological advancements have allowed for high-throughput proteomic studies examining biofluids such as aqueous humor, vitreous humor, tear, and serum. Many DR biomarkers have been identified, especially proteins involved in retinal inflammatory processes. This review attempts to summarize the proteomic biomarkers of DR-associated retinal inflammation identified over the last several years.
1. Introduction
Diabetic retinopathy (DR) is the leading cause of irreversible blindness in the developed world and contributes to the majority of blindness in working-age adults, affecting more than four million individuals [1,2,3]. The prevalence of this sight-threatening neurovasculopathy is expected to increase with longer life expectancies and the growing elderly population [1,4,5]. DR is the most common microvascular complication arising from diabetes, and diabetic patients have a twenty-five-fold greater risk of blindness than non-diabetic individuals. Since DR arises as a result of extended exposure to hyperglycemia, it occurs in almost all type I diabetics and the majority of type II diabetics, thereby nearly tripling their treatment costs [6,7,8,9].
DR is characterized by leaky retinal vasculature, retinal ischemia, angiogenesis, and retinal inflammation. These pathologies manifest clinically as cotton-wool spots, exudates, small tortuous veins, aneurysms, and areas of hemorrhage, which may result in reduced acuity, loss of color sensitivity, and problematic night vision [1,10,11]. While the underlying cause of DR is prolonged hyperglycemia, still much is unknown about the precise pathogenesis of the disease [12,13]. Inflammation triggered by increased glycolytic metabolites has been well established in individuals with DR, and retinal inflammation leads to vascular permeabilization and loss of the blood-retinal barrier [1,5,13,14,15,16,17,18,19]. As a result, macular edema (diabetic macular edema (DME)) may develop, reducing central vision [1,5,14,15,16,17]. Retinal ischemia may also induce the growth of new, small, abnormal blood vessels into the central portion of the posterior segment, a condition known as proliferative diabetic retinopathy (PDR) [1,5,10,11,16,17]. As these vessels grow and attach to the surface of the vitreous body, they easily rupture and may cause retinal detachment, leading to vision loss [1,16,17,20]. These two forms of DR may occur separately or concurrently [21,22].
Diagnosis of DR is made based on clinical features observed during comprehensive eye examination [23]. Current recommendations include initial screening exams for type I diabetic patients three to five years after disease onset and, for type II diabetic patients, at the time of diagnosis, with regular follow-up with an ophthalmologist experienced in treating DR [23]. Risk factors for DR include the duration of diabetes as well as modifiable risk factors such as poor glycemic control, hypertension, dyslipidemia, and obesity [24,25,26,27,28]. Managing blood glucose, lipid, and A1c levels are the primary means of reducing the risk of developing DR among diabetic patients, and have been shown to reduce severity upon its incidence [29,30,31].
Currently, treatment strategies for DR are limited to more advanced stages of the disease when retinal damage becomes symptomatic [11]. Standard of care for most patients includes intravitreal injections of corticosteroids or anti-vascular endothelial growth factor (VEGF) agents, such as bevacizumab, ranibizumab, pegaptanib, or aflibercept, with therapeutic efficacy dependent on a patients’ baseline visual acuity [2,3,5,11,15,32,33,34,35,36,37,38,39,40]. In advanced cases, laser photocoagulation may be used to reduce the amount of blood vessels entering the posterior segment of the eye [2,39]. While laser photocoagulation does control the effects of neovascularization and some macular edema, it typically achieves its effect through destructive processes. Anti-VEGF therapy is far less destructive, but is primarily aimed at limiting disease progression through repeated intra-ocular injections, which are not without adverse effects [35,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55]. Therefore, new therapies to prevent retinal injury and enhance repair remain a critical unmet need.
In diabetes, elevated blood glucose levels alter critical homeostatic mechanisms, resulting in changes to the proteomic microenvironment crucial to proper cellular function. Several of these changes, including altered expression of inflammatory mediators and leukocyte adhesion molecules, have been correlated to the progression of DR. A better understanding of the precise proteomic changes that occur during DR development and progression could provide new insight into disease pathophysiology and may lead to the development of novel treatment options.
2. Use of Proteomics Technologies for Biomarker Discovery in Diabetic Retinopathy
The last several decades have seen a rapid advancement in methodology, engineering, and equipment design, and it is now possible to generate large amounts of data using small amount of samples. Remarkable advances in mass spectrometry (MS) techniques are allowing for deeper analysis and the identification of more proteins at faster speeds [7,22,56]. In addition, MS technology is useful for identification of post-translational modifications and variants of proteins [16,22,57,58,59,60]. The use of high throughput proteomics has expanded to include ophthalmic investigations. Numerous studies have been conducted on samples from DR patients including tear, cornea, aqueous humor (AH), lens, vitreous humor (VH), retina, and serum [61] using proteomic approaches such as two-dimensional difference gel electrophoresis (2D-DIGE) coupled with MS [10,20,39,62,63,64,65], SDS-PAGE coupled with MS [16,66], liquid chromatography coupled with tandem MS (LC-MS/MS) [3,4,13,15,17,33,35,56,67,68,69,70,71,72], and bead-based multiplex immunoassays [73,74]. Several well-characterized biomarkers of DR have been identified, including complement component C3, intercellular adhesion molecule 1 (ICAM-1), interleukin-6 (IL-6), serum amyloid A protein (SAA), vascular endothelial growth factor (VEGF), etc. [4,16,66,72,75,76,77,78,79,80,81], as shown in Table 1.
3. Proteomic Changes in Biofluids Associated with Diabetic Retinopathy
Increased vascular permeability and elevated levels of inflammatory proteins in serum and ocular biofluids (VH, AH, and tear) are the primary characteristics of retinal inflammation associated with DR [11,15,95,96,97,98,99,100,101]. While AH and tear are distally located and interact indirectly with the retina, both serum and VH have direct contact with the retina. On the other hand, AH and VH sample collection requires highly invasive procedures, whereas serum and tear samples can be collected using relatively non-invasive methods. The circulatory proteins in these biofluids can not only provide clues about DR pathogenesis, but can also serve as biomarkers, with diagnostic or prognostic potential [102,103,104]. Furthermore, proteomic changes in biofluids could offer a means of more personalized medicine. For example, plasma kallikrein, a central component of the pro-inflammatory kallikrein kinin system, has been shown to be elevated in the VH of DR patients [15]. The kallikrein kinin system works independently of VEGF regulation, and standard anti-VEGF intravitreal injection might not be effective in these subjects [11,15]. Several studies examining proteomic changes associated with DR using biofluids are discussed below and are summarized in Figure 1.
3.1. Serum
Diabetes is a systemic disease therefore, biomarkers found in circulation may not only be indicators of the disease, but also of the progression of specific diabetic complications. As DR is primarily a microvascular complication, proteomic changes involved in DR pathology may be evident in the systemic circulation. Serum is one of the most accessible and easily obtained biofluids, allowing for sample collection from both DR patients and healthy controls. The ease of sample collection relative to other relevant fluids like VH or AH provides sufficient power to detect potential proteomic differences in patients with various clinical stages of DR including non-proliferative DR (NPDR), PDR, and DME [105].
A number of serum proteins have been found to be altered in DR, including α-2-antiplasmin (SERPINF2), C-reactive protein (CRP), C-C motif chemokine 5 (CCL5), intercellular adhesion molecule 1 (ICAM-1), interleukin-6 (IL-6), pentraxin-related protein 3 (PTX3), pigment epithelium-derived factor (PEDF), plasminogen activator inhibitor 1 (PAI-1), serum amyloid A (SAA), soluble endothelial molecule-1 (sE-selectin), stromal cell-derived factor 1α (CXCL12), tumor necrosis factor α (TNF-α), vascular adhesion molecule 1 (VCAM-1), and vascular endothelial growth factor (VEGF) [84,85,86,87,88,90,91,92,93,94,105]. VEGF is one of the most well-established biomarkers associated with DR [87,92,93,94,106]. Its expression is promoted by retinal ischemia stemming from dyslipidemia and leukostasis and results in the initiation of neovascularization [105]. In our previous study, we identified five inflammatory proteins with significantly higher levels in the serum of type I diabetic patients with DR as compared to those without DR [74]. These proteins included C-responsive protein (CRP), ICAM-1, soluble glycoprotein 130 (sgp130), TNF receptor I, and VCAM-1 [74]. High levels of any of these five proteins significantly increased the odds of developing DR [74].
In another study, the inflammation-regulating proteins α2-HS-glycoprotein (AHSG), α1-acid glycoprotein (AGP), apolipoprotein A-1 (APOA1), and haptoglobin (HP) were found to be differentially expressed in the serum from patients with NPDR and PDR as compared to healthy controls [10]. The serum levels of α-HS-glycoprotein were increased in PDR patients, whereas the levels of AGP and APOA1 were decreased relative to healthy controls [10]. The downregulation of AGP was not expected, since α1-glycoprotein is involved in pro-inflammatory response [10,107,108]. In a separate study, the inflammatory response protein azurocidin (AZU1) was identified as being elevated in the serum of diabetic patients, especially in patients with diabetic complications including retinopathy [109]. This protein is released by neutrophils in response to inflammatory stimuli on vascular endothelium and is known to play a role in vascular permeability within the retina [110,111].
After identifying many differentially expressed proteins in patient serum and VH, Kim et al. validated a set of twenty-seven biomarkers of mild stage NPDR, including apolipoprotein A-I (APOA1), α-2-macroglobulin (A2M), complement factor H (CFH), and prothrombin (F2), using multiple reaction monitoring (MRM) assays [82]. From these proteins, a four-protein biomarker panel was assembled, including afamin (AFM), apolipoprotein C-III (APOC3), complement factor B (CFB), and kallistatin (SERPINA4), to differentiate between diabetic patients with and without DR with ~85–100% accuracy [82].
3.2. Vitreous Humor
The vitreous humor is the gelatinous component of the posterior segment of the eye that gives the eye its spherical shape. In addition to its role in structural support, the transparent nature of the vitreous body aids in light transmission to the retina. Due to the proximal location of the vitreous body to the retina, pathological events in the retina can be monitored through VH examination [4,7,13,16,22,56,101,112,113]. In fact, due to its avascular nature, much of the protein content of the VH comes from the retina itself [81,113,114,115]. VH is often obtained from DR patients during pars plana vitrectomy, in which the entire vitreous body is removed and replaced due to hemorrhage [2,5,22]. Vitreous can also be obtained by a needle biopsy, which is less invasive and can be conducted in the clinic rather than the operating room [22]. VH is obtained from individuals undergoing treatment for a pathological state such as proliferative vitreoretinopathy, rhegmatogenous retinal detachment, idiopathic macular hole (IMH), or epiretinal membrane (ERM) [4,22,63,81,116,117]. In addition, post-mortem VH is obtained from organ donors.
