Infrapatellar Fat Pad Gene Expression and Protein Production in Patients with and without Osteoarthritis

 , ,
, ,  ,
,  , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Demographic and Clinical Characteristics of Patients
2.2. Histopathological Grading
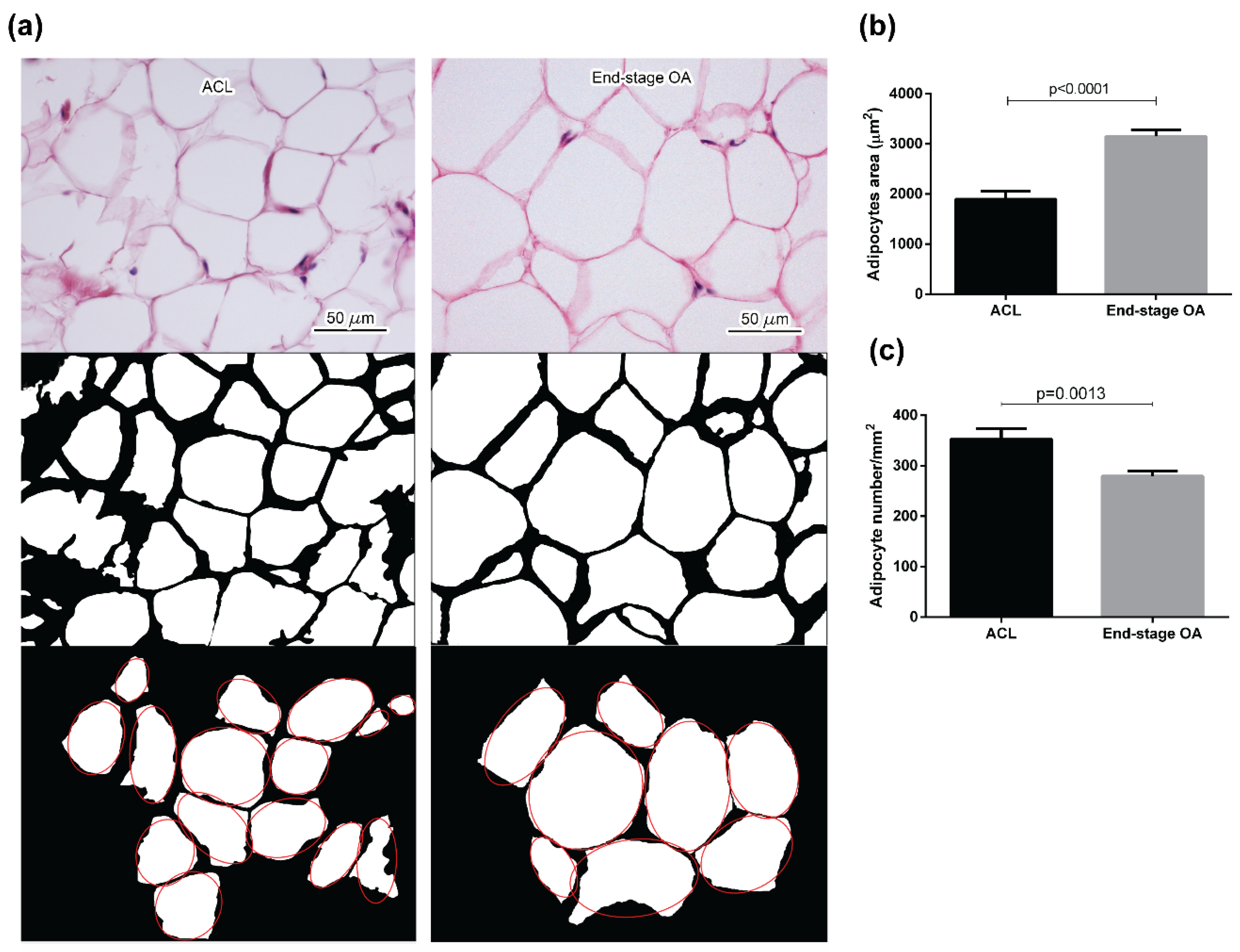
2.3. Adipocyte Morphology Evaluation
2.4. Gene Expression Analysis and Immunohistochemistry
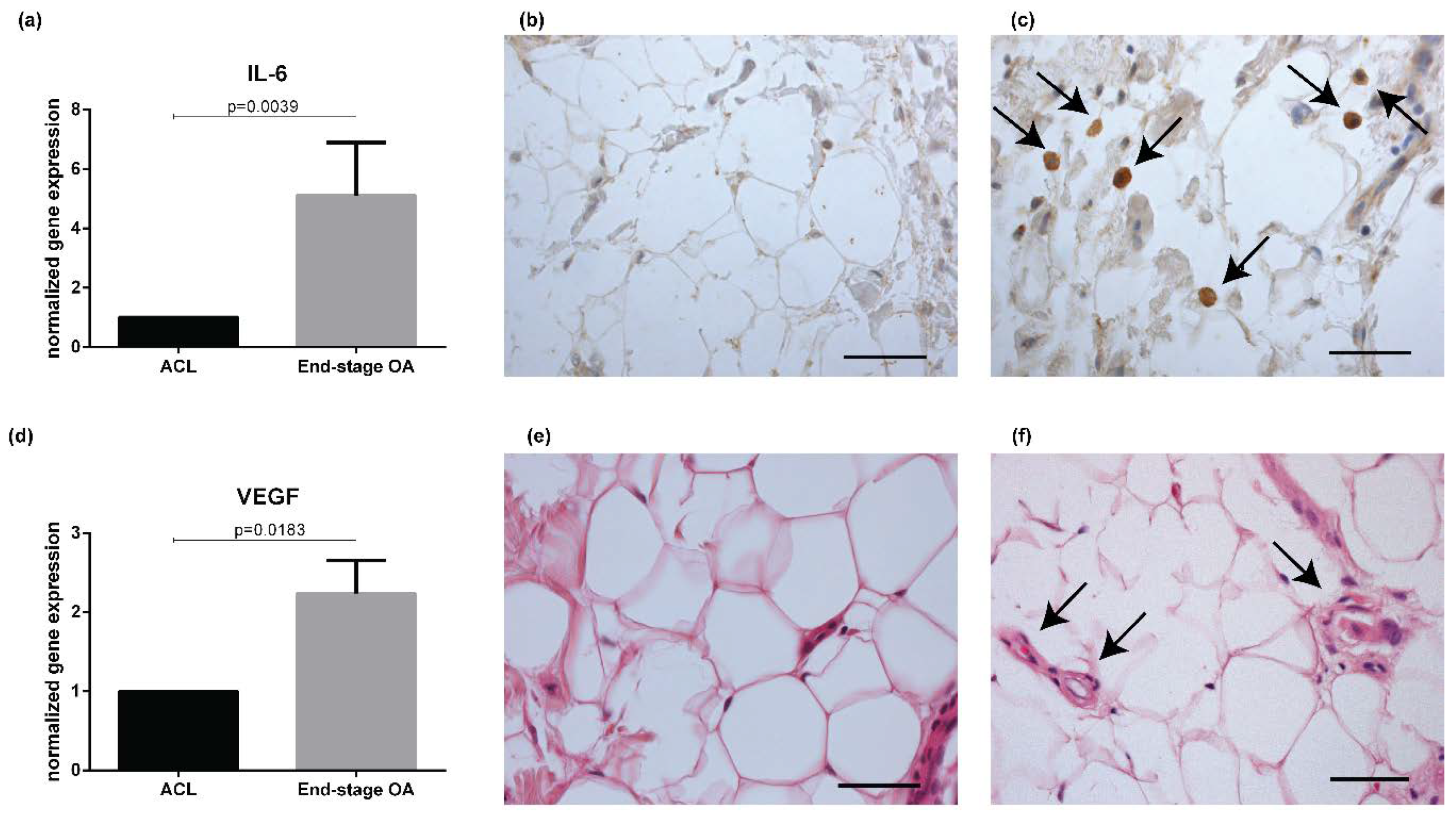
2.4.1. Inflammation and Vascularization
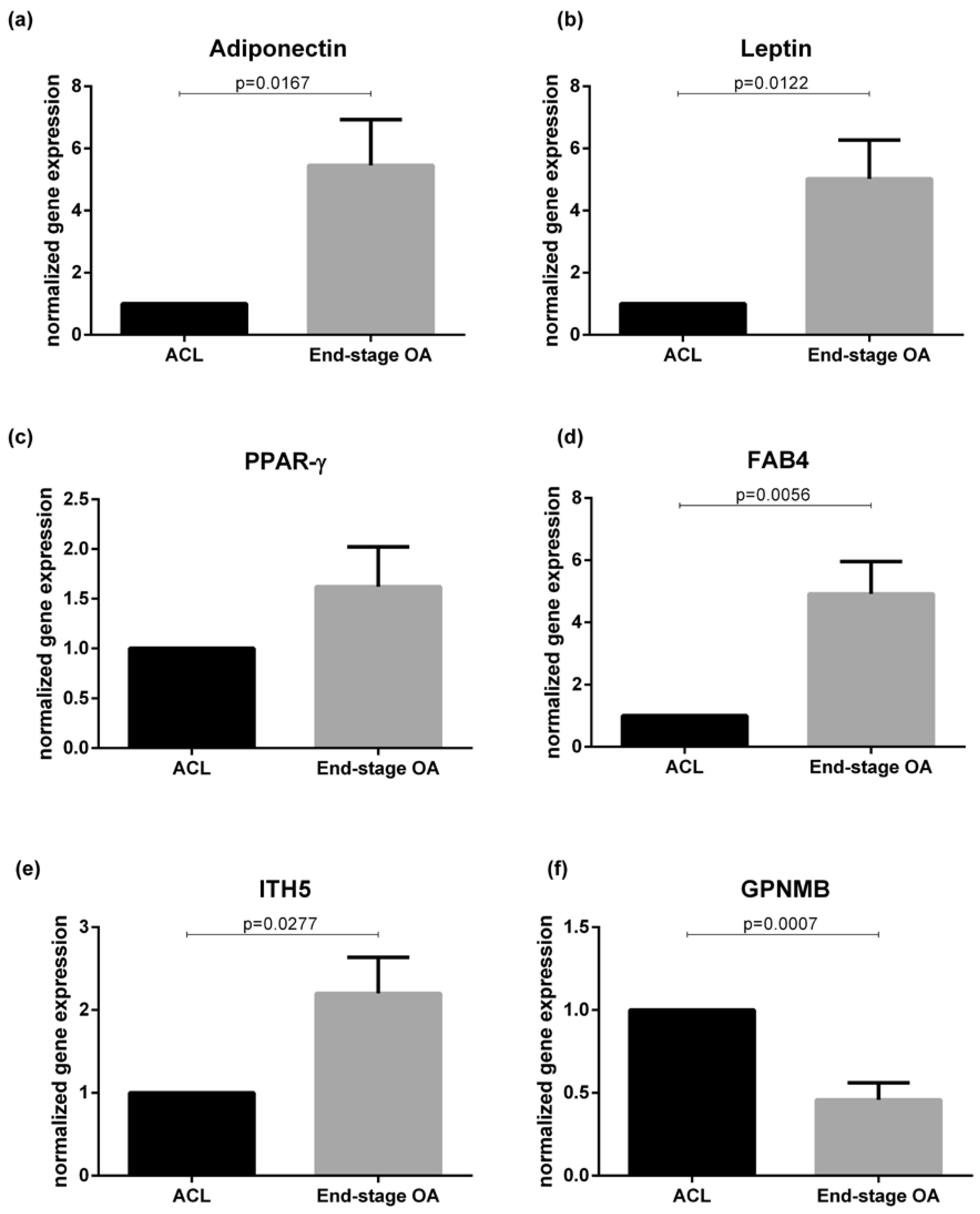
2.4.2. Adipokines
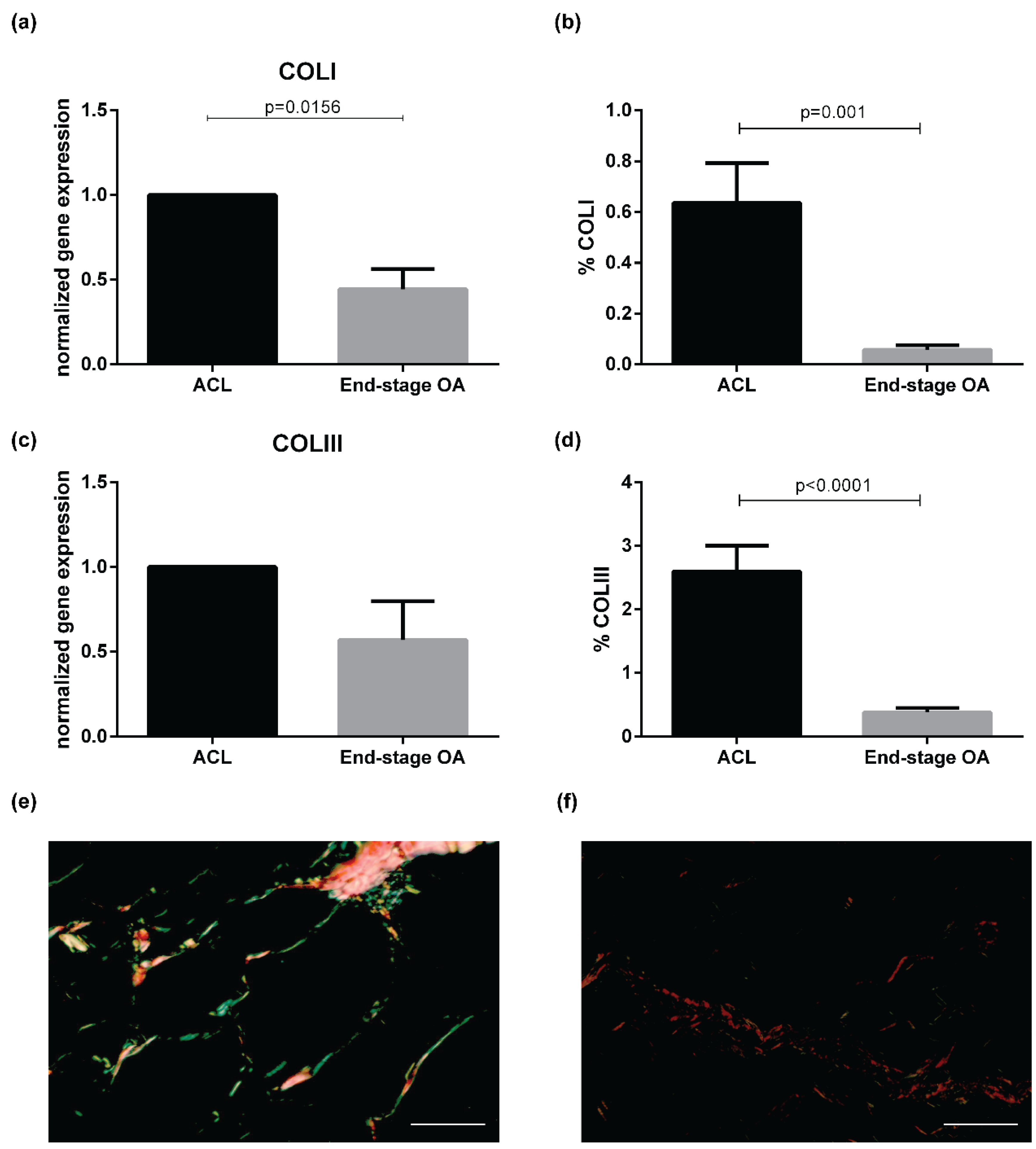
2.4.3. Extracellular Matrix Remodeling
2.5. Correlations Between Histological Data and Morphometric Analysis
2.6. Influence of BMI and Age
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Histology and Immunohistochemistry
4.3. Morphometric Analysis
4.4. Gene Expression Analysis
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ACLR | anterior cruciate ligament reconstruction |
| COLI | collagen Type I |
| COLIII | collagen Type Iii |
| COLVI | collagen Type Vi |
| CXCL8 | C-X-C motif chemokine ligand 8 |
| FABP4 | fatty acid-binding protein 4 |
| GPNMB | transmembrane glycoprotein NMB |
| HE | hematoxylin–eosin |
| IFP | infrapatellar fat pad |
| IL-6 | interleukin-6 |
| ITH5 | inter-A-trypsin inhibitor heavy chain 5 |
| MCP-1 | monocyte chemotactic protein 1 |
| OA | osteoarthritis |
| PPARγ | peroxisome proliferative activated receptor gamma |
| QRT-PCR | quantitative real-time PCR |
| SERPIN2 | serine proteinase inhibitor 2 |
| TGF-Β | transforming growth factor Β |
| TNF-A | tumor necrosis factor-A |
| TKR | total knee replacement |
| VEGF | vascular endothelial growth factor |
References
- Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Lond. Engl. 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Cross, M.; Smith, E.; Hoy, D.; Nolte, S.; Ackerman, I.; Fransen, M.; Bridgett, L.; Williams, S.; Guillemin, F.; Hill, C.L.; et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Belluzzi, E.; El Hadi, H.; Granzotto, M.; Rossato, M.; Ramonda, R.; Macchi, V.; De Caro, R.; Vettor, R.; Favero, M. Systemic and local adipose tissue in knee osteoarthritis. J. Cell Physiol. 2017, 232, 1971–1978. [Google Scholar] [CrossRef] [PubMed]
