Circulating CRP Levels Are Associated with Epicardial and Visceral Fat Depots in Women with Metabolic Syndrome Criteria

 , and
, and
Abstract
:1. Introduction
2. Results
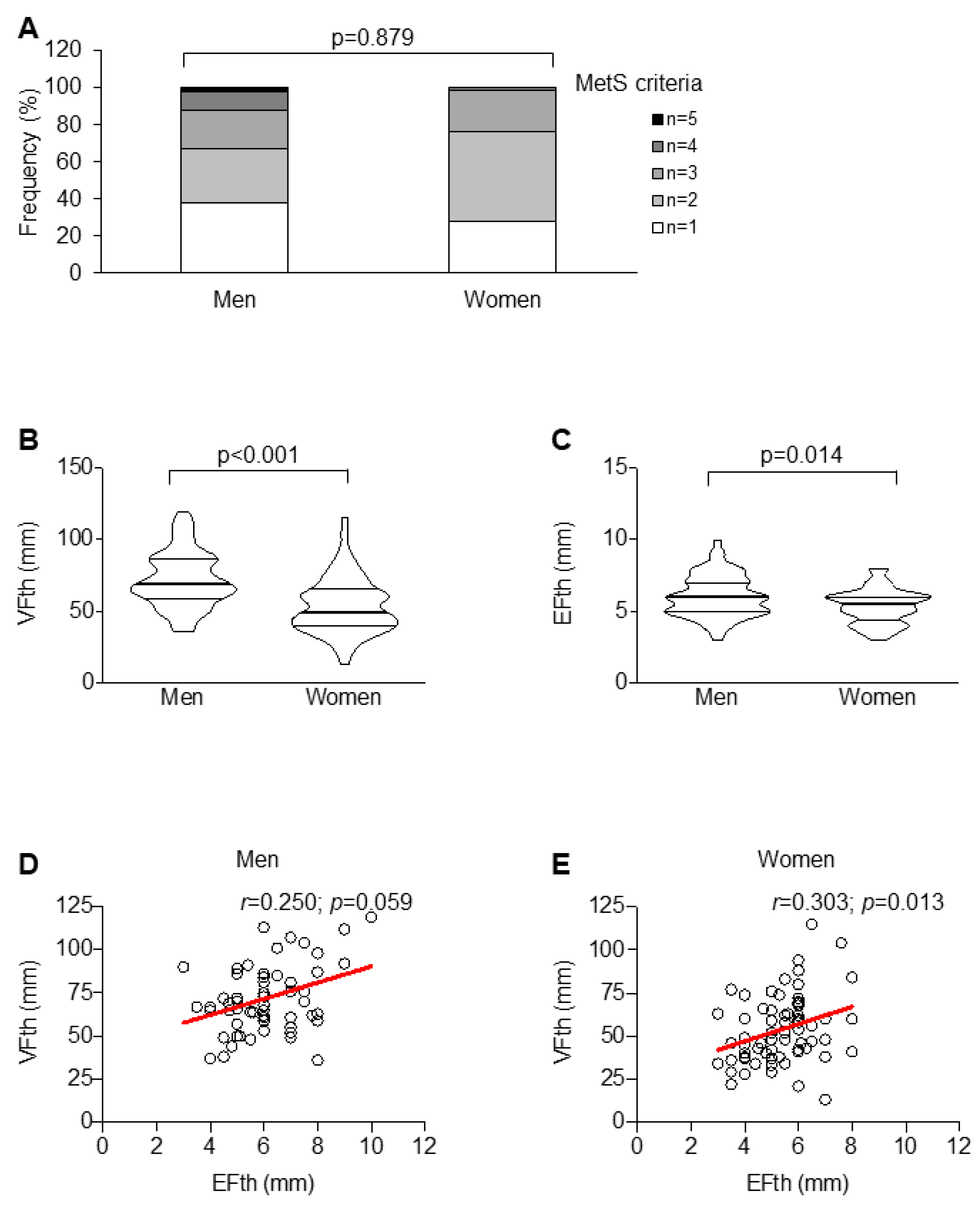
2.1. Men and Women Have a Similar Metabolic Profile
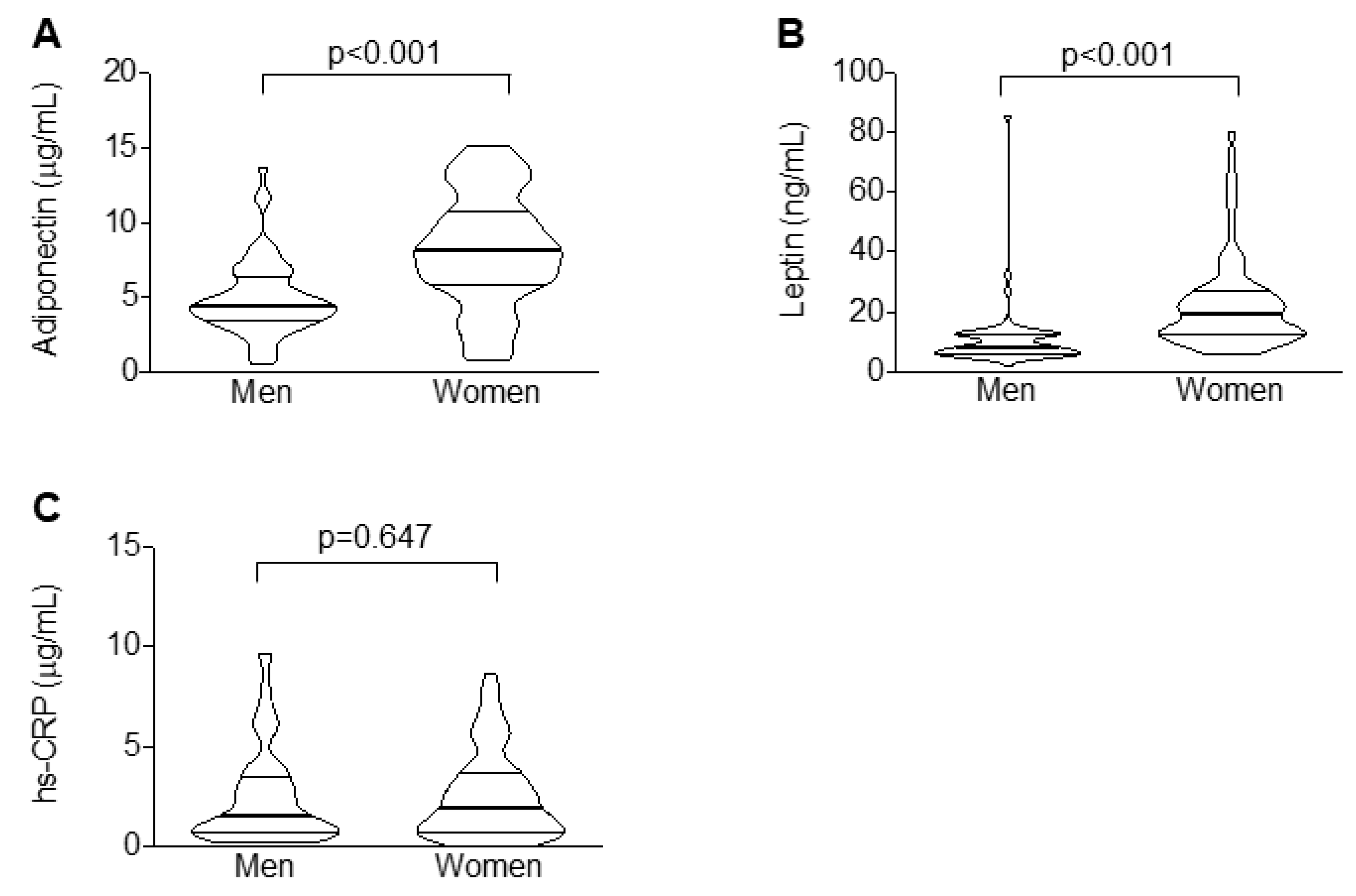
2.2. Men Have Increased Ectopic Fat Depots but Reduced Circulating Adipocytokine Levels as Compared to Women
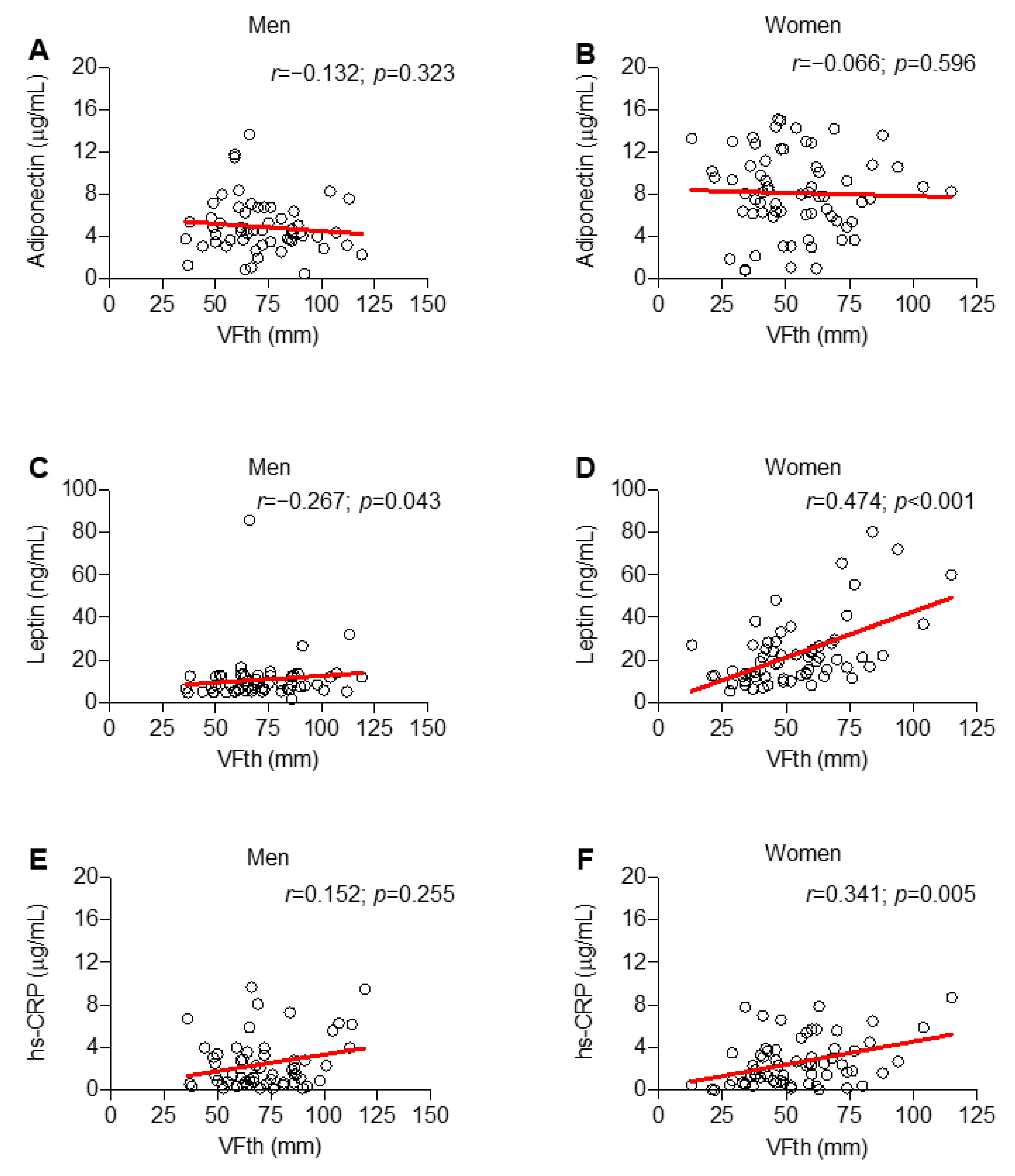
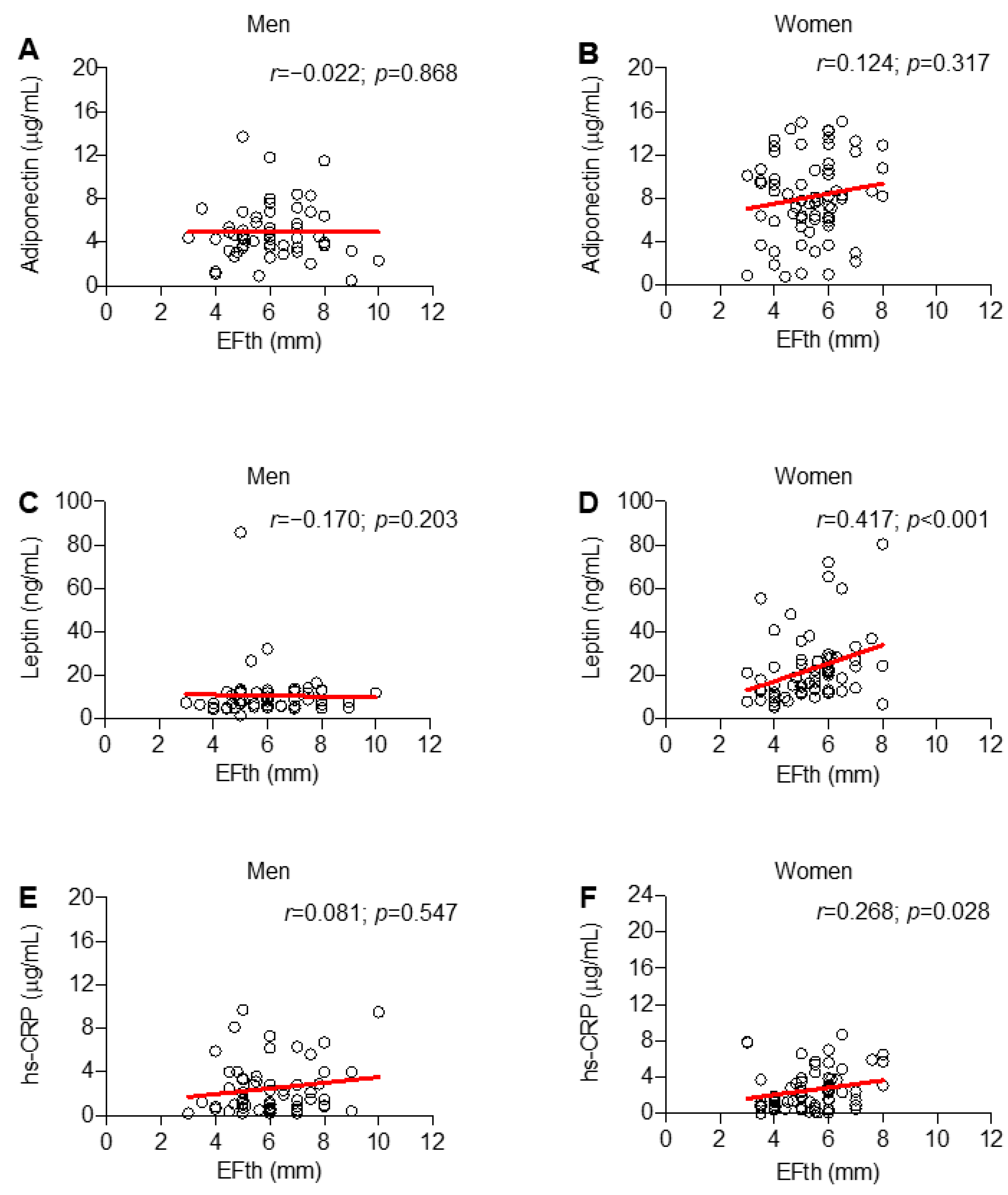
2.3. Only in Women, Circulating Levels of Leptin and CRP are Associated with Visceral and Ectopic Fat Depots
3. Discussion
4. Material and Methods
4.1. Patients
4.2. Study Endpoints and Statistical Power Calculation
4.3. Data Collection and Assessment
4.4. Ultrasound Assessment of Fat Depots
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Vecchie, A.; Dallegri, F.; Carbone, F.; Bonaventura, A.; Liberale, L.; Portincasa, P.; Fruhbeck, G.; Montecucco, F. Obesity phenotypes and their paradoxical association with cardiovascular diseases. Eur. J. Intern. Med. 2018, 48, 6–17. [Google Scholar] [CrossRef] [PubMed]
- Bays, H.E. Adiposopathy is “sick fat” a cardiovascular disease? J. Am. Coll Cardiol 2011, 57, 2461–2473. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C.; Tremblay, A.; Despres, J.P.; Nadeau, A.; Lupien, P.J.; Theriault, G.; Dussault, J.; Moorjani, S.; Pinault, S.; Fournier, G. The response to long-term overfeeding in identical twins. N. Engl. J. Med. 1990, 322, 1477–1482. [Google Scholar] [CrossRef] [PubMed]
- Nazare, J.A.; Smith, J.D.; Borel, A.L.; Haffner, S.M.; Balkau, B.; Ross, R.; Massien, C.; Almeras, N.; Despres, J.P. Ethnic influences on the relations between abdominal subcutaneous and visceral adiposity, liver fat, and cardiometabolic risk profile: The International Study of Prediction of Intra-Abdominal Adiposity and Its Relationship With Cardiometabolic Risk/Intra-Abdominal Adiposity. Am. J. Clin. Nutr 2012, 96, 714–726. [Google Scholar] [PubMed]