Several proteins in the VH have been identified as biomarkers for different stages of DR. Components of the acute phase response (e.g., α-1-antitrypsin, α-1-glycoproteins, interleukins), complement system (e.g., C3), coagulation pathway (e.g., fibrinogen, prothrombin), and other inflammatory pathways (e.g., VEGF, amyloid-β A4 protein, kininogen-1, metalloproteinase inhibitor 1) have been identified by multiple studies in DR [3,4,11,13,15,39,56,62,63,66,70,71,72,118]. Interleukins have been well characterized for their role in promoting inflammation in eyes with DR [66,119,120,121,122,123,124,125]. Additionally, many members of the apolipoprotein family have been identified in the VH [4,39,63,70,126]. A negative regulator of inflammatory processes, pigment epithelium-derived factor (PEDF) has lower levels in VH from DR subjects as compared to subjects without DR, suggesting that there is not only an increase in pro-inflammatory cytokines, but also a decrease in balancing anti-inflammatory proteins [20,62,63]. Similarly, clusterin (CLU), a protein involved in the regulation of the complement cascade, also had higher levels in control samples relative to DR samples [13,20,39,63]. It has been suggested that clusterin functions in an anti-inflammatory protective role of the blood-retinal barrier [13,67]. Kita et al. showed that plasma kallikrein, a central component of the pro-inflammatory kallikrein kinin system, was elevated in the VH from DR patients [3,15,72]. Gao et al. has shown upregulation of angiotensinogen and downregulation of calsyntenin-1 (CLSTN1), interphotoreceptor retinoid-binding protein (IRBP), interphotoreceptor matrix proteoglycan 2 (IMPG2), extracellular superoxide dismutase (SOD3), and neuroserpin (SERPINI1) in the VH of PDR patients [16].
Several studies have also used VH proteomics to examine the effects of anti-VEGF intravitreal injections on disease progression [3,33,35]. Although Loukovaara et al. observed an increased presence of complement, coagulation, and other inflammatory proteins in the VH of DR patients, they were unable to identify a significant effect of the anti-VEGF agent bevacizumab on these proteins [3]. Interestingly, Wei et al. observed an increase in complement factors, coagulation factors, apolipoproteins, and immunoglobulins following intravitreal injection, while photocoagulation was able to reduce levels of the pro-inflammatory protein osteopontin (SPP1) [35]. Zou et al. compared the VH proteomes of DR patients treated with the anti-VEGF agent ranibizumab and found an expected decrease in VEGF levels as well as a decrease in acute inflammatory response, platelet degranulation, and complement activation proteins [33,34].
3.3. Aqueous Humor
Aqueous humor is the fluid in the anterior chamber of the eye; it is produced by the ciliary body epithelium [127,128]. AH is an integral component in many ocular health functions, including nutrient and oxygen supply, removal of metabolic waste, ocular immunity, and ocular shape and refraction [129]. The major constituents of AH are proteins, water, and electrolytes. Although proteins in AH are present in relatively low concentrations compared to blood serum, they are vital in the maintenance of anterior segment homeostasis [65,128,129,130,131,132,133,134,135,136]. Previous studies [130,131,132,133,137], including one of our own [138], have shown significant alteration in several proteins in the AH obtained from glaucomatous eyes. Proteins in the systemic circulation may cross through fenestrated capillaries into the ciliary body, the production center of AH [13,65,139].
In a recent study examining the AH proteomic profile of PDR patients, LC-MS/MS analysis identified 10 proteins associated with PDR [13]. These proteins were involved in a number of biological processes including inflammation and included apolipoprotein A-I (APOA1), apolipoprotein A-II (APOA2), apolipoprotein A-IV (APOA4), and α-1-acid glycoprotein 1 (ORM1) [13]. This finding evidenced a retinal inflammatory response in individuals with PDR in which pro-inflammatory cytokines entered the AH via either the vasculature or the VH [13]. Another proteomic analysis compared the AH of patients with DR to that of patients without diabetes undergoing cataract surgery [65]. Following 2D-DIGE and MALDI-TOF MS, this study identified eleven differentially expressed proteins, three of which are associated with inflammation: apolipoprotein A-I (APOA1), selenoprotein P (SELENOP), and cystathionine β-synthase (CBS). Selenoprotein P plays an important role in maintaining oxidative balance, and was strongly downregulated in the AH of DR patients [140]. Cystathione β-synthase was highly upregulated in DR patients; this enzyme is responsible for the synthesis of hydrogen sulfide and is linked to inflammation and cellular apoptosis [141]. Chiang et al. conducted a study focusing on the proteomic differences of AH from diabetic patients with and without DR [65]. Inflammation-related protein, apolipoprotein A-I, and a number of other proteins related to angiogenesis, structural remodeling, and oxidative stress were identified [65]. Similar to the findings in VH, overall protein concentrations were higher in the AH from DR patients as compared to patients without DR [65].
3.4. Tears
Tears are an aqueous solution of proteins, lipids, and other components, and their proteome has been shown to respond to insults such as cataract surgery [17,68,142,143,144]. Tear sampling can provide pathological information in retinal disease and is the least invasive method of biofluid collection, offering a potential method for diagnosis and pre-screening [17,68,69]. The tear proteome of DR patients has become the special focus of several recent studies since the first study by Herber et al. in 2000 [145].
Csosz et al. created a methodology for identifying DR biomarkers using MS analysis of pooled tear samples from healthy controls and diabetic patients at various stages of retinopathy (no DR, NPDR, and PDR) [17,104]. A general decrease in protein content was observed with DR onset, perhaps resulting from defective tear formation or more diluted tears [17]. Furthermore, several proteins were identified as being differentially expressed, including the inflammation-related protein lactotransferrin (LTF) which was significantly upregulated in DR [17]. Lactrotransferrin, along with the other five candidate biomarkers identified by this study (lipocalin 1 (LCN1), lacritin (LACRT), lysozyme C (LYZ), lipophilin A (SCGB1D1), and immunoglobulin λ chain (IGLC1)), were used to develop a machine learning model for diagnosis based on both the combined expression of these and other proteins and clinical images of the retina [17,68,69,104]. In a separate study, β-2-microglobulin (B2M) evidenced a decreased expression in DR patients relative to both healthy controls and diabetic patients without DR [104,146]. In addition to proteomic analysis, tear samples have also been used to examine glycomic differences between DR patients and healthy controls [59,104].
4. Post-Translational Modifications as Biomarkers of Diabetic Retinopathy
High mass accuracy instruments have enabled the identification of post-translational modifications (PTMs) in proteins [147,148]. Recent studies have examined the role of protein acetylation and glycosylation in DR pathogenesis [58,59]. MS proteomic approaches have shown that hyperglycemia induces histone acetylation in diabetic rat retinas, which correlates with increased retinal expression of the pro-inflammatory proteins ICAM-1, iNOS, and VEGF [58]. These changes in both histone acetylation and pro-inflammatory cytokine expression were significantly inhibited by a drug used in DR treatment (minocycline) as well as by a histone acetyltransferase inhibitor (garcinol) and histone deacetylase agonists (theophylline and resveratrol) [58]. The correlation between histone acetylation and the expression of pro-inflammatory cytokines suggests that such PTMs and epigenetic regulation may play a role in DR development and progression.
In another study, the inflammation-related proteins antithrombin III (ATIII), clusterin (CLU/APOJ), osteopontin (OPN), and vitronectin (VTN) were found to be present in truncated forms as indicated by unexpectedly low molecular weights obtained via SDS-PAGE/LC-MS/MS. Similarly, a glycomic study on tear proteins found that one O-linked glycan and five N-linked glycans evidenced differences between DR patients and healthy controls [59]. The specific proteins that were glycosylated by these polysaccharides, however, were not identified by the study [59,104].
5. Limitations
The primary limitations of large-scale proteomic analysis of VH and AH is the difficulty in obtaining adequate numbers and volumes of samples, as well as the lack of true controls [63]. Obtaining vitreous and aqueous humor samples requires highly invasive procedures that should only be undertaken when necessary for the patient’s health [4,61]. In this way, it is impossible to obtain AH and VH samples from completely healthy living human eyes [4,61]. For these reasons, much recent focus has been turned towards proteomic screening of tear and serum, both of which can be obtained through non-invasive or minimally invasive procedures.
Different pathological states may cause changes in the total protein content, as retinal vascular leakage is known to increase the amount of proteins present in the VH and the AH by introducing non-native proteins [2,4,5,22,39,57,65,81,149]. Furthermore, highly abundant proteins like serum albumin, hemoglobin, and crystallins can mask the detection of lower abundance proteins [3,16,20,22,57,63,70,149]. Depletion of the most abundant proteins using column chromatography can ameliorate some of these issues and enrich proteins that are less abundant.
6. Future Directions
Proteomic studies examining the ocular biofluids of diabetic patients and diabetic animal models have made an important contribution to the advancement in our understanding of DR pathogenesis. As high-throughput protein analysis techniques have continued to improve, these studies have great future potential for both biomarker discovery and identification of novel therapeutic targets. It is now becoming possible to accurately characterize the proteomes of very small biological samples, making the use of AH and VH from both patients and diabetic animal models more feasible. Greater dynamic range makes it easier to reliably detect very low abundance proteins, which is particularly important for the use of serum samples in the study of DR [150]. Technological improvements have also expanded our ability to detect post-translational modifications of proteins, making it possible to evaluate differences in glycosylation, phosphorylation, and acetylation states, providing more functional context to proteomic differences between healthy and disease states [151].
Lastly, it is important that these wide-scale proteomic analyses are not limited to the identification of diagnostic biomarkers and therapeutic targets. Proteomic and other “–omic” analyses are also valuable tools to screen the effects of novel therapeutic agents. For example, phlorizin, a naturally occurring compound found in fruit trees and known to have anti-inflammatory and antioxidant effects, was used to treat C57BLKS/J db/db mice [9,152,153]. An iTRAQ proteomic analysis of retinal tissue showed changes in the expression of proteins involved in inflammation, apoptosis, and oxidative stress, which corresponded to functionally validated decreases in retinal cell apoptosis and injury [9]. In conclusion, high-throughput proteomic analyses offer a promising future for the discovery of diagnostic, prognostic, and theraputic monitoring biomarkers, as well as for the development of new therapies for this sight-threatening disease.
Author Contributions
Conceptualization, S.S. Writing-Original Draft Preparation, H.Y. and R.R.; Writing-Review & Editing, H.Y., R.R., A.S., and S.S.; Funding Acquisition, S.S.
Funding
Supported by the National Institutes of Health, National Eye Institute (Bethesda, MD, USA) Grant R01-EY026936, awarded to Shruti Sharma, PhD.