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef] [Green Version]
- Favero, M.; Belluzzi, E.; Trisolino, G.; Goldring, M.B.; Goldring, S.R.; Cigolotti, A.; Pozzuoli, A.; Ruggieri, P.; Ramonda, R.; Grigolo, B.; et al. Inflammatory molecules produced by meniscus and synovium in early and end-stage osteoarthritis: A coculture study. J. Cell Physiol. 2019, 234, 11176–11187. [Google Scholar] [CrossRef]
- Favero, M.; Ramonda, R.; Goldring, M.B.; Goldring, S.R.; Punzi, L. Early knee osteoarthritis. RMD Open 2015, 1, e000062. [Google Scholar] [CrossRef]
- Castrogiovanni, P.; Di Rosa, M.; Ravalli, S.; Castorina, A.; Guglielmino, C.; Imbesi, R.; Vecchio, M.; Drago, F.; Szychlinska, M.A.; Musumeci, G. Moderate physical activity as a prevention method for knee osteoarthritis and the role of synoviocytes as biological key. Int. J. Mol. Sci. 2019, 20, 511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castrogiovanni, P.; Trovato, F.M.; Loreto, C.; Nsir, H.; Szychlinska, M.A.; Musumeci, G. Nutraceutical supplements in the management and prevention of osteoarthritis. Int. J. Mol. Sci. 2016, 17, 2042. [Google Scholar] [CrossRef]
- Szychlinska, M.A.; Castrogiovanni, P.; Trovato, F.M.; Nsir, H.; Zarrouk, M.; Lo Furno, D.; Di Rosa, M.; Imbesi, R.; Musumeci, G. Physical activity and mediterranean diet based on olive tree phenolic compounds from two different geographical areas have protective effects on early osteoarthritis, muscle atrophy and hepatic steatosis. Eur. J. Nutr. 2019, 58, 565–581. [Google Scholar] [CrossRef]
- Belluzzi, E.; Stocco, E.; Pozzuoli, A.; Granzotto, M.; Porzionato, A.; Vettor, R.; De Caro, R.; Ruggieri, P.; Ramonda, R.; Rossato, M.; et al. Contribution of infrapatellar fat pad and synovial membrane to knee osteoarthritis pain. BioMed Res. Int. 2019, 2019, 18. [Google Scholar] [CrossRef]