- Chella Krishnan, K.; Mehrabian, M.; Lusis, A.J. Sex differences in metabolism and cardiometabolic disorders. Curr Opin Lipidol 2018, 29, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Singer, K.; Maley, N.; Mergian, T.; DelProposto, J.; Cho, K.W.; Zamarron, B.F.; Martinez-Santibanez, G.; Geletka, L.; Muir, L.; Wachowiak, P.; et al. Differences in Hematopoietic Stem Cells Contribute to Sexually Dimorphic Inflammatory Responses to High Fat Diet-induced Obesity. J. Biol. Chem. 2015, 290, 13250–13262. [Google Scholar] [CrossRef]
- Fall, T.; Hagg, S.; Ploner, A.; Magi, R.; Fischer, K.; Draisma, H.H.; Sarin, A.P.; Benyamin, B.; Ladenvall, C.; Akerlund, M.; et al. Age- and sex-specific causal effects of adiposity on cardiovascular risk factors. Diabetes 2015, 64, 1841–1852. [Google Scholar] [CrossRef]
- Rabkin, S.W. The relationship between epicardial fat and indices of obesity and the metabolic syndrome: A systematic review and meta-analysis. Metab. Syndr. Relat. Disord. 2014, 12, 31–42. [Google Scholar] [CrossRef]
- Bredella, M.A. Sex Differences in Body Composition. Adv. Exp. Med. Biol 2017, 1043, 9–27. [Google Scholar]
- Ferrara, D.; Montecucco, F.; Dallegri, F.; Carbone, F. Impact of different ectopic fat depots on cardiovascular and metabolic diseases. J. Cell. Physiol. 2019, 234, 21630–21641. [Google Scholar] [CrossRef]
- Thorand, B.; Baumert, J.; Doring, A.; Herder, C.; Kolb, H.; Rathmann, W.; Giani, G.; Koenig, W.; Group, K. Sex differences in the relation of body composition to markers of inflammation. Atherosclerosis 2006, 184, 216–224. [Google Scholar] [CrossRef]