Acknowledgments
This work was supported by the National Institutes of Health, National Eye Institute (Bethesda, MD, USA) Grant R01-EY026936, awarded to Shruti Sharma, PhD.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kempen, J.H.; O’Colmain, B.J.; Leske, M.C.; Haffner, S.M.; Klein, R.; Moss, S.E.; Taylor, H.R.; Hamman, R.F. The prevalence of diabetic retinopathy among adults in the United States. Arch. Ophthalmol. 2004, 122, 552–563. [Google Scholar] [PubMed]
- Simo-Servat, O.; Hernandez, C.; Simo, R. Usefulness of the vitreous fluid analysis in the translational research of diabetic retinopathy. Mediat. Inflamm. 2012, 2012, 872978. [Google Scholar] [CrossRef] [PubMed]
- Loukovaara, S.; Nurkkala, H.; Tamene, F.; Gucciardo, E.; Liu, X.; Repo, P.; Lehti, K.; Varjosalo, M. Quantitative proteomics analysis of vitreous humor from diabetic retinopathy patients. J. Proteome Res. 2015, 14, 5131–5143. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Feng, L.; Hu, J.; Xie, C.; Wang, F. Differentiating vitreous proteomes in proliferative diabetic retinopathy using high-performance liquid chromatography coupled to tandem mass spectrometry. Exp. Eye Res. 2013, 108, 110–119. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, J.P.; Santos, F.M.; Rocha, A.S.; Castro-de-Sousa, J.P.; Queiroz, J.A.; Passarinha, L.A.; Tomaz, C.T. Vitreous humor in the pathologic scope: Insights from proteomic approaches. Proteom. Clin. Appl. 2015, 9, 187–202. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.S.; Aiello, L.; Gardner, T.W.; King, G.L.; Blankenship, G.; Cavallerano, J.D.; Ferris, F.L., 3rd; Klein, R.; The American Diabetes Association. Retinopathy in diabetes. Diabetes Care 2004, 27 (Suppl. S1), 84–87. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Yang, C.; Tao, Y.; Zhou, H.; Wang, Y. Recent technological developments in proteomics shed new light on translational research on diabetic microangiopathy. FEBS J. 2013, 280, 5668–5681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Standards of medical care in diabetes–2012. Diabetes Care 2012, 35 (Suppl. S1), 11–63. [CrossRef] [PubMed]
- Zhang, S.Y.; Li, B.Y.; Li, X.L.; Cheng, M.; Cai, Q.; Yu, F.; Wang, W.D.; Tan, M.; Yan, G.; Hu, S.L.; et al. Effects of phlorizin on diabetic retinopathy according to isobaric tags for relative and absolute quantification-based proteomics in db/db mice. Mol. Vis. 2013, 19, 812–821. [Google Scholar]
- Liu, Y.P.; Hu, S.W.; Wu, Z.F.; Mei, L.X.; Lang, P.; Lu, X.H. Proteomic analysis of human serum from diabetic retinopathy. Int. J. Ophthalmol. 2011, 4, 616–622. [Google Scholar]
- Gardner, T.W.; Sundstrom, J.M. A proposal for early and personalized treatment of diabetic retinopathy based on clinical pathophysiology and molecular phenotyping. Vis. Res. 2017, 139, 153–160. [Google Scholar] [CrossRef] [PubMed]
- El-Asrar, A.M. Role of inflammation in the pathogenesis of diabetic retinopathy. Middle East Afr. J. Ophthalmol. 2012, 19, 70–74. [Google Scholar] [CrossRef] [PubMed]
- Balaiya, S.; Zhou, Z.; Chalam, K.V. Characterization of Vitreous and Aqueous Proteome in Humans With Proliferative Diabetic Retinopathy and Its Clinical Correlation. Proteom. Insights 2017, 8, 1178641816686078. [Google Scholar] [CrossRef] [PubMed]
- Klaassen, I.; Van Noorden, C.J.; Schlingemann, R.O. Molecular basis of the inner blood-retinal barrier and its breakdown in diabetic macular edema and other pathological conditions. Prog. Retin. Eye Res. 2013, 34, 19–48. [Google Scholar] [CrossRef] [PubMed]
- Kita, T.; Clermont, A.C.; Murugesan, N.; Zhou, Q.; Fujisawa, K.; Ishibashi, T.; Aiello, L.P.; Feener, E.P.J.D. Plasma kallikrein-kinin system as a VEGF-independent mediator of diabetic macular edema. Diabetes 2015, 64, 3588–3599. [Google Scholar] [CrossRef] [PubMed]
- Gao, B.-B.; Chen, X.; Timothy, N.; Aiello, L.P.; Feener, E.P. Characterization of the vitreous proteome in diabetes without diabetic retinopathy and diabetes with proliferative diabetic retinopathy. J. Proteome 2008, 7, 2516–2525. [Google Scholar] [CrossRef] [PubMed]
- Csosz, E.; Boross, P.; Csutak, A.; Berta, A.; Toth, F.; Poliska, S.; Torok, Z.; Tozser, J. Quantitative analysis of proteins in the tear fluid of patients with diabetic retinopathy. J. Proteom. 2012, 75, 2196–2204. [Google Scholar] [CrossRef]
- Farhangkhoee, H.; Khan, Z.A.; Kaur, H.; Xin, X.; Chen, S.; Chakrabarti, S. Vascular endothelial dysfunction in diabetic cardiomyopathy: Pathogenesis and potential treatment targets. Pharmacol. Ther. 2006, 111, 384–399. [Google Scholar] [CrossRef]
- Krentz, A.J.; Clough, G.; Byrne, C.D. Interactions between microvascular and macrovascular disease in diabetes: Pathophysiology and therapeutic implications. Diabetes Obes. Metab. 2007, 9, 781–791. [Google Scholar] [CrossRef]
- Wang, H.; Feng, L.; Hu, J.W.; Xie, C.L.; Wang, F. Characterisation of the vitreous proteome in proliferative diabetic retinopathy. Proteome Sci. 2012, 10, 15. [Google Scholar] [CrossRef]
- Lattanzio, R.; Brancato, R.; Pierro, L.; Bandello, F.; Iaccher, B.; Fiore, T.; Maestranzi, G. Macular thickness measured by optical coherence tomography (OCT) in diabetic patients. Eur. J. Ophthalmol. 2002, 12, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Velez, G.; Tang, P.H.; Cabral, T.; Cho, G.Y.; Machlab, D.A.; Tsang, S.H.; Bassuk, A.G.; Mahajan, V.B. Personalized proteomics for precision health: Identifying biomarkers of vitreoretinal disease. Transl. Vis. Sci. Technol. 2018, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Chew, E.; Duh, E.J.; Sobrin, L.; Sun, J.K.; VanderBeek, B.L.; Wykoff, C.C.; Gardner, T.W. Diabetic retinopathy: A position statement by the American Diabetes Association. Diabetes Care 2017, 40, 412–418. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.; Wong, T.Y.; Sabanayagam, C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye Vis. 2015, 2, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Do, D.V.; Wang, X.; Vedula, S.S.; Marrone, M.; Sleilati, G.; Hawkins, B.S.; Frank, R.N. Blood pressure control for diabetic retinopathy. Cochrane Database Syst. Rev. 2015. [Google Scholar] [CrossRef] [PubMed]
- Fullerton, B.; Jeitler, K.; Seitz, M.; Horvath, K.; Berghold, A.; Siebenhofer, A. Intensive glucose control versus conventional glucose control for type 1 diabetes mellitus. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef] [PubMed]
- Ding, J.; Wong, T.Y. Current epidemiology of diabetic retinopathy and diabetic macular edema. Curr. Diabetes Rep. 2012, 12, 346–354. [Google Scholar] [CrossRef] [PubMed]
- Cheung, N.; Wong, T.Y. Obesity and eye diseases. Surv. Ophthalmol. 2007, 52, 180–195. [Google Scholar] [CrossRef]
- Frank, R.N. Diabetic retinopathy and systemic factors. Middle East Afr. J. Ophthalmol. 2015, 22, 151–156. [Google Scholar] [CrossRef]
- Long, M.; Wang, C.; Liu, D. Glycated hemoglobin A1C and vitamin D and their association with diabetic retinopathy severity. Nutr. Diabetes 2017, 7, e281. [Google Scholar] [CrossRef]
- El Rami, H.; Barham, R.; Sun, J.K.; Silva, P.S. Evidence-Based Treatment of Diabetic Retinopathy. Semin. Ophthalmol. 2017, 32, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Massin, P.; Bandello, F.; Garweg, J.G.; Hansen, L.L.; Harding, S.P.; Larsen, M.; Mitchell, P.; Sharp, D.; Wolf-Schnurrbusch, U.E.; Gekkieva, M.; et al. Safety and efficacy of ranibizumab in diabetic macular edema (RESOLVE Study): A 12-month, randomized, controlled, double-masked, multicenter phase II study. Diabetes Care 2010, 33, 2399–2405. [Google Scholar] [CrossRef] [PubMed]
- Zou, C.; Han, C.; Zhao, M.; Yu, J.; Bai, L.; Yao, Y.; Gao, S.; Cao, H.; Zheng, Z. Change of ranibizumab-induced human vitreous protein profile in patients with proliferative diabetic retinopathy based on proteomics analysis. Clin. Proteom. 2018, 15, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osaadon, P.; Fagan, X.; Lifshitz, T.; Levy, J. A review of anti-VEGF agents for proliferative diabetic retinopathy. Eye 2014, 28, 510. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Zhang, T.; Jiang, R.; Chang, Q.; Zhang, Y.; Huang, X.; Gao, X.; Jin, H.; Xu, G. Vitreous Fibronectin and Fibrinogen Expression Increased in Eyes with Proliferative Diabetic Retinopathy After Intravitreal Anti-VEGF Therapy. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5783–5791. [Google Scholar] [CrossRef] [PubMed]