- Belluzzi, E.; Olivotto, E.; Toso, G.; Cigolotti, A.; Pozzuoli, A.; Biz, C.; Trisolino, G.; Ruggieri, P.; Grigolo, B.; Ramonda, R.; et al. Conditioned media from human osteoarthritic synovium induces inflammation in a synoviocyte cell line. Connect. Tissue Res. 2019, 60, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Eymard, F.; Pigenet, A.; Citadelle, D.; Flouzat-Lachaniette, C.H.; Poignard, A.; Benelli, C.; Berenbaum, F.; Chevalier, X.; Houard, X. Induction of an inflammatory and prodegradative phenotype in autologous fibroblast-like synoviocytes by the infrapatellar fat pad from patients with knee osteoarthritis. Arthritis Rheumatol. 2014, 66, 2165–2174. [Google Scholar] [CrossRef] [PubMed]
- Eymard, F.; Pigenet, A.; Citadelle, D.; Tordjman, J.; Foucher, L.; Rose, C.; Flouzat Lachaniette, C.H.; Rouault, C.; Clement, K.; Berenbaum, F.; et al. Knee and hip intra-articular adipose tissues (IAATs) compared with autologous subcutaneous adipose tissue: A specific phenotype for a central player in osteoarthritis. Ann. Rheum. Dis. 2017, 76, 1142–1148. [Google Scholar] [CrossRef] [Green Version]
- Macchi, V.; Stocco, E.; Stecco, C.; Belluzzi, E.; Favero, M.; Porzionato, A.; De Caro, R. The infrapatellar fat pad and the synovial membrane: An anatomo-functional unit. J. Anat. 2018, 233, 146–154. [Google Scholar] [CrossRef] [Green Version]
- Zhong, Y.C.; Wang, S.C.; Han, Y.H.; Wen, Y. Recent advance in source, property, differentiation, and applications of infrapatellar fat pad adipose-derived stem cells. Stem Cells Int. 2020, 2020, 2560174. [Google Scholar] [CrossRef]
- Stocco, E.; Barbon, S.; Piccione, M.; Belluzzi, E.; Petrelli, L.; Pozzuoli, A.; Ramonda, R.; Rossato, M.; Favero, M.; Ruggieri, P.; et al. Infrapatellar fat pad stem cells responsiveness to microenvironment in osteoarthritis: From morphology to function. Front. Cell Dev. Biol. 2019, 7, 323. [Google Scholar] [CrossRef] [PubMed]