- Carbone, F.; Nulli Migliola, E.; Bonaventura, A.; Vecchie, A.; De Vuono, S.; Ricci, M.A.; Vaudo, G.; Boni, M.; Dallegri, F.; Montecucco, F.; et al. High serum levels of C-reactive protein (CRP) predict beneficial decrease of visceral fat in obese females after sleeve gastrectomy. Nutr Metab Cardiovasc Dis 2018, 28, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Belanger, C.; Luu-The, V.; Dupont, P.; Tchernof, A. Adipose tissue intracrinology: Potential importance of local androgen/estrogen metabolism in the regulation of adiposity. Horm Metab Res. 2002, 34, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Fei, J.; Cook, C.; Blough, E.; Santanam, N. Age and sex mediated changes in epicardial fat adipokines. Atherosclerosis 2010, 212, 488–494. [Google Scholar] [CrossRef]
- Kocher, C.; Christiansen, M.; Martin, S.; Adams, C.; Wehner, P.; Gress, T.; Santanam, N. Sexual dimorphism in obesity-related genes in the epicardial fat during aging. J. Physiol Biochem 2017, 73, 215–224. [Google Scholar] [CrossRef]
- El Khoudary, S.R.; Shields, K.J.; Janssen, I.; Hanley, C.; Budoff, M.J.; Barinas-Mitchell, E.; Everson-Rose, S.A.; Powell, L.H.; Matthews, K.A. Cardiovascular Fat, Menopause, and Sex Hormones in Women: The SWAN Cardiovascular Fat Ancillary Study. J. Clin. Endocrinol Metab 2015, 100, 3304–3312. [Google Scholar] [CrossRef]
- El Khoudary, S.R.; Shields, K.J.; Janssen, I.; Budoff, M.J.; Everson-Rose, S.A.; Powell, L.H.; Matthews, K.A. Postmenopausal Women With Greater Paracardial Fat Have More Coronary Artery Calcification Than Premenopausal Women: The Study of Women’s Health Across the Nation (SWAN) Cardiovascular Fat Ancillary Study. J. Am. Heart Assoc. 2017, 6, 2. [Google Scholar] [CrossRef]
- Chu, A.Y.; Deng, X.; Fisher, V.A.; Drong, A.; Zhang, Y.; Feitosa, M.F.; Liu, C.T.; Weeks, O.; Choh, A.C.; Duan, Q.; et al. Multiethnic genome-wide meta-analysis of ectopic fat depots identifies loci associated with adipocyte development and differentiation. Nat. Genet. 2017, 49, 125–130. [Google Scholar] [CrossRef]