- Simo, R.; Sundstrom, J.M.; Antonetti, D.A. Ocular Anti-VEGF therapy for diabetic retinopathy: The role of VEGF in the pathogenesis of diabetic retinopathy. Diabetes Care 2014, 37, 893–899. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.; Bandello, F.; Schmidt-Erfurth, U.; Lang, G.E.; Massin, P.; Schlingemann, R.O.; Sutter, F.; Simader, C.; Burian, G.; Gerstner, O.; et al. The RESTORE study: Ranibizumab monotherapy or combined with laser versus laser monotherapy for diabetic macular edema. Ophthalmology 2011, 118, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Zechmeister-Koss, I.; Huic, M. Vascular endothelial growth factor inhibitors (anti-VEGF) in the management of diabetic macular oedema: A systematic review. Br. J. Ophthalmol. 2012, 96, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Hernández, C.; Garcia-Ramírez, M.; Simó, R. Overexpression of hemopexin in the diabetic eye: A new pathogenic candidate for diabetic macular edema. Diabetes Care 2013, 36, 2815–2821. [Google Scholar] [CrossRef]
- Cai, S.; Bressler, N.M. Aflibercept, bevacizumab or ranibizumab for diabetic macular oedema: Recent clinically relevant findings from DRCR. net Protocol T. Curr. Opin. Ophthalmol. 2017, 28, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, Q.; Gillies, M.C.; Wong, T.Y. Management of diabetic retinopathy: A systematic review. JAMA 2007, 298, 902–916. [Google Scholar] [CrossRef] [PubMed]
- Simo, R.; Hernandez, C. Intravitreous anti-VEGF for diabetic retinopathy: Hopes and fears for a new therapeutic strategy. Diabetologia 2008, 51, 1574. [Google Scholar] [CrossRef] [PubMed]
- Brand, C.S. Management of retinal vascular diseases: A patient-centric approach. Eye 2012, 26, S1. [Google Scholar] [CrossRef] [PubMed]
- Elman, M.J.; Aiello, L.P.; Beck, R.W.; Bressler, N.M.; Bressler, S.B.; Edwards, A.R.; Ferris, F.L., 3rd; Friedman, S.M.; Glassman, A.R.; Miller, K.M.; et al. Randomized trial evaluating ranibizumab plus prompt or deferred laser or triamcinolone plus prompt laser for diabetic macular edema. Ophthalmology 2010, 117, 1064–1077.e35. [Google Scholar] [CrossRef] [PubMed]
- Ip, M.S.; Domalpally, A.; Hopkins, J.J.; Wong, P.; Ehrlich, J.S. Long-term effects of ranibizumab on diabetic retinopathy severity and progression. Arch. Ophthalmol. 2012, 130, 1145–1152. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Ren, X.; Wei, H.; Zhao, L.; Zhang, X.; Liu, J.; Su, C.; Tan, L.; Li, X. Intravitreal conbercept (KH902) for surgical treatment of severe proliferative diabetic retinopathy. Retina 2016, 36, 938–943. [Google Scholar] [CrossRef]
- Bressler, S.B.; Beaulieu, W.T.; Glassman, A.R.; Gross, J.G.; Jampol, L.M.; Melia, M.; Peters, M.A.; Rauser, M.E. Factors Associated with Worsening Proliferative Diabetic Retinopathy in Eyes Treated with Panretinal Photocoagulation or Ranibizumab. Ophthalmology 2017, 124, 431–439. [Google Scholar] [CrossRef]
- Parikh, R.N.; Traband, A.; Kolomeyer, A.M.; VanderBeek, B.L.; Kim, B.J.; Maguire, A.M.; Brucker, A.J. Intravitreal bevacizumab for the treatment of vitreous hemorrhage due to proliferative diabetic retinopathy. Am. J. Ophthalmol. 2017, 176, 194–202. [Google Scholar] [CrossRef]
- Ahmadieh, H.; Shoeibi, N.; Entezari, M.; Monshizadeh, R. Intravitreal bevacizumab for prevention of early postvitrectomy hemorrhage in diabetic patients: A randomized clinical trial. Ophthalmology 2009, 116, 1943–1948. [Google Scholar] [CrossRef]
- Yeh, P.T.; Yang, C.H.; Yang, C.M. Intravitreal bevacizumab injection for recurrent vitreous haemorrhage after diabetic vitrectomy. Acta Ophthalmol. 2011, 89, 634–640. [Google Scholar] [CrossRef]
- Yeh, P.-T.; Yang, C.-M.; Lin, Y.-C.; Chen, M.-S.; Yang, C.-H. Bevacizumab pretreatment in vitrectomy with silicone oil for severe diabetic retinopathy. Retina 2009, 29, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, M.S.; Contreras, I.; Noval, S. Anti-angiogenic drugs as an adjunctive therapy in the surgical treatment of diabetic retinopathy. Curr. Diabetes Rev. 2009, 5, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Demir, M.; Oba, E.; Can, E.; Kara, O.; Cinar, S. Effect of bevacizumab injection before vitrectomy on intravitreal hemorrhage in pseudophakic patients with proliferative diabetic retinopathy. Ophthalmol. Eye Dis. 2013, 5, OED–S12352. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Zou, C.; Cao, H.; Zhao, M.; Yu, S.; Qiu, Q.; Xu, X.; Zheng, Z. Preoperative intravitreal injection of ranibizumab for patients with severe proliferative diabetic retinopathy contributes to a decreased risk of postoperative neovascular glaucoma. Acta Ophthalmol. 2016, 94, 414–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, B.; Zhang, Y.; Zeng, Q.; Han, Q.; Zhang, L.; Liu, M.; Li, X. Intravitreal injection of ranibizumab and CTGF shRNA improves retinal gene expression and microvessel ultrastructure in a rodent model of diabetes. Int. J. Mol. Sci. 2014, 15, 1606–1624. [Google Scholar] [CrossRef] [PubMed]
- Skeie, J.M.; Mahajan, V.B. Proteomic interactions in the mouse vitreous-retina complex. PLoS ONE 2013, 8, e82140. [Google Scholar] [CrossRef]
- Kim, K.; Kim, Y. Preparing multiple-reaction monitoring for quantitative clinical proteomics. Expert Rev. Proteom. 2009, 6, 225–229. [Google Scholar] [CrossRef] [Green Version]
- Kadiyala, C.S.; Zheng, L.; Du, Y.; Yohannes, E.; Kao, H.Y.; Miyagi, M.; Kern, T.S. Acetylation of retinal histones in diabetes increases inflammatory proteins: Effects of minocycline and manipulation of histone acetyltransferase (HAT) and histone deacetylase (HDAC). J. Biol. Chem. 2012, 287, 25869–25880. [Google Scholar] [CrossRef]
- Nguyen-Khuong, T.; Everest-Dass, A.V.; Kautto, L.; Zhao, Z.; Willcox, M.D.; Packer, N.H. Glycomic characterization of basal tears and changes with diabetes and diabetic retinopathy. Glycobiology 2015, 25, 269–283. [Google Scholar] [CrossRef]
- Fu, Q.; Chen, Z.; Zhang, S.; Parker, S.J.; Fu, Z.; Tin, A.; Liu, X.; Van Eyk, J.E. Multiple and selective reaction monitoring using triple quadrupole mass spectrometer: Preclinical large cohort analysis. In Quantitative Proteomics by Mass Spectrometry; Springer: Berlin/Heidelberg, Germany, 2016; pp. 249–264. [Google Scholar]
- Jay, N.L.; Gillies, M.J.C.; Ophthalmology, E. Proteomic analysis of ophthalmic disease. Clin. Exp. Ophthalmol. 2012, 40, 755–763. [Google Scholar] [CrossRef]
- Garcia-Ramirez, M.; Canals, F.; Hernandez, C.; Colome, N.; Ferrer, C.; Carrasco, E.; Garcia-Arumi, J.; Simo, R. Proteomic analysis of human vitreous fluid by fluorescence-based difference gel electrophoresis (DIGE): A new strategy for identifying potential candidates in the pathogenesis of proliferative diabetic retinopathy. Diabetologia 2007, 50, 1294–1303. [Google Scholar] [CrossRef] [PubMed]
- Shitama, T.; Hayashi, H.; Noge, S.; Uchio, E.; Oshima, K.; Haniu, H.; Takemori, N.; Komori, N.; Matsumoto, H. Proteome Profiling of Vitreoretinal Diseases by Cluster Analysis. Proteom. Clin. Appl. 2008, 2, 1265–1280. [Google Scholar] [CrossRef]
- Hernández, C.; García-Ramírez, M.; Colomé, N.; Villarroel, M.; Corraliza, L.; García-Pacual, L.; Casado, J.; Canals, F.; Simó, R. New pathogenic candidates for diabetic macular edema detected by proteomic analysis. Diabetes Care 2010, 33, e92. [Google Scholar] [CrossRef] [PubMed]
- Chiang, S.-Y.; Tsai, M.-L.; Wang, C.-Y.; Chen, A.; Chou, Y.-C.; Hsia, C.-W.; Wu, Y.-F.; Chen, H.-M.; Huang, T.-H.; Chen, P.-H. Proteomic analysis and identification of aqueous humor proteins with a pathophysiological role in diabetic retinopathy. J. Proteom. 2012, 75, 2950–2959. [Google Scholar] [CrossRef] [PubMed]