- Fontanella, C.G.; Belluzzi, E.; Rossato, M.; Olivotto, E.; Trisolino, G.; Ruggieri, P.; Rubini, A.; Porzionato, A.; Natali, A.; De Caro, R.; et al. Quantitative MRI analysis of infrapatellar and suprapatellar fat pads in normal controls, moderate and end-stage osteoarthritis. Ann. Anat. Anat. Anz. Off. Organ Anat. Ges. 2019, 221, 108–114. [Google Scholar] [CrossRef]
- Wang, K.; Ding, C.; Hannon, M.J.; Chen, Z.; Kwoh, C.K.; Hunter, D.J. Quantitative signal intensity alteration in infrapatellar fat pad predicts incident radiographic osteoarthritis: The osteoarthritis initiative. Arthritis Care Res. 2019, 71, 30–38. [Google Scholar] [CrossRef]
- Han, W.; Aitken, D.; Zhu, Z.; Halliday, A.; Wang, X.; Antony, B.; Cicuttini, F.; Jones, G.; Ding, C. Hypointense signals in the infrapatellar fat pad assessed by magnetic resonance imaging are associated with knee symptoms and structure in older adults: A cohort study. Arthritis Res. Ther. 2016, 18, 234. [Google Scholar] [CrossRef] [Green Version]
- Fontanella, C.G.; Macchi, V.; Carniel, E.L.; Frigo, A.; Porzionato, A.; Picardi, E.E.E.; Favero, M.; Ruggieri, P.; de Caro, R.; Natali, A.N. Biomechanical behavior of Hoffa’s fat pad in healthy and osteoarthritic conditions: Histological and mechanical investigations. Australas. Phys. Eng. Sci. Med. 2018, 41, 657–667. [Google Scholar] [CrossRef]
- Fontanella, C.G.; Carniel, E.L.; Frigo, A.; Macchi, V.; Porzionato, A.; Sarasin, G.; Rossato, M.; De Caro, R.; Natali, A.N. Investigation of biomechanical response of Hoffa’s fat pad and comparative characterization. J. Mech. Behav. Biomed. Mater. 2017, 67, 1–9. [Google Scholar] [CrossRef]
- Pauli, C.; Whiteside, R.; Heras, F.L.; Nesic, D.; Koziol, J.; Grogan, S.P.; Matyas, J.; Pritzker, K.P.; D’Lima, D.D.; Lotz, M.K. Comparison of cartilage histopathology assessment systems on human knee joints at all stages of osteoarthritis development. Osteoarthr. Cartil. 2012, 20, 476–485. [Google Scholar] [CrossRef] [Green Version]