- Tamura, Y. Ectopic fat, insulin resistance and metabolic disease in non-obese Asians: Investigating metabolic gradation. Endocr. J. 2019, 66, 1–9. [Google Scholar] [CrossRef]
- Mancuso, P.; Bouchard, B. The Impact of Aging on Adipose Function and Adipokine Synthesis. Front. Endocrinol. 2019, 10, 137. [Google Scholar] [CrossRef]
- Neeland, I.J.; Poirier, P.; Despres, J.P. Cardiovascular and Metabolic Heterogeneity of Obesity: Clinical Challenges and Implications for Management. Circulation 2018, 137, 1391–1406. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Joseph, L.; Pilote, L. Obesity and C-reactive protein in various populations: A systematic review and meta-analysis. Obes Rev. 2013, 14, 232–244. [Google Scholar] [CrossRef] [PubMed]
- Soriano-Maldonado, A.; Aparicio, V.A.; Felix-Redondo, F.J.; Fernandez-Berges, D. Severity of obesity and cardiometabolic risk factors in adults: Sex differences and role of physical activity. The HERMEX study. Int J. Cardiol 2016, 223, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Camporez, J.P.; Lyu, K.; Goldberg, E.L.; Zhang, D.; Cline, G.W.; Jurczak, M.J.; Dixit, V.D.; Petersen, K.F.; Shulman, G.I. Anti-inflammatory effects of oestrogen mediate the sexual dimorphic response to lipid-induced insulin resistance. J. Physiol. 2019, 597, 3885–3903. [Google Scholar] [CrossRef] [PubMed]
- Abildgaard, J.; Danielsen, E.R.; Dorph, E.; Thomsen, C.; Juul, A.; Ewertsen, C.; Pedersen, B.K.; Pedersen, A.T.; Ploug, T.; Lindegaard, B. Ectopic Lipid Deposition Is Associated With Insulin Resistance in Postmenopausal Women. J. Clin. Endocrinol Metab 2018, 103, 3394–3404. [Google Scholar] [CrossRef]