- Srividya, G.; Jain, M.; Mahalakshmi, K.; Gayathri, S.; Raman, R.; Angayarkanni, N. A novel and less invasive technique to assess cytokine profile of vitreous in patients of diabetic macular oedema. Eye 2018, 32, 820–829. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Kim, J.H.; Jun, H.O.; Yu, Y.S.; Min, B.H.; Park, K.H.; Kim, K.-W. Protective effect of Clusterin from oxidative stress–induced apoptosis in human retinal pigment epithelial cells. Investig. Ophthalmol. Vis. Sci. 2010, 51, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Torok, Z.; Peto, T.; Csosz, E.; Tukacs, E.; Molnar, A.; Maros-Szabo, Z.; Berta, A.; Tozser, J.; Hajdu, A.; Nagy, V.; et al. Tear fluid proteomics multimarkers for diabetic retinopathy screening. BMC Ophthalmol. 2013, 13, 40. [Google Scholar] [CrossRef] [PubMed]
- Torok, Z.; Peto, T.; Csosz, E.; Tukacs, E.; Molnar, A.M.; Berta, A.; Tozser, J.; Hajdu, A.; Nagy, V.; Domokos, B.; et al. Combined Methods for Diabetic Retinopathy Screening, Using Retina Photographs and Tear Fluid Proteomics Biomarkers. J. Diabetes Res. 2015, 2015, 623619. [Google Scholar] [CrossRef] [PubMed]
- Ohman, T.; Tamene, F.; Goos, H.; Loukovaara, S.; Varjosalo, M. Systems pathology analysis identifies neurodegenerative nature of age-related vitreoretinal interface diseases. Aging Cell 2018, 17, e12809. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Lu, Q.; Lu, P. Quantitative proteomics analysis of vitreous body from type 2 diabetic patients with proliferative diabetic retinopathy. BMC Ophthalmol. 2018, 18, 151. [Google Scholar] [CrossRef]
- Schori, C.; Trachsel, C.; Grossmann, J.; Zygoula, I.; Barthelmes, D.; Grimm, C. The Proteomic Landscape in the Vitreous of Patients With Age-Related and Diabetic Retinal Disease. Investig. Ophthalmol. Vis. Sci. 2018, 59, AMD31–AMD40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.; Kim, S.J.; Yu, H.G.; Yu, J.; Park, K.S.; Jang, I.-J.; Kim, Y. Verification of biomarkers for diabetic retinopathy by multiple reaction monitoring. J. Proteome Res. 2010, 9, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Purohit, S.; Sharma, A.; Hopkins, D.; Steed, L.; Bode, B.; Anderson, S.W.; Caldwell, R.; She, J.X. Elevated Serum Levels of Soluble TNF Receptors and Adhesion Molecules Are Associated with Diabetic Retinopathy in Patients with Type-1 Diabetes. Mediat. Inflamm. 2015, 2015, 279393. [Google Scholar] [CrossRef] [PubMed]
- Funatsu, H.; Yamashita, T.; Yamashita, H. Vitreous fluid biomarkers. Adv. Clin. Chem. 2006, 42, 111–166. [Google Scholar]
- Zhang, X.; Bao, S.; Hambly, B.D.; Gillies, M.C. Vascular endothelial growth factor-A: A multifunctional molecular player in diabetic retinopathy. Int. J. Biochem. Cell Biol. 2009, 41, 2368–2371. [Google Scholar] [CrossRef]
- Yoshimura, T.; Sonoda, K.H.; Sugahara, M.; Mochizuki, Y.; Enaida, H.; Oshima, Y.; Ueno, A.; Hata, Y.; Yoshida, H.; Ishibashi, T. Comprehensive analysis of inflammatory immune mediators in vitreoretinal diseases. PLoS ONE 2009, 4, e8158. [Google Scholar] [CrossRef]
- Loukovaara, S.; Robciuc, A.; Holopainen, J.M.; Lehti, K.; Pessi, T.; Liinamaa, J.; Kukkonen, K.T.; Jauhiainen, M.; Koli, K.; Keski-Oja, J.; et al. Ang-2 upregulation correlates with increased levels of MMP-9, VEGF, EPO and TGFbeta1 in diabetic eyes undergoing vitrectomy. Acta Ophthalmol. 2013, 91, 531–539. [Google Scholar] [CrossRef]
- Mohan, N.; Monickaraj, F.; Balasubramanyam, M.; Rema, M.; Mohan, V. Imbalanced levels of angiogenic and angiostatic factors in vitreous, plasma and postmortem retinal tissue of patients with proliferative diabetic retinopathy. J. Diabetes Its Complicat. 2012, 26, 435–441. [Google Scholar] [CrossRef]
- Fong, A.H.; Lai, T.Y. Long-term effectiveness of ranibizumab for age-related macular degeneration and diabetic macular edema. Clin. Interv. Aging 2013, 8, 467–483. [Google Scholar] [Green Version]
- Mahajan, V.B.; Skeie, J.M. Translational vitreous proteomics. Proteom. Clin. Appl. 2014, 8, 204–208. [Google Scholar] [CrossRef]
- Kim, K.; Kim, S.J.; Han, D.; Jin, J.; Yu, J.; Park, K.S.; Yu, H.G.; Kim, Y. Verification of multimarkers for detection of early stage diabetic retinopathy using multiple reaction monitoring. J. Proteome Res. 2013, 12, 1078–1089. [Google Scholar] [CrossRef] [PubMed]
- Polat, S.B.; Ugurlu, N.; Yulek, F.; Simavli, H.; Ersoy, R.; Cakir, B.; Erel, O. Evaluation of serum fibrinogen, plasminogen, alpha2-anti-plasmin, and plasminogen activator inhibitor levels (PAI) and their correlation with presence of retinopathy in patients with type 1 DM. J. Diabetes Res. 2014, 2014, 317292. [Google Scholar] [CrossRef] [PubMed]
- Sasongko, M.B.; Wong, T.Y.; Jenkins, A.J.; Nguyen, T.T.; Shaw, J.E.; Wang, J.J. Circulating markers of inflammation and endothelial function, and their relationship to diabetic retinopathy. Diabet. Med. J. Br. Diabet. Assoc. 2015, 32, 686–691. [Google Scholar] [CrossRef]
- Yang, H.S.; Woo, J.E.; Lee, S.J.; Park, S.H.; Woo, J.M. Elevated plasma pentraxin 3 levels are associated with development and progression of diabetic retinopathy in Korean patients with type 2 diabetes mellitus. Investig. Ophthalmol. Vis. Sci. 2014, 55, 5989–5997. [Google Scholar] [CrossRef] [PubMed]
- Meleth, A.D.; Agron, E.; Chan, C.C.; Reed, G.F.; Arora, K.; Byrnes, G.; Csaky, K.G.; Ferris, F.L., 3rd; Chew, E.Y. Serum inflammatory markers in diabetic retinopathy. Investig. Ophthalmol. Vis. Sci. 2005, 46, 4295–4301. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Saxena, S.; Khanna, V.K.; Shukla, R.K.; Meyer, C.H. Status of serum VEGF and ICAM-1 and its association with external limiting membrane and inner segment-outer segment junction disruption in type 2 diabetes mellitus. Mol. Vis. 2013, 19, 1760–1768. [Google Scholar]
- Doganay, S.; Evereklioglu, C.; Er, H.; Turkoz, Y.; Sevinc, A.; Mehmet, N.; Savli, H. Comparison of serum NO, TNF-alpha, IL-1beta, sIL-2R, IL-6 and IL-8 levels with grades of retinopathy in patients with diabetes mellitus. Eye 2002, 16, 163–170. [Google Scholar] [CrossRef] [PubMed]
- Kaviarasan, K.; Jithu, M.; Arif Mulla, M.; Sharma, T.; Sivasankar, S.; Das, U.N.; Angayarkanni, N. Low blood and vitreal BDNF, LXA4 and altered Th1/Th2 cytokine balance are potential risk factors for diabetic retinopathy. Metab. Clin. Exp. 2015, 64, 958–966. [Google Scholar] [CrossRef]
- Rajab, H.A.; Baker, N.L.; Hunt, K.J.; Klein, R.; Cleary, P.A.; Lachin, J.; Virella, G.; Lopes-Virella, M.F. The predictive role of markers of Inflammation and endothelial dysfunction on the course of diabetic retinopathy in type 1 diabetes. J. Diabetes Its Complicat. 2015, 29, 108–114. [Google Scholar] [CrossRef]
- Ogata, N.; Matsuoka, M.; Matsuyama, K.; Shima, C.; Tajika, A.; Nishiyama, T.; Wada, M.; Jo, N.; Higuchi, A.; Minamino, K.; et al. Plasma concentration of pigment epithelium-derived factor in patients with diabetic retinopathy. J. Clin. Endocrinol. Metab. 2007, 92, 1176–1179. [Google Scholar] [CrossRef]
- Cavusoglu, A.C.; Bilgili, S.; Alaluf, A.; Dogan, A.; Yilmaz, F.; Aslanca, D.; Karaca, B.; Yuksel, B.; Topaloglu, E. Vascular endothelial growth factor level in the serum of diabetic patients with retinopathy. Ann. Ophthalmol. 2007, 39, 205–208. [Google Scholar] [CrossRef]
- Ozturk, B.T.; Bozkurt, B.; Kerimoglu, H.; Okka, M.; Kamis, U.; Gunduz, K. Effect of serum cytokines and VEGF levels on diabetic retinopathy and macular thickness. Mol. Vis. 2009, 15, 1906–1914. [Google Scholar] [PubMed]
- Du, J.H.; Li, X.; Li, R.; Xu, L.; Ma, R.R.; Liu, S.F.; Zhang, Z.; Sun, H.Z. Elevation of serum apelin-13 associated with proliferative diabetic retinopathy in type 2 diabetic patients. Int. J. Ophthalmol. 2014, 7, 968–973. [Google Scholar] [PubMed]
- Joussen, A.M.; Poulaki, V.; Le, M.L.; Koizumi, K.; Esser, C.; Janicki, H.; Schraermeyer, U.; Kociok, N.; Fauser, S.; Kirchhof, B.; et al. A central role for inflammation in the pathogenesis of diabetic retinopathy. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2004, 18, 1450–1452. [Google Scholar] [CrossRef] [PubMed]
- Gerhardinger, C.; Costa, M.B.; Coulombe, M.C.; Toth, I.; Hoehn, T.; Grosu, P. Expression of acute-phase response proteins in retinal Muller cells in diabetes. Investig. Ophthalmol. Vis. Sci. 2005, 46, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Funatsu, H.; Yamashita, H.; Sakata, K.; Noma, H.; Mimura, T.; Suzuki, M.; Eguchi, S.; Hori, S. Vitreous levels of vascular endothelial growth factor and intercellular adhesion molecule 1 are related to diabetic macular edema. Ophthalmology 2005, 112, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Krady, J.K.; Basu, A.; Allen, C.M.; Xu, Y.; LaNoue, K.F.; Gardner, T.W.; Levison, S.W. Minocycline reduces proinflammatory cytokine expression, microglial activation, and caspase-3 activation in a rodent model of diabetic retinopathy. Diabetes 2005, 54, 1559–1565. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kim, J.H.; Park, J.A.; Lee, S.W.; Kim, W.J.; Yu, Y.S.; Kim, K.W. Blood-neural barrier: Intercellular communication at glio-vascular interface. J. Biochem. Mol. Biol. 2006, 39, 339–345. [Google Scholar] [CrossRef]