- Benito, M.J.; Veale, D.J.; FitzGerald, O.; van den Berg, W.B.; Bresnihan, B. Synovial tissue inflammation in early and late osteoarthritis. Ann. Rheum. Dis. 2005, 64, 1263–1267. [Google Scholar] [CrossRef] [Green Version]
- Harasymowicz, N.S.; Clement, N.D.; Azfer, A.; Burnett, R.; Salter, D.M.; Simpson, A. Regional differences between perisynovial and infrapatellar adipose tissue depots and their response to class II and class III obesity in patients with osteoarthritis. Arthritis Rheumatol 2017, 69, 1396–1406. [Google Scholar] [CrossRef]
- de Jong, A.J.; Klein-Wieringa, I.R.; Andersen, S.N.; Kwekkeboom, J.C.; Herb-van Toorn, L.; de Lange-Brokaar, B.J.E.; van Delft, D.; Garcia, J.; Wei, W.; van der Heide, H.J.L.; et al. Lack of high BMI-related features in adipocytes and inflammatory cells in the infrapatellar fat pad (IFP). Arthritis Res. Ther. 2017, 19, 186. [Google Scholar] [CrossRef] [Green Version]
- Barboza, E.; Hudson, J.; Chang, W.P.; Kovats, S.; Towner, R.A.; Silasi-Mansat, R.; Lupu, F.; Kent, C.; Griffin, T.M. Profibrotic infrapatellar fat pad remodeling without M1 macrophage polarization precedes knee osteoarthritis in mice with diet-induced obesity. Arthritis Rheumatol 2017, 69, 1221–1232. [Google Scholar] [CrossRef]
- Garcia, J.; Wei, W.; Runhaar, J.; Wright, K.; Mennan, C.; Roberts, S.; Van Osch, G.; Bastiaansen-Jenniskens, Y. Obesity does not affect the size of infrapatellar fat pad adipocytes: Implications for the pathogenesis of knee osteoarthritis. Osteoarthr. Cartil. 2016, 24, S334–S335. [Google Scholar] [CrossRef]
- Mansour, M.F.; Chan, C.-W.J.; Laforest, S.; Veilleux, A.; Tchernof, A. Sex differences in body fat distribution. In Adipose Tissue Biology; Symonds, M.E., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 257–300. [Google Scholar]
- Michaud, A.; Laforest, S.; Pelletier, M.; Nadeau, M.; Simard, S.; Daris, M.; Lebœuf, M.; Vidal, H.; Géloën, A.; Tchernof, A. Abdominal adipocyte populations in women with visceral obesity. Endocrinology 2016, 174, 227–239. [Google Scholar] [CrossRef] [Green Version]