- Ridker, P.M.; Hennekens, C.H.; Rifai, N.; Buring, J.E.; Manson, J.E. Hormone replacement therapy and increased plasma concentration of C-reactive protein. Circulation 1999, 100, 713–716. [Google Scholar] [CrossRef]
- Rexrode, K.M.; Pradhan, A.; Manson, J.E.; Buring, J.E.; Ridker, P.M. Relationship of total and abdominal adiposity with CRP and IL-6 in women. Ann. Epidemiol. 2003, 13, 674–682. [Google Scholar] [CrossRef]
- White, U.A.; Tchoukalova, Y.D. Sex dimorphism and depot differences in adipose tissue function. Biochim Biophys Acta 2014, 1842, 377–392. [Google Scholar] [CrossRef]
- Valencak, T.G.; Osterrieder, A.; Schulz, T.J. Sex matters: The effects of biological sex on adipose tissue biology and energy metabolism. Redox Biol. 2017, 12, 806–813. [Google Scholar] [CrossRef]
- Hickey, M.S.; Israel, R.G.; Gardiner, S.N.; Considine, R.V.; McCammon, M.R.; Tyndall, G.L.; Houmard, J.A.; Marks, R.H.; Caro, J.F. Gender differences in serum leptin levels in humans. Biochem. Mol. Med. 1996, 59, 1–6. [Google Scholar] [CrossRef]
- Kennedy, A.; Gettys, T.W.; Watson, P.; Wallace, P.; Ganaway, E.; Pan, Q.; Garvey, W.T. The metabolic significance of leptin in humans: Gender-based differences in relationship to adiposity, insulin sensitivity, and energy expenditure. J. Clin. Endocrinol Metab 1997, 82, 1293–1300. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.; Punyanitya, M.; Silva, A.M.; Chen, J.; Gallagher, D.; Sardinha, L.B.; Allison, D.B.; Heymsfield, S.B. Sexual dimorphism of adipose tissue distribution across the lifespan: A cross-sectional whole-body magnetic resonance imaging study. Nutr. Metab. 2009, 6, 17. [Google Scholar] [CrossRef] [PubMed]
- Salami, S.S.; Tucciarone, M.; Bess, R.; Kolluru, A.; Szpunar, S.; Rosman, H.; Cohen, G. Race and epicardial fat: The impact of anthropometric measurements, percent body fat and sex. Ethn. Dis. 2013, 23, 281–285. [Google Scholar] [PubMed]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed] [Green Version]