- Antonetti, D.A.; Klein, R.; Gardner, T.W. Diabetic retinopathy. N. Engl. J. Med. 2012, 366, 1227–1239. [Google Scholar] [CrossRef]
- Monteiro, R.; Vitorino, R.; Domingues, P.; Radhouani, H.; Carvalho, C.; Poeta, P.; Torres, C.; Igrejas, G. Proteome of a methicillin-resistant Staphylococcus aureus clinical strain of sequence type ST398. J. Proteom. 2012, 75, 2892–2915. [Google Scholar] [CrossRef]
- Biomarkers and surrogate endpoints: Preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [CrossRef] [PubMed]
- Gutman, S.; Kessler, L.G. The US Food and Drug Administration perspective on cancer biomarker development. Nat. Rev. Cancer 2006, 6, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Hagan, S.; Martin, E.; Enriquez-de-Salamanca, A. Tear fluid biomarkers in ocular and systemic disease: Potential use for predictive, preventive and personalised medicine. EPMA J. 2016, 7, 15. [Google Scholar] [CrossRef] [PubMed]
- Pusparajah, P.; Lee, L.H.; Abdul Kadir, K. Molecular Markers of Diabetic Retinopathy: Potential Screening Tool of the Future? Front. Physiol. 2016, 7, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, J.; Kern, T.S. Inflammation in diabetic retinopathy. Prog. Retin. Eye Res. 2011, 30, 343–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christiansen, M.S.; Hommel, E.; Magid, E.; Feldt-Rasmussen, B. Orosomucoid in urine is a powerful predictor of cardiovascular mortality in normoalbuminuric patients with type 2 diabetes at five years of follow-up. Diabetologia 2005, 48, 386–393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, N.; Shankernarayan, N.P.; Dharmalingam, K. alpha1-acid glycoprotein as a putative biomarker for monitoring the development of the type II reactional stage of leprosy. J. Med. Microbiol. 2010, 59 Pt 4, 400–407. [Google Scholar] [CrossRef]
- Caseiro, A.; Ferreira, R.; Quintaneiro, C.; Pereira, A.; Marinheiro, R.; Vitorino, R.; Amado, F. Protease profiling of different biofluids in type 1 diabetes mellitus. Clin. Biochem. 2012, 45, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Ipek, E.; Yolcu, M.; Yildirim, E.; Altinkaynak, K.; Ozbek Sebin, S.; Kalkan, K.; Gulcu, O.; Ermis, E.; Ozturk, M. A Novel Marker of Inflammation: Azurocidin in Patients with ST Segment Elevation Myocardial Infarction. Int. J. Mol. Sci. 2018, 19, 3797. [Google Scholar] [CrossRef]
- Skondra, D.; Noda, K.; Almulki, L.; Tayyari, F.; Frimmel, S.; Nakazawa, T.; Kim, I.K.; Zandi, S.; Thomas, K.L.; Miller, J.W. Characterization of azurocidin as a permeability factor in the retina: Involvement in VEGF-induced and early diabetic blood-retinal barrier breakdown. Investig. Ophthalmol. Vis. Sci. 2008, 49, 726–731. [Google Scholar] [CrossRef]
- Lam, T.C.; Chun, R.K.; Li, K.K.; To, C.H.; Optometry, E. Application of proteomic technology in eye research: A mini review. Clin. Exp. 2008, 91, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Murthy, K.R.; Goel, R.; Subbannayya, Y.; Jacob, H.K.; Murthy, P.R.; Manda, S.S.; Patil, A.H.; Sharma, R.; Sahasrabuddhe, N.A.; Parashar, A. Proteomic analysis of human vitreous humor. Clin. Proteom. 2014, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Funaki, H.; Sawaguchi, S.; Yaoeda, K.; Koyama, Y.; Yaoita, E.; Funaki, S.; Shirakashi, M.; Oshima, Y.; Shukunami, C.; Hiraki, Y. Expression and localization of angiogenic inhibitory factor, chondromodulin-I, in adult rat eye. Investig. Ophthalmol. Vis. Sci. 2001, 42, 1193–1200. [Google Scholar]
- Halfter, W.; Dong, S.; Dong, A.; Eller, A.; Nischt, R. Origin and turnover of ECM proteins from the inner limiting membrane and vitreous body. Eye 2008, 22, 1207. [Google Scholar] [CrossRef] [PubMed]
- Davuluri, G.; Espina, V.; Petricoin, E.F.; Ross, M.; Deng, J.; Liotta, L.A.; Glaser, B.M. Activated VEGF receptor shed into the vitreous in eyes with wet AMD: A new class of biomarkers in the vitreous with potential for predicting the treatment timing and monitoring response. Arch. Ophthalmol. 2009, 127, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Ecker, S.M.; Pfahler, S.M.; Hines, J.C.; Lovelace, A.S.; Glaser, B.M. Sequential in-office vitreous aspirates demonstrate vitreous matrix metalloproteinase 9 levels correlate with the amount of subretinal fluid in eyes with wet age-related macular degeneration. Mol. Vis. 2012, 18, 1658. [Google Scholar] [PubMed]
- Yenihayat, F.; Ozkan, B.; Kasap, M.; Karabas, V.L.; Guzel, N.; Akpinar, G.; Pirhan, D. Vitreous IL-8 and VEGF levels in diabetic macular edema with or without subretinal fluid. Int. Ophthalmol. 2019, 39, 821–828. [Google Scholar] [CrossRef] [PubMed]
- El Asrar, A.M.A.; Maimone, D.; Morse, P.H.; Gregory, S.; Reder, A.T. Cytokines in the vitreous of patients with proliferative diabetic retinopathy. Am. J. Ophthalmol. 1992, 114, 731–736. [Google Scholar] [CrossRef]
- Arend, W.P. Interleukin-1 receptor antagonist. In Advances in Immunology; Elsevier: Amsterdam, The Netherlands, 1993; Volume 54, pp. 167–227. [Google Scholar]
- Carmo, A.; Cunha-Vaz, J.G.; Carvalho, A.P.; Lopes, M.C. L-arginine transport in retinas from streptozotocin diabetic rats: Correlation with the level of IL-1 beta and NO synthase activity. Vis. Res. 1999, 39, 3817–3823. [Google Scholar] [CrossRef]
- Arend, W.P.; Gabay, C. Physiologic role of interleukin-1 receptor antagonist. Arthritis Res. Ther. 2000, 2, 245. [Google Scholar] [CrossRef] [PubMed]
- Demircan, N.; Safran, B.G.; Soylu, M.; Ozcan, A.A.; Sizmaz, S. Determination of vitreous interleukin-1 (IL-1) and tumour necrosis factor (TNF) levels in proliferative diabetic retinopathy. Eye 2006, 20, 1366–1369. [Google Scholar] [CrossRef] [PubMed]
- Gerhardinger, C.; Liu, Y.; Dagher, Z. Overexpression of IL-1 receptor antagonist in the rat retina by AAV2-mediated gene transfer prevents capillary loss in experimental diabetes. Investig. Ophthalmol. Vis. Sci. 2012, 53, 5764. [Google Scholar]
- Stahel, M.; Becker, M.; Graf, N.; Michels, S. Systemic interleukin 1β inhibition in proliferative diabetic retinopathy: A prospective open-label study using Canakinumab. Retina 2016, 36, 385. [Google Scholar] [CrossRef] [PubMed]
- Ouchi, M.; West, K.; Crabb, J.W.; Kinoshita, S.; Kamei, M. Proteomic analysis of vitreous from diabetic macular edema. Exp. Eye Res. 2005, 81, 176–182. [Google Scholar] [CrossRef]
- Carreon, T.; van der Merwe, E.; Fellman, R.L.; Johnstone, M.; Bhattacharya, S.K. Aqueous outflow—A continuum from trabecular meshwork to episcleral veins. Prog. Retin. Eye Res. 2017, 57, 108–133. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, U.R.; Madden, B.J.; Charlesworth, M.C.; Fautsch, M.P. Proteome analysis of human aqueous humor. Investig. Ophthalmol. Vis. Sci. 2010, 51, 4921–4931. [Google Scholar] [CrossRef]
- Grus, F.H.; Joachim, S.C.; Pfeiffer, N. Proteomics in ocular fluids. Proteom. Clin. Appl. 2007, 1, 876–888. [Google Scholar] [CrossRef]
- Kliuchnikova, A.A.; Samokhina, N.I.; Ilina, I.Y.; Karpov, D.S.; Pyatnitskiy, M.A.; Kuznetsova, K.G.; Toropygin, I.Y.; Kochergin, S.A.; Alekseev, I.B.; Zgoda, V.G.; et al. Human aqueous humor proteome in cataract, glaucoma, and pseudoexfoliation syndrome. Proteomics 2016, 16, 1938–1946. [Google Scholar] [CrossRef]
- Funke, S.; Perumal, N.; Bell, K.; Pfeiffer, N.; Grus, F.H. The potential impact of recent insights into proteomic changes associated with glaucoma. Expert Rev. Proteom. 2017, 14, 311–334. [Google Scholar] [CrossRef]
- Kaeslin, M.A.; Killer, H.E.; Fuhrer, C.A.; Zeleny, N.; Huber, A.R.; Neutzner, A. Changes to the Aqueous Humor Proteome during Glaucoma. PLoS ONE 2016, 11, e0165314. [Google Scholar] [CrossRef]