- Favero, M.; El-Hadi, H.; Belluzzi, E.; Granzotto, M.; Porzionato, A.; Sarasin, G.; Rambaldo, A.; Iacobellis, C.; Cigolotti, A.; Fontanella, C.G.; et al. Infrapatellar fat pad features in osteoarthritis: A histopathological and molecular study. Rheumatol. Oxf. 2017, 56, 1784–1793. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, R.; Takahashi, M.; Virtanen, C.; Syed, K.; Davey, J.R.; Mahomed, N.N. Microarray analysis of the infrapatellar fat pad in knee osteoarthritis: Relationship with joint inflammation. J. Rheumatol. 2011, 38, 1966–1972. [Google Scholar] [CrossRef]
- Conde, J.; Scotece, M.; Abella, V.; Gomez, R.; Lopez, V.; Villar, R.; Hermida, M.; Pino, J.; Gomez-Reino, J.J.; Gualillo, O. Identification of novel adipokines in the joint. Differential expression in healthy and osteoarthritis tissues. PLoS ONE 2015, 10, e0123601. [Google Scholar] [CrossRef] [Green Version]
- Gabriel, T.L.; Tol, M.J.; Ottenhof, R.; van Roomen, C.; Aten, J.; Claessen, N.; Hooibrink, B.; de Weijer, B.; Serlie, M.J.; Argmann, C.; et al. Lysosomal stress in obese adipose tissue macrophages contributes to MITF-dependent Gpnmb induction. Diabetes 2014, 63, 3310–3323. [Google Scholar] [CrossRef] [Green Version]
- Rugg, M.S.; Willis, A.C.; Mukhopadhyay, D.; Hascall, V.C.; Fries, E.; Fulop, C.; Milner, C.M.; Day, A.J. Characterization of complexes formed between TSG-6 and inter-alpha-inhibitor that act as intermediates in the covalent transfer of heavy chains onto hyaluronan. J. Biol. Chem. 2005, 280, 25674–25686. [Google Scholar] [CrossRef] [Green Version]
- Anveden, A.; Sjoholm, K.; Jacobson, P.; Palsdottir, V.; Walley, A.J.; Froguel, P.; Al-Daghri, N.; McTernan, P.G.; Mejhert, N.; Arner, P.; et al. ITIH-5 expression in human adipose tissue is increased in obesity. Obes. Silver Spring Md. 2012, 20, 708–714. [Google Scholar] [CrossRef] [Green Version]