- American Diabetes, A. 2. Classification and Diagnosis of Diabetes. Diabetes Care 2016, 39, S13–S22. [Google Scholar]
- Amato, M.C.; Giordano, C.; Galia, M.; Criscimanna, A.; Vitabile, S.; Midiri, M.; Galluzzo, A.; AlkaMeSy Study, G. Visceral Adiposity Index: A reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care 2010, 33, 920–922. [Google Scholar] [CrossRef] [Green Version]
- Amato, M.C.; Giordano, C.; Pitrone, M.; Galluzzo, A. Cut-off points of the visceral adiposity index (VAI) identifying a visceral adipose dysfunction associated with cardiometabolic risk in a Caucasian Sicilian population. Lipids Health Dis. 2011, 10, 183. [Google Scholar] [CrossRef] [Green Version]
- Stolk, R.P.; Meijer, R.; Mali, W.P.; Grobbee, D.E.; van der Graaf, Y.; Secondary Manifestations of Arterial Disease (SMART) Study Group. Ultrasound measurements of intraabdominal fat estimate the metabolic syndrome better than do measurements of waist circumference. Am. J. Clin. Nutr 2003, 77, 857–860. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.K.; Kim, H.J.; Hur, K.Y.; Choi, S.H.; Ahn, C.W.; Lim, S.K.; Kim, K.R.; Lee, H.C.; Huh, K.B.; Cha, B.S. Visceral fat thickness measured by ultrasonography can estimate not only visceral obesity but also risks of cardiovascular and metabolic diseases. Am. J. Clin. Nutr 2004, 79, 593–599. [Google Scholar] [CrossRef] [Green Version]
- Trouwborst, I.; Bowser, S.M.; Goossens, G.H.; Blaak, E.E. Ectopic Fat Accumulation in Distinct Insulin Resistant Phenotypes; Targets for Personalized Nutritional Interventions. Front. Nutr. 2018, 5, 77. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Overall Cohort (n = 125) |
|---|---|
| Clinical | |
| Age, yr. [IQR] | 56 (49–62) |
| Men, no. (%) | 58 (46.4) |
| Active smokers, no. (%) | 21 (16.8) |