- Izzotti, A.; Longobardi, M.; Cartiglia, C.; Sacca, S.C. Proteome alterations in primary open angle glaucoma aqueous humor. J. Proteome Res. 2010, 9, 4831–4838. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Lu, Q.; Xue, P.; Zhang, H.; Dong, Z.; Yang, F.; Wang, N. Proteomic analysis of aqueous humor from patients with myopia. Mol. Vis. 2008, 14, 370–377. [Google Scholar] [PubMed]
- Semba, R.D.; Enghild, J.J.; Venkatraman, V.; Dyrlund, T.F.; Van Eyk, J.E. The Human Eye Proteome Project: Perspectives on an emerging proteome. Proteomics 2013, 13, 2500–2511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, T.W.; Kang, J.W.; Ahn, J.; Lee, E.K.; Cho, K.C.; Han, B.N.; Hong, N.Y.; Park, J.; Kim, K.P. Proteomic analysis of the aqueous humor in age-related macular degeneration (AMD) patients. J. Proteome Res. 2012, 11, 4034–4043. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Xue, P.; Wang, N.; Dong, Z.; Lu, Q.; Yang, F. Proteomic analysis of aqueous humor from patients with primary open angle glaucoma. Mol. Vis. 2010, 16, 2839–2846. [Google Scholar] [PubMed]
- Sharma, S.; Bollinger, K.E.; Kodeboyina, S.K.; Zhi, W.; Patton, J.; Bai, S.; Edwards, B.; Ulrich, L.; Bogorad, D.; Sharma, A. Proteomic Alterations in Aqueous Humor From Patients With Primary Open Angle Glaucoma. Investig. Ophthalmol. Vis. Sci. 2018, 59, 2635–2643. [Google Scholar] [CrossRef] [PubMed]
- Freddo, T.F. A contemporary concept of the blood-aqueous barrier. Prog. Retin. Eye Res. 2013, 32, 181–195. [Google Scholar] [CrossRef] [PubMed]
- Barrett, C.W.; Short, S.P.; Williams, C.S. Selenoproteins and oxidative stress-induced inflammatory tumorigenesis in the gut. Cell. Mol. Life Sci. 2017, 74, 607–616. [Google Scholar] [CrossRef]
- Qi, F.; Zhou, Y.; Xiao, Y.; Tao, J.; Gu, J.; Jiang, X.; Xu, G.-Y. Promoter demethylation of cystathionine-β-synthetase gene contributes to inflammatory pain in rats. PAIN® 2013, 154, 34–45. [Google Scholar] [CrossRef]
- de Souza, G.A.; Godoy, L.M.; Mann, M. Identification of 491 proteins in the tear fluid proteome reveals a large number of proteases and protease inhibitors. Genome Biol. 2006, 7, R72. [Google Scholar] [CrossRef]
- Li, N.; Wang, N.; Zheng, J.; Liu, X.M.; Lever, O.W.; Erickson, P.M.; Li, L. Characterization of human tear proteome using multiple proteomic analysis techniques. J. Proteome Res. 2005, 4, 2052–2061. [Google Scholar] [CrossRef] [PubMed]
- Csutak, A.; Silver, D.M.; Tozser, J.; Steiber, Z.; Bagossi, P.; Hassan, Z.; Berta, A. Plasminogen activator inhibitor in human tears after laser refractive surgery. J. Cataract Refract. Surg. 2008, 34, 897–901. [Google Scholar] [CrossRef] [PubMed]
- Herber, S.; Grus, F.H.; Sabuncuo, P.; Augustin, A.J. Two-dimensional analysis of tear protein patterns of diabetic patients. Electrophoresis 2001, 22, 1838–1844. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, P.K.; Yoo, H.S.; Kim, C.W. Comparison of tear proteins between healthy and early diabetic retinopathy patients. Clin. Biochem. 2012, 45, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Sadygov, R.G. High mass accuracy phosphopeptide identification using tandem mass spectra. Int. J. Proteom. 2012, 2012, 104681. [Google Scholar] [CrossRef]
- Doll, S.; Burlingame, A.L. Mass spectrometry-based detection and assignment of protein posttranslational modifications. ACS Chem. Biol. 2015, 10, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Angi, M.; Kalirai, H.; Coupland, S.E.; Damato, B.E.; Semeraro, F.; Romano, M.R. Proteomic analyses of the vitreous humour. Mediat. Inflamm. 2012, 2012. [Google Scholar] [CrossRef]
- Ronsein, G.E.; Pamir, N.; von Haller, P.D.; Kim, D.S.; Oda, M.N.; Jarvik, G.P.; Vaisar, T.; Heinecke, J.W. Parallel reaction monitoring (PRM) and selected reaction monitoring (SRM) exhibit comparable linearity, dynamic range and precision for targeted quantitative HDL proteomics. J. Proteom. 2015, 113, 388–399. [Google Scholar] [CrossRef]
- Pagel, O.; Loroch, S.; Sickmann, A.; Zahedi, R.P. Current strategies and findings in clinically relevant post-translational modification-specific proteomics. Expert Rev. Proteom. 2015, 12, 235–253. [Google Scholar] [CrossRef] [Green Version]
- Ehrenkranz, J.R.; Lewis, N.G.; Kahn, C.R.; Roth, J. Phlorizin: A Review. Diabetes Metab. Res. Rev. 2005, 21, 31–38. [Google Scholar]
- Masumoto, S.; Akimoto, Y.; Oike, H.; Kobori, M. Dietary phloridzin reduces blood glucose levels and reverses Sglt1 expression in the small intestine in streptozotocin-induced diabetic mice. J. Agric. Food Chem. 2009, 57, 4651–4656. [Google Scholar] [CrossRef] [PubMed]
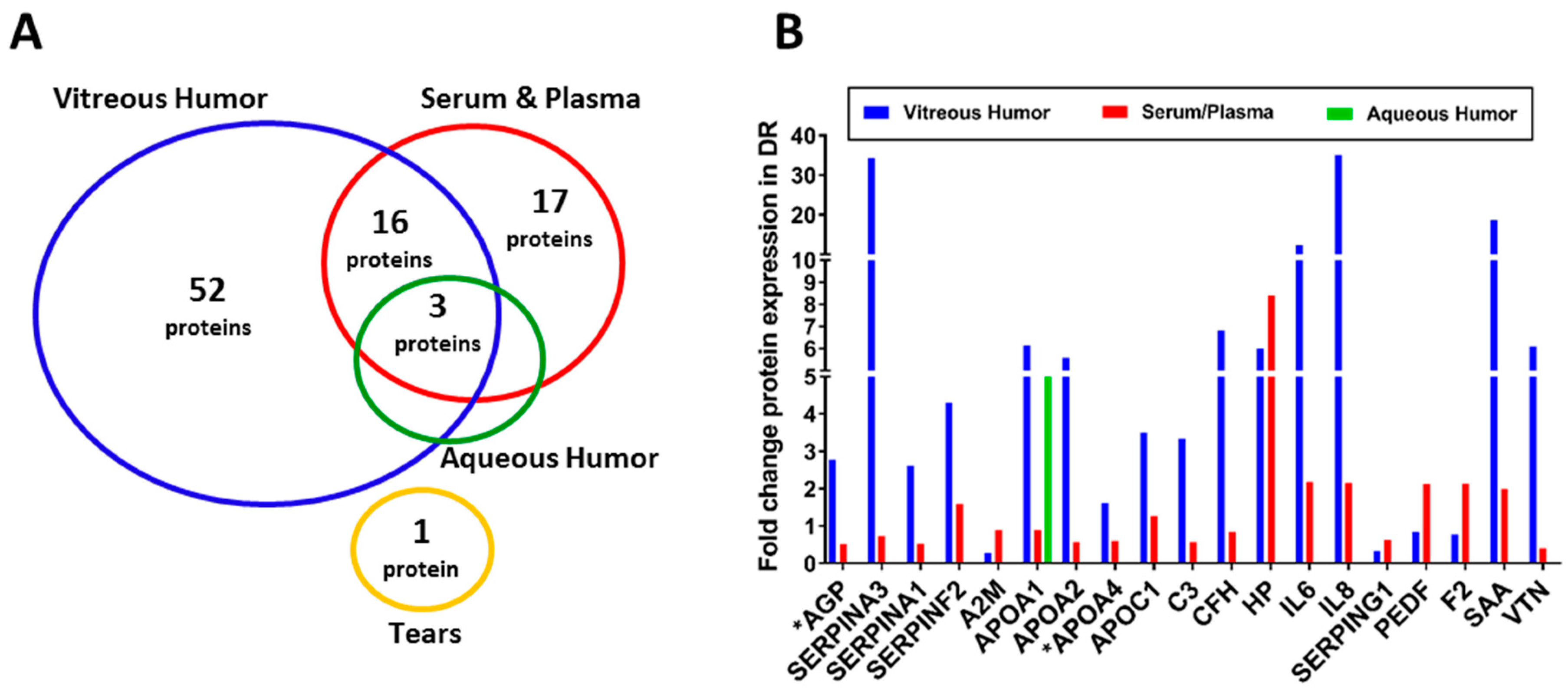
Figure 1.
Summary of differentially expressed proteins identified in biofluids of DR patients. (A) The number of potential biomarkers of retinal inflammation in each biofluid, as identified by the studies discussed in this review. (B) The bar graphs represent fold change in expression of 19 biomarkers identified in at least two biofluids. * AGP and APOA4 proteins were detected in the AH of DR patients, but fold change was not available.
Figure 1.
Summary of differentially expressed proteins identified in biofluids of DR patients. (A) The number of potential biomarkers of retinal inflammation in each biofluid, as identified by the studies discussed in this review. (B) The bar graphs represent fold change in expression of 19 biomarkers identified in at least two biofluids. * AGP and APOA4 proteins were detected in the AH of DR patients, but fold change was not available.


{kind=link}
Table 1.
Biomarkers of retinal inflammation in diabetic retinopathy (DR) patients detected using proteomic approaches.
Table 1.
Biomarkers of retinal inflammation in diabetic retinopathy (DR) patients detected using proteomic approaches.
| Biomarker | Symbol | Fluid | Comparison | Detection Method | Ref. |
|---|---|---|---|---|---|
| α-1-acid glycoprotein | AGP | Serum; Plasma; VH; AH | DR/noDR; PDR/Healthy; PDR/NDM; PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS; SDS-PAGE/LC-MS/MS; LC-MS/MS; MRM | [4,10,13,16,82] |
| α-1-antichymotrypsin | SERPINA3 | Plasma;VH | DR/noDR; PDR/NDM; PDR/Post-mortem | SDS-PAGE/LC-MS/MS; LC-MS/MS; MRM | [4,16,82] |
| α-1-antitrypsin | SERPINA1 | Plasma; VH | DR/noDR; NPDR/NDM; PDR/NDM; PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS; SDS-PAGE/LC-MS/MS; LC-MS/MS; MRM | [4,16,63,82] |
| α-2-antiplasmin | SERPINF2 | Plasma;VH | DME/NDM; NPDR/NDM; PDR/NDM | LC-MS/MS; ELISA | [15,83] |
| α-2-HS-glycoprotein | AHSG | VH | DME/NDM; PDR/NDM | SDS-PAGE/LC-MS/MS; LC-MS/MS | [15,16] |
| α-2-macroglobulin | A2M | Plasma; VH | DR/noDR; PDR/Post-mortem | LC-MS/MS; MRM | [4,82] |
| Amyloid β A4 protein | APP | VH | PDR/NDM; PDR/noDR | SDS-PAGE/LC-MS/MS; LC-MS/MS | [13,16] |
| Angiotensinogen | AGT | VH | PDR/NDM; PDR/noDR | SDS-PAGE/LC-MS/MS | [16] |
| Antithrombin III | SERPINC1 | VH | PDR/NDM; PDR/Post-mortem | SDS-PAGE/LC-MS/MS; LC-MS/MS | [4,16] |
| Apolipoprotein A-I | APOA1 | Plasma; VH; AH | DME/NDM; DR/noDR; NPDR/NDM; PDR/NDM; PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS; SDS-PAGE/LC-MS/MS; LC-MS/MS; MRM | [4,13,15,16,63,65,82] |
| Apolipoprotein A-II | APOA2 | Plasma; VH | DME/NDM; DR/noDR; PDR/NDM | SDS-PAGE/LC-MS/MS; LC-MS/MS; MRM | [13,15,16,82] |
| Apolipoprotein A-IV | APOA4 | Plasma; VH; AH | DR/noDR; NPDR/NDM; PDR/NDM; PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS LC-MS/MS; MRM | [4,13,63,82] |
| Apolipoprotein C-I | APOC1 | Plasma; VH | DR/noDR;PDR/NDM; Anti-VEGF treated PDR/untreated PDR | LC-MS/MS; MRM | [33,82] |
| Apolipoprotein C-III | APOC3 | VH | PDR/NDM | SDS-PAGE/LC-MS/MS | [16] |
| Apolipoprotein E | APOE | VH | DME/NDM; PDR/Post-mortem | LC-MS/MS | [4,70] |
| ATP-binding cassette subfamily F member 1 | ABCF1 | VH | DME/NDM | LC-MS/MS | [70] |
| Basement membrane-specific heparan sulfate proteoglycan core protein | HSPG2 | VH | PDR/NDM | SDS-PAGE/LC-MS/MS | [16] |
| β-2-microglobulin | B2M | VH | PDR/NDM | SDS-PAGE/LC-MS/MS | [16] |
| β-crystallin A3 | CRYBA1 | VH | PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS/MS; LC-MS/MS | [4,20] |
| C-reactive protein | CRP | Serum; Plasma | DR/NDM; DR/noDR; NPDR/PDR | Multiplex Bead Array; ELISA | [74,84,85] |
| C-C motif chemokine 5 | CCL13 | Serum | Severe DR/Mild DR | ELISA | [86] |