- Pasarica, M.; Gowronska-Kozak, B.; Burk, D.; Remedios, I.; Hymel, D.; Gimble, J.; Ravussin, E.; Bray, G.A.; Smith, S.R. Adipose tissue collagen VI in obesity. J. Clin. Endocrinol. Metab. 2009, 94, 5155–5162. [Google Scholar] [CrossRef] [Green Version]
- Onuma, H.; Tsuji, K.; Hoshino, T.; Inomata, K.; Udo, M.; Nakagawa, Y.; Katagiri, H.; Miyatake, K.; Watanabe, T.; Sekiya, I.; et al. Fibrotic changes in the infrapatellar fat pad induce new vessel formation and sensory nerve fiber endings that associate prolonged pain. J. Orthop. Res. 2020, 38, 1296–1306. [Google Scholar] [CrossRef]
- Punzi, L.; Galozzi, P.; Luisetto, R.; Favero, M.; Ramonda, R.; Oliviero, F.; Scanu, A. Post-traumatic arthritis: Overview on pathogenic mechanisms and role of inflammation. RMD Open 2016, 2, e000279. [Google Scholar] [CrossRef]
- Bigoni, M.; Sacerdote, P.; Turati, M.; Franchi, S.; Gandolla, M.; Gaddi, D.; Moretti, S.; Munegato, D.; Augusti, C.A.; Bresciani, E.; et al. Acute and late changes in intraarticular cytokine levels following anterior cruciate ligament injury. J. Orthop. Res. Off. Publ. Orthop. Res. Soc. 2013, 31, 315–321. [Google Scholar] [CrossRef]
- Heilmeier, U.; Mamoto, K.; Amano, K.; Eck, B.; Tanaka, M.; Bullen, J.A.; Schwaiger, B.J.; Huebner, J.L.; Stabler, T.V.; Kraus, V.B.; et al. Infrapatellar fat pad abnormalities are associated with a higher inflammatory synovial fluid cytokine profile in young adults following ACL tear. Osteoarthr. Cartil. 2020, 28, 82–91. [Google Scholar] [CrossRef] [Green Version]
- Macchi, V.; Porzionato, A.; Sarasin, G.; Petrelli, L.; Guidolin, D.; Rossato, M.; Fontanella, C.G.; Natali, A.; De Caro, R. The infrapatellar adipose body: A histotopographic study. Cells Tissues Organs 2016, 201, 220–231. [Google Scholar] [CrossRef]
- Pfaffl, M.W.; Tichopad, A.; Prgomet, C.; Neuvians, T.P. Determination of stable housekeeping genes, differentially regulated target genes and sample integrity: BestKeeper—Excel-based tool using pair-wise correlations. Biotechnol. Lett. 2004, 26, 509–515. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IFP Histopathological Grading | ACL (n = 23) | End-Stage OA (n = 25) | p-Value |