| Hypertension, no (%) | 100 (80.0) |
| IFG, no (%) | 1 (0.8) |
| T2DM, no (%) | 17 (13.6) |
| sBP, mmHg [IQR] | 130 (120–135) |
| dBP, mmHg [IQR] | 80 (72–85) |
| Waist circumference, cm [IQR] | 99 (93–108) |
| Weight, Kg [IQR] | 77 (68–90) |
| BMI, Kg/m2 [IQR] | 27.2 (25.1–30.3) |
| MetS criteria | |
| 1 | 41 (32.7) |
| 2 | 49 (39.2) |
| 3 | 27 (21.6) |
| 4 | 7 (5.6) |
| 5 | 1 (0.8) |
| MetS | 35 (28.0) |
| Ultrasound assessment | |
| EFth, mm [IQR] | 5.6 (4.8–6.5) |
| VFth, mm [IQR] | 61 (46–76) |
| Hepatic steatosis, no. (%) | 85 (68.0) |
| Biochemistry | |
| Serum total-c, mg/dL [IQR] | 194 (168–219) |
| Serum LDL-c, mg/dL [IQR] | 111 (83–129) |
| Serum HDL-c, mg/dL [IQR] | 60 (50–71) |
| Serum TAG, mg/dL [IQR] | 101 (71–139) |
| Fasting glycaemia, mg/dL [IQR] | 89 (83–99) |
| VAI, n [IQR] | 1.3 (0.8–1.9) |
| Clinical Data | Men (n = 66) | Women (n = 75) | p-Value |
|---|---|---|---|
| Age, yr. (IQR) | 56 (49–60) | 57 (47–63) | 0.335 |
| Active smokers, no. (%) | 11 (19.0) | 10 (14.9) | 0.634 |
| sBP, mmHg (IQR) | 130 (125–135) | 125 (115–136) | 0.017 |
| dBP, mmHg (IQR) | 80 (80–89) | 80 (70–85) | 0.010 |
| Waist circumference, cm (IQR) | 103 (95–110) | 97 (90–102) | 0.005 |
| Weight, Kg (IQR) | 86 (76–93) | 70 (63–80) | < 0.001 |
| BMI, kg/m2 (IQR) | 28.4 (25.7–30.4) | 26.7 (24.8–30.0) | 0.216 |
| Biochemistry | |||
| Serum total-c, mg/dL (IQR) | 186 (161–210) | 197 (170–225) | 0.042 |
| Serum LDL-c, mg/dL (IQR) | 110 (81–127) | 116 (89–133) | 0.259 |
| Serum HDL-c, mg/dL (IQR) | 53 (43–59) | 69 (60–77) | < 0.001 |
| Serum TAG, mg/dL (IQR) | 118 (85–169) | 90 (65–126) | 0.001 |
| Fasting glycaemia, mg/dL (IQR) | 92 (86–104) | 87 (82–98) | 0.013 |
| VAI, n (IQR) | 1.4 (0.9–2.2) | 1.3 (0.8–1.7) | 0.130 |
| Variables | Univariate | Adjusted | ||
|---|---|---|---|---|
| VFth | B (95% CI) | p-Value | B (95% CI) | p-Value |
| Age | 0.69 (0.22–1.15) | 0.004 | 0.33 (–0.09–0.76) | 0.122 |
| MetS criteria | 13.37 (7.84–18.91) | < 0.001 | 9.46 (3.78–15) | 0.001 |
| Leptin | 0.15 (0.02–0.28) | 0.025 | 0.14 (0.03–0.24) | 0.012 |
| hs-CRP | 3.52 (1.47–5.57) | 0.001 | 2.61 (0.75–4.47) | 0.007 |
| EFth | B (95% CI) | p–value | B (95% CI) | p-value |
| Age | 0.05 (0.02–0.08) | < 0.001 | 0.03 (0.01–0.06) | 0.006 |
| MetS criteria | 0.85 (0.51–1.18) | < 0.001 | 0.61 (0.30–0.12) | 0.001 |
| Leptin | 0.01 (–0.00–0.01) | 0.116 | - | - |
| hs-CRP | 0.12 (0.02–0.25) | 0.026 | 0.05 (–0.06–0.17) | 0.390 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carbone, F.; Lattanzio, M.S.; Minetti, S.; Ansaldo, A.M.; Ferrara, D.; Molina-Molina, E.; Belfiore, A.; Elia, E.; Pugliese, S.; Palmieri, V.O.; et al. Circulating CRP Levels Are Associated with Epicardial and Visceral Fat Depots in Women with Metabolic Syndrome Criteria. Int. J. Mol. Sci. 2019, 20, 5981. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20235981
Carbone F, Lattanzio MS, Minetti S, Ansaldo AM, Ferrara D, Molina-Molina E, Belfiore A, Elia E, Pugliese S, Palmieri VO, et al. Circulating CRP Levels Are Associated with Epicardial and Visceral Fat Depots in Women with Metabolic Syndrome Criteria. International Journal of Molecular Sciences. 2019; 20(23):5981. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20235981
Chicago/Turabian StyleCarbone, Federico, Maria Stefania Lattanzio, Silvia Minetti, Anna Maria Ansaldo, Daniele Ferrara, Emilio Molina-Molina, Anna Belfiore, Edoardo Elia, Stefania Pugliese, Vincenzo Ostilio Palmieri, and et al. 2019. "Circulating CRP Levels Are Associated with Epicardial and Visceral Fat Depots in Women with Metabolic Syndrome Criteria" International Journal of Molecular Sciences 20, no. 23: 5981. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms20235981