| Chitinase-3-like protein 1 | CHI3L1 | VH | PDR/NDM | SDS-PAGE/LC-MS/MS | [16] |
| Clusterin | CLU | VH | DME/NDM; PDR/NDM; PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS/MS; 2D-DIGE/MALDI-TOF-TOF MS; LC-MS/MS | [4,20,39,64] |
| Cofilin-1 | CFL1 | VH | PDR/Post-mortem | LC-MS/MS | [4] |
| Complement C1 | C1 | VH | DME/NDM; PDR/NDM | 2D-DIGE/MALDI-TOF-TOF MS; LC-MS/MS | [39,70] |
| Complement C3 | C3 | Plasma;VH | DME/NDM; DR/noDR NPDR/NDM; PDR/NDM; PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS; SDS-PAGE/LC-MS/MS; LC-MS/MS; MRM | [4,15,16,63,82] |
| Complement C4 | C4 | VH | DME/NDM; PDR/NDM; PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS; LC-MS/MS | [4,39] |
| Complement C7 | C7 | VH | DME/NDM | LC-MS/MS | [15] |
| Complement C8 | C8 | VH | DME/NDM | LC-MS/MS | [15] |
| Complement factor B | CFB | Plasma | DR/noDR | MRM | [82] |
| Complement factor H | CFH | Plasma; VH | DME/NDM; DR/noDR | LC-MS/MS; MRM | [15,82] |
| Complement factor I | CFI | VH | PDR/NDM; PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS/MS; SDS-PAGE/LC-MS/MS; LC-MS/MS | [13,16,20] |
| Estrogen receptor | ESR1 | VH | PDR/Post-mortem | LC-MS/MS | [4] |
| Fibrinogen | FGA, FGB, FGG | VH | DME/NDM; NPDR/NDM; PDR/NDM; PDR/Post-mortem; Anti-VEGF treated PDR/untreated PDR | 2D-DIGE/MALDI-TOF-TOF MS; LC-MS/MS | [4,35,39,63] |
| Fibronectin | FN1 | VH | Anti-VEGF treated PDR/untreated PDR | LC-MS/MS | [35] |
| Gelsolin | GSN | VH | DME/PDR; PDR/NDM | 2D-DIGE/MALDI-TOF-TOF MS | [39] |
| Guanylate-binding protein3 | GBP3 | VH | PDR/Post-mortem | LC-MS/MS | [4] |
| Haptoglobin | HP | Serum; Plasma; VH | DME/NDM; DR/NDM; PDR/Healthy | 2D-DIGE/MALDI-TOF-TOF MS; LC-MS/MS; MRM | [10,15,73] |
| Immunoglobulin α chain | IGHA1 | VH | PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS/MS | [20] |
| Immunoglobulin γ chain | IGHG1 | VH | PDR/NDM; PDR/Post-mortem | SDS-PAGE/LC-MS/MS; LC-MS/MS | [4,16] |
| Immunogloulin heavy chain V-III region BRO | IGHV3-13 | VH | PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS/MS | [20] |
| Immunoglobulin κ chain | IGK | VH | PDR/NDM; PDR/Post-mortem | SDS-PAGE/LC-MS/MS; LC-MS/MS | [4,16] |
| Immunoglobulin λ chain | IGH | VH | PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS/MS | [20] |
| Inter-α-trypsin inhibitor heavy chain family, member 4 | ITIH4 | VH | DME/NDM | LC-MS/MS | [15] |
| Intercellular adhesion molecule 1 | ICAM1 | Serum | NPDR/NDM; NPDR/noDR; NPDR/PDR; PDR/NDM; PDR/noDR | Multiplex Bead Array; ELISA | [74,87] |
| Interferon γ-induced protein 10 | CXCL10 | VH | DME/NDM | Multiplex Bead Array | [66] |
| Interleukin-1 | IL1 | VH | DME/NDM | Multiplex Bead Array | [66] |
| Interleukin-1 receptor antagonist | IL1RN | VH | DME/NDM; PDR/NDM | Multiplex Bead Array | [66] |
| Interleukin-2 receptor | IL2R | Serum | NPDR/NDM; PDR/NPDR/noDR; NPDR/PDR; PDR/NDM; PDR/noDR | Chemiluminescent Immunometric Assay | [88] |
| Interleukin-6 | IL6 | Plasma; VH | DME/NDM; nPDR/NDM; PDR/NDM | Multiplex Bead Array; ELISA | [66,89] |
| Interleukin-6 receptor | IL6R | Serum | DR/noDR | Multiplex Bead Array | [74] |
| Interleukin-8 | CXCL8 | Serum; VH | DME/NDM; NPDR/NDM; nPDR/noDR; NPDR/PDR; PDR/NDM; PDR/noDR | Multiplex Bead Array; Chemiluminescent Immunometric Assay | [66,88] |
| Interleukin-10 | IL10 | VH | PDR/NDM | Multiplex Bead Array | [66] |
| Interleukin-12 | IL12 | VH | PDR/NDM | Multiplex Bead Array | [66] |
| Interleukin-13 | IL13 | VH | PDR/NDM | Multiplex Bead Array | [66] |
| Keratin, type II cytoskeletal I | KRT1 | VH | PDR/NDM; Anti-VEGF treated PDR/untreated PDR | LC-MS/MS | [33] |
| Kininogen 1 | KNG1 | VH | DME/NDM; PDR/NDM | LC-MS/MS | [13,15] |
| Lactotransferrin | LTF | Tear | PDR/noDR | LC-MS/MS | [17] |
| Leukocyte platelet-activating factor receptor | PTAFR | VH | PDR/Post-mortem | LC-MS/MS | [4] |
| Macrophage inflammatory protein 1 | CCL3, CCL4 | VH | PDR/NDM | Multiplex Bead Array | [66] |
| Metalloproteinase inhibitor 2 | TIMP2 | VH | PDR/NDM; Anti-VEGF treated PDR/untreated PDR | LC-MS/MS | [33] |
| Monocyte chemoattractant protein-1 | CCL2 | VH | PDR/NDM | Multiplex Bead Array | [66] |
| Monocyte differentiation antigen CD14 | CD14 | VH | PDR/NDM | SDS-PAGE/LC-MS/MS | [16] |
| Nuclear receptor subfamily 1D2 | NR1D2 | VH | DME/NDM | LC-MS/MS | [70] |
| Osteopontin | SPP1 | VH | Post-photocoagulation/Pre- photocoagulation | LC-MS/MS | [35] |
| Pentraxin-related protein 3 | PTX3 | Plasma | DR/NDM; DR/noDR | ELISA | [85] |
| Peptidyl-prolyl cis-trans isomerase a | PPIA | VH | PDR/Post-mortem | LC-MS/MS | [4] |
| Peroxiredoxin 2 | PRDX2 | Plasma | DR/NDM | MRM | [73] |
| Plasma protease C1 inhibitor | SERPING1 | Plasma; VH | DR/noDR; PDR/Post-mortem | LC-MS/MS; MRM | [4,82] |
| Plasma serine protease inhibitor | SERPINA5 | VH | PDR/NDM; Anti-VEGF treated PDR/untreated PDR | LC-MS/MS | [33] |
| Plasminogen activator inhibitor 1 | SERPINE1 | Serum | Dr/noDR | Protein Array | [90] |
| Pigment epithelium-derived factor | PEDF | Plasma; VH | DR/NDM; DR/noDR; PDR/NDM; PDR/Post-mortem | 2D-DIGE/MALDI-TOF-TOF MS/MS; SDS-PAGE/LC-MS/MS; LC-MS/MS; MRM; ELISA | [4,16,82,91] |
| Protein Dj-1 | PARK7 | VH | PDR/Post-mortem | LC-MS/MS | [4] |
| Protein FAM3C | FAM3C | VH | DME/NDM | LC-MS/MS | [70] |
| Prothrombin | F2 | Plasma; VH | DME/NDM; DR/noDR; PDR/NDM; PDR/Post-mortem | SDS-PAGE/LC-MS/MS; LC-MS/MS; MRM | [4,13,16,82] |
| Retinoic acid receptor responder 2 | RARRES2 | VH | DME/NDM | LC-MS/MS | [15] |
| Serum amyloid A protein | SAA | Serum;VH | DME/NDM; DR/noDR | LC-MS/MS; Multiplex Bead Array | [15,74] |
| E-selectin | SELE | Serum | DR/noDR | Protein Array | [90] |
| Soluble glycoprotein 130 | sgp130 | Serum | DR/noDR | Multiplex Bead Array | [74] |
| Stromal cell-derived factor 1α | CXCL12 | Serum | Severe DR/Mild DR | ELISA | [86] |
| Transthyretin | TTR | VH | DME/NDM; DME/PDR | 2D-DIGE/MALDI-TOF-TOF MS | [39] |
| Tumor necrosis factor α | TNF | Serum | NPDR/NDM; NPDR/noDR; NPDR/PDR; PDR/NDM; PDR/noDR | Chemiluminescent Immunometric Assay | [88] |
| Tumor necrosis factor receptor | TNFR | Serum | DR/noDR | Multiplex Bead Array | [74,88] |
| Vascular cell adhesion protein 1 | VCAM1 | Serum | NPDR/NDM; NPDR/noDR; NPDR/PDR; PDR/NDM; PDR/noDR | Multiplex Bead Array; ELISA | [74,87] |
| Vascular endothelial growth factor | VEGF | Serum; Plasma | NPDR/NDM; NPDR/noDR; PDR/NDM; PDR/noDR; NPDR/PDR | ELISA; Multiplex Bead Array | [87,92,93,94] |
| Vascular endothelial growth factor receptor 1 | FLT1 | VH | Anti-VEGF treated PDR/untreated PDR | LC-MS/MS | [35] |
| Vitronectin | VTN | Plasma; VH | DME/NDM; DR/noDR; PDR/NDM | LC-MS/MS; MRM | [13,15,82] |
AH: Aqueous humor; VH: Vitreous humor; DR: Diabetic retinopathy; noDR: Diabetic controls without diabetic retinopathy; PDR: Proliferative diabetic retinopathy; NPDR: Non-proliferative diabetic retinopathy; DME: Diabetic macular edema; NDM: Non-diabetic controls; LC-MS/MS: Liquid chromatography tandem mass spectrometry; SDS-PAGE/LC-MS/MS: Sodium dodecyl sulfate polyacrylamide gel electrophoresis coupled with liquid chromatography mass spectrometry; 2D-DIGE/MALDI-TOF-TOF MS: Two-dimensional gel electrophoresis coupled with matrix-assisted laser desorption/ionization time of flight tandem mass spectrometry; MRM: Multiple reaction monitoring; ELISA: Enzyme-linked immunosorbent assay.
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Youngblood, H.; Robinson, R.; Sharma, A.; Sharma, S. Proteomic Biomarkers of Retinal Inflammation in Diabetic Retinopathy. Int. J. Mol. Sci. 2019, 20, 4755. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20194755
AMA Style
Youngblood H, Robinson R, Sharma A, Sharma S. Proteomic Biomarkers of Retinal Inflammation in Diabetic Retinopathy. International Journal of Molecular Sciences. 2019; 20(19):4755. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20194755
Chicago/Turabian StyleYoungblood, Hannah, Rebekah Robinson, Ashok Sharma, and Shruti Sharma. 2019. "Proteomic Biomarkers of Retinal Inflammation in Diabetic Retinopathy" International Journal of Molecular Sciences 20, no. 19: 4755. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20194755
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.