|---|---|---|---|
| Lymphocytic Infiltration, number (%) | 1 (3.6) | 20 (80) | <0.0001 |
| Grade 0, number (%) | 22 (95.7) | 5 (20) | |
| Grade 1, number (%) | 1 (3.6) | 7 (28) | |
| Grade 2, number (%) | 0 (0) | 13 (52) | |
| Vascularity, median (IQR) | 8.9 (17.5–7.2) | 30.6 (42.9–30.6) | <0.0001 |
| IFP Adipocytes | ACL (n = 24) | End-Stage OA (n = 25) | p-Value |
|---|---|---|---|
| Area (μm2), median (IQR) | 1798.03 (2362.46–1113.82) | 3128.72 (3632.46–2583.45) | <0.0001 |
| Major axis (μm), median (IQR) | 53.60 (62.68–42.47) | 72.16 (78.98–66.45) | <0.0001 |
| Minor axis (μm), median (IQR) | 39.79 (49.43–32.63) | 52.73 (58.90–48.70) | <0.0001 |
| eccentricity, median (IQR) | 0.66 (0.70–0.63) | 0.67 (0.70–0.64) | 0.211 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Belluzzi, E.; Macchi, V.; Fontanella, C.G.; Carniel, E.L.; Olivotto, E.; Filardo, G.; Sarasin, G.; Porzionato, A.; Granzotto, M.; Pozzuoli, A.; et al. Infrapatellar Fat Pad Gene Expression and Protein Production in Patients with and without Osteoarthritis. Int. J. Mol. Sci. 2020, 21, 6016. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21176016
Belluzzi E, Macchi V, Fontanella CG, Carniel EL, Olivotto E, Filardo G, Sarasin G, Porzionato A, Granzotto M, Pozzuoli A, et al. Infrapatellar Fat Pad Gene Expression and Protein Production in Patients with and without Osteoarthritis. International Journal of Molecular Sciences. 2020; 21(17):6016. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21176016
Chicago/Turabian StyleBelluzzi, Elisa, Veronica Macchi, Chiara Giulia Fontanella, Emanuele Luigi Carniel, Eleonora Olivotto, Giuseppe Filardo, Gloria Sarasin, Andrea Porzionato, Marnie Granzotto, Assunta Pozzuoli, and et al. 2020. "Infrapatellar Fat Pad Gene Expression and Protein Production in Patients with and without Osteoarthritis" International Journal of Molecular Sciences 21, no. 17: 6016. https://0-doi-org.brum.beds.ac.uk/10.3390/ijms21